Is There Magic in These Mushrooms?' Discussing Current Psychiatric Treatment Options, and the Potential of Psilocybin Mushrooms in the Future of ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Chapter 11
‘Is There Magic in These Mushrooms?’ Discussing
Current Psychiatric Treatment Options, and the Potential
of Psilocybin Mushrooms in the Future of Such
Treatments
Sasha Faichuk
“The psychedelics are a red-hot social issue, ethical issue, whatever the term for
it is, and it is precisely because they are a deconditioning agent: they will cast
doubt in you if you are a Hasidic rabbi, a Marxist anthropologist, or an altar boy,
because their business is to dissolve belief systems, and they do this very well and
then they leave you with the raw datum of experience.” (Terence McKenna,
Psychedelic Society Speech, 1984)
Psilocybin mushrooms, commonly referred to as “Magic Mushrooms,” are the
various species of fungi that cause hallucinogenic effects. Daniel & Haberman
(2017) indicate that there are over a hundred magic mushroom species worldwide
(e.g., Psilocybe cubensis, Stropharia coronilla, or Panaeolus subbalteatus), both
wild and cultivated, with varying potencies. Cultivated magic mushrooms are often
more potent because of the selection processes for strains with higher levels of
psilocybin (Daniel & Haberman, 2017). Psilocybin, which breaks down into
psilocin in the body, is the active ingredient in magic mushrooms that causes the
hallucinogenic effects. This hallucinogen has been used ritualistically in countries
like Mexico for thousands of years and is still commonly used today (Carod-Artal,
2015). In 1957, this hallucinogen became of interest in western science, and, in the
following years, psilocybin was isolated, identified and synthesized in a laboratory
(Hofmann et al., 1958). In the 1960s, psilocybin started to be researched for its
treatment potential for psychiatric illnesses (Tylš et al., 2014). In the meantime,
189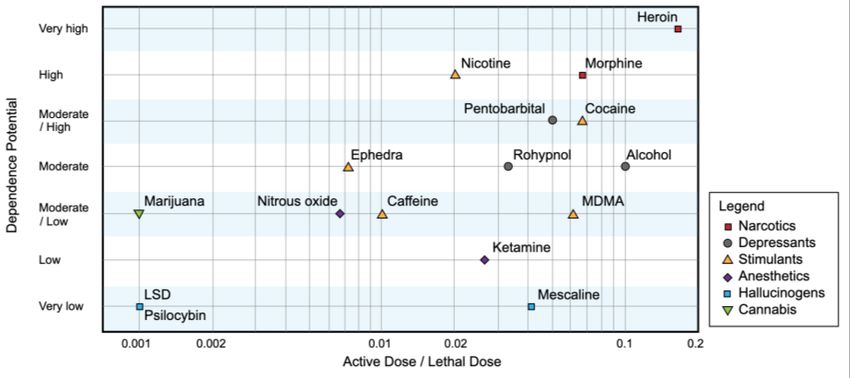
Are We There Yet? The Golden Standards of Forensic Science
however, political concern surrounding magic mushrooms grew as they became
popular recreationally amongst the general public (Belouin & Henningfield, 2018).
This concern eventually sparked the classification of psilocybin as a Schedule I
drug during the 1971 United Nations Psychotropic Convention (Nichols, 2004;
Sellers, 2017). This marked the end of not only the personal possession and use of
psilocybin, but also its presence in human experiments (Tylš et al., 2014). The
treatment potential of psilocybin was therefore never concretely outlined. A
Schedule I drug is one with high abuse potential or one without medical use.
Despite the classification, magic mushrooms have been shown to have medicinal
benefits, are non-toxic, and are not addictive (Griffiths et al., 2011). Recently, the
medicinal benefits of psilocybin have regained traction and interest in the scientific
community because of its potential in treating mental illness (Daniel & Haberman,
2017), pointing toward their use as a possible ‘gold standard’ in mental health
treatment.
Figure 11.1: Image of Psilocybin Mushrooms
Current Gold Standard in the Treatment of Mental Illness
Current mental illness treatments, with antidepressant medications like selective
serotonin reuptake inhibitors (SSRIs), aim to provide relief from the symptoms of
the disorder. Remission from a mental disorder is considered to be a near absence
190Is There Magic in These Mushrooms?
of these symptoms (Frank, 1991). A high risk of relapse, which is the return of the
disorder’s symptoms, remains upon remission. If remission persists for six months,
then the patient is deemed to be recovered. Nonetheless, individuals who have
recovered from depression by using antidepressants have a significantly elevated
risk of experiencing a new depressive episode (DeRubeis et al., 2008). Contrary to
their name, SSRI antidepressants are used to treat more than major depression
(Arroll et al., 2009; Blier & De Montigny, 1994). SSRIs are also prescribed for
anxiety (Bystritsky et al., 2013), anxiety disorders such as panic disorder,
obsessive-compulsive disorder (OCD), post-traumatic stress disorder (PTSD), and
social phobias (Zohar & Westenberg, 2000), as well as obsessive-compulsive
spectrum disorders (OCSDs)(Hollander, 1998), anorexia (Marvanova & Gramith,
2018), borderline personality disorder (Rinne et al, 2002), binge eating disorder,
bulimia (Capasso et al., 2009), and substance abuse (Knudsen et al., 2007), to name
a few. This solely biomedical approach to treatment is often criticized, as it only
addresses the symptoms of the illness instead of the potential cognitive and
psychological causes or components.
The aforementioned drug therapies do not come without their sets of side
effects. SSRIs are notorious for decreased libido, weight gain, insomnia, nausea,
and dizziness, which can interfere severely with one’s day-to-day life (Cascade et
al., 2009). Experiences of amotivation, detachment and emotional blunting are not
uncommon with these drugs and have been described as a “chemical lobotomy”
(Healy et al., 2006). Some of the most worrisome side effects of mental health
medications can include bouts of self-harm, worsened depression and suicidal
tendencies (Healy et al., 2006). The use of these medications could therefore have
lethal implications, effectively decreasing the public health standard and
threatening community wellbeing. Recent research has also demonstrated that
antidepressants may induce aggression and violence in a subset of individuals.
These findings imply that the justice system may face violent cases caused by
psychotropic drugs. As such, public safety and the legal system may both be
unnecessarily threatened or overwhelmed by the effects of the high antidepressant
prevalence in the community (Healy et al., 2006).
Additional treatments exist to alleviate the symptoms or processes behind
psychiatric disorders. The most notable would be cognitive behavioral therapy
(CBT) (DeRubeis et al., 2008). CBT is a tailored form of weekly or bi-weekly talk
therapy with the goal of treating mental illness and/or emotional, social, behavioral,
or cognitive problems (Dickerson & Lehman, 2006; Weissman et al., 2000). CBT
191Are We There Yet? The Golden Standards of Forensic Science
is based around the theory that false beliefs and maladaptive information processing
cause some psychiatric disorders. This model implies that rectifying these
maladaptive thoughts will lessen the risk of symptoms recurring (DeRubeis et al.,
2008). Psychiatric professionals believe that this type of talk therapy protects
patients against relapse and illness recurrence, as it addresses the psychological
cause of the disorder and teaches individuals with mental health issues coping
mechanisms that are applicable for their ailments (Hollon et al., 2002).
