July 2021 - What works to support the mental health and wellbeing of children aged 0-12? A review of the latest research evidence Prepared for the ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

What works to support the mental health and wellbeing of children aged 0-12? A review of the latest research evidence Prepared for the Mental Health Commission of NSW by Dr Stephen Carbone, Prevention United July 2021
Suggested citation: Carbone, Stephen. What works to support the mental health and wellbeing of children aged 0-12? A review of the latest research evidence, prepared for the Mental Health Commission of NSW. Melbourne, Prevention United, 2021 Copies of the review may be download from the Mental Health Commission’s website at: https://www.nswmentalhealthcommission.com.au/research-and-evidence Disclaimer: This Review was produced in response to specific questions from the commissioning agency. It is not necessarily a comprehensive review of all literature relating to the topic area. It was current at the time of production (but not necessarily at the time of publication). It is reproduced for general information and third parties rely upon it at their own risk.
Contents
Executive Summary ........................................................................................................................i
1. Introduction .................................................................................................................... 1
2. Understanding child and adolescent mental health and wellbeing ................................. 2
2.1. Key concepts ........................................................................................................................... 2
2.2. Prevalence of mental wellbeing and mental ill-health ............................................................. 3
2.3. Promotion, prevention and early intervention ......................................................................... 4
2.4. Risk and protective factors ...................................................................................................... 4
2.5. Promotion, prevention and early intervention benefits ............................................................ 6
3. Interventions for perinatal mental health. ....................................................................... 8
3.1. Health behaviours. .................................................................................................................. 8
3.2. Self-help programs .................................................................................................................. 9
3.3. Mindfulness and mind-body interventions ............................................................................... 9
3.4. Psychoeducation and psychological interventions................................................................ 10
3.5. Web-based interventions ...................................................................................................... 11
3.6. Couples or family interventions ............................................................................................. 11
3.7. Social support........................................................................................................................ 12
3.8. Father’s mental health........................................................................................................... 12
3.9. Mixed intervention studies..................................................................................................... 13
3.10. Screening and referral........................................................................................................... 13
4. Interventions to promote wellbeing and/or prevent mental health conditions among
children and adolescents.............................................................................................. 14
4.1. Parenting programs ............................................................................................................... 14
4.2. Preschool-based programs ................................................................................................... 16
4.3. School based programs ........................................................................................................ 16
4.4. Programs in mixed settings ................................................................................................... 23
4.5. Primary care .......................................................................................................................... 25
5. Interventions to tackle risk factors. ............................................................................... 26
5.1. Adverse Childhood Experiences ........................................................................................... 26
5.2. Intimate partner violence ....................................................................................................... 30
5.3. Children of parents with a mental illness .............................................................................. 31
5.4. Bullying .................................................................................................................................. 32
6. Low intensity interventions for children and adolescents.............................................. 34
6.1. What are low intensity interventions? ................................................................................... 34
6.2. Exercise................................................................................................................................. 34
6.3. Self-help parenting programs ................................................................................................ 34
6.4. Supported playgroups. .......................................................................................................... 35
6.5. Telephone interventions ........................................................................................................ 35
6.6. Technology based interventions ........................................................................................... 36
6.7. Therapist-guided parenting programs. .................................................................................. 37
6.8. Therapist led parenting programs. ........................................................................................ 38
7. Interventions for priority populations ............................................................................ 40
7.1. Aboriginal and Torres Strait Islander children ....................................................................... 40
7.2. Children and adolescents who identify as LGBTIQ .............................................................. 43
7.3. Children from Culturally and Linguistically Diverse backgrounds ......................................... 43
7.4. Children living in rural and remote areas. ............................................................................. 44
8. Summary ...................................................................................................................... 45
9. Policy implications ........................................................................................................ 47
Appendix 1: List of evidence-based wellbeing and prevention programs .................................... 50
References .................................................................................................................................. 56What works to support the mental health and wellbeing of children aged 0-12?
Executive Summary
Good mental health and wellbeing is a positive asset for life. High levels of emotional and social
wellbeing enable children and adolescents to develop a strong sense of self, forge positive
relationships with others, engage effectively in education, become involved in their community, and
achieve their full potential. By contrast, mental health difficulties cause distress, disrupt
relationships, interfere with study and vocational attainment, and increase the risk of poor physical
and mental health in youth and adulthood.
It is therefore vital that governments implement programs and services to promote and protect the
mental health and wellbeing of children and adolescents and respond effectively to children and
young people who experience mental health challenges, while ensuring their parents and carers are
also supported. Within this context, the Mental Health Commission of New South Wales
commissioned Prevention United to undertake a literature review to examine what is known about
the mental health and wellbeing of children aged 0 – 12 years, and how we can enhance the
programs and services that are available to them, and their carers. The literature review aims to
answer two main questions:
• “What interventions have been shown to promote the social, emotional and mental wellbeing of
children aged 0-12 or prevent emotional and behavioural problems, and mental health
conditions in this age group?”
• “What non-clinical, self or parent-management or other low-intensity interventions can enable
children aged 0-12 with mild mental health difficulties to experience recovery from these
difficulties?”
The literature review examines peer-reviewed systematic reviews, meta-analyses and reviews of
reviews on wellbeing and prevention, and supplements these with peer-reviewed articles on low
intensity treatments in childhood where the research is just starting to emerge.
In relation to the first question, the literature review found that while no wellbeing or prevention
program works for every child, every time, it is nevertheless clear that child mental wellbeing can be
enhanced, and a sizeable proportion of common mental health conditions can be prevented from
occurring through evidence-based initiatives implemented at scale.
