INSIDIOUS COGNITIVE DECLINE IN CADASIL - KAARINA AMBERLA, MSC; MINNA WA LJAS, MSC; SUSANNA TUOMINEN, MD; OVE ALMKVIST, PHD; MINNA PO YHO NEN, MD; ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Insidious Cognitive Decline in CADASIL
Kaarina Amberla, MSc; Minna Wäljas, MSc; Susanna Tuominen, MD; Ove Almkvist, PhD;
Minna Pöyhönen, MD; Seppo Tuisku, MD; Hannu Kalimo, MD; Matti Viitanen, MD
Background and Purpose—Cerebral autosomal-dominant arteriopathy with subcortical infarcts and leukoencephalopathy
(CADASIL) causes repeated ischemic attacks leading to subcortical vascular dementia. The aim of this study was to
characterize cognitive function in subjects with a C475T (R133C) mutation in the Notch3 gene, leading to CADASIL.
Methods—Prestroke (n⫽13) and poststroke (n⫽13) mutation carriers and mutation carriers with dementia (n⫽8) were
compared with healthy noncarriers from the same families using a comprehensive set of neuropsychological tests.
Results—Changes in working memory and executive function were observed in the very early phase of the disease before
transient ischemic attack (TIA) or stroke. Later, in the poststroke phase, the cognitive impairment concerned also mental
speed and visuospatial ability. Finally, the subjects with dementia had multiple cognitive deficits, which engaged even
verbal functions, verbal episodic memory, and motor speed. The 2 mutation carrier groups without dementia and the
controls could be reliably distinguished using 3 tests that assessed working memory/attention, executive function, and
mental speed. Episodic memory was relatively well-preserved late in the disease.
Conclusion—A deterioration of working memory and executive function was already observed in the prestroke phase,
which means that cognitive decline may start insidiously before the first onset of symptomatic ischemic episodes.
(Stroke. 2004;35:1598-1602.)
Key Words: CADASIL 䡲 neuropsychology 䡲 vascular diseases 䡲 small vessel disease
C erebral autosomal-dominant arteriopathy with subcorti-
cal infarcts and leukoencephalopathy (CADASIL) is a
generalized small-vessel disease caused by mutations in the
carriers compared with controls from the same family.6
Another study showed in 2 of 8 symptomatic, but not
demented, patients a clear cognitive decline already before
Notch3 gene on chromosome 19. The Notch3 gene encodes any major vascular event, suggesting early cognitive impair-
Notch3 receptor protein that is expressed in adults only on ment.7 In both studies, the pattern of cognitive decline
vascular smooth muscle cells (SMC). Mutated Notch3 in- indicated frontal lobe and subcortical involvement, but the
duces destruction of these SMCs with parallel deposition of results are somewhat contradictory with respect to how early
granular osmiophilic material (GOM) and fibrosis.1 These the cognitive decline becomes manifest. Also, the low num-
arterial changes result in decreased cerebral blood flow ber of subjects has hampered the power of these studies.
(CBF), especially in the white matter,2– 4 and consequent Larger subject groups in different phases of the disease need
periventricular white matter degeneration and lacunar infarcts to be examined to get a more reliable description of the
in deep white matter and basal ganglia.1,4 The natural course pattern of cognitive decline in CADASIL. We performed a
of CADASIL is variable. Recurrent transient ischemic attacks cross-sectional study of 34 genetically confirmed carriers of
(TIA) and strokes are the main manifestations. One third of the same Notch3 mutation. We describe the pattern of
the patients have migraine headache and one fifth have mood cognitive function in 3 different phases of the disease. We
disorders, these being mostly depression or anxiety.1 focused on the early signs of cognitive decline and compared
The cumulative brain lesions lead to insidious cognitive nondemented mutation carriers with 15 healthy nonmutation
decline, the progression of which to subcortical dementia is carriers from the same kindreds.
still poorly known. There have been only a few studies
concerning the pattern of decline in cognitive functions in the Subjects and Methods
different phases of the disease. In 1 study, no evidence was Thirty-four subjects from 8 Finnish families were genetically con-
found for cognitive decline in 5 asymptomatic mutation firmed to carry the same C475T (R133C) mutation in exon 3 of the
Received September 17, 2003; accepted March 18, 2004.