Compared to medication treatment alone, a combination treatment with
both CBT and antidepressant therapy has been associated with greater mental
health improvement rates (Pampallona et al., 2004) for the treatments of OCD,
major depression, and panic disorder (Cuijpers et al., 2014). Clinical psychology
seems to encourage an SSRI-CBT combination treatment method for a variety of
disorders because together they address the biological, cognitive and psychological
aspects of mental illness. Notably, however, most Canadians being treated with a
mood disorder are only taking medication (47.6%), while only 27.3% have received
both medication and therapy (O’Donnell et al., 2017). In practice, talk therapy
needs are largely unmet, which results in inadequate healthcare for many. A major
reason for the lack of counselling is financial hardship and low access to relevant
health care (O’Donnell et al., 2017). In Canada, it is the provincial governments’
responsibilities to supply the public with proper access to healthcare (Bentivegna,
1998, p.107). Lack of adequate healthcare generates costs in a variety of sectors
such as the social, criminal justice, business, health, education, law enforcement,
and emergency sectors (Druss et al., 2008; Kessler et al., 1999, 2008; Merikangas
et al., 2007). The main costs are derived from criminal justice costs, loss of
earnings, medical costs, and accidents (Kazdin & Blase, 2011). CBT is expensive
and frequent visits are necessary for results. Moreover, SSRIs are not always
effective and have a long side-effect profile (Cipriani et al., 2018). Given these
realities, a combination approach to treatment may not be feasible for everyone.
Outlining Psilocybin Treatment
Psilocybin triggers perceptual changes, such as synesthesia, hallucinations and
illusions. It also alters one’s sense of time, attention and self-perception, and creates
feelings of depersonalization and derealization (Geyer & Vollenweider, 2008).
These effects may better the current treatment processes in clinical psychology
because they offer unparalleled experiences, outlooks, perceptions and benefits that
192Is There Magic in These Mushrooms?
may aid or serve as a new cutting-edge therapeutic tool. Psilocybin treatment can
either involve taking a full dose of psilocybin (with or without a therapy session)
or involve microdosing psilocybin.
Full-dose Psychedelic Psychotherapy and Full-dose Psychedelic Treatment
Full doses of psilocybin facilitate psychological insight and dissolve psychological
defences, which may increase one’s emotional responsiveness and catalyze their
reception to talk therapy treatment (Winkelman, 2014). This implies that an eclectic
approach to treatment, with a mix of talk therapy and psilocybin, may prove to be
extremely effective in the treatment of some mental illnesses. A combination
treatment should follow a drug-free therapy session, used to establish a foundation
and a sense of comfort between the patient and clinician. In full-dose psychedelic
psychotherapy, the dose of psilocybin remains low enough for the patient and
psychiatrist to discuss thoughts, feelings and experiences, but remains high enough
to perceive the hallucinogenic effects. Full doses promote the patient’s connections
with their traumatic memories, which is necessary for working through trauma. The
drug may also alleviate the fear associated with a stressor or traumatic event
(Winkelman, 2014), and decrease anxiety reactions, effectively reducing the body’s
stress response. A reduction in conditioned fear responses, anxiety-inducing
feelings and avoidance allows patients to trust their feelings and dissolve their
emotional blockages (Mithoefer, 2007). Researchers also suggest that
hallucinogens have the power to lead an individual in identifying problems and
their possible solutions, guided by the processes of the individual’s unconscious
mind (Grof, 2009). Psychedelic therapy is also known to create a deep sense of
unity, meaningfulness, and interconnectedness, ultimately giving patients a sense
of self-control and the opportunity to apply these insights to positive life
transformations (Winkelman, 2014). The key difference between the eclectic
approaches of combination SSRI and combination psilocybin treatments is that the
full-dose psilocybin treatments require fewer sessions (Carhart-Harris et al., 2017),
and have no long-term symptoms (Studerus et al., 2010), therefore posing less of a
strain on the patients and the healthcare system.
Although full-dose psychedelic psychotherapy is a feasible and beneficial
option, full-dose psychedelic treatment without therapy is also effective. This
treatment consists of the mere experience of the hallucinogenic effects. The
psychedelic experience has lasting positive effects on mental health, mood,
193Are We There Yet? The Golden Standards of Forensic Science
connection, sociability and attitude, all of which are discussed in the “Mental and
Social Benefits of Magic Mushrooms” section below. The guidance of clinicians,
however, which is a feature of the therapy treatment, may be crucial in minimizing
the drawbacks of this treatment, namely flashbacks, bad trips, recklessness and
psychosis. This will also be discussed in a following section of this chapter (see the
“Drawbacks of Magic Mushrooms” section below).
Microdosing
Microdosing involves the scheduled ingestion of a sub-perceptual dose of
psilocybin (5-10% of a full psychedelic dose) (Kuypers et al., 2019). Psilocybin
microdoses are either taken every day, or on an on-off schedule to prevent the
buildup of a tolerance to the drug. A drug tolerance is a reduced reaction to the drug
after its repeated use. If magic mushrooms are used more than once a week, the
benefits and hallucinogenic effects plummet, as the brain becomes temporarily
desensitized to the drug (Nicholas et al., 2006).
On paper, it appears that microdoses of psilocybin could provide similar
therapeutic results to full doses, while eliminating the drawbacks of high doses and
the clinical oversight required for full-dose treatments (Anderson et al., 2019). On
the other hand, microdosing does not bring forth the problem-solving capabilities
and insights that are present in full doses of psilocybin, as small doses do not
dissolve psychological defences and increase emotional responsiveness. Research
has yet to conclusively outline the efficacy of microdosing for the treatment of
psychiatric disorders. Recent small-scale studies, however, have demonstrated the
positive effects of microdosing psilocybin on cognitive processes (Kuypers, 2020),
mental health (Lea et al., 2020), mood, anxiety, extraversion, focus, and the
occasional reduction in trauma sensitivity and substance dependence (Anderson et
al., 2019). Another study reports that microdosing seems to alleviate the symptoms
of anxiety disorders and attention hyperdeficit disorder (ADHD), more so than
conventional treatment, but the therapeutic effects for general anxiety and
depression remain lower than those from full psilocybin doses (Hutten et al., 2019).
For some individuals, however, microdosing increased anxiety and hindered mood
(Anderson et al., 2019; Kuypers, 2020). Surprisingly, Szigeti et al. (2021) found
that well-being, life satisfaction, mindfulness, and paranoia improved greatly for
both the microdose and the placebo groups that they studied, with no significant
differences between the two. These results validate the psychological benefits of
194Is There Magic in These Mushrooms?
microdosing, while also suggesting that this enhancement is not rooted in the
pharmacological action of the microdoses, but by the placebo effect. Although
these are mostly positive results, the conclusions must not be treated as concrete
because of the uncertainty, conflicting results, small sample sizes and low number
of experiments. Further research must be conducted in order to build a foundation
upon which to base treatment plans.
