Insulin Resistance and Hypertension - The Insulin Resistance Atherosclerosis Study
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Insulin Resistance and Hypertension
The Insulin Resistance Atherosclerosis Study
Mohammed F. Saad, Marian Rewers, Joseph Selby, George Howard, Sujata Jinagouda, Salwa Fahmi,
Dan Zaccaro, Richard N. Bergman, Peter J. Savage, Steven M. Haffner
Abstract—The association between insulin resistance and insulinemia and hypertension is controversial. We examined the
relation between insulin resistance and hypertension in 564 non-Hispanic whites (NHW), 505 Hispanics (H), and 413
African Americans (AA) who participated in the Insulin Resistance Atherosclerosis Study (IRAS). Insulin sensitivity
was measured with a frequently sampled intravenous glucose tolerance test with minimal model analysis. The
prevalence of hypertension was 32.5%, 49.4%, and 32.3% in NHW, AA, and H, respectively (P⬍0.001). When subjects
without diabetes in all ethnic groups were combined, age, male sex, race (AA), body mass index (BMI), and insulin
resistance, but not fasting insulin, were significantly associated with hypertension. When each ethnic group was
analyzed separately, insulin resistance was significantly associated with hypertension in NHW and H, but not AA. After
excluding subjects taking antihypertensive medications, male sex, BMI, fasting glucose, and insulin resistance, but not
fasting insulin, were significant determinants of blood pressure. When the 3 ethnic groups were analyzed separately,
insulin resistance was significantly associated with blood pressure in H, but not NHW, or AA. Neither insulin resistance
nor fasting insulin was significantly associated with hypertension or blood pressure in subjects with diabetes of the 3
ethnic groups after adjusting for age, sex, BMI, and waist. In conclusion, insulin resistance, but not insulinemia, was
related to hypertension and blood pressure in subjects without diabetes, but ethnic differences in these relations appear
to exist. Neither insulin resistance nor insulinemia was related to hypertension or blood pressure in patients with type
2 diabetes in the 3 ethnic groups. (Hypertension. 2004;43:1324-1331.)
Key Words: insulin resistance 䡲 insulin 䡲 hypertension 䡲 blood pressure 䡲 diabetes
I n 1966, Welborn and colleagues1 described hyperinsu-
linemia in normoglycemic patients with hypertension
and suggested that these subjects could be insulin resistant.
vations, it was proposed that insulin resistance might lead
to hypertension because of diminished insulin-induced
vasodilation and an imbalance between its pressor and
Two decades later, Ferrannini et al2 confirmed this obser- depressor effects.7
vation by showing that lean white hypertensive patients Although a large number of studies examined the
had lower insulin-mediated glucose disposal than normal relation between insulinemia and hypertension and/or
controls. It has been hypothesized, therefore, that insulin blood pressure (BP), the results have been inconsistent
and/or insulin resistance could contribute to the pathogen- with some reporting strong and others weak, or no asso-
esis of hypertension.3 Insulin was shown to stimulate the ciation.8 –19 A smaller number of studies measured insulin
sympathetic nervous system, increase renal sodium reten- resistance directly, mostly in small groups of subjects with
tion, modulate cation transport, and induce vascular still conflicting results.20 –27 Herein, we describe the rela-
smooth muscle hypertrophy (reviewed in Reference 4). It is tion between insulin resistance and hypertension in a large
plausible that insulin resistance through the concomitant triethnic population that participated in the Insulin Resis-
compensatory hyperinsulinemia could contribute to the tance Atherosclerosis Study (IRAS). Insulin sensitivity
pathogenesis of hypertension by one or more of these was measured directly with the insulin-modified fre-
mechanisms. Nonetheless, acute insulin infusion was quently sampled intravenous glucose tolerance test
found to have a vasodilator hypotensive rather than a (FSIGT) with minimal model analysis (MINMOD) in 1482
hypertensive effect.5,6 To reconcile these discrepant obser- subjects.
Received March 15, 2004; first decision March 16, 2004; revision accepted March 24, 2004.
From the Department of Medicine (M.F.S., S.J., S.F.), UCLA School of Medicine, Los Angeles, Calif; the Department of Preventive Medicine and
Biometrics (M.R.), University of Colorado, Denver; the Division of Research (J.S.), Kaiser Permanente, Oakland, Calif; the Department of Public Health
Sciences (G.H., D.Z.), Wake Forest University Medical School, Winston-Salem, NC; the Department of Physiology and Biophysics (R.N.B.), University
of Southern California, Los Angeles; the Division of Epidemiology and Clinical Applications (P.J.S.), National Heart, Lung and Blood Institute, National
Institutes of Health, Bethesda, Md; and the Department of Medicine (S.M.H.), University of Texas at San Antonio.
Correspondence to Mohammed F. Saad, MD, Division of Clinical Epidemiology, UCLA Medical School, 924 Westwood Blvd, Suite 335 (Mail Box
15), Los Angeles, CA 90024. E-mail msaad@mednet.ucla.edu
© 2004 American Heart Association, Inc.