From the Division of Clinical Geriatrics (K.A., O.A., M.V.), Karolinska Institutet, Stockholm, Sweden; Tampere University Hospital (M.W.),
Department of Neurosurgery, Finland; Department of Psychology (O.A.), Stockholm University, Stockholm, Sweden; the Department of Medical
Genetics (M.P.), Family Federation of Finland, Helsinki, Finland; the Keski-Pohjanmaa Central Hospital (S.Tuisku), Kokkola, Finland; the Departments
of Neurology (S.Tuominen) and Pathology (H.K.), Turku University Hospital, Turku, Finland; the Department of Pathology (H.K.), Uppsala University
and University Hospital, Uppsala, Sweden; the Department of Pathology (H.K.), University Hospital of Helsinki, Helsinki, Finland; and the Department
of Geriatric Medicine (M.V.), University of Turku, Finland.
Correspondence to Matti Viitanen, Division of Clinical Geriatrics, Karolinska Institutet, Huddinge University Hospital, S-14186 Stockholm, Sweden.
E-mail matti.viitanen@neurotec.ki.se
© 2004 American Heart Association, Inc.
Stroke is available at http://www.strokeaha.org DOI: 10.1161/01.STR.0000129787.92085.0a
1598
Downloaded from http://stroke.ahajournals.org/ by guest on October 23, 2015Amberla et al Cognitive Impairment in CADASIL 1599
TABLE 1. Demographic Characteristics of Healthy Controls and the 3 Mutation
Carrier Groups
Subjects
Controls Prestroke Poststroke Dementia
N (female/male) 15 (5/10) 13 (5/8) 13 (4/9) 8 (3/5)
Age (y) 39.5⫾10.8 39.3⫾11.0 48.7⫾6.9 54.5⫾5.8
Education (y) 12.1⫾4.3 10.2⫾3.5 9.3⫾3.5 6.5⫾0.9
Migraine (frequency) 2/15 7/13 9/13 3/8
Mood change (frequency) 0 5/13 6/13 3/8
Notch3 gene. All had typical periventricular white matter changes on Results
T2-weighted magnetic resonance imaging (MRI). The controls
(n⫽15) were genetically confirmed to be negative for the mutation Demographics
and they showed no pathological findings on MRI. Information In Table 1, the demographic data for the 4 groups are
about the history of TIA and stroke as well as occurrence of migraine presented. The mean age of the poststroke and dementia
and mood changes was collected through semistructured interviews groups was significantly higher (P⬍0.001) than that of the
of the subjects and close informants as well as from medical files.
The mutation carriers were divided into 3 groups defined by control and prestroke groups. The latter 2 groups did not
occurrence of clinical ischemic symptoms and dementia. The pre- differ from each other. The mean level of education differed
stroke group (n⫽13) comprised subjects without TIA, stroke, or significantly (P⬍0.001) between the dementia group versus
dementia. The poststroke group (n⫽13) included subjects who had control and prestroke and poststroke groups, but there was no
experienced at least 1 cerebrovascular ischemic symptom but were significant difference between the latter 3 groups.
not demented. Subjects in the dementia group (n⫽8) fulfilled the
DSM-III-R criteria for dementia and 6 of them had had 1 or more
strokes. Impairment in the Cognitive Performance in
Different Phases of the Disease
Neuropsychological Assessment The prestroke group performed poorer than controls in 3
The neuropsychological examination included the following tests: tests: digit span forward (P⬍0.05), digit span backward
similarities, block design, digit symbol, digit span total score, digit (P⬍0.001), and Rey–Osterreith memory test (P⬍0.001). The
span forwards, and digit span backwards from the Wechsler Adult poststroke CADASIL subjects performed more poorly than
Intelligence Scale-Revised (WAIS-R),8 letter fluency (FAS),9 Trail-
Making Test, parts A and B (TMTA, TMTB;10 number of correct prestroke subjects in 4 tests: number correct responses
responses and log-transformed time score), Luria clock-setting and (P⬍0.01), log time (P⬍0.01) of TMTB, digit symbol
clock-reading test,11 Rey–Osterreith copying12 and Rey–Osterreith (P⬍0.001), and the block design test (P⬍0.01). Unexpect-
memory, immediate reproduction,10 Rey Auditory Verbal Learning edly, the poststroke group performed almost as well as the
Test (RAVLT;10 total learning and 30-minute delayed recall), word controls.