The medical legalization of psilocybin brings up legal challenges in terms
of criminality and community safety. The association between mental illness and
violent crimes should not be ignored by the legal and justice systems (Marzuk,
1996). Regardless of treatment type, effective treatment of mental illness prevents
poverty, crime (Marzuk, 1996), homelessness, involuntary psychiatric hospital
admissions, and police contact (Detrick & Stiepock, 1992), and should thus be of
utmost importance to the legal system.
Mental and Social Benefits of Magic Mushrooms
Research has shown that psilocybin is effective at treating treatment-resistant
depression (Carhart-Harris et al., 2018; Goldberg et al., 2020; Johnson & Griffiths,
2017), and that the quality of the psychedelic experience is related to its treatment
efficacy (Roseman et al., 2018). Functional magnetic resonance images (fMRIs)
have uncovered positive post-treatment changes in the brain, even after a single
full-dose treatment session, that correlate with the decrease in depressive symptoms
(Carhart-Harris et al., 2017). Psilocybin has been shown to be a similarly effective
treatment for PTSD (Mithoefer, 2007), OCD (Moreno et al., 2006), alcohol
dependence (Bogenschutz et al., 2015), smoking cessation (Johnson et al., 2016)
and anxiety (Goldberg et al., 2020; Mithoefer et al., 2016; de Veen et al., 2016).
The breadth of the treatment efficacy makes psilocybin an effective treatment for
individuals with comorbid psychiatric disorders. It should be noted that genetic
factors, however, may moderate individual responses to psilocybin, and therefore
this mental health treatment may not be effective for everyone (Barrett et al., 2017).
Full-dose psilocybin treatments require a low number of sessions, but the
resulting effects last longer than other treatment options, including the non-
frontline treatments, such as ketamine infusions, electroconvulsive therapy, or
transcranial magnetic stimulation (Thomas et al., 2017). Additionally, in the long
term, psilocybin use did not indicate any association with an increased need for
195Are We There Yet? The Golden Standards of Forensic Science
mental health treatment (Johansen & Krebs, 2015), further supporting the social,
economic and health benefits of this drug therapy.
Research has found that magic mushrooms can treat feelings of distress
related to terminal cancer, such as overwhelming feelings of fear, despair and
existential anxiety (Grob et al., 2011, 2012). The spirituality effects of this drug
reach beyond conventional psychotherapy and promote the processing of such
feelings, thereby having powerful therapeutic effects and enhancing emotional
wellbeing (Winkelman, 2014). Griffiths et al. (2006; 2008) found that many
patients reported that their magic mushroom experience was one of their most
meaningful life experiences. Such satisfaction might improve treatment outcomes
and efficacy because patient buy-in to therapy and treatment is crucial for positive
results (Griffiths et al., 2006; 2008). Psilocybin has been shown to reach beyond
mental illness, as it is an effective treatment of cluster headaches. There is a moral
imperative to supply this treatment to those that need it, because these headaches
are virtually untreatable with current biomedicine and the afflicted are in dire need
of relief, as illustrated by this afflictions nickname: suicide headaches (Sewell et
al., 2006).
A major benefit to psilocybin treatment is that no association between its
lifetime use and increased suicidal thoughts, plans, or attempts appear to exist
(Johansen & Krebs, 2015). Research has demonstrated that suicidal thoughts and
degree of planning are lower in psilocybin users compared to non-users and those
who use it with other psychedelics (Hendricks et al., 2015), which highlights the
safety of this treatment for those with suicidal tendencies (Hendricks et al., 2015).
Lifetime use of psilocybin may serve as a protective factor, intervention method
and prophylactic in regard to suicidality and distress (Gable, 2004; Hendricks et
al., 2015). Therefore, unlike current SSRI treatments, this treatment does not have
lethal implications, which may raise the public health standard, promote
community wellbeing, decrease hospital workload and prevent premature
mortality.
Psilocybin mushrooms also trigger improvements in general well-being. At
both two and fourteen months post-treatment, patients not only reported much
higher ratings of mood, harmony, positivity, peace, intense happiness and joy, but
also increased feelings of unity, transcendence of space and time, mysticism,
sacredness, boundlessness, and ineffability (Griffiths et al., 2006, 2008). Patients
have also testified that, after psilocybin treatment, they felt an increased sense of
connectedness and acceptance (Watts et al., 2017), as well as lasting enhancements
196Is There Magic in These Mushrooms?
of their attitudes towards themselves and their lives. These changes may make
individuals more aware of and open to their support network, which is essential to
a healthy social life and dealing with mental illness, conflict and stress. Altruistic
social behaviors were also reported by third-party observers from the patients’
lives. These reports of vast and lasting positive effects point to potential for social
and societal benefit of through the therapeutic use of this drug (Griffiths et al.,
2006). Together, these outcomes promote prosocial behavior, wellbeing and
connection, which ultimately improve quality of life, prevent premature mortality
(Umberson & Montez, 2010), decrease health care costs (Holt-Lunstad et al.,
2017), and serve as a protective factor against violence (Stoddard et al., 2010).
Upon evaluation, psilocybin use does not indicate increased tendency
towards drug abuse, prolonged psychosis, persisting perception disorders, or other
long-term negative side effects. In experiments, adverse reactions to the drug were
rare, quickly resolved, and were only linked to high doses (Studerus et al., 2010).
As such, adverse reactions can be easily be mediated with proper medical oversight,
dosage and planning. It is important to mention that psilocybin has one of the most
positive safety profiles of all psychedelics and psychoactive drugs, as it has a very
low dependence potential and has a lethal dose one thousand times larger than its
effective dose (see Figure 11.2) (Gable, 2004, 2006; Griffiths et al., 2011). This
signifies that the likelihood of becoming addicted to or overdosing on psilocybin is
very low.
Figure 11.2: Plot of dependence potential and active dose:lethal dose ratio of
psychoactive drugs (Gable, 2006)
197Are We There Yet? The Golden Standards of Forensic Science
The general public may see psilocybin as a ‘gateway drug’ that will promote
further drug use or ritualistic abuse, because mushroom-naïve individuals often
view this drug as dangerous (Roberts et al., 2020). Some may, incorrectly, believe
that the benefits of microdosing psilocybin could be used to excuse the abuse of
drugs or alcohol for their perceived benefits, effectively promoting criminality and
harmful behavior. Research, however, has shown that microdosers construct
boundaries between themselves and recreational drug users by emphasizing their
embrace of middle-class values like happiness, self-control and ambition. This
parallel with conventional citizens helps microdosers normalize their drug use,
while facilitating their persistence through their treatment (Webb et al., 2019). This
persistence may be key to effective treatment. These boundaries also serve as a way
to decrease the dissonance that stems from the stigma that patients may hold
towards drug use, while keeping undesirable groups and behaviours, such as drug
use, away. This drug does not, therefore, occasion the abuse of other drugs
(Studerus et al., 2010), which, again, is of social, medical and legal benefit.