Hypertension is available at http://www.hypertensionaha.org DOI: 10.1161/01.HYP.0000128019.19363.f9
1324
Downloaded from http://hyper.ahajournals.org/ by guest on May 17, 2015Saad et al Insulin Resistance and Hypertension 1325
Subjects and Methods
Subjects
Details of subject recruitment and study protocol were described.28
In brief, the IRAS included 1625 subjects who were studied at 4
clinical centers at Oakland and Los Angeles, Calif; San Luis, Co; and
San Antonio, Tex. Clinical centers in California enrolled non-
Hispanic whites (NHW) and African-Americans (AA) from Kaiser
Permanente, a nonprofit health maintenance organization. Those in
San Antonio, Tex, and San Luis Valley, Co, studied NHW and
Hispanics (H) recruited from two ongoing population-based studies
(San Antonio Heart Study and the San Luis Valley Diabetes
Study), respectively.
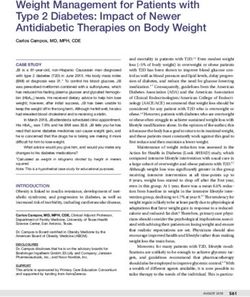
The study aimed to include equal numbers of subjects in different Figure 1. The prevalence of hypertension across the spectrum
categories of glucose tolerance (normal glucose tolerance [NGT], of glucose tolerance in the 3 ethnic groups. P⬍0.001 in each.
impaired glucose tolerance [IGT], and type 2 diabetes) according to
the 1985 World Health Organization criteria. Therefore, subjects
with IGT and type 2 diabetes were oversampled. Insulin-treated correlation coefficient of 0.18 in the 3 ethnic groups combined (0.29
patients with diabetes and those with a fasting glucose in whites, 0.37 in AA, and 0.28 in H) at a significance level of 0.05.
⬎16.7 mmol/L were excluded. The final IRAS cohort included 721
men and 904 women aged 40 to 69 years; 614 NHW, 548 H, and 464 Results
AA. There were 720 subjects (44%) with NGT, 369 (23%) with IGT,
and 537 (33%) with type 2 diabetes. The current analysis includes Glucose Intolerance, Obesity, and Hypertension
1482 subjects in whom insulin sensitivity was measured. The prevalence of hypertension was 32.5% in NHW, 49.4%
The IRAS examination required 2 visits, ⬇1 week apart. Partici- in AA, and 32.3% in H (P⬍0.001). Hypertension was more
pants were asked to fast for 12 hours before each visit and to abstain common in subjects with type 2 diabetes, followed by IGT,
from heavy exercise and alcohol for 24 hours and from smoking the and then NGT in each ethnic group (Figure 1). Controlling for
morning of each visit. An oral glucose tolerance test (OGTT) was
performed with a 75-g glucose load in the first visit. An insulin- age and sex, both overall and central adiposity were signifi-
modified FSIGT was done in the second visit for the determination cantly associated with hypertension in individuals without
of the insulin sensitivity index (SI) with the computer program diabetes in the 3 ethnic groups. In subjects with diabetes,
MINMOD.29 An injection of insulin was used to ensure adequate hypertension was significantly associated with BMI in NHW
plasma insulin levels for the accurate computation of insulin resis-
tance across a broad range of glucose tolerance.30 –32
(P⫽0.01) and H (P⫽0.04) but not in AA, after adjusting for
BP was measured during each visit with a mercury sphygmoma- age and sex. The prevalence of hypertension tended to
nometer before the OGTT and the FSIGT. A standardized protocol in increase with the waist circumference in subjects with diabe-
which the appropriate cuff size was used depending on the arm tes controlling for age and sex, but the association was
circumference was followed. Three measurements were taken 5 statistically significant only in H (P⫽0.01). Logistic regres-
minutes apart in the right arm in the sitting position after 5 minutes
of rest. The average of the second and third measurements was taken sion analysis of subjects with and without diabetes combined
as the participant’s BP during each visit. The average BP of the two showed that race, age, BMI (or waist circumference), and
visits is used in this analysis. Mean BP (MBP) was calculated as glycemia were significantly associated with hypertension.
0.33⫻systolic BP (SBP)⫹0.66⫻diastolic BP (DBP). Hypertension Adjusting for age, sex, BMI, and glycemia, the prevalence of
was defined as SBP ⱖ140 mm Hg or DBP ⱖ90 mm Hg or as taking
antihypertensive medications. Body mass index (weight [kg]/height
hypertension was higher in AA than in NHW (odds ratio:
[m2]) is used as a measure of overall adiposity and minimum waist 2.35; 95% CI: 1.67 to 3.30) and H (odds ratio 2.96; CI: 1.82
circumference as an index of body fat distribution. to 4.81), but there was no difference between H and NHW.
An increase in 2-hour plasma glucose of 1 mmol/L was
Statistical Analysis associated with a 5% increase in the likelihood of having
Data are expressed as means⫾SE or as means with 95% confidence hypertension (CI 2.7 to 7.1%), controlling for the other
interval (Cl). Insulin levels and SI values were log-transformed to
normalize the distribution. The log of SI⫹1 was used in the analysis variables.
because of the existence of zero SI values. Statistical analyses were
performed with programs of SPSS, Inc. One-way ANOVA and 2 Insulinemia, Insulin Resistance, and Hypertension
tests were used to compare continuous and categorical variables, in Subjects Without Diabetes
respectively, among the 3 ethnic groups. Two-way ANOVA was Hypertensive subjects without diabetes were older and had
used to evaluate the effects of ethnicity and hypertension on different
variables. The sample size provided more than 90% to detect
significantly higher BMI, waist circumference, and fasting
differences in fasting and 2-hour insulin concentrations and SI in the and 2-hour post-load plasma glucose and insulin concentra-
subjects without diabetes by race and hypertension status at a tions and lower SI than their normotensive counterparts
significance level of 0.05. For the subjects with diabetes, the sample (Table 1). After adjusting for age, sex, BMI, and waist,
size provided ⬍60% power to detect significant differences in these differences in fasting insulinemia between hypertensive and
variables. The Tukey method was used for multiple comparisons.