recall (number of correct responses) and recognition (d-prime-
integrated measure of current and false recognitions) from Stock- In the dementia group, only 11 of the 21 neuropsycholog-
holm Gerontology Research Center (SGRC),13 and finger-tapping ical tests could be administered because of the severity of the
for dominant, nondominant, and alternating hands.14 cognitive impairment. In 8 of these 11 tests, the dementia
Six mutation carriers and 4 controls were tested in the late 1980s group differed from all the other groups. Only in a single test,
and early 1990s at the Department of Neurology of Oulu University clock-setting, did the groups not differ from each other. For
Hospital. The remaining 28 mutation carriers and 11 controls were
examined between 1997 to 1999 at the Department of Neurology of detailed comparisons between the groups, see Table 2.
Keski-Pohjanmaa Central Hospital and Turku University Hospital by
2 neuropsychologists (K.A. and M.W.). Of the mutation carriers, 14 Discriminant Analysis
had a history of mood changes but none of them had severe Using all neuropsychological tests, a stepwise discriminant
depression according to clinical evaluation at the time of the analysis was performed on control, prestroke, and poststroke
neuropsychological investigation. Nineteen of the 34 mutation car- groups. This analysis resulted in 2 significant discriminant
riers had a history of migraine and 1 had experienced epileptic
seizures. functions (P⬍0.001) in 3 tests: Rey–Osterreith memory, digit
The joint Ethical Committee of Turku University Hospital and span backwards, and digit symbol, which are primarily
University of Turku approved the study. associated with executive function, working memory, and
mental speed. The first discriminant function explained 79%
Statistical Methods of the variance and was associated with low performance in
Groups were compared by 1-way ANOVA or with ANCOVA when 2 tests to approximately the same extent (standardized coef-
possible confounding factors (age and education) were included.
Sheffé test was used for the post-hoc analysis. Because of the ficients 0.63 for Rey–Osterreith memory and 0.69 for digit
exploratory nature of this study, P⬍0.05 was regarded as a differ- span backwards). The second discriminant function explained
ence and no correction for multiple testing was performed. Stepwise 21% of the variance and was associated with high perfor-
discriminant analysis with Wilks lambda as criterion was used to find mance in digit symbol (standardized coefficient ⫺0.74)
the best combination of tests to separate groups of nondemented compared with the performance in Rey–Osterreith memory
mutation carriers and controls. Cross-validation of classification of
cases was performed using jack-knife procedure (each case is (0.32) and digit span backwards (0.50). The first discriminant
classified by functions derived from all cases other than that case). function differentiated the poststroke group from the pre-
All analyses were performed using SPSS version 11.0. stroke and control groups by low level of cognitive perfor-
Downloaded from http://stroke.ahajournals.org/ by guest on October 23, 20151600 Stroke July 2004
TABLE 2. Neuropsychological Test Results (meanⴞSD) in Healthy Controls and Prestroke,
Stroke, and Dementia Groups of CADASIL Patients
Subjects
Neuropsychological Tests Controls Prestroke Poststroke Dementia
Similarities 21.5⫾3.4 21.2⫾3.0 20.9⫾4.1 3 8.0⫾4.9
FAS letter fluency 44.7⫾8.6 36.9⫾12.8 35.8⫾14.6 3 10.0⫾4.2
Clock-reading, # corr 5.0⫾0.0 4.9⫾0.3 4.5⫾1.0 3 3.3⫾0.9
Clock-setting, # corr 4.7⫾0.6 4.4⫾0.8 4.5⫾0.9 3.8⫾1.2
R-O copying 35.2⫾0.8 33.5⫾2.0 32.2⫾4.1 na
Block design 31.9⫾2.8 36.0⫾4.4 3 30.0⫾5.4 3 9.9⫾4.7
TMTA, log time (sec) 1.5⫾0.2 1.5⫾0.2 1.7⫾0.2 3 2.5⫾0.2
TMTB, # corr 24.0⫾0.0 23.8⫾0.8 3 17.5⫾6.6 na
TMTB, log time (sec) 1.9⫾0.2 2.0⫾0.2 3 2.2⫾0.2 na
Digit symbol 42.1⫾10.0 49.0⫾7.6 3 28.0⫾5.3 na
Digit span, total 14.9⫾3.8 12.7⫾2.1 13.4⫾2.0 3 7.1⫾2.8
Digit span forward 6.9⫾1.1 3 6.0⫾0.9 6.2⫾0.4 na
Digit span backward 5.9⫾1.0 3 4.7⫾0.5 4.3⫾0.8 na
RAVL learning 49.1⫾9.3 47.6⫾7.6 43.2⫾9.7 na
RAVL retention 10.9⫾2.5 9.9⫾2.3 8.9⫾2.7 na
SGRC recall, # corr 8.1⫾1.4 7.1⫾1.8 6.8⫾1.0 3 4.8⫾1.0
SGRC recognition, d-prime 3.3⫾1.1 3.4⫾0.9 2.6⫾0.9 2.3⫾0.5