Psilocybin may play a role in preventing violence. Men who use magic
mushrooms are less likely to perpetrate domestic violence because they have better
emotion regulation compared to psychedelic-naïve males. Use of psilocybin
enhances interpersonal functioning, ultimately preventing conflict and aggression
(Thiessen et al., 2018). Further evidence suggests that hallucinogens decrease
criminality by reducing the likelihood of criminal recidivism (Hendricks et al.,
2014). Together, these conclusions highlight the fact that psilocybin prevents
violence and increases community safety, implying that it may serve the justice
system as well by shrinking the incidence of violent crime and criminality.
The medical legalization of psilocybin would spawn additional benefit to
the community and legal system by bringing this therapy out from ‘the
underground’ with clinically grown mushrooms, proper treatment methodology,
tailored dosing, and clinical oversight. This would increase the safety and treatment
effectiveness for those who are currently illegally self-medicating with psilocybin
because dosing precision, consistency, and safety is rare in illegal mushroom
consumption (Beug & Bigwood, 1982). Medical legalization would further reduce
the caseload in the justice system by eliminating some drug possession charges,
thus allowing the courts and police to focus on investigations that threaten public
safety to a greater degree.
198Is There Magic in These Mushrooms?
Drawbacks of Magic Mushrooms
Magic mushrooms may seem to live up to their name based on their benefits, but
they are not without their own set of drawbacks and legal implications.
Disadvantages lie within the tolerance, criminality, recklessness, bad trip and
flashback potentials of this drug. First and foremost, it should be noted that a
tolerance against psilocybin builds up, but also disappears, very quickly (Nicholas
et al., 2006). Drug tolerance to psilocybin weakens after a several days, so spacing
doses a few days apart would avoid this phenomenon. Although drug tolerances
can be conquered by increasing the dose, it is recommended to wait a few days
between doses instead in order to allow the brain and psyche to return to baseline
(Nicholas et al., 2006).
Another drawback to the current state of magic mushrooms is that they
remain largely illegal, and a strong social stigma exists against the use of this drug
(Anderson et al., 2019). The illegal nature and the difficulty of obtaining this
treatment are the most frequently reported barriers to treatment, which, once again,
leaves individuals without effective treatment or without the social and personal
benefits of the treatments (Cameron et al., 2020).
Notably, psilocybin also produces psychosis-like symptoms akin to those
in the first episodes of schizophrenia (Vollenweider et al., 1998). Additionally,
using this drug might exacerbate mental illness in those predisposed to episodes of
psychosis (Johnson et al., 2018). Although some researchers believe that magic
mushrooms do not cause prolonged psychosis (Studerus et al., 2010), a full dose of
psilocybin may lead to dangerous thoughts and behaviors that stem from delusions.
This outlines the less noticeable negative social ramifications of psilocybin,
especially in those with psychotic psychiatric conditions. Consequently, magic
mushrooms should be avoided by those who are predisposed to episodes of
psychosis. The risk of psychosis should be evaluated by physicians on a case-by-
case basis. These dangerous behaviors could be mediated with a risk management
plan and proper oversight.
The general public often fears hallucinogens because of what is known as a
“bad trip.” A bad trip is an unpleasant experience stimulated by psychoactive drugs.
Bad trips may be of small magnitude, with a bout of mild anxiety, or they may be
substantial, with feelings of terror, alienation, or identity loss. The implications of
these potential states show that anxiety management should be essential during
psilocybin administration. Bad trips, for example, have been shown to be more
199Are We There Yet? The Golden Standards of Forensic Science
likely with high psilocybin doses (Bienemann et al., 2020; Carbonaro et al., 2016).
A further study has found that bad trips can occasionally have positive value in
peoples’ lives if approached from a different perspective (Gashia et al., 2021). This
implies that bad trips can be somewhat undone or prevented by oversight by a
psychiatrist after or during the trip.
Unsupervised and unprepared psilocybin users may partake in reckless
behaviors, such as driving under the influence, mixing drugs, or exploring the
ledges of buildings, which is a threat to both the individual and the community
surrounding them. This behavior could also be prevented with proper education
and a “babysitter” to watch over individuals partaking in a psilocybin session. It
remains to be said that proper care and methodology cannot be enforced if the
treatment is taken at home without medical supervision. This, however, may not be
any different than the expectation of care that lies with current medication
standards. Notably, psilocybin can be detected in the blood (Moeller & Kraemer,
2002), and in urine samples (Grieshaber et al., 2001), which may help authorities
find and penalize those who are reckless under its influence.
Although very rarely seen in a clinical setting, Hallucinogen Persisting
Perception Disorder (HPPD) is a diagnosable disorder that may follow
hallucinogen use. HPPD is the re-experiencing of hallucinogen hallucinations (also
known as flashbacks) that later cause distress or functional impairment (Espiard et
al., 2005; Halpern et al., 2016). Long-term health issues after the use of magic
mushrooms, like these flashbacks or seizures, are caused by mixing magic
mushrooms with other substances (Amsterdam et al., 2011). This disorder is so rare
that researchers have even suggested that psilocybin does not cause persisting
perception disorder (Studerus et al., 2010). Nonetheless, this disorder can and
should be prevented by taking pure psilocybin treatments.
Medical legalization would leave most of the preventative burden of these
drawbacks to the physicians in charge of the psilocybin treatment. The potential for
flashbacks, bad trips and recklessness could be minimized by controlling the
dosage of psilocybin and creating a safe and comfortable environment for those
taking the medication. Psychosis could be managed by accounting for the patient’s
medical history and genetic predisposition.
Much like in the 1960s, magic mushrooms are gaining public interest for
recreational, personal and medical reasons. Thanks to modern technology, the
general public has access to information about the appearance and morphology of
magic mushrooms (Marciniak et al., 2010). This access may allow inexperienced
200Is There Magic in These Mushrooms?
individuals to seek psilocybin mushrooms in the wild to satisfy their recreational,
personal or medical problems. Unfortunately, this mushroom picking often has
fatal outcomes (Marciniak et al., 2010). Notably, however, this fatal consequence
will happen regardless of legalization, as public interest in the drug will exist
regardless of its legal status. Medical or recreational legalization of psilocybin
would increase safe public access to the mushrooms and may function as a
protective factor against wild mushroom picking. Education about the dangers of
eating wild mushrooms should also be commonplace in order to further prevent
unnecessary deaths.
Conclusion
Although they are not magical, magic mushrooms bring novel benefits to the table
of mental illness treatment in a clinical setting. Even in a single dose session, they
cause long term benefits for treatment-resistant depression (Carhart-Harris et al.,
2018; Goldberg et al., 2020; Johnson & Griffiths, 2017), PTSD (Mithoefer, 2007),
OCD (Moreno et al., 2006), alcohol dependence (Bogenschutz et al., 2015),
smoking cessation (Johnson et al., 2016) and anxiety (Goldberg et al., 2020;
Mithoefer et al., 2016; de Veen et al., 2016). Psilocybin also improves mood and
attitude, while promoting prosocial behavior, wellbeing and connection, which
ultimately improves quality of life, prevents premature mortality (Umberson &
Karas Montez, 2010), prevents suicidal tendencies (Gable, 2004; Hendricks et al.,
2015), decreases health care costs (Holt-Lunstad et al., 2017), and serves as a
protective factor against violence (Stoddard et al., 2010). The medical legalization
of psilocybin would benefit the community and legal system by bringing this
therapy into the light with clinically grown mushrooms, and proper treatment
methodology, dosing and oversight. This would increase the safety and treatment
effectiveness for those who are currently illegally self-medicating with psilocybin.