In terms of ‘what works’, the literature review shows that various parenting programs can support
parents to help their children to thrive. While results vary from program to program, there is good
evidence that structured skills-building programs delivered face-to-face or online are effective in
enhancing parenting skills, improving parental wellbeing, and preventing child internalising and
externalising disorders, and adolescent depression and anxiety. There is also good evidence that well
designed and delivered home visiting programs in the perinatal period and early childhood can
enhance parenting and reduce child maltreatment.
The literature review suggests that it is also possible to promote healthy child development in
education settings. Indeed, there is strong evidence from numerous systematic reviews and meta-
analyses that classroom-based, social and emotional learning (SEL) programs, resilience-building
programs, and disorder specific prevention programs are effective at promoting children’s mental
wellbeing and reducing their likelihood of experiencing an emotional and behavioural disorder in
childhood and anxiety and depression in adolescence. These programs typically draw on strategies
derived from clinical and positive psychology, such as cognitive behaviour therapy (CBT),
interpersonal therapy (IPT) and mindfulness.
iWhat works to support the mental health and wellbeing of children aged 0-12?
There is also very good evidence that anti-bullying programs in schools can prevent bullying, and this
is likely to have flow-on benefits in reducing the risk of depression and anxiety disorders among
children and adolescents, as well as later in life. In addition, there is some evidence that whole-of-
school mental health promotion programs can promote student mental wellbeing and prevent
mental health conditions, although this approach is unlikely to work unless classroom-based
psychological skills-building programs, and anti-bullying program are included in the suite of
strategies.
There is also very clear evidence to show that parental mental wellbeing in the perinatal period can
have a major impact on children’s mental health and wellbeing, and it is therefore vital to support
parents’ own mental health during pregnancy and the postpartum period. The literature review
suggests that certain strategies can help to promote parental wellbeing and avert perinatal
depression including regular physical activity, some mindfulness programs, and CBT- and IPT-based
psychological interventions delivered one-to-one, in groups or potentially online during the ante-
natal or post-natal period. Screening and referral for perinatal anxiety and depression can also
improve parent and child mental health outcomes.
Disappointingly, there is limited evidence around what works to promote the mental health and
wellbeing of children and adolescents from Aboriginal and Torres Strait Islander communities,
lesbian, gay, bisexual, transgender, intersex or queer/questioning (LGBTIQ) young people, and
children and adolescents from Culturally and Linguistically Diverse and rural and remote
communities. While many programs have been trialled, few have been rigorously evaluated.
Another major concern is the relatively limited research into ways to prevent key risk factors that
impact child and adolescent mental health from occurring. In particular, despite the considerable
negative impact that adverse childhood experiences (ACEs), such as child maltreatment and
exposure to domestic violence, have on children’s mental health and wellbeing, the evidence around
what works to stop ACEs from occurring is relative sparse. As noted, (nurse) home visiting programs
hold significant promise in preventing child abuse and neglect, but program design and quality of
implementation are crucial to success. Certain structured parenting skills-building programs, like
Triple-P, also show great potential. Structured parenting programs are also effective in reducing the
risk of childhood mental health difficulties among children who have a parent with a mental illness.
Currently, there is limited evidence on how to effectively prevent domestic violence from occurring
although the evidence base is slowly building around education programs to promote respectful
relationships and initiatives that aim to shift attitudes around gender equality.
In terms of what works in relation to low intensity interventions (LIIs) for emotional and behavioural
disorders (internalising and externalising disorders), the literature review found that the evidence
for LIIs in the child mental health field is not very extensive as this is a relatively new area of interest.
Despite this, there is emerging evidence that self-help information resources, telephone support,
online programs, and therapist-guided parenting programs are effective in supporting children with
mild-moderate mental health difficulties. These interventions are particularly useful for
oppositional-defiant disorder, conduct disorders and anxiety disorders in children. There is also good
evidence that therapist-led, group-based parenting programs can also be used to treat these
difficulties, thereby reducing the need for more intensive one-to-one therapy.
As in the adult realm, it is critical that child LIIs are provided within a model of stepped care so that
children who fail to respond well to these first-line efforts can be linked seamlessly to existing
primary care and specialist mental health service to receive a higher level of therapeutic support.
iiWhat works to support the mental health and wellbeing of children aged 0-12?
When considering the policy implications of this literature review, it is important to recognise that
the risk of mental ill-health starts from conception, in the form of genetic predisposition and other
biological vulnerabilities and accumulates over childhood and adolescence. Childhood and
adolescence is the prime time for promotion and prevention activities to occur given that 50% of
lifetime mental health conditions commence before age 14 years, and 75% of conditions have their
onset before age 25. Programs and services for children and adolescents need to be equipped to
respond to this epidemiological reality.
It is also important to remember that a child’s mental health and wellbeing is influenced by multiple
biopsychosocial factors in the environments in which children are born, grow, learn and live, and
these factors vary by age and stage of development. It is therefore vital to take a developmental,
ecosystems approach and embed responses in the various social environments around children –
their home, early learning service, school, sports and recreational club, neighbourhood and local
community. Efforts to improve child mental health therefore need to go well beyond the mental
healthcare sector, and a whole-of-government, cross-sectoral approach is critical.
The timing of wellbeing and prevention initiatives is also important. Most wellbeing and prevention
programs are designed for certain age groups or to prevent certain conditions at particular ages. It is
important to ensure the right program is available at the right time. Furthermore, while many
individual skills-building programs achieve positive results, these benefits can gradually wane over
time, and regular boosters are needed to reinforce these skills, and ensure they become
consolidated in a child’s day-to-day approach to life. This requires ‘intervention scheduling’.