Logistic regression analysis was used to evaluate the relation normotensive subjects remained significant only in H and
between different variables and hypertension. Linear regression those in SI in NHW and H. The prevalence of hypertension
and/or Pearson product moment correlations were used to evaluate increased with fasting insulinemia. This association was
the relation between BP and different variables. The sample size of significant in NHW and Hispanics (P⬍0.01 for linear trend),
subjects without diabetes provided 80% power to detect a correlation
coefficient of 0.11 in the 3 ethnic groups combined (0.16 in whites,
but not in AA (P⫽0.16). After adjusting for age, sex, BMI,
0.22 in AA, and 0.18 in H) at a significance level of 0.05. The sample and waist, insulinemia was significantly associated with
size of subjects with diabetes provided 80% power to detect a hypertension only in H (P⫽0.001). Similarly, the prevalence
Downloaded from http://hyper.ahajournals.org/ by guest on May 17, 20151326 Hypertension June 2004
TABLE 1. Characteristics of Hypertensive and Nonhypertensive Subjects Without Diabetes
NHW AA H P
Normotensive, Hypertensive, Normotensive, Hypertensive, Normotensive, Hypertensive,
Variable n⫽293 n⫽107 n⫽157 n⫽103 n⫽246 n⫽97 Ethnicity Hypertension
Age, y* 55⫾0.5 59⫾0.7 53⫾0.7 57⫾0.8 53⫾0.5 57⫾0.7 0.003 ⬍0.001
Sex, % F 50.5 54.2 55.4 59.2 59.3 53.6 0.183 0.778
BMI, kg/m2* 26.77⫾0.28 29.39⫾0.54 28.50⫾0.39 31.13⫾0.70 28.0⫾0.35 30.57⫾0.63 ⬍0.001 ⬍0.001
Minimum waist, cm* 88.3⫾0.7 94.2⫾1.2 89.02⫾0.9 95.4⫾1.4 89.1⫾0.8 96.1⫾1.3 0.195 ⬍0.001
SBP, mm Hg* 115⫾0.7 135⫾1.7 117⫾0.9 136⫾1.5 113⫾0.7 137⫾1.7 0.37 ⬍0.001
DBP, mm Hg* 75⫾0.4 82⫾0.9 76⫾0.6 83⫾0.9 76⫾0.4 84⫾1.0 0.066 ⬍0.001
Fasting glucose, mmol/L* 5.41⫾0.04 5.60⫾0.07 5.53⫾0.06 5.80⫾0.06 5.31⫾0.03 5.57⫾0.06 ⬍0.001 ⬍0.001
2-hour glucose, mmol/L* 6.65⫾0.11 7.48⫾0.18 6.56⫾0.15 7.63⫾0.16 6.76⫾0.12 7.48⫾0.19 0.582 ⬍0.001
Fasting insulin, pmol/L† 63 (59–68) 81 (71–91) 78 (71–86) 91 (82–102) 77 (71–84) 109 (98–120) ⬍0.001 ⬍0.001
2-hour insulin, pmol/L† 328 (298–362) 442 (381–512) 383 (336–437) 566 (489–655) 467 (419–519) 650 (567–745) ⬍0.001 ⬍0.001
SI⫻10⫺4 2.27 (2.07–2.47) 1.46 (1.24–1.71) 1.82 (1.59–2.07) 1.15 (0.97–1.34) 1.78 (1.59–1.98) 0.96 (0.80–1.13) ⬍0.001 ⬍0.001
(min⫺1 䡠 U⫺1 䡠 mL⫺1)†
IGT, % 28.0 43.9 25.5 46.6 30.5 41.2 0.894 ⬍0.001
Abbreviations are defined in the text.
*Mean⫾SE is shown.
†Mean and 95% CI are shown.
of hypertension was higher at lower SI values in all ethnic with hypertension (Table 2). Fasting insulin was significantly
groups (P⬍0.05 in each), but this association remained associated with hypertension only when SI was not included
significant only in H (P⫽0.02) after controlling for age, sex, in the logistic regression models. The interaction term be-
BMI, and waist (Figure 2). tween SI and ethnicity was not statistically significant
When subjects without diabetes of all ethnic groups were (P⫽0.94), but when each ethnic group was analyzed sepa-
combined, logistic regression analysis showed that age, race rately, insulin resistance was significantly associated with
(AA), BMI (or waist), and SI were significantly associated hypertension in NHW and H, but not AA (Figure 3).
Figure 2. The prevalence of hypertension by quartiles of fasting insulin (upper panels) and SI (lower panels) before (left) and after (right)
adjusting for age, sex, BMI, and minimum waist in subjects without diabetes in the 3 ethnic groups. The symbols correspond to the
median value in each quartile.