The medical legalization would also decrease wild mushroom picking and some of
the drug-related caseload in the legal system. Therefore, the justice system and
police force would be able to focus on investigations that threaten public safety to
a greater degree. Although psilocybin is beneficial for a wide range of
circumstances and sectors, it remains a psychoactive drug that must only be used
with proper precautions, education, care and respect. Doses should not be too large
and must not be mixed with other substances, in order to decrease the likelihood of
flashbacks or bad trips. With physician oversight, bad trips can be prevented or
201Are We There Yet? The Golden Standards of Forensic Science turned into a positive experience, thus lessening the potential harm from this treatment. Medical legalization would leave most of the caution, care and educational burden to the physicians and drug suppliers. This would shrink the potential for adverse reactions like flashbacks, bad trips, recklessness and psychosis by controlling for the triggering factors like dosage, environment and medical history respectively. Psilocybin has its positives and negatives, but it may nonetheless be the key to treating select mental disorders, and in turn decreasing the associated societal and judicial costs tied to these illnesses. As such, magic mushrooms deserve to be researched and should not be dismissed on the account of social stigma and political bureaucracy. References Amsterdam, J. V., Opperhuizen, A., & Brink, W. Belouin, S. J., & Henningfield, J. E. (2018). van. (2011). Harm potential of magic Psychedelics: Where we are now, why we got mushroom use: A review. Regulatory here, what we must do. Neuropharmacology, Toxicology and Pharmacology, 59(3), 423– 142, 7–19. 429. https://doi.org/10.1016/j.neuropharm.2018.02 https://doi.org/10.1016/j.yrtph.2011.01.006 .018 Anderson, T., Petranker, R., Rosenbaum, D., Bentivegna, G. (1998). The effects of inadequate Weissman, C. R., Dinh-Williams, L.-A., Hui, mental health resources on the operation of K., Farb, N. A. (2019). Microdosing the mental disorder provisions (thesis). psychedelics: personality, mental health, and Retrieved from creativity differences in microdosers. https://digitalcommons.schulichlaw.dal.ca/cgi Psychopharmacology, 236(2), 731–740. /viewcontent.cgi?article=1045&context=llm_ https://doi.org/10.1007/s00213-018-5106-2 theses Arroll, B., Elley, C. R., Fishman, T., Goodyear- Beug, M. W., & Bigwood, J. (1982). Psilocybin Smith, F. A., Kenealy, T., Blashki, G., . . . and psilocin levels in twenty species from MacGillivray, S. (2009). Antidepressants seven genera of wild mushrooms in the versus placebo for depression in primary Pacific Northwest, U.S.A. Journal of care. Cochrane Database of Systematic Ethnopharmacology, 5(3), 271–285. Reviews. Cochrane Library. https://doi.org/10.1016/0378-8741(82)90013- https://doi.org/10.1002/14651858.cd007954 7 Barrett, F. S., Johnson, M. W., & Griffiths, R. R. Bienemann, B., Ruschel, N. S., Campos, M. L., (2017). Neuroticism is associated with Negreiros, M. A., & Mograbi, D. C. (2020). challenging experiences with psilocybin Self-reported negative outcomes of mushrooms. Personality and Individual psilocybin users: A quantitative textual Differences, 117, 155–160. analysis. PLoS ONE. https://doi.org/10.1016/j.paid.2017.06.004 https://doi.org/10.1371/journal.pone.0229067 202
Is There Magic in These Mushrooms?
Blier, P., & De Montigny, C. (1994). Current for treatment-resistant depression: six-month
advances and trends in the treatment of follow-up. Psychopharmacology 235, 399–
depression. Trends in Pharmacological 408 (2018). https://doi.org/10.1007/s00213-
Sciences, 15(7), 220-226. 017-4771-x
https://doi.org/10.1016/0165-6147(94)90315-
8 Carhart-Harris, R. L., Roseman, L., Bolstridge,
M., Demetriou, L., Pannekoek, J. N., Wall,
Bogenschutz, M. P., Forcehimes, A. A., Pommy, M. B., … Nutt, D. J. (2017). Psilocybin for
J. A., Wilcox, C. E., Barbosa, P. C. R., & treatment-resistant depression: fMRI-
Strassman, R. J. (2015). Psilocybin-assisted measured brain mechanisms. Scientific
treatment for alcohol dependence: A proof- Reports, 7(1). https://doi.org/10.1038/s41598-
of-concept study. Journal of 017-13282-7
Psychopharmacology, 29(3), 289–299.
https://doi.org/10.1177/0269881114565144 Carod-Artal, F. J. (2015). Hallucinogenic drugs in
pre-Columbian Mesoamerican cultures.
Bystritsky, A., Khalsa, S. S., Cameron, M. E., & Neurología (English Edition), 30(1), 42–49.
Schiffman, J. (2013). Current diagnosis and https://doi.org/10.1016/j.nrleng.2011.07.010
treatment of anxiety disorders. P & T: A
peer-reviewed journal for formulary Cascade, E., Kalali, A. H., & Kennedy, S. H.
management, 38(1), 30–57. (2009). Real-world data on SSRI
https://www.ncbi.nlm.nih.gov/pmc/articles/P antidepressant side effects. Psychiatry
MC3628173/ (Edgmont), 6(2), 16–18.
https://pubmed.ncbi.nlm.nih.gov/19724743/
Cameron, L. P., Nazarian, A., & Olson, D. E.
(2020). Psychedelic Microdosing: Prevalence Cipriani, A., Furukawa, T. A., Salanti, G.,
and Subjective Effects. Journal of Chaimani, A., Atkinson, L. Z., Ogawa, Y., …
Psychoactive Drugs, 52(2), 113–122. Geddes, J. R. (2018). Comparative efficacy
https://doi.org/10.1080/02791072.2020.17182 and acceptability of 21 antidepressant drugs
50 for the acute treatment of adults with major
depressive disorder: a systematic review and
Capasso, A., Petrella, C., & Milano, W. (2009). network meta-analysis. The Lancet,
Pharmacological profile of ssris and snris in 391(10128), 1357–1366.
the treatment of eating disorders. Current https://doi.org/10.1016/s0140-
Clinical Pharmacology, 4(1), 78-83. 6736(17)32802-7
https://doi.org/10.2174/157488409787236092
Cuijpers, P., Sijbrandij, M., Koole, S. L.,
Carbonaro, T. M., Bradstreet, M. P., Barrett, F. Andersson, G., Beekman, A. T., & Reynolds,
S., MacLean, K. A., Jesse, R., Johnson, M. C. F. (2014). Adding psychotherapy to
W., & Griffiths, R. R. (2016). Survey study antidepressant medication in depression and
of challenging experiences after ingesting anxiety disorders: A meta-analysis. World
psilocybin mushrooms: Acute and enduring Psychiatry, 13(1), 56-67.
positive and negative consequences. Journal https://doi.org/10.1002/wps.20089
of Psychopharmacology, 30(12), 1268–1278.
https://doi.org/10.1177/0269881116662634 Daniel, J., & Haberman, M. (2017). Clinical
potential of psilocybin as a treatment for
Carhart-Harris, R.L., Bolstridge, M., Day, C.M.J. mental health conditions. Mental Health
et al. Psilocybin with psychological support
203Are We There Yet? The Golden Standards of Forensic Science
Clinician, 7(1), 24-28. Gable, R. S. (2004). Comparison of acute lethal
https://doi.org/10.9740/mhc.2017.01.024 toxicity of commonly abused psychoactive
substances. Addiction, 99(6), 686–696.