For example, universal perinatal exercise and CBT- or IPT-based skills building programs for parents
could be followed by home nurse visiting parenting programs through to pre-school, particularly for
parents with additional needs. These could then be followed by universal access to structured
parenting programs for the prevention and/or management of emotional and behavioural disorders
targeting parents of children in primary school. Next, all schools should offer social and emotional
learning (SEL) and resilience building programs at regular intervals over the child’s primary school
years. Secondary schools could then provide anxiety, depression and alcohol and other drug (AOD)
disorder specific prevention programs for secondary school students. They could also offer parenting
programs that prevent adolescent depression and anxiety. This sequenced approach, could also help
to identify children and adolescents who seem to be vulnerable to mental health difficulties, or who
are already experiencing them. This would then enable fast-tracking into low intensity interventions.
Another issue that policy makers need to recognise it is that not all wellbeing, prevention and LII
programs work equally well. It is therefore important to select and commission programs with the
strongest and most consistent evidence of benefit, while noting that investment in further research
is critical to creating new and better interventions, particularly those to prevent ACEs. The
prevention of ACEs, in particular child abuse and neglect, would prevent around 38% of childhood-
onset and 32% of adolescence-onset mental health conditions, and a similar proportion of adult
disorders.
The quality of program implementation is also important. What works in experimental conditions
does not always work in the real world, unless the same attention to program fidelity and
implementation quality occurs. At present, this is difficult, as many interventions – particularly those
in education settings – rely on personnel that may not have any specific training in mental health.
Efforts are needed to ensure that non-mental health professionals receive appropriate training,
supervision and support to implement programs effectively. Alternatively, we need to develop a
skilled, mental health promotion workforce to take on this responsibility.
iiiWhat works to support the mental health and wellbeing of children aged 0-12?
Last, it is clear that the key to success in child mental health is to work with the pivotal adults in a
child’s life, particularly their parents/caregivers and educators. These individuals need to be
equipped with the knowledge and skills required to support healthy child social and emotional
development, teach children the psychological skills that will enable them to work through the
inevitable challenges of life, and play a role in managing emerging difficulties effectively. While
parents and educators should not be expected to replace therapists when children experience
significant mental health difficulties, they can make an enormous contribution to promotion,
prevention and early intervention efforts if given the skills and support to play this role.
Ultimately, by investing time, effort and resources into expanding and enhancing upstream
wellbeing, prevention and low intensity interventions governments will be able to better promote
child mental health and reduce demand on very stretched child, youth and even adult specialist
mental health services over time.
Investment is also required to develop new and better programs to promote mental wellbeing,
prevent mental health conditions and support children and adolescents who experience mental
health difficulties through low intensity interventions. Particular attention needs to be given to
undertaking more robust research into what works for Aboriginal and Torres Strait Islander children,
LGBTIQ young people, and children and adolescents from culturally and linguistically diverse (CALD)
backgrounds and rural and remote communities. Research into the primary prevention of adverse
childhood experiences should also be an urgent priority.
ivWhat works to support the mental health and wellbeing of children aged 0-12?
1. Introduction
Child and adolescent mental health is a major focus of government action, and as our understanding
of the mental health and wellbeing needs of children and adolescent has increased, so too have our
responses to the needs of children aged 0-12 years, and their parents and carers.
Over the last year we have seen the Commonwealth Government’s commit to developing a National
Children’s Mental Health and Wellbeing Strategy, and its recent Budget announcements include
funding to establish child mental health and wellbeing hubs to provide multidisciplinary care and
preventive services to this cohort, and for parenting education and support to parents and carers
with children aged under 12 years, among other initiatives. Increased focus on child and adolescent
mental health is also reflected in the NSW Government’s recent funding commitment of $109.5
million over four years to enhance community child and youth mental health services and create 25
Safeguards Child and Adolescent Mental Health Response Teams across NSW to provide services to
children and teenagers with significant mental health issues, and their families and carers.
It is therefore timely to take stock and examine what we know about the mental health and
wellbeing of children aged 0 – 12 years, and where the opportunities are for continuing to enhance
the programs and services that are available to them and their parents. Within this context, the
Mental Health Commission of New South Wales has commissioned Prevention United to undertake
a literature review relating to certain aspects of child and adolescent mental health.
The review is set against a backdrop of rising demand for children’s mental health services, and
increases in wait times in some areas, leading to a need to either prevent mental health difficulties
from occurring, supporting parents to manage these emotional and behavioural problems without
the need for specialist support, or offering them effective support while they are waiting for any
necessary services. The purpose of this literature review is to therefore to answer two key questions:
• “What interventions have been shown to promote the social, emotional and mental wellbeing of
children aged 0-12 or prevent emotional and behavioural problems, and mental health
conditions in this age group?”
• “What non-clinical, self/parent-management or other low-intensity interventions can enable
children 0-12 with mild mental health difficulties to experience recovery from these difficulties?”
The literature review examines peer-reviewed systematic reviews, meta-analyses and reviews of
reviews, and supplements these with some additional peer-reviewed primary research articles and
grey literature. We limited our searches to the period 1 January 2010 to May 2021 and to English-
language articles.
Its focus is on interventions designed to promote wellbeing, prevent ‘common’ high-prevalence
conditions or manage them through low intensity treatments. It does not focus on mental health
awareness programs to promote mental health literacy, reduce stigma, or promote help seeking, nor
does it review research into suicide prevention. It also does not focus on neurodevelopmental
conditions such as autism spectrum disorders, or low prevalence conditions such as eating disorders,
bipolar disorder or schizophrenia, or on clinical treatment provided through mainstream primary,
secondary and tertiary treatment services.