R-O memory 27.7⫾2.8 3 20.9⫾5.6 16.8⫾6.5 na
Finger-tapping, dominant 57.8⫾10.2 60.2⫾8.2 52.0⫾8.0 3 32.8⫾7.1
Finger-tapping, nondominant 50.6⫾7.4 53.0⫾6.0 48.8⫾8.1 40.8⫾14.0
Finger-tapping, alternating 87.0⫾13.2 91.0⫾29.0 84.9⫾16.7 na
na indicates not assessed; 3, pair-wise difference between the groups; # corr, number of correct reponses; R-O,
Rey–Osterreith; TMTA, Trail Making Test A; TMTB, Trail Making Test B; RAVL, Rey Auditory Verbal Learning; SGRC,
Stockholm Gerontology Research Center.
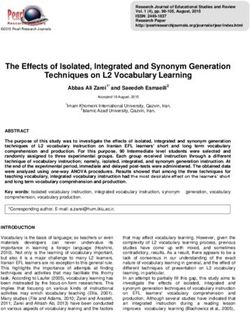
mance in general. In the second discriminant function, there digit span backwards (P⬍0.01 and P⬍0.05, respectively).
was a contrast between high performance in the test of mental Among the prestroke subjects, 3 were misclassified (2 were
speed (digit symbol) and low performance in the 2 tests misclassified as controls because they performed as well as
assessing aspects of executive function and working memory the those in the control group in the Rey–Osterreith memory
(Rey–Osterreith memory and digit span backwards). This test; P⬍0.001). In summary, misclassification of individuals
function primarily differentiated the control group with intact was related to patterns of relative performance as demon-
cognitive performance from the prestroke group, which had strated by a scatter-plot of all prestroke and poststroke
lower performance in the tests of executive function. subjects and the controls in terms of the 2 discriminant
The combination of the 3 tests (Rey–Osterreith memory, functions (Figure 1).
digit span backwards, and digit symbol) correctly classified
85% of all subjects included. After cross-validation, 78%
Discussion
were correctly classified (Table 3). When correctly and Cognitive decline could be observed very early during the
incorrectly classified subjects were compared, 3 of 15 con- course of CADASIL as shown in the prestroke and poststroke
trols were misclassified as prestroke subjects because of groups. The performance of the prestroke group was poorer
poorer performance in the Rey–Osterreith memory test and than that of the controls in 3 cognitive domains: short-term
memory (digit span forwards), working memory (digit span
TABLE 3. Classification (Original/Cross-Validated) of Subjects backwards), and executive function (Rey–Osterreith mem-
According to Discriminant Analysis of CADASIL Subjects
ory), because of poor strategy and planning in completing the
Without Dementia and the Controls
task. The cognitive domain, which distinguished prestroke
Classification from the poststroke group, was mental slowing as verified by
Diagnostic Group Controls Prestroke Poststroke Total poor results in digit symbol and TMTB time and set-shifting
ability (TMTB, number correct responses). This pattern of
Control subjects 12/11 3/4 0/0 15
cognitive decline was also confirmed by the discriminant
Prestroke patients 2/3 10/9 1/1 13
analysis in which tests of working memory (digit span
Poststroke patients 0/0 0/1 13/12 13
backwards), executive function (Rey–Osterreith memory),
Downloaded from http://stroke.ahajournals.org/ by guest on October 23, 2015Amberla et al Cognitive Impairment in CADASIL 1601
in basal ganglia.5 These changes are in accordance with the
more severe of the cognitive impairment in later phases of
CADASIL. The frontal involvement became more accentu-
ated in the poststroke subjects, as indicated by poorer perfor-
mance in tests measuring mental speed (digit symbol) and
set-shifting ability (TMTB, number correct). Also in the
subjects with dementia, cognitive impairment still showed
predominantly frontal–subcortical involvement, whereas cog-
nitive functions associated with posterior regions were less
affected. This type of cognitive decline is also seen in other
diseases with frontal subcortical involvement, such as other
stroke-related dementias, Huntington disease, and multiple
sclerosis.22
In previous clinical studies of CADASIL, the focus has
mostly been on the poststroke and dementia phases of the
disease.6,7,23–25 Of the 2 studies mentioned, Taillia et al7
showed results concordant with ours. Their 8 symptomatic
Scatter-plot of root values from a discriminant analysis of all
nondemented subjects. *Two controls with the same values.