DeRubeis, R. J., Siegle, G. J., & Hollon, S. D. https://doi.org/10.1111/j.1360-
(2008). Cognitive therapy versus medication 0443.2004.00744.x
for depression: Treatment outcomes and
neural mechanisms. Nature Reviews Gable, R. S. (2006). Acute toxicity of drugs
Neuroscience, 9(10), 788-796. versus regulatory status. In J. M. Fish (Ed.),
https://doi.org/10.1038/nrn2345 Drugs and society: U.S. public policy (pp.
149–162). essay, Rowman & Littlefield
Detrick, A., & Stiepock, V. (1992). Treating Publishers.
persons with mental illness, substance abuse,
and legal problems: The Rhode Island Gashia, L., Sandberg, S., & Pedersen, W. (2021).
experience. New Directions for Mental Making “bad trips” good: How users of
Health Services, 1992(56), 65–77. psychedelics narratively transform
https://doi.org/10.1002/yd.23319925607 challenging trips into valuable experiences.
International Journal of Drug Policy, 87.
Dickerson, F. B., & Lehman, A. F. (2006). https://doi.org/10.1016/j.drugpo.2020.102997
Evidence-based psychotherapy for
schizophrenia. Journal of Nervous & Mental
Disease, 194(1), 3-9. Geyer, M., & Vollenweider, F. (2008). Serotonin
https://doi.org/10.1097/01.nmd.0000195316. research: Contributions to understanding
86036.8a psychoses. Trends in Pharmacological
Sciences, 29(9), 445–453.
Druss, B. G., Hwang, I., Petukhova, M., https://doi.org/10.1016/j.tips.2008.06.006
Sampson, N. A., Wang, P. S., & Kessler, R.
C. (2008). Impairment in role functioning in Goldberg, S. B., Pace, B. T., Nicholas, C. R.,
mental and chronic medical disorders in the Raison, C. L., & Hutson, P. R. (2020). The
United States: results from the National experimental effects of psilocybin on
Comorbidity Survey Replication. Molecular symptoms of anxiety and depression: A meta-
Psychiatry, 14(7), 728–737. analysis. Psychiatry Research, 284, 112749.
https://doi.org/10.1038/mp.2008.13 https://doi.org/10.1016/j.psychres.2020.1127
49
Espiard, M.-L., Lecardeur, L., Abadie, P.,
Halbecq, I., & Dollfus, S. (2005). Grieshaber, A. F., Moore, K. A., & Levine, B.
Hallucinogen persisting perception disorder (2001). The detection of psilocin in human
after psilocybin consumption: a case study. urine. Journal of Forensic Sciences, 46(3),
European Psychiatry , 20(5-6), 458–460. 627–630.
https://doi.org/10.1016/j.eurpsy.2005.04.008 https://pubmed.ncbi.nlm.nih.gov/11373000/
Frank, E. (1991). Conceptualization and rationale Griffiths, R. R., Johnson, M. W., Richards, W.
for consensus definitions of terms in major A., Richards, B. D., McCann, U., & Jesse, R.
depressive disorder. Archives of General (2011). Psilocybin occasioned mystical-type
Psychiatry, 48(9), 851. experiences: immediate and persisting dose-
https://doi.org/10.1001/archpsyc.1991.01810 related effects. Psychopharmacology, 218(4),
330075011 649–665. https://doi.org/10.1007/s00213-
011-2358-5
204Is There Magic in These Mushrooms?
Griffiths, R. R., Richards, W. A., Johnson, M. Healy, D., Herxheimer, A., & Menkes, D. B.
W., McCann, U. D., & Jesse, R. (2008). (2006). Antidepressants and Violence:
Mystical-type experiences occasioned by Problems at the Interface of Medicine and
psilocybin mediate the attribution of personal Law. PLoS Medicine, 3(9).
meaning and spiritual significance 14 months https://doi.org/10.1371/journal.pmed.003037
later. Journal of Psychopharmacology, 22(6), 2
621–632.
https://doi.org/10.1177/0269881108094300 Hendricks, P. S., Clark, C. B., Johnson, M. W.,
Fontaine, K. R., & Cropsey, K. L. (2014).
Griffiths, R. R., Richards, W. A., McCann, U., & Hallucinogen use predicts reduced recidivism
Jesse, R. (2006). Psilocybin can occasion among substance-involved offenders under
mystical-type experiences having substantial community corrections supervision. Journal
and sustained personal meaning and spiritual of Psychopharmacology, 28(1), 62–66.
significance. Psychopharmacology, 187(3), https://doi.org/10.1177/0269881113513851
268–283. https://doi.org/10.1007/s00213-
006-0457-5 Hendricks, P. S., Johnson, M. W., & Griffiths, R.
R. (2015). Psilocybin, psychological distress,
Grob, C. S., Bossis, A. P., & Griffiths, R. R. and suicidality. Journal of
(2012). Use of the classic hallucinogen Psychopharmacology, 29(9), 1041–1043.
psilocybin for treatment of existential distress https://doi.org/10.1177/0269881115598338
associated with cancer. Psychological
Aspects of Cancer. New York, NY: Springer. Hofmann, A., Frey, A., Ott, H., Petrzilka, T., &
291–308. https://doi.org/10.1007/978-1-4614- Troxler, F. (1958). Elucidation of the
4866-2_17 structure and the synthesis of psilocybin.
Experientia, 14(11), 397–399.
Grob, C. S., Danforth, A. L., Chopra, G. S., https://doi.org/10.1007/bf02160424
Hagerty, M., McKay, C. R., Halberstadt, A.
L., & Greer, G. R. (2011). Pilot study of Hollander, E. (1998). Treatment of obsessive-
psilocybin treatment for anxiety in patients compulsive spectrum disorders with ssris.
with advanced-stage cancer. Archives of British Journal of Psychiatry, 173(S35), 7-12.
General Psychiatry, 68(1), 71. https://doi.org/10.1192/s0007125000297845
https://doi.org/10.1001/archgenpsychiatry.20
10.116 Hollon, S. D., Thase, M. E., & Markowitz, J. C.
(2002). Treatment and prevention of
Grof, S. (2009). LSD: doorway to the numinous: depression. Psychological Science in the
the groundbreaking psychedelic research into Public Interest, 3(2), 39-77.
realms of the human unconscious. Vermont: https://doi.org/10.1111/1529-1006.00008
Park Street Press.
Holt-Lunstad, J., Robles, T. F., & Sbarra, D. A.