The literature review does not purport to be a systematic review of the literature or of systematic
reviews and meta-analyses. Rather it is narrative review, that seeks to examine as much evidence as
possible, to guide the policy, and program and service development in this important area of mental
health. The table at Appendix 1 provides a brief summary of the findings using a star rating system
that represents the extent of positive findings relating to various categories of interventions.
1What works to support the mental health and wellbeing of children aged 0-12?
2. Understanding child and adolescent mental health and wellbeing
2.1. Key concepts
2.1.1. Wellbeing
There are important differences in the terms used in the area of child and adolescent mental health
compared to those used in the youth, adult and older adult spheres. One example of this difference
relates to the concept of mental wellbeing. In the adult field, ‘good’ mental health (aka mental
wellbeing) has been defined as “a state of well-being in which an individual realizes his or her own
abilities, can cope with the normal stresses of life, can work productively and is able to make a
contribution to his or her community”. It is about feeling good emotionally and functioning well
psychologically and socially, and having direction and purpose in life. Scales to measure adult mental
wellbeing include questions about the balance of positive and negative emotions, psychological
functioning, interpersonal relationships, contribution to society and sense of meaning in life. (1-4)
By contrast, there no agreed definition of ‘good’ mental health in child and adolescent mental
health, and the term mental wellbeing is less commonly used and instead terms like thriving, or
positive behavioural, social and emotional development tend to be used. Emerging Minds states that
mental health is a child’s capacity to meet challenges, express a range of emotions in response to
experiences, regulate those emotions, explore their environment, and form secure relationships,
within the context of their developmental stage and their age. (5) Similarly, a toolkit developed by
the Frameworks Institute on behalf of Emerging Minds states that “Child mental health is more than
the absence of mental illness. It is a positive state of wellbeing; the result of a complex set of
influences, including environments and social conditions and the culture and public policies that
shape them.” (6) Every child and adolescent experiences a ‘level of mental health’ and it is important
to promote the mental wellbeing of all children, whether or not they are experiencing mental health
difficulties.
2.1.2. Mental ill-health
Another difference is the terminology used for mental ill-health. Within the child and adolescent
mental health field, the term mental health difficulties, emotional and behavioural disorders or
internalising and externalising conditions, are more commonly used than terms like mental health
conditions, mental disorders and mental illnesses. In addition, within a therapeutic context,
clinicians often prefer to focus on a biopsychosocial formulation of a child or adolescent’s difficulties
rather than using diagnostic terms.
Nevertheless, manuals like the International Classification of Disease or the Diagnostic and Statistical
Manual contain a list of child and adolescent related mental health conditions, such as depression,
specific phobia, separation anxiety, social phobia, generalised anxiety, oppositional defiant disorder
and conduct disorder, and it is crucial to note that many of these conditions can occur at a very early
age. (7) Overall, it is estimated that 50% of lifetime mental health conditions commence by age 14,
and 75% by age 24. (8)
2.1.3. The mental health continuum
This distinction between mental wellbeing and mental ill-health and their inter-relationship is
complex. In adult mental health two different models have been proposed to explain the connection
– the single continuum model and the dual continua model. The former proposes that mental
wellbeing and mental health conditions lie at opposite ends of a single continuum, while the latter
proposes that mental wellbeing and mental health conditions exist on two separate but correlated
continua. This model proposes that mental wellbeing can vary from high to low, and mental health
conditions can vary from absent to severe, and at any given point in time individuals can therefore
experience varying levels of mental wellbeing as well as varying symptoms of a mental health
condition. (9)
2What works to support the mental health and wellbeing of children aged 0-12?
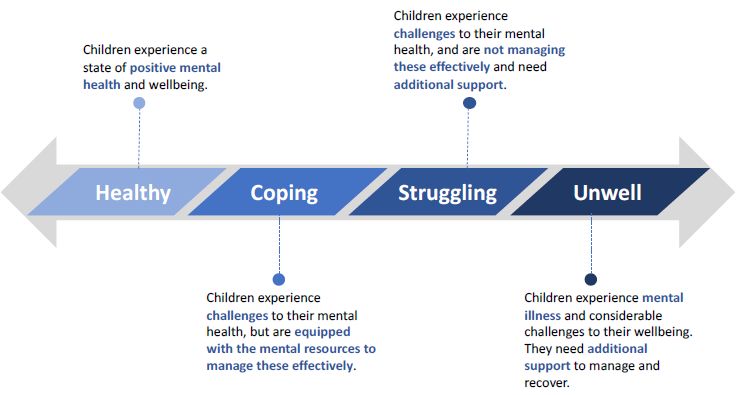
There has been far less research into the dual continuum model in child mental health and while
there is some evidence to support this model (10), the single continuum model is commonly used
and has been adopted in the Draft National Children’s Mental Health Strategy as shown in Figure 1
below.