Downloaded from http://hyper.ahajournals.org/ by guest on May 17, 2015Saad et al Insulin Resistance and Hypertension 1327
TABLE 2. Logistic Regression Analysis Showing Variables Insulinemia, Insulin Resistance, and Hypertension
Associated with Hypertension in Subjects Without Diabetes in Subjects With Diabetes
(nⴝ1003) Hypertensive subjects with diabetes were older and more
Variable Odds Ratio (95% CI) P obese and had higher fasting glucose than their normotensive
counterparts. There was no significant difference, however,
Age (increase of 10 y) 1.98 (1.64–2.38) ⬍0.001
between normotensive and hypertensive subjects in waist,
Sex (M⫽1, F⫽2) 1.10 (0.81–1.49) 0.534
2-hour post-load glucose, insulinemia, or SI (Table 5). Hy-
Race 0.005 pertension was not related to fasting insulinemia or SI in any
AA vs NHW 2.00 (1.28–3.13) 0.002 of the 3 ethnic groups, before and after adjusting for age, sex,
AA vs H 2.49 (1.35–4.06) 0.004 BMI, and waist. When all subjects with diabetes were
BMI, increase of 1 kg/m2* 1.06 (1.03–1.09) ⬍0.001 combined, logistic regression showed that age, race (AA),
2-h glucose (increase of 1 mmol) 1.08 (0.99–1.18) 0.094 and BMI, but not insulinemia or SI were significantly asso-
SI (2-fold decrease)† 1.64 (1.28–2.10) 0.001 ciated with hypertension (Table 6).
Abbreviations are defined in the text.
*Could be replaced with minimum waist without a change in the strength of
Discussion
the model; a 1-cm increase in minimum waist was associated with an odds The association between insulin resistance and insulinemia
ratio of 1.03 (Cl:1.01–1.04; P⬍0.001). and hypertension is controversial. Whereas some studies
†Analyzed after log transformation of “SI⫹1” to circumvent the zero values reported that insulin resistance and/or hyperinsulinemia were
and to normalize the distribution; the interaction term between SI and ethnicity strongly related to hypertension, others show only a weak or
was not significant. even no association.7–27 Our data add some insights and show
that insulin resistance is at most a modest determinant of
hypertension and BP. This effect was not mediated by
Insulinemia, Insulin Resistance, and Blood insulinemia, which was significantly related to hypertension
Pressure in Subjects Without Diabetes only when SI was not included in the regression models. In
Because some antihypertensive drugs can affect insulin sen- addition, neither insulin resistance nor insulinemia was sig-
sitivity, the relation of insulinemia and insulin resistance with nificantly related to hypertension or BP in patients with
BP was examined in subjects without diabetes not receiving diabetes after controlling for age, sex, and obesity.
medications (n⫽773). SBP, DBP, and MBP correlated sig- Our data show that an increase in insulin resistance from
nificantly with fasting insulin and SI before and after adjust- the lowest to the highest quartile of the distribution in NHW
ing for age, sex, BMI, and waist (Table 3). When each ethnic and H was associated with a 70% higher likelihood of having
hypertension, an effect that was similar to a 10-year increase
group was considered separately, SBP, DBP, and MBP
in age. It is to be noted, however, that several antihyperten-
correlated significantly with fasting insulin and SI in NHW
sive medications could worsen insulin resistance33 and that
and H, but not in AA before and after adjusting for age, sex,
we could not estimate the effect of drugs because of the
BMI, and waist (Figure 4). Linear regression showed that
cross-sectional nature of the study. Furthermore, the number
age, male sex, BMI (or waist), fasting glucose, and SI were
of hypertensive subjects (⬇7%) not receiving medications
significant determinants of MBP (Table 4). When both SI and was too small to allow analyzing their data separately.
fasting insulin were included in the same model, SI but not Nonetheless, SI was weakly associated with BP in Hispanic
insulin was significantly associated with MBP. The interac- and NHW subjects without diabetes not receiving antihyper-
tion term between SI and ethnicity was not statistically tensive medications, explaining 2% to 4% of its variance.
significant (P⫽0.78), but when each ethnic group was ana- Figure 5 shows that a decrease in SI of 2 U (equivalent to change
lyzed separately, SI was significantly associated with MBP in from 20 to 80 percentile of the population) was associated with
H, but not in NHW or AA (Figure 4). Figure 5 shows the a 1.2-mm Hg increase in MBP in NHW and H.
estimated change in MBP in relation to insulin sensitivity as The relation between insulinemia and/or insulin resistance
predicted from a linear regression equation, adjusting for age, and BP appears to vary among ethnic groups. Nearly all
sex, BMI, and waist. studies showing a strong association between insulin and BP
were conducted among NHW. Studies in African Ameri-
cans,10,19,26 Hispanics,16 Nauruans, Pima Indians,15,25 and
Asian Indians18 showed a weak or no association. Even
among NHW, the association between insulinemia and BP
was inconsistent with some studies reporting a weak or
insignificant relationship.17,19 Similarly, when insulin resis-
tance was directly measured, the findings were discrepant.