Halpern, J. H., Lerner, A. G., & Passie, T. (2016). (2017). Advancing social connection as a
A review of hallucinogen persisting public health priority in the United States.
perception disorder (HPPD) and an American Psychologist, 72(6), 517–530.
exploratory study of subjects claiming https://doi.org/10.1037/amp0000103
symptoms of HPPD. Behavioral
Neurobiology of Psychedelic Drugs, 333– Hutten, N. R., Mason, N. L., Dolder, P. C., &
360. https://doi.org/10.1007/7854_2016_457 Kuypers, K. P. (2019). Self-Rated
Effectiveness of Microdosing With
205Are We There Yet? The Golden Standards of Forensic Science
Psychedelics for Mental and Physical Health Kessler, R. C., Barber, C., Birnbaum, H. G.,
Problems Among Microdosers. Frontiers in Frank, R. G., Greenberg, P. E., Rose, R. M.,
Psychiatry, 10. … Wang, P. (1999). Depression In The
https://doi.org/10.3389/fpsyt.2019.00672 Workplace: Effects On Short-Term
Disability. Health Affairs, 18(5), 163–171.
Johansen, P.-Ø., & Krebs, T. S. (2015). https://doi.org/10.1377/hlthaff.18.5.163
Psychedelics not linked to mental health
problems or suicidal behavior: A population Kessler, R. C., Heeringa, S., Lakoma, M. D.,
study. Journal of Psychopharmacology, Petukhova, M., Rupp, A. E., Schoenbaum,
29(3), 270–279. M., … Zaslavsky, A. M. (2008). Individual
https://doi.org/10.1177/0269881114568039 and Societal Effects of Mental Disorders on
Earnings in the United States: Results From
Johnson, M. W., Garcia-Romeu, A., Cosimano, the National Comorbidity Survey
M. P., & Griffiths, R. R. (2014). Pilot study Replication. American Journal of Psychiatry,
of the 5-HT2AR agonist psilocybin in the 165(6), 703–711.
treatment of tobacco addiction. Journal of https://doi.org/10.1176/appi.ajp.2008.080101
Psychopharmacology, 28(11), 983–992. 26
https://doi.org/10.1177/0269881114548296
Knudsen, H. K., Ducharme, L. J., & Roman, P.
Johnson, M. W., Garcia-Romeu, A., & Griffiths, M. (2007). The adoption of medications in
R. R. (2016). Long-term follow-up of substance abuse treatment: Associations with
psilocybin-facilitated smoking cessation. The organizational characteristics and technology
American Journal of Drug and Alcohol clusters. Drug and Alcohol Dependence,
Abuse, 43(1), 55–60. 87(2-3), 164-174.
https://doi.org/10.3109/00952990.2016.11701 https://doi.org/10.1016/j.drugalcdep.2006.08.
35 013
Johnson, M.W., & Griffiths, R.R. Potential Kuypers, K. P. C. (2020). The therapeutic
Therapeutic Effects of Psilocybin. potential of microdosing psychedelics in
Neurotherapeutics 14, 734-740 (2017). depression. Therapeutic Advances in
https://doi.org/10.1007/s13311-017-0542-y Psychopharmacology, 10, 204512532095056.
https://doi.org/10.1177/2045125320950567
Johnson, M. W., Griffiths, R. R., Hendricks, P.
S., & Henningfield, J. E. (2018). The abuse Kuypers, K. P. C., Ng, L., Erritzoe, D., Knudsen,
potential of medical psilocybin according to G. M., Nichols, C. D., Nichols, D. E., …
the 8 factors of the Controlled Substances Nutt, D. (2019). Microdosing psychedelics:
Act. Neuropharmacology, 142, 143–166. More questions than answers? An overview
https://doi.org/10.1016/j.neuropharm.2018.05 and suggestions for future research. Journal
.012 of Psychopharmacology, 33(9), 1039–1057.
https://doi.org/10.1177/0269881119857204
Kazdin, A. E., & Blase, S. L. (2011). Rebooting
psychotherapy research and practice to Lea, T., Amada, N., Jungaberle, H., Schecke, H.,
reduce the burden of mental illness. Scherbaum, N., & Klein, M. (2020).
Perspectives on Psychological Science, 6(1), Perceived outcomes of psychedelic
21-37. microdosing as self-managed therapies for
https://doi.org/10.1177/1745691610393527 mental and substance use disorders.
206Is There Magic in These Mushrooms?
Psychopharmacology, 237(5), 1521–1532. medicine: New evidence for hallucinogenic
https://doi.org/10.1007/s00213-020-05477-0 substances as treatments, 1, 155-176.
https://doi.org/10.1007/s00213-019-05249-5
Mahapatra, A., & Gupta, R. (2016). Role of
psilocybin in the treatment of depression. Mithoefer, M. C., Grob, C. S., & Brewerton, T.
Therapeutic Advances in D. (2016). Novel psychopharmacological
Psychopharmacology, 7(1), 54–56. therapies for psychiatric disorders: psilocybin
https://doi.org/10.1177/2045125316676092 and MDMA. The Lancet Psychiatry, 3(5),
481–488. https://doi.org/10.1016/s2215-
Marciniak, B., Ferenc, T., Kusowska, J., 0366(15)00576-3
Ciećwierz, J., & Kowalczyk, E. (2010).
Zatrucia wybranymi grzybami o działaniu Moeller, M. R., & Kraemer, T. (2002). Drugs of
neurotropowym i halucynogennym Abuse Monitoring in Blood for Control of
[Poisoning with selected mushrooms with Driving Under the Influence of Drugs.
neurotropic and hallucinogenic effect]. Therapeutic Drug Monitoring, 24(2), 210–
Medycyna pracy, 61(5), 583–595. 221. https://doi.org/10.1097/00007691-
200204000-00003
Marvanova, M., & Gramith, K. (2018). Role of
antidepressants in the treatment of adults with Moreno, F. A., Wiegand, C. B., Taitano, E. K., &
anorexia nervosa. Mental Health Clinician, Delgado, P. L. (2006). Safety, Tolerability,
8(3), 127-137. and Efficacy of Psilocybin in 9 Patients With
https://doi.org/10.9740/mhc.2018.05.127 Obsessive-Compulsive Disorder. The Journal
of Clinical Psychiatry, 67(11), 1735–1740.
Marzuk, P. M. (1996). Violence, Crime, and https://doi.org/10.4088/jcp.v67n1110
Mental Illness. Archives of General
Psychiatry, 53(6), 481–486. Nicholas, L. G., & Ogame, K. (2006). In
https://doi.org/10.1001/archpsyc.1996.01830 Psilocybin mushroom handbook: Easy indoor
060021003 and outdoor cultivation (p. 164). Essay,
Quick American
McKenna, T. (1984, February). Psychedelic Archives. https://www.researchgate.net/profil
Society. AskTMK. Big Sur, California; Esalen e/Yehya_Salih/post/How_does_one_keep_co
Institute. ntaminants_away_in_outdoor_cultivation_of
https://www.asktmk.com/talks/Psychedelic+S _mushroom_Will_it_be_necessary_to_steriliz
ociety e_substrate_before_spreading_on_beds/attach
ment/59d6480379197b80779a2c37/AS%3A4
Merikangas, K. R., Ames, M., Cui, L., Stang, P. 65000243437569%401487876106026/downl
E., Ustun, T. B., Von Korff, M., & Kessler, oad/Mushroom+handbook-
R. C. (2007). The Impact of Comorbidity of Easy+indoor+and+outdoorncultivation.pdf
Mental and Physical Conditions on Role
Disability in the US Adult Household Nichols, D. E. (2004). Hallucinogens.