(TIA, stroke, migraine or seizures) CADASIL patients with-
out dementia had significantly impaired performance in
Wisconsin Card Sorting Test, trail-making test, and Rey–
and mental speed (digit symbol) determined the classification
Osterreith copying. Two of them showed cognitive decline
of the prestroke and poststroke subjects and controls.
without having had TIA or stroke. This is in accordance with
It was unexpected that motor speed (finger-tapping domi-
the results for our prestroke group. In accordance with our
nant, nondominant, and alternating hands) did not distinguish
study, the decline began with deterioration in tests associated
the prestroke and poststroke groups from the control group,
with executive function, attention, and mental speed. How-
because motor slowing is considered to be a common
ever, the results of Trojano et al6 differ from those of our
symptom in stroke-related dementia disorders.15 In concor-
prestroke subjects. In a 2-year follow-up study, Trojano et al6
dance with other vascular dementias, verbal episodic memory
did not find any significant differences in cognitive perfor-
was not significantly impaired in the prestroke and poststroke
mance between the controls and 5 asymptomatic CADASIL
groups compared with the controls. This is in contrast to its
patients.
early appearance in Alzheimer disease.
In our study, the groups differed significantly with respect
The dementia group demonstrated considerable decline in to age and length of education. The age difference between
multiple cognitive domains, which is in accordance with the the patient groups is explained by the progressive nature of
clinical picture of CADASIL.16,17 Interestingly, in 3 tests the disease; therefore, the 2 symptomatic groups are older.
(SGRC word recognition, finger-tapping dominant hand, and The difference in years of education was caused by a cohort
clock-setting) there was no difference compared with the effect, with the oldest subjects being less educated as com-
other groups, suggesting that episodic memory, motor speed, pared with the younger ones. However, when age and
and visuospatial ability are relatively spared late in the education were controlled for, the group differences remained
disease development. The cognitive impairment in the de- unchanged. Importantly, the prestroke group and controls did
mentia group corresponded to early frontal–subcortical vas- not differ for age or education, thus supporting our findings of
cular dementia, in which episodic memory is relatively subclinical cognitive impairment in CADASIL without con-
well-preserved, showing predominantly difficulties of re- founding effects of demographic variables. In our material,
trieval and less decline in encoding and storage. This is in frequencies of mood change (39%) and migraine (54%) were
agreement with previous research.7,18 somewhat higher than reported earlier.17,26 However, none of
Hypothetically, the pattern of cognitive impairment in our subjects had depression according to clinical evaluation at
various phases of CADASIL can be associated with dysfunc- the time of the neuropsychological investigation. Although
tion in certain brain regions. The early decline in Rey– there is some evidence of cognitive impairment in persons
Osterreith memory and digit span forwards and backwards with life-long migraine,27,28 in our patients, history of mi-
may reflect a common underlying insufficiency of working graine or mood change did not significantly associate with
memory and executive function. Experimental studies have cognitive performance. There was also an overrepresentation
demonstrated an association between prefrontal structures of men among our subjects (approximately two thirds), which
and working memory capacity.19 Deterioration of executive deviates from that generally seen in CADASIL.17 The de-
function has also been associated with decreased activity in mentia group was small and the subjects were severely
the prefrontal cortex.20 Concordantly, the cerebral blood flow impaired and not able to perform all the tests. This may limit
in frontal white matter is decreased already in the prestroke the power of comparison with the other groups.
phase and degeneration of the white matter is already detect- In conclusion, our findings indicate that the cognitive
able by MRI.4,21 In the progression of the disease, white decline in CADASIL begins before the first TIA or stroke. It
matter lesions were more extended in the periventricular can be detected as an impaired performance in neuropsycho-
areas. Lacunar infarcts are also seen in deep white matter and logical tests of working memory, executive function, and
Downloaded from http://stroke.ahajournals.org/ by guest on October 23, 20151602 Stroke July 2004
mental speed. The most sensitive tests to detect cognitive 10. Lezak M. Neuropsychological Assessment. New York: Oxford University
decline in CADASIL appear to reflect frontal subcortical Press; 1995.