Pooled European data showed a weak but significant associ-
ation between insulin resistance and BP.7 Saad et al25 found
insulin resistance and BP to be related in NHW, but not in AA
Figure 3. The odds ratio (with 95% CI) for having hypertension or Pima Indians. Falkner et al26 described insulin resistance in
in relation to a 2-fold increase in insulin resistance adjusting for
age, sex, BMI, and glycemia in all subjects without diabetes and young hypertensive AA men. Mattiasson et al27 showed that
in the 3 ethnic groups analyzed separately. insulin resistance and BP were related only in postmeno-
Downloaded from http://hyper.ahajournals.org/ by guest on May 17, 20151328 Hypertension June 2004
TABLE 3. Correlation Between Blood Pressure and Insulinemia and Insulin Resistance in Subjects Without Diabetes Not
Receiving Antihypertensive Medications
Fasting Insulin SI
Population SBP DBP MBP SBP DBP MBP
Simple Correlation
All 0.18 (⬍0.001) 0.19 (⬍0.001) 0.21 (⬍0.001) ⫺0.21 (⬍0.001) ⫺0.17 (⬍0.001) ⫺0.21 (⬍0.001)
NHW 0.19 (0.001) 0.23 (⬍0.001) 0.24 (⬍0.001) ⫺0.19 (0.001) ⫺0.17 (0.003) ⫺0.20 (⬍0.001)
AA ⫺0.02 (0.771) ⫺0.01 (0.944) ⫺0.02 (0.848) ⫺0.08 (0.298) ⫺0.04 (0.633) ⫺0.07 (0.412)
H 0.26 (⬍0.001) 0.23 (⬍0.001) 0.27 (⬍0.001) ⫺0.29 (⬍0.001) ⫺0.21 (0.001) ⫺0.28 (⬍0.001)
Partial Correlation (controlling for age, sex, BMI, and minimum waist)
All 0.10 (0.007) 0.12 (0.002) 0.12 (0.001) ⫺0.10 (0.009) ⫺0.10 (0.007) ⫺0.11 (0.003)
NHW 0.13 (0.027) 0.15 (0.012) 0.15 (0.009) ⫺0.10 (0.093) ⫺0.09 (0.125) ⫺0.10 (0.077)
AA ⫺0.10 (0.235) ⫺0.05 (0.512) ⫺0.08 (0.324) 0.01 (0.895) ⫺0.01 (0.940) 0.001 (0.983)
H 0.16 (0.010) 0.14 (0.022) 0.16 (0.008) ⫺0.15 (0.018) ⫺0.13 (0.035) ⫺0.15 (0.015)
The values of the correlation coefficient (r) are given with P values in parenthesis. Abbreviations are defined in the text.
pausal NHW women with IGT, but not in those with NGT. The mechanism through which insulin resistance is asso-
Our data unfortunately add to the confusion. We found SI to ciated with hypertension and BP is not known. It is thought
be related to hypertension and BP in H and NHW without that insulin resistance could cause hypertension through
diabetes, but not in AA. compensatory hyperinsulinemia.3 Insulin has been shown to
Figure 4. The relation between each of fasting insulinemia (upper panels) and SI (lower panels) and MBP in the 3 ethnic groups after
adjusting for age, sex, BMI, and minimum waist. The regression lines between fasting insulin and MBP in the 3 ethnic groups were not
different in the slope (P⫽0.0792) or the intercept (P⫽0.642). Likewise, the regression lines between SI and MBP in the 3 ethnic groups
were not different in the slope (P⫽0.435) or the intercept (P⫽0.675).
Downloaded from http://hyper.ahajournals.org/ by guest on May 17, 2015Saad et al Insulin Resistance and Hypertension 1329
TABLE 4. Linear Regression Analysis of Determinants of Mean
Blood Pressure in Subjects Without Diabetes Not Receiving
Antihypertensive Medications (nⴝ669)
Variable* B (95% Cl) R2 P
Age (increase of 10 y) 1.37 (0.61–2.13) 0.019 ⬍0.001
Sex (F⫽1, M⫽2) 2.60 (1.31–3.88) 0.015 ⬍0.001
Race 0.003 0.210
BMI (1 kg/m2)† 0.20 (0.06–0.34) 0.011 0.006
Fasting glucose, mmol/L 1.58 (0.41–2.75) 0.011 0.008
SI (2-fold decrease)‡ 1.25 (0.46–2.04) 0.014 0.002
Model R 2 ⫽ 0.106. Abbreviations defined in the text.
*Dependent variable: MBP.
†BMI and minimum waist were not included in the same model because
they were highly correlated (r⫽0.78), BMI could be replaced by minimum waist
without a change in the model strength (B⫽0.08, partial R 2⫽0.008). Figure 5. The relation between MBP and SI in the 3 ethnic
‡Analyzed after log transformation of SI⫹1 to circumvent the zero values groups as predicted from regression equations that included
age, sex, BMI, and waist in subjects without diabetes not
and to normalize the distribution; the interaction term between SI and ethnicity
receiving antihypertensive medications in the 3 ethnic groups
was not significant. analyzed separately (the means of age, BMI, and waist and male
sex were used).
