Infection Prevention Updates for Acute Care and Outpatient Settings
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Guidance and responses were provided based on information known on 5/26/2021
and may become out of date. Guidance is being updated rapidly, so users should look
to CDC and NE DHHS guidance for updates.
Infection Prevention Updates for
Acute Care and Outpatient
Settings
May 26, 2021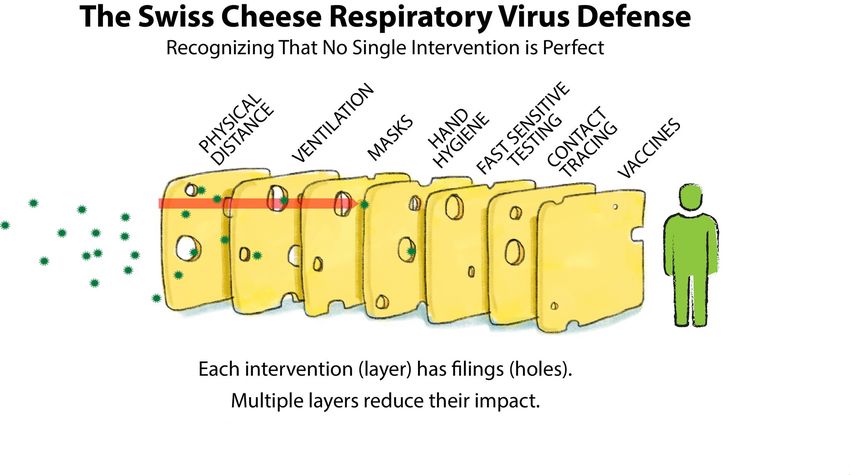
Questions and Answer Session
• Use the QA box in the webinar platform to type a question.
• Questions will be read aloud by the moderator as time allows.
• If your question is not answered during the webinar, please e-mail it to Nebraska ICAP or
call during our office hours to speak with one of our Infection Preventionists (IPs).
• A transcript of the discussion will be made available on the ICAP website
• https://icap.nebraskamed.com/coronavirus/
• https://icap.nebraskamed.com/covid-19-webinars/
Presenters :
Gary Anthone, MD gary.anthone@nebraska.gov
Matthew Donahue, MD matthew.donahue@@nebraska.gov
Richard Starlin, MD rick.starlin@unmc.edu
Rebecca Martinez, BSN, BA, RN, CIC remartinez@nebraskamed.com
Sarah Stream, MPH, CDA, FADAA sstream@nebraskamed.com
Kate Tyner, RN, BSN, CIC ltyner@nebraskamed.com
Lacey Pavlovsky RN, MSN, CIC lpavlovsky@nebraskamed.com
Panelists:
Daniel Brailita, MD dabrailita@unmc.edu
Jody Scebold, EdD, MSN, RN jodscebold@nebraskamed.com
Jean Ellis, RN, BSN jean.ellis@nebraska.gov
Moderator:
Margaret Deacy mdeacy@nebraskamed.com
Learning Objectives During this series, participants should be better able to: 1. Recognize infection prevention and control issues for application of the recommendations to mitigate these issues. 2. Identify resources on infection prevention and control that will be helpful to mitigate infection prevention and control challenges. 3. Describe latest updates on COVID-19 pandemic related to infection prevention and control practices in acute and outpatient settings. Target Audience Healthcare professionals working in acute and outpatient settings. To include medical directors, nursing staff, directors of nursing, infection preventionists, quality program leaders, administrators, consultant pharmacists or other staff working in long-term care settings.
Mission and Goals To provide an educational venue that connects infection preventionists and providers from acute and outpatient facilities across Nebraska with the objective of promoting the latest research and best practices in infection prevention and control. These educational webinars are aimed to help promote and strengthen the Nebraska infection prevention and control infrastructure. The goals for this educational activity include: 1. Increase knowledge of infection control processes for acute and outpatient settings. 2. Increasing awareness of specific infection prevention and control issues that may be confronted in acute and outpatient settings. 3. Provide resources to attendees to help them with infection prevention and control efforts in their own facilities. 4. Provide resources to attendees on the most up to date COVID-19 pandemic related guidance and recommendations.

Continuing Education
1.0 Nursing Contact Hour is awarded for the LIVE viewing of this
webinar
Nebraska Medicine is approved as a provider of nursing continuing
professional development by the Midwest Multistate Division, an accredited approver by
the American Nurses Credentialing Center’s Commission on Accreditation.
In order to obtain either contact hour, you must be present for the entire live webinar
and complete the post webinar survey
No conflicts of interest were identified for any member of the planning committee,
presenters or panelists of the program content
This CE is hosted by Nebraska Medicine and UNMC along with Nebraska ICAP and
Nebraska DHHS
Continuing Education
1.0 AMA PRA Category 1 Credit™ for Physicians offered by UNMC is awarded
for the live viewing of this webinar
In support of improving patient care, University of Nebraska
Medical Center is jointly accredited by the Accreditation Council
for Continuing Medical Education (ACCME), the Accreditation
Council for Pharmacy Education (ACPE), and the American
Nurses Credentialing Center (ANCC), to provide continuing
education for the healthcare team.
The University of Nebraska Medical Center designates this live
activity for a maximum of 1 AMA PRA Category 1 Credit™.
Physicians should claim only the credit commensurate with the
extent of their participation in the activity.
Disclosure Declaration
As a jointly accredited provider, the University of Nebraska Medical Center (UNMC) ensures accuracy, balance, objectivity,
independence, and scientific rigor in its educational activities and is committed to protecting learners from promotion, marketing, and
commercial bias. All faculty, planner and others in a position to control continuing education content participating in an accredited
continuing education activity are required to disclose all financial relationships with ineligible companies. Ineligible companies are
organizations whose primary business is producing, marketing, selling, re-selling, or distributing healthcare products used by or on
patients. The accredited provider is responsible for mitigating all relevant financial relationships in accredited continuing