11. Christensen AL. Luria’s Neuropsychological Investigation. Copenhagen:
involvement. Cognitive impairment begins with deterioration Munksgaard; 1979.
of executive functions and working memory/attention in the 12. Rey A. L’examen psychologique dans les cas d’encéphalopathie trau-
asymptomatic prestroke phase, an impairment of mental matique. Archives de Psychologie. 1941;28:286 –340.
13. Bäckman L, Forsell Y. Episodic memory functioning in a
speed and visuospatial ability are seen in the poststroke community-based sample of very old adults with major depression:
phase. Finally, multiple deficits of cognition including verbal utilisation of cognitive support. J Abnorm Psychol. 1994;103:361–370.
functions, verbal episodic memory, and motor speed are 14. Iregren A, Gamberale F, Kjellberg A. SPES: a psychological test system
observed in the patients who fulfill the criteria of dementia. to diagnose environmental hazards. Neurotoxicol Teratol. 1996;18:
485– 491.
15. Cummings JL. Vascular subcortical dementias: clinical aspects.
Acknowledgments Dementia. 1994;5:177–180.
The study was financially supported by Gamla Tjänarinnor, Gros- 16. Chabriat H, Vahedi K, Iba-Zizen MT, Joutel A, Nibbio A, Nagy TG,
chinsky, and Bertil Stohne foundations, the Academy of Finland, Krebs MO, Julien J, Dubois B, Ducrocq X, Levasseur M, Homeyer P,
project 50046, Sigrid Juselius Foundation, EVO research Funds of Mas JL, Lyon-Caen O, Tournier Lasserve E, Bousser MG. Clinical
Turku University Hospital, Turku University Foundation, Neurology spectrum of CADASIL: a study of 7 families. Cerebral autosomal
Foundation, Finnish Cultural Foundation. We express our gratitude dominant arteriopathy with subcortical infarcts and leukoencephalopathy.
to Professor Vilho Myllylä, MD and Helinä Mononen, MSc, Depart- Lancet. 1995;346:934 –939.
ment of Neurology, Oulu University Hospital for their engagement 17. Dichgans M, Mayer M, Uttner I, Bruning R, Muller-Hocker J, Rungger
G, Ebke M, Klockgether T, Gasser T. The phenotypic spectrum of
in our study and for providing us with valuable material
CADASIL: clinical findings in 102 cases. Ann Neurol. 1998;44:731–739.
and information.
18. Wentzel C, Darvesh S, MacKnight C, Shea C, Rockwood K. Inter-rater
reliability of the diagnosis of vascular cognitive impairment at a memory
References clinic. Neuroepidemiology. 2000;19:186 –193.
1. Kalimo H, Ruchoux MM, Viitanen M, Kalaria RN. CADASIL: a 19. Levy R, Goldman-Rakic PS. Segregation of working memory functions
common form of hereditary arteriopathy causing brain infarcts and within the dorsolateral prefrontal cortex. Exp Brain Res. 2000;133:23–32.
dementia. Brain Pathol. 2002;12:371–384. 20. Cabeza R, Nyberg L. Imaging cognition II: an empirical review of 275
2. Chabriat H, Pappata S, Ostergaard L, Clark CA, Pachot-Clouard M, PET and fMRI studies. J Cogn Neurosci. 2000;12:1– 47.
Vahedi K, Jobert A, Le Bihan D, Bousser MG. Cerebral hemodynamics 21. Chabriat H, Pappata S, Poupon C, Clark CA, Vahedi K, Poupon F,
in CADASIL before and after acetazolamide challenge assessed with Mangin JF, Pachot-Clouard M, Jobert A, Le Bihan D, Bousser MG.