stimulate the sympathetic nervous system, increase renal
sodium retention, modulate cation transport, and induce linked indirectly through mechanisms of an inherited or
hypertrophy of vascular smooth muscle (reviewed in 4). Our acquired nature. A possible link is through the sympathetic
data do not support this notion, however, because insulin was nervous system. Enhanced adrenergic tone may lead to
not independently related to hypertension or BP. In addition, increased insulin resistance on the one hand and a rise in BP
acute insulin infusion was found to have a vasodilator on the other. Ethnic or racial differences in sympathetic
hypotensive and not a hypertensive effect.5,6 It has been nervous system activity might explain the differences in the
relation of insulin resistance to BP. Increased levels of
known for years that insulin could lower BP substantially in
inflammatory markers such as tumor necrosis factor-␣ could
patients with diabetes with autonomic neuropathy.34 More-
contribute to both insulin resistance and endothelial dysfunc-
over, administration of insulin to individuals without35 and
tion37 and underlie the link between insulin resistance and
with36 diabetes does not cause a rise in BP in absence of hypertension. A further possibility is that a cellular or
hypoglycemia. It is plausible, however, that it is the resistance structural defect, genetic or acquired, may constitute the link
to the vasodilator effect of insulin that could lead to a rise in between insulin resistance and BP. Reduced activity of
BP. In addition, insulin resistance has been associated with sodium-potassium ATPase, decreased intracellular magne-
impaired endothelium-dependent vasodilatation,37 which sium, and increased sodium-lithium countertransport have
could contribute to increased BP. been proposed as possible links. Racial differences in ion
Alternatively, the association between insulin resistance regulation have been described and could account for the
and hypertension may not be causal. Instead, they may be observed variation in the relation of insulin resistance to BP.38
TABLE 5. Characteristics of Hypertensive and Nonhypertensive Subjects With Diabetes
NHW AA H P
Normotensive, Hypertensive, Normotensive, Hypertensive, Normotensive, Hypertensive,
Variable n⫽88 n⫽76 n⫽52 n⫽101 n⫽96 n⫽66 Ethnicity Hypertension
Age, y* 56⫾0.9 58⫾0.8 55⫾1.2 58⫾0.8 56⫾0.9 59⫾1.0 0.853 ⬍0.001
Sex, % F 48.9 50.0 58.1 58.4 54.2 65.2 0.241 0.778
BMI, kg/m2* 30.10⫾0.62 32.15⫾0.73 31.99⫾0.82 32.46⫾0.57 30.17⫾0.54 31.25⫾0.66 0.533 0.017
Minimum waist, cm* 99.0⫾1.5 101.1⫾1.6 98.6⫾1.5 99.5⫾1.2 97.0⫾1.18 99.1⫾1.5 0.312 0.101
SBP, mm Hg* 118⫾1.1 134⫾1.7 122⫾1.3 137⫾1.4 120⫾1.1 139⫾1.9 0.191 ⬍0.001
DBP, mm Hg* 74⫾0.7 81⫾1.0 76⫾0.9 83⫾1.0 74⫾0.8 80⫾1.1 0.135 ⬍0.001
Fasting glucose, mmol/L* 9.72⫾0.34 9.20⫾0.34 10.28⫾0.52 9.15⫾0.29 9.92⫾0.38 9.41⫾0.41 0.731 0.026
2-hour glucose, mmol/L* 16.95⫾0.44 17.21⫾0.53 17.38⫾0.71 16.75⫾0.44 18.23⫾0.58 17.92⫾0.64 0.186 0.698
Fasting insulin, pmol/L† 106 (92–122) 117 (98–140) 107 (91–126) 116 (102–131) 124 (111–139) 126 (110–144) 0.899 0.253
2-hour insulin, pmol/L† 361 (309–423) 403 (333–488) 375 (302–467) 444 (374–528) 490 (405–592) 456 (370–563) 0.235 0.410
SI⫻10⫺4 (min⫺1 䡠 U⫺1 䡠 mL⫺1)† 0.56 (0.41–0.72) 0.38 (0.27–0.50) 0.49 (0.37–0.61) 0.38 (0.28–0.48) 0.35 (0.26–0.45) 0.42 (0.28–0.58) 0.578 0.124
Abbreviations are defined in the text.
*Mean⫾SE is shown.
†Mean and 95% CI are shown
Downloaded from http://hyper.ahajournals.org/ by guest on May 17, 20151330 Hypertension June 2004
TABLE 6. Logistic Regression Analysis Showing Variables 6. Laakso M, Edelman SV, Brechtel G, Baron AD. Decreased effect of
Associated With Hypertension in Subjects With insulin to stimulate skeletal muscle blood flow in obese men: a novel
Diabetes (nⴝ479) mechanism for insulin resistance. J Clin Invest. 1990;85:1844 –1852.
7. Ferrannini E, Natali A, Capaldo B, Lehtovira M, Jacob S, Yki-Järvinen H,
Variable Odds Ratio, 95% CI P for the European Group for the Study of Insulin Resistance (EGIR).
Insulin resistance, hyperinsulinemia, and blood pressure. Role of age and
Age (increase of 10 y) 1.68 (1.32–2.16) ⬍0.001 obesity. Hypertension. 1997;30:1144 –1149.
Sex (M⫽1, F⫽2) 0.82 (0.65–1.22) 0.33 8. Manicardi V, Camellini L, Bellodi G, Coscelli C, Ferrannini E. Evidence
for an association of high blood pressure and hyperinsulinemia in obese
Race 0.04
men. J Clin Endocrinol Metab. 1986;62:1302–1304.
AA vs NHW 2.37 (1.39–4.04) 0.001 9. Rose HG, Yalow RS, Schweitzer E. Insulin as a potential factor influ-
AA vs H 3.25 (1.42–7.46) 0.005 encing blood pressure in amputees. Hypertension. 1986;8:793– 800.
10. Mbanya J-CN, Thomas TH, Wilkinson R, Alberti KGMM, Taylor R.
BMI (increase of 1 kg/m2)* 1.05 (1.02–1.09) 0.006 Hypertension and hyperinsulinemia: a relation in diabetes but not
Fasting glucose, mmol/L 0.95 (0.90–1.01) 0.131 essential hypertension. Lancet. 1988;1:733–734.
11. Verdecchia P, Gatteschi C, Benemio G, Guerrieri M, Porcellati C. Hy-
SI (2-fold decrease) 1.38 (0.48–1.94) 0.275 perinsulinemia and hypertension in diabetes. Lancet. 1988;2:242–244.