Figure 1: The single continuum model of child mental health. Source: Draft National Children’s Mental Health Strategy
available at https://www.mentalhealthcommission.gov.au/Mental-health-Reform/Childrens-Mental-Health-and-
Wellbeing-Strategy
2.2. Prevalence of mental wellbeing and mental ill-health
While there are limited data on the prevalence of ‘good’ mental health among children and
adolescents, in large part due to the lack of agreement on how best to define and measure thriving
among children (11), a study by Goldfeld et al undertaken in 2017 provides some information. Using
data from the 2012 Australian Early Development Census the researchers found that 25% of children
experienced ‘optimal’ mental health and wellbeing as defined by high competence and low
difficulties, with the remainder experiencing varying levels of sub-optimal mental health and
wellbeing. This included 26% of children who had low competence and high difficulties. (10-12)
By contrast, the Australian Child and Adolescent Survey of Mental Health and Wellbeing provides a
very accurate picture of the prevalence of mental ill-health among children and young people in
Australia. Based on the findings from the most recent survey in 2015, in a given year it is likely that 1
in 7 children aged 4-11 years (13.6%), and a similar proportion of adolescents (14.4%) aged 12-17
will experience a mental health condition. Boys aged 4–11 years are more likely to experience
difficulties than girls of the same age (16.5% versus 10.6%). The most common conditions among 4–
11-year-olds include AHDH (8.2% of children), anxiety conditions (6.9%), conduct disorder (2%) and
depression (1.1%). (13)
Mental ill-health can have a profound negative impact on multiple aspects of a child or adolescent’s
life, and that of their parents/carers, and other family members. The impacts on schooling are
considerable. Children and adolescents with a mental health condition tend to feel less engaged with
and connected to schooling, and miss more days from school compared to students without a
condition. On average, they also score lower than students with no condition in every NAPLAN
domain and year level. By year 9 students with a mental health condition are on average 1.5-2.8
years behind students with no condition. (14) Mental health conditions in childhood and
adolescence also impact negatively on school completion rates, and contribute to poorer training,
education and employment outcomes post-secondary school, and into adulthood. (15-17)
3What works to support the mental health and wellbeing of children aged 0-12?
Children and adolescents with mental health conditions are also more likely to engage in health risk
behaviours such as smoking, alcohol and illicit drug use, and are more likely to be in contact with law
enforcement agencies. Critically, individuals who experience mental health difficulties in childhood
and adolescence are at higher risk of experiencing mental disorders in adulthood particularly if their
conditions are not properly identified, and treated. (18)
2.3. Promotion, prevention and early intervention
The Institute of Medicine (IOM) define mental health promotion as interventions which aim to
“enhance individuals’ ability to achieve developmentally appropriate tasks (competence), and a
positive sense of self-esteem, mastery, wellbeing and social inclusion, and strengthen their ability to
cope with adversity”. (19, 20) Others use the term ‘promoting mental wellbeing’ as an alternative
phrase for this outcome, and use mental health promotion as an umbrella term for any ‘population’
mental health activity focused on wellbeing and prevention, or on building mental health literacy,
reducing stigma, and promoting help-seeking. (21)
The IOM then define prevention as efforts to “reduce the incidence, prevalence and severity of
mental health conditions” and described three types of prevention – universal prevention for
initiatives target the whole population regardless of risk; selective prevention for those that target
groups that are at higher-than-average risk of mental ill-health; and indicated prevention for
initiatives that target individuals with detectable but subclinical symptoms of a mental health
condition. (22) While there is some overlap between promotion and prevention, the difference is in
the intended outcome – promotion aims to enhance an individual's wellbeing regardless of illness
status, while prevention focuses on reducing the occurrence of new cases of a diagnosable mental
health condition.
The IOM uses the term early intervention for initiatives that target individuals who have a
diagnosable disorder but where the intervention occurs at an early stage or before the disorder
becomes severe. (19) While acknowledging there is some blurring of boundaries between indicated
prevention and early intervention, the IOM make a point of distinguishing between the two, stating
that prevention occurs prior to the onset of a disorder while early intervention occurs after the
onset.
2.4. Risk and protective factors
Mental health conditions are complex disorders that evolve over time moving from subthreshold
symptoms, to attenuated psychiatric syndromes, to first episode disorders and through to no further
difficulties or relapsing-remitting or persistent disorders. (23) These conditions arise from the
dynamic interplay of various risk and protective factors operating over the life course rather than
any single factor in isolation. (19)
The social ecology theory developed by Bronfenbrenner provides an excellent framework for
understanding these contributing factors. The model highlights that child and adolescent
development is influenced by the interplay of a range of intrinsic biological and psychological factors
unique to each child, and external factors in the home, school, neighbourhood and broader
community environments around them. The model places the child at the centre of an ever
widening circle of influences including those in the microsystem (family and friends), mesosystem
(school and local community) and macrosystem (social, economic and cultural factors) (see Figure 2).
(24)
4What works to support the mental health and wellbeing of children aged 0-12?
Chronosystem (influence of time)
Macrosystem
(broader social, cultural & economic
factors)
Mesosystem
(neighbourhood, school, workplace)
Microsystem
(Parents, family, peers)
Child or adolescent
Figure 2: Bronfenbrenner’s Social Ecology Model
Risk factors increase a person’s likelihood of experiencing a particular condition, while protective
factors lower the likelihood. There are numerous risk and protective factors for each mental health
condition, which vary by age and stage of development (see Table 1). While some factors are unique
to a particular condition, most factors are implicated in a variety of conditions. The timing and the
total number of risk factors that an individual experiences over their life, and the degree to which
they are offset by protective factors is important in determining whether a person experiences a
condition or not. (25)
Risk and protective factors vary in their prevalence. They also vary in the strength of their
association with mental health conditions with some, such as exposure to child maltreatment,
appearing to be more influential than others. (26) Risk and protective factors also vary in how
modifiable they are. For example, a person’s genetic profile cannot be readily altered, whereas the
nature of an individual’s family, school or work environment can be changed through appropriate
designed interventions.