Population. Archives of General Psychiatry, Pharmacology & Therapeutics, 101(2), 131–
64(10), 1180. 181.
https://doi.org/10.1001/archpsyc.64.10.1180 https://doi.org/10.1016/j.pharmthera.2003.11.
002
Mithoefer, M. (2007). MDMA-assisted
psychotherapy for the treatment of post- O’Donnell, S., Syoufi, M., Jones, W., & Bennett,
traumatic stress disorder. Psychedelic K. (2017). Use of medication and
207Are We There Yet? The Golden Standards of Forensic Science
psychological counselling among Canadians https://doi.org/10.1212/01.wnl.0000219761.0
with mood and/or anxiety disorders. Health 5466.43
Promotion and Chronic Disease Prevention
in Canada, 37(5), 160-171. Stoddard, S. A., McMorris, B. J., & Sieving, R.
https://doi.org/10.24095/hpcdp.37.5.04 E. (2010). Do Social Connections and Hope
Matter in Predicting Early Adolescent
Pampallona, S., Bollini, P., Tibaldi, G., Violence? American Journal of Community
Kupelnick, B., & Munizza, C. (2004). Psychology, 48(3-4), 247–256.
Combined pharmacotherapy and https://doi.org/10.1007/s10464-010-9387-9
psychological treatment for depression.
Archives of General Psychiatry, 61(7), 714. Studerus, E., Kometer, M., Hasler, F., &
https://doi.org/10.1001/archpsyc.61.7.714 Vollenweider, F. X. (2010). Acute, subacute
and long-term subjective effects of psilocybin
Rinne, T., Van den Brink, W., Wouters, L., & in healthy humans: A pooled analysis of
Van Dyck, R. (2002). SSRI treatment of experimental studies. Journal of
borderline personality disorder: A Psychopharmacology, 25(11),
randomized, placebo-controlled clinical trial https://doi.org/10.1177/0269881110382466
for female patients with borderline
personality disorder. American Journal of Szigeti, B., Kartner, L., Blemings, A., Rosas, F.,
Psychiatry, 159(12), 2048-2054. Feilding, A., Nutt, D. J., … Erritzoe, D.
https://doi.org/10.1176/appi.ajp.159.12.2048 (2021). Self-blinding citizen science to
explore psychedelic microdosing. ELife, 10.
Roberts, C. A., Osborne-Miller, I., Cole, J., Gage, https://doi.org/10.7554/elife.62878
S. H., & Christiansen, P. (2020). Perceived
harm, motivations for use and subjective Thiessen, M. S., Walsh, Z., Bird, B. M., &
experiences of recreational psychedelic Lafrance, A. (2018). Psychedelic use and
‘magic’ mushroom use. Journal of intimate partner violence: The role of
Psychopharmacology, 34(9), 999–1007. emotion regulation. Journal of
https://doi.org/10.1177/0269881120936508 Psychopharmacology, 32(7), 749-755.
https://doi.org/10.1177/0269881118771782
Roseman, L., Nutt , D. J., & Carhart-Harris, R. L.
(2018). Quality of Acute Psychedelic Thomas, K., Malcolm, B., & Lastra, D. (2017).
Experience Predicts Therapeutic Efficacy of Psilocybin-Assisted Therapy: A Review of a
Psilocybin for Treatment-Resistant Novel Treatment for Psychiatric Disorders.
Depression. Frontiers in Pharmacology. Journal of Psychoactive Drugs, 49(5), 446–
https://doi.org/10.3389/fphar.2017.00974 455.
https://doi.org/10.1080/02791072.2017.13207
Sellers, E. M. (2017). Psilocybin: Good Trip or 34
Bad Trip. Clinical Pharmacology &
Therapeutics, 102(4), 580–584. Tylš, F., Páleníček, T., & Horáček, J. (2014).
https://doi.org/10.1002/cpt.697 Psilocybin – Summary of knowledge and new
perspectives. European
Sewell, R. A., Halpern, J. H., & Pope, H. G. Neuropsychopharmacology, 24(3), 342–356.
(2006). Response of cluster headache to https://doi.org/10.1016/j.euroneuro.2013.12.0
psilocybin and LSD. Neurology, 66(12), 06
1920–1922.
208Is There Magic in These Mushrooms?
Umberson, D., & Montez, K.J. (2010). Social Webb, M., Copes, H., & Hendricks, P. S. (2019).
Relationships and Health: A Flashpoint for Narrative identity, rationality, and
Health Policy. Journal of Health and Social microdosing classic psychedelics.
Behavior, 51(1_suppl). International Journal of Drug Policy, 70, 33–
https://doi.org/10.1177/0022146510383501 39.
https://doi.org/10.1016/j.drugpo.2019.04.013
deVeen, B. T. H., Schellekens, A. F. A., Verheij,
M. M. M., & Homberg, J. R. (2016). Weissman, M. M., Markowitz, J. C., & Klerman,
Psilocybin for treating substance use G. L. (2000). Comprehensive guide to
disorders? Expert Review of interpersonal psychotherapy. New York:
Neurotherapeutics, 17(2), 203–212. Basic Books.
https://doi.org/10.1080/14737175.2016.12208 https://psycnet.apa.org/record/2000-07539-
34 000
Vollenweider, F. X., Vollenweider- Winkelman, M. J. (2014). Therapeutic
Scherpenhuyzen, M. F., Bäbler, A., Vogel, applications of ayahuasca and other sacred
H., & Hell, D. (1998). Psilocybin induces medicines. The Therapeutic Use of
schizophrenia-like psychosis in humans via a Ayahuasca, 1–21.
serotonin-2 agonist action. NeuroReport, https://doi.org/10.1007/978-3-642-40426-
9(17), 3897–3902. 9_1
https://doi.org/10.1097/00001756-
199812010-00024 Zohar, J., & Westenberg, H. G. (2000). Anxiety
disorders: A review of tricyclic
Watts, R., Day, C., Krzanowski, J., Nutt, D., & antidepressants and selective serotonin
Carhart-Harris, R. (2017). Patients’ Accounts reuptake inhibitors. Acta Psychiatrica
of Increased “Connectedness” and Scandinavica, 101(S403), 39-49.
“Acceptance” After Psilocybin for https://doi.org/10.1111/j.1600-
Treatment-Resistant Depression. Journal of 0447.2000.tb10947.x
Humanistic Psychology, 57(5), 520–564.
https://doi.org/10.1177/0022167817709585
209You can also read

















