Abbreviations are defined in the text. 12. Zavaroni I, Mazza S, Dall’Aglio E, Gasparini P, Passseri M, Reaven GM.
*Minimum waist was not a significant predictor of hypertension in subjects Prevalence of hyperinsulinemia in patients with high blood pressure. J Int
with diabetes. Med. 1992;231:235–240.
13. Muscelli EOA, Saad MJA, Contijo JAR. Insulinemia and blood pressure
responses to oral glucose load in primary hypertensive patients. Cardi-
ology. 1991;79:14 –19.
Our data show that neither insulin resistance nor insuline- 14. Bonora E, Zavaroni I, Alpi O, Pezzarossa A, Bruschi F, Dall’Aglio E,
Guerra L, Coscelli C, Butturini U. Relationship between blood pressure
mia was related to hypertension in patients with diabetes of and plasma insulin in non-obese and obese non-diabetic subjects. Diabe-
any ethnic group. This is in agreement with those of Bonora tologia. 1987;30:719 –723.
et al39 who found no difference in insulin sensitivity between 15. Saad MF, Knowler WC, Pettitt DJ, Nelson RG, Mott DM, Bennett PH.
normotensive and hypertensive patients with diabetes. Laakso Insulin and hypertension: relationship to obesity and glucose intolerance
in Pima Indians. Diabetes. 1990;39:1430 –1435.
et al40 reported similar data in obese subjects with diabetes, 16. Haffner SM, Fong D, Hazuda HP, Pugh JA, Patterson JK. Hyperinsulin-
but found lean hypertensive patients with diabetes more emia, upper body adiposity, and cardiovascular risk factors in non-
insulin resistant than normotensive counterparts. This latter diabetics. Metabolism. 1988;37:338 –345.
17. Folsom AR, Burke GL, Ballew C, Jacobs DR Jr., Haskell WL, Donahue
study included only, however, a small number of lean
RP, Liu K, Hilner JE. Relation of body fatness and its distribution to
subjects with diabetes (11 hypertensive and 6 normotensive). cardiovascular risk factors in young blacks and whites; the role of insulin.
Thus, insulin resistance does not appear to be a feature of Am J Epidemiol. 1989;130:911–924.
hypertension in subjects with type 2 diabetes. 18. Nagi DK, Hendra TJ, Ryle AJ, Cooper TM, Temple RC, Clark PMS,
Eschneider AE, Hales CN, Yudkin JS. The relationship of concentrations
of insulin, intact proinsulin and 32–33 split proinsulin with cardiovascular
Perspectives risk factors in type 2 (non-insulin-dependent) diabetic subjects. Diabe-
The current study shows that insulin resistance, but not tologia. 1990;33:532–537.
insulinemia, was weakly but significantly related to hyper- 19. Manolio TA, Savage PJ, Burke GL, Liu K, Wagenknecht LE, Sidney S,
Jacobs DR Jr., Roseman JM, Donahue RP, Oberman A. Association of
tension and BP in subjects without diabetes. This weak fasting insulin with blood pressure and lipids in young adults: The
association argues against a major role for insulin resistance CARDIA study. Arteriosclerosis. 1990;10:430 – 436.
in the regulation of blood pressure or pathogenesis of hyper- 20. Pollare T, Lithell H, Berne C. Insulin resistance is a characteristic feature
of primary hypertension independent of obesity. Metabolism. 1990;39:
tension. This is especially true in individuals with type 2
167–174.
diabetes in whom neither insulin resistance nor insulinemia 21. Swislocki ALM, Hoffman BB, Reaven GM. Insulin resistance, glucose
were related to hypertension or BP. intolerance and hyperinsulinemia in patients with hypertension. Am J
Hypertens. 1989;2:419 – 423.
22. Shen D-C, Sheih S-M, Fuh MM-T, Wu D-A, Chen Y-DI, Reaven GM.
Acknowledgments Resistance to insulin-stimulated glucose-uptake in patients with hyper-
This study was supported by National Heart, Lung, and Blood tension. J Clin Endocrinol Metab. 1988;66:580 –583.
Institute grants U01-HL47887, U01-HL47889, U01-HL47892, 23. Cepaldo B, Lembo G, Napoli R, Rendina V, Albano G, Sacc L, Trimarco
and U01-HL47902. B. Skeletal muscle is a primary site of insulin resistance in essential
hypertension. Metabolism. 1991;40:1320 –1322.
24. Natali A, Santoro D, Palombo C, Cerri M, Ghione S, Ferrannini E.
References Impaired insulin action on skeletal muscle metabolism in essential hyper-
1. Welborn TA, Breckenridge A, Rubinstein AH, Dollery CT, Fraser TR. tension. Hypertension. 1991;17:170 –178.
Serum insulin in essential hypertension and in peripheral vascular disease. 25. Saad MF, Lillioja S, Nyomba BL, Castillo C, Ferraro R, DeGregorio M,
Lancet. 1966;1:1336 –1337. Ravussin E, Knowler WC, Bennett PH, Howard BV, Bogardus C. Racial
2. Ferrannini E, Buzzigoli G, Bonadonna R, Giorico MA, Oleggini M, differences in the relation between blood pressure and insulin resistance.