MRI bolus tracking. Stroke. 2000;31:1904 –1912. Clinical severity in CADASIL related to ultrastructural damage in white
3. Bruening R, Dichgans M, Berchtenbreiter C, Yousry T, Seelos KC, Wu matter. In vivo study with diffusion tensor MRI. Stroke. 1999;30:
RH, Mayer M, Brix G, Reiser M. Cerebral autosomal dominant arteri- 2637–2643.
opathy with subcortical infarcts and leukoencephalopathy: decrease in 22. Butters MA, Goldstein G, Allen DN, Shemansky WJ. Neuropsycho-
regional cerebral blood volume in hyperintense subcortical lesions logical similarities and differences among Huntington’s disease, multiple
inversely correlates with disability and cognitive performance. Am J sclerosis, and cortical dementia. Arch Clin Neuropsychol. 1998;13:
Neuroradiol. 2001;22:1268 –1274. 721–735.
4. Tuominen S, Miao Q, Kurki T, Tuisku S, Pöyhönen M, Kalimo H, 23. Adair JC, Hart BL, Kornfeld M, Graham GD, Swanda RM, Ptacek LJ,
Viitanen M, Sipilä HT, Bergman J, Rinne JO. Positron emission Davis LE. Autosomal dominant cerebral arteriopathy: neuropsychiatric
tomography examination of cerebral blood flow and glucose metabolism syndrome in a family. Neuropsychiatry Neuropsychol Behav Neurol.
in young CADASIL patients. Stroke. 2004;35:1063–1067. 1998;11:31–39.
5. Chabriat H, Levy C, Taillia H, Iba-Zizen MT, Vahedi K, Joutel A, 24. Desmond DW, Moroney JT, Lynch T, Chan S, Chin SS, Shungu DC,
Tournier-Lasserve E, Bousser MG. Patterns of MRI lesions in CADASIL. Naini AB, Mohr JP. CADASIL in a North American family: clinical
Neurology. 1998;51:452– 457. pathologic and radiologic findings. Neurology. 1998;51:844 – 849.
6. Trojano L, Ragno M, Manca A, Caruso G. A kindred affected by cerebral 25. Harris JG, Filley CM. CADASIL: neuropsychological findings in three
autosomal dominant arteriopathy with subcortical infarcts and leukoen- generations of an affected family. J Int Neuropsychol Soc. 2001;7:
cephalopathy (CADASIL): a 2-year neuropsychological follow-up. 768 –774.
J Neurol. 1998;245:217–222. 26. Desmond DW, Moroney JT, Lynch T, Chan S, Chin SS, Mohr JP. The
7. Taillia H, Chabriat H, Kurtz A, Verin M, Levy C, Vahedi K, Tournier- natural history of CADASIL. A pooled analysis of previously published
Lasserve E, Bousser MG. Cognitive alterations in non-demented cases. Stroke. 1999;30:1230 –1233.
CADASIL patients. Cerebrovasc Dis. 1998;8:97–101. 27. Waldie KE, Hausmann M, Milne BJ, Poulton R. Migraine and cognitive
8. Wechsler D. Wechsler Adult Intelligence Scale, Revised: Manual. New function. A life-course study. Neurology. 2002;59:904 –908.
York: Harcourt Brace, Jovanovich; 1981. 28. Calandre EP, Bembibre J, Arnedo ML, Becerra D. Cognitive disturbances
9. Spreen O, Benton AL. Neurosensory Center Comprehensive Examination and regional cerebral blood flow abnormalities in migraine patients: their
for Aphasia. Victoria, BC: University of Victoria Neuropsychological relationship with the clinical manifestations of the illness. Cephalalgia.
Laboratory; 1977. 2002;22:291–302.
Downloaded from http://stroke.ahajournals.org/ by guest on October 23, 2015Insidious Cognitive Decline in CADASIL
Kaarina Amberla, Minna Wäljas, Susanna Tuominen, Ove Almkvist, Minna Pöyhönen, Seppo
Tuisku, Hannu Kalimo and Matti Viitanen
Stroke. 2004;35:1598-1602; originally published online May 13, 2004;
doi: 10.1161/01.STR.0000129787.92085.0a
Stroke is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 2004 American Heart Association, Inc. All rights reserved.
Print ISSN: 0039-2499. Online ISSN: 1524-4628
The online version of this article, along with updated information and services, is located on the
World Wide Web at:
http://stroke.ahajournals.org/content/35/7/1598
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published
in Stroke can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.
Once the online version of the published article for which permission is being requested is located, click
Request Permissions in the middle column of the Web page under Services. Further information about this
process is available in the Permissions and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Stroke is online at:
http://stroke.ahajournals.org//subscriptions/
Downloaded from http://stroke.ahajournals.org/ by guest on October 23, 2015You can also read