In essence, population mental health activities that aim to promote mental wellbeing and prevent
mental health conditions work by trying to influence these underlying risk and protective factors
through a focus on individual behaviour change and by enhancing the home, school, work,
neighbourhood and community environments around people using strategies derived from health
promotion. These strategies include public education/awareness social marketing campaigns; skills-
building programs; community mobilisation initiatives; the creation of mentally healthy
5What works to support the mental health and wellbeing of children aged 0-12?
organisational environments; healthy public policies; and service system reorientation initiatives.
(27)
Table 1. Common risk and protective factors in childhood and adolescence
Protective factors Risk factors
• Easy temperament • Prematurity, low birth weight, birth complications
• Secure attachment • Inhibited temperament
• Adequate nutrition • Insecure and disorganised attachment
• Above-average intelligence • Poor health in infancy
• Optimism • Low self-esteem
• Resilience • Poor social skills
• Internal locus of control • Large family size
• Good emotion regulation • Poor supervision and monitoring of child
• Problem solving skills. • Lack of warmth and affection
• Social competence, social skills • Harsh or inconsistent discipline style
• Problem solving skills • Low parental involvement in child’s activities
• Parent warmth • Childhood neglect or physical, emotional and sexual
• Supportive caring parents abuse
• Family harmony • Marital discord in parents
• Small family size and more than two years • Divorce and family breakup, death of family
between siblings member
• Supportive relationship with another adult • Child exposure to family violence
• Strong family norms and morality • Teenage parents
• Prosocial peer influence • Parent with a severe mental illness, alcohol or other
• Positive school climate drug use difficulties or parental incarceration.
• Sense of school belonging • Parentification (child takes on parent role)
• Opportunities for some success and • Poor attachment to school
recognition of achievement • School transitions
• School norms against violence • Anti-social peer group
• Social support • Low social participation, less frequent social
• Attachment to and networks within the contact, loneliness and social isolation
community • Bullying and peer victimisation
• Strong cultural identity and ethnic pride • Racism
• Sense of connectedness • Perceived discrimination/racism
• Participation in community groups • Screen time based sedentary behaviour.
• Community/cultural norms against violence • Low physical activity
• Economic security • Low quality diet
• Alcohol use, smoking, cannabis use in adolescence
• Poor sleep hygiene
• Socioeconomic disadvantage
• Homelessness
• Neighbourhood violence and crime
• Lack of support services including transport,
shopping, recreational facilities
Source: Commonwealth of Australia (2000). Promotion, Prevention and Early Intervention for Mental Health. A
Monograph. (28)
2.5. Promotion, prevention and early intervention benefits
High levels of mental wellbeing are associated with better learning, increased creativity, greater
productivity, more pro-social behaviours and civic engagement, better quality relationships, greater
adoption of positive health behaviours, better physical health (including better immune, endocrine
and cardiovascular functioning), lower rates of mental health conditions, and longer life expectancy.
(2, 29-31) High levels of mental wellbeing are indeed a driver for these outcomes and not just a
6What works to support the mental health and wellbeing of children aged 0-12?
result of them. (31) These benefits contribute to improvements in productivity and to reductions in
costs (health and welfare). (32)
Prevention is also crucial. Mental health conditions are common, distressing, potentially disabling
and they are associated with an increased risk of death by suicide. Overall mental health and
substance misuse conditions account for 12% of the total burden of injury and disease in Australia.
(33) At a societal level, the Productivity Commission recently estimated that the direct economic
costs of mental ill health and suicide in Australia was $43–70 billion in 2018-19. In addition, the cost
of disability and premature death due to mental ill-health, suicide and self-inflicted injury is
equivalent to a further $151 billion.
While effective treatments are available for most conditions, there is still considerable merit
focusing on the prevention of mental health conditions. Over half of people who experience a
mental health condition will experience relapsing and remitting difficulties following their first
episode, and a significant minority will experience persistent and ongoing challenges despite the
best available supports and services. Preventing these conditions from occurring can reduce the
emotional strain, avert the risk of disability, save money and save lives.
7What works to support the mental health and wellbeing of children aged 0-12?
3. Interventions for perinatal mental health.
A parent’s own mental health can have a significant influence on their child’s wellbeing, particularly
during the perinatal period. While estimates vary, up to one in ten women experience depression
while pregnant, and one in seven women in the year after birth. Men can also experience perinatal
mental health conditions, with approximately one in ten expectant and new fathers experiencing
depression, anxiety or other forms of emotional distress in the perinatal period. (34) A range of
factors are known to contribute to the development of these conditions. These include sleep
problems, lack of social support, not living with a partner, intimate partner violence, multiple births,
alcohol, cigarette, and substance use and a past history of mental health conditions. (35, 36)
Perinatal depression and anxiety are not only problematic for the parent and their partner, but they
are associated with an increased risk of emotional and behavioural disorders among their offspring.
They are also linked to more negative affect/behaviour, lower levels of positive affect/behaviour,
and poorer cognitive, language, motor, and adaptive behaviour development among children who
have a parent with a perinatal mental health condition. (37-39) In addition, these conditions also
increase the risk of child maltreatment. (40) Improving parental mental health through primary
prevention strategies or early intervention for perinatal conditions can therefore help to avert child
and adolescent mental health conditions.
3.1. Health behaviours.
3.1.1. Exercise
A systematic review by Nakamura et al of experimental and observational studies examining the link
between exercise and perinatal mental health, found that women who were physically active during
pregnancy experienced a lower incidence of postnatal depression relative to those who were not.