Graziadei L, Pedrinelli R, Brandi L, Bevilacqua S. Insulin resistance in N Engl J Med. 1991;324:733–739.
essential hypertension. N Engl J Med. 1987;317:350 –357. 26. Falkner B, Hulman S, Tannenbaum J, Kushner H. Insulin resistance and
3. Reaven GM, Hoffman BB. A role for insulin in the aetiology and course blood pressure in young black men. Hypertension. 1990;16:706 –711.
of hypertension. Lancet. 1987;2:435– 436. 27. Mattiasson I, Berntorp K, Lindgarde F. Insulin resistance and Na⫹/K(⫹)-
4. Reaven GM, Lithell H, Landsberg L. Hypertension and associated met- ATPase in hypertensive women: a difference in mechanism depending on
abolic abnormalities–the role of insulin resistance and the sympathoa- the level of glucose tolerance. Clin Sci (Lond). 1992;82:105–111.
drenal system. N Engl J Med. 1996;334:374 –381. 28. Wagenknecht LE, Mayer EJ, Rewers M, Haffner SM, Selby J, Borok
5. Creager MA, Liang C-S, Coffman JD. Beta adrenergic-mediated vaso- GM, Henkin L, Howard G, Savage PJ, Saad MF, Bergman RN, Hamman
dilator response to insulin in the human forearm. J Pharmacol Exp Ther. R. The Insulin Resistance Atherosclerosis Study (IRAS): objectives,
1985;235:709 –714. design, and recruitment results. Ann Epidemiol. 1995;5:464 – 471.
Downloaded from http://hyper.ahajournals.org/ by guest on May 17, 2015Saad et al Insulin Resistance and Hypertension 1331
29. Pacini G, Bergman RN. MINMOD: a computer program to calculate 34. Page M McB, Watkins PJ. Provocation of postural hypotension by insulin
insulin sensitivity and pancreatic responsitivity from the frequently in diabetic autonomic neuropathy. Diabetes. 1976;25:90 –95.
sampled intravenous glucose tolerance test. Comput Methods Programs 35. Heise T, Magnusson K, Heinemann L, Sawicki PT. Insulin resistance and
Biomed. 1986;23:113–122. the effect of insulin on blood pressure in essential hypertension. Hyper-
30. Welch S, Gebhart SSP, Bergman RN, Phillips LS. Minimal model anal- tension. 1998;32:243–248.
ysis of intravenous glucose tolerance derived insulin sensitivity in 36. Genev NM, Lau IT, Willey KA, Molyneaux LM, Xu ZR, Zilkens RR,
diabetic subjects. J Clin Endocrinol Metab. 1990;71:1508 –1518. Wyndham RN, Yue DK. Does insulin therapy have a hypertensive effect
31. Saad MF, Anderson RL, Laws A, Watanabe R, Kades WW, Chen Y-DI, in type 2 diabetes. J Cardiovascular Pharmacol. 1998;32:39 – 41.
Sands RE, Savage PJ, Bergman RN. A comparison between the minimal
37. Wheatcroft SB, Williams IL, Shah AM, Kearney MT. Pathophysiological
model and the glucose clamp techniques in the assessment of insulin
implications of insulin resistance on vascular endothelial function. Diabet
sensitivity across the spectrum of glucose tolerance. Diabetes. 1994;43:
Med. 2003;20:255–268.
1114 –1121.
32. Coates PA, Luzio SD; Brunel P, Owens DR. Comparison of estimates of 38. Aviv A, Gardner J. Racial difference in ion regulation and their possible
insulin sensitivity from minimal model analysis of the insulin-modified links to hypertension in Blacks. Hypertension. 1989;14:584 –589.
frequently sampled intravenous glucose tolerance test and the iso- 39. Bonora E, Bonadonna RC, Del Prato S, Gulli G, Solini A, Matsuda M,
glycemic hyperinsulinemic clamp in subjects with NIDDM. Diabetes. DeFronzo RA. In vivo glucose metabolism in obese and type 2 diabetic
1995;44:631– 635. subjects with or without hypertension. Diabetes. 1993;42:764 –772.
33. Pollare T, Lithell H, Berne CN. A comparison of the effects of hydrochlo- 40. Laakso M, Sarlund H, Mykkanen L. Essential hypertension and insulin
rothiazide and captopril on glucose and lipid metabolism in patients with resistance in non-insulin-dependent diabetes. Eur J Clin Invest. 1989;19:
hypertension. N Engl J Med. 1989;321:868 – 873. 518 –526.
Downloaded from http://hyper.ahajournals.org/ by guest on May 17, 2015Insulin Resistance and Hypertension: The Insulin Resistance Atherosclerosis Study
Mohammed F. Saad, Marian Rewers, Joseph Selby, George Howard, Sujata Jinagouda, Salwa
Fahmi, Dan Zaccaro, Richard N. Bergman, Peter J. Savage and Steven M. Haffner
Hypertension. 2004;43:1324-1331; originally published online May 3, 2004;
doi: 10.1161/01.HYP.0000128019.19363.f9
Hypertension is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 2004 American Heart Association, Inc. All rights reserved.
Print ISSN: 0194-911X. Online ISSN: 1524-4563
The online version of this article, along with updated information and services, is located on the
World Wide Web at:
http://hyper.ahajournals.org/content/43/6/1324
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published
in Hypertension can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial
Office. Once the online version of the published article for which permission is being requested is located,
click Request Permissions in the middle column of the Web page under Services. Further information about
this process is available in the Permissions and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Hypertension is online at:
http://hyper.ahajournals.org//subscriptions/
Downloaded from http://hyper.ahajournals.org/ by guest on May 17, 2015You can also read