(41)
Other reviews have focused on experimental trials. For example, Daley et al (2015) conducted a
systematic review and meta-analysis of RCTs that examined the effectiveness of exercise in the
prevention and treatment of antenatal depression. Six trials were included in their analysis and these
showed a significant reduction in depression scores for exercise interventions relative to comparator
groups, although it is important to note the majority of trials included women who were already
experiencing some depressive symptoms. (42)
A later systematic review and meta-analysis of intervention studies (RCTs and non-RCTs) conducted
by Poyatos-León et al in 2017 found that women who participated in exercise interventions during
pregnancy or the postpartum period experienced significantly lower postnatal depressive symptoms
compared to women in the control groups. While the effect size was larger for women who were
already experiencing symptoms at baseline, women with no baseline depressive symptoms also
experienced significantly lower symptoms post-partum compared to women in control conditions.
(43)
A systematic review and meta-analysis published by Carter et al in 2019 also examined the impact of
exercise on postnatal depression. This review included both universal and targeted prevention
interventions (selective and indicated) as well as treatment interventions. Their meta-analysis of 18
RCTs found exercise/physical activity interventions led to a moderately significant reduction in
depressive symptoms compared to control conditions. Targeted prevention and treatment
interventions yielded a greater effect size than universal prevention interventions although universal
prevention interventions did lead to statistically significant reductions in depressive symptoms. The
authors noted that the quality of evidence was fairly low across the individual studies. (44)
8What works to support the mental health and wellbeing of children aged 0-12?
A more recent systematic review of 16 RCTs by Kołomańska-Bogucka and Mazur-Bialy published in
2019 also found that interventions that aimed to promote regular physical activity during pregnancy
or the postnatal period reduced depressive symptoms as well as the risk of developing postnatal
depression when compared to inactivity. (45)
Davenport et al’s 2018 systematic review of prenatal exercise on prenatal and postnatal anxiety and
depressive symptoms reported somewhat different findings. As in other studies, their review of 52
trials (26 RCTs, 7 non-randomised trials, 10 cohort, 6 cross-sectional and 3 case control studies)
found that exercise-only interventions, but not exercise plus co-interventions, reduced the severity
of prenatal depressive symptoms (13 RCTs) and the odds of prenatal depression by 67% (5 RCTs)
compared with no exercise. However, in contrast to other reviews they found that prenatal exercise
did not alter the odds of postpartum depression or the severity of depressive symptoms, nor anxiety
symptoms or disorders during or following pregnancy. However, as noted, this review included a far
broader range of research designs. (46)
3.1.2. Sleep
Poor sleep quality is associated with an increased risk of perinatal mood disturbances. (47) As result,
researchers have examined the potential benefits of assisting parents to manage their child’s
sleeping patterns. A 2013 systematic review by Douglas et al concluded that behavioural
interventions in the first 6 months do not decrease infant crying, prevent sleep and behavioural
problems in later childhood, or protect against postnatal depression. (48) A later systematic review
by Sasaki et al (2021) found two studies that focused on universal preventative interventions
provided during pregnancy to improve infant and maternal sleep hygiene. One study found no
significant difference in the incidence of postnatal depression while the other found a significant
difference. (49)
3.2. Self-help programs
Lin et al conducted a meta-analysis of self-help interventions (e.g. books, videos, websites) designed
to prevent or treat postpartum depression. The analysis included nine RCTs and found that there
was no significant difference between self-help interventions and control conditions in preventing
depression. However, self-help interventions were significantly more effective, relative to control
conditions in promoting recovery from postpartum depression post-intervention and at follow-up.
(50)
3.3. Mindfulness and mind-body interventions
Mindfulness can be defined as “the intentional and non-judgemental awareness of experience in the
present moment. This is characterised by an openness to and acceptance of all internal and external
stimuli, and an ability to switch awareness between stimuli.” (51)
Lever-Taylor et al (2016) conducted a systematic review and meta-analysis of the effectiveness of
mindfulness-based interventions for reducing depression, anxiety and stress in the perinatal period.
The review identified 17 studies of mindfulness-based interventions, including both controlled trials
and pre-post uncontrolled studies of mindfulness based cognitive therapy and mindfulness-based
stress reduction. The majority of studies were carried out in the prenatal period and included a mix
of studies that focused on improving wellbeing, reducing general distress or stress, or on selective
prevention or indicated prevention. While the analysis of pre-post-intervention results from the
uncontrolled studies showed significant reductions in depression, anxiety and stress, each with small
to medium effect sizes, the analysis of the eight studies that used a more robust controlled design
failed to find any significant post-intervention benefits for depression, anxiety or stress of
mindfulness-based interventions in comparison to control groups. (52)
9What works to support the mental health and wellbeing of children aged 0-12?
Matvienko-Sikar et al (2016) also conducted a systematic review and meta-analysis of studies
examining whether mindfulness-based interventions were able to reduce levels of depression,
anxiety and negative affect during pregnancy. The meta-analysis included eight RCTs and found that
mindfulness interventions led to reduced levels of depression, anxiety and negative affect during
pregnancy among women in the intervention groups compared to the control groups, but not in
reducing stress or increasing positive affect. However, it is important to note only some of the
studies examined the preventive benefits of mindfulness rather than its benefits for women already
experiencing depression or anxiety. The authors concluded that mindfulness interventions may
improve prenatal wellbeing, but the quality of existing studies is variable and further higher quality
research is needed to better understand intervention effects. (51)
Marc et al undertook an analysis of studies that used a broader range of mind-body interventions to
reduce perinatal anxiety. The review included eight RCTs of mind-body interventions such as
autogenic training, biofeedback, hypnotherapy, imagery, meditation, prayer, auto-suggestion, tai-chi
and yoga targeting pregnant women of any age at any time from conception to one month after
birth. The results were quite variable and overall the authors concluded that there is limited
evidence for the effectiveness of mind-body interventions for the management of anxiety during
pregnancy. (53)
A later systematic review and meta-analysis by Guo et al published in 2021, also examined a range of
mind–body interventions including mindfulness, relaxation techniques and yoga groups. The meta-
analysis of 28 studies involving 1,944 participants found that such interventions led to significant
improvements in stress levels among women in the intervention groups compared with the control
groups. Both individual and group-based formats were effective, and 4–8 weeks of intervention
seemed the optimal choice. While significant differences in anxiety and depressive symptoms were
also noted between the intervention and control groups, the analysis did not specifically examine
whether the interventions prevented perinatal mental health conditions. (54)
3.4. Psychoeducation and psychological interventions
There has been considerable research into the preventive effects of psychoeducation and
psychological interventions during and/or after pregnancy. Two main psychological interventions
have been studied – CBT and IPT. CBT teaches people how to use the natural relationship between
thoughts, behaviours and mood to manage negative thoughts and create positive actions, while IPT
helps people to communicate better with others and focuses on addressing interpersonal issues that
contribute to depression or anxiety. These strategies can be taught through individual or group
settings by a range of professionals, paraprofessionals or even online. (55)
Fontein-Kuipers at al conducted a review of RCTs of antenatal interventions designed to reduce
perinatal stress, anxiety or depressive symptoms which they collectively referred to as maternal
distress. Data from ten trials with 3,167 participants (six preventive interventions and three
treatment trials) were included in the meta-analysis. The preventive interventions included
antenatal education, mentoring interventions, music therapy, and group antenatal care. Overall, the
review found no beneficial reduction of maternal distress in the intervention groups compared to
the control groups. However, the results of the subgroup analysis from three trials in which
participants were selected on the basis of increased risk of maternal distress showed a small
significant effect, while the treatment interventions also showed a significant effect for the
reduction of maternal distress. The authors concluded that while preventive antenatal interventions
for maternal distress show no effect, interventions for women at risk or those already experiencing
maternal distress were associated with a small but significant reduction in distress. (56)
The systematic review by Bright et al (2020) looked more specifically at perinatal anxiety. This review
found that only one of seven prevention studies which investigated the use of IPT to prevent
10What works to support the mental health and wellbeing of children aged 0-12?
perinatal anxiety reported a significant reduction in the risk level of anxiety symptoms. Another
systematic review by Matvienko-Sikar et al (2021) found that there was inconsistent evidence
around psychological interventions to prevent stress and anxiety among women in the antenatal
period and first 1,000 days of their child’s life. (57) However, another review by Missler et al (2021)
did find that psychological interventions such as psychoeducation CBT, IPT and mindfulness
implemented during pregnancy on a universal basis, can led to a decrease in stress and anxiety post-
partum although the effect on anxiety was smaller than on depression. (58)
Trials that have focused on the prevention of perinatal depression appear more promising. For
example, a systematic review by Sockol in 2015 found that CBT was effective in the prevention of
perinatal depression, as well as its treatment. The author found that interventions initiated during
the postpartum period were more effective than antenatal interventions, and individual therapy was
more effective than group interventions. Preventive effects were noted across universal, selective
and indicated prevention studies. (59) In another systematic review, Sockol found that IPT was also
effective in reducing depressive symptoms and the incidence of depressive episodes during the
antenatal and postnatal period when used on either a universal, selective or indicated prevention
basis. (60)
Yasumaa et al (2020) examined the impact of psychological interventions for the prevention of
perinatal depression and also found a significant positive effect of antenatal psychological
intervention on both antenatal and postnatal depression when provided on a universal prevention
basis, while Missler et al also found that the universal provision of psychoeducation CBT, IPT and
mindfulness during pregnancy led to a decrease in depression and stress, but the effect on anxiety
was smaller. (58) (61)
The benefits of psychoeducation, CBT, IPT, peer mentoring or other supportive interventions during
pregnancy or in the postpartum period were also noted in a systematic review of 50 studies by
O’Connor et al. Their review found such interventions were associated with a lower likelihood of
perinatal depression onset in the intervention groups compared to control groups (31.8% greater
reduction), although the evidence was mostly for women at increased risk for perinatal depression.
(62) It is worth noting that based on this review the U.S. Preventive Services Task Force concluded
with moderate certainty that counselling interventions to prevent perinatal depression have a
moderate net benefit for pregnant or postpartum women at increased risk. This include women with
a history of depression, socioeconomic disadvantage (e.g., low income or young or single
parenthood) or have current depressive symptoms. (63)
3.5. Web-based interventions
Online approaches for the prevention of perinatal mental health conditions also be studied. Lee et al
conducted a systematic review of web-based interventions for prevention and treatment of
perinatal mood disorders. Four studies met their inclusion criteria including three RCTs and one
feasibility trial. All studies included a therapist/external contact in addition to a web-based
component although the extent of external support was variable. The review found that women in
the intervention groups experienced fewer depressive symptoms post-intervention and at follow-up,
however the review did not include tests of significance between intervention and control groups.
The authors concluded that there was emerging evidence that web-based therapies for perinatal
depression delivered in the post-partum period may play a role in improving maternal mood but
more studies are needed. (64)
3.6. Couples or family interventions
Interpersonal difficulties such as poor division of responsibilities, a lack of partner availability or
support, low intimacy, and conflict or dissatisfaction between partners has been implicated in the
11You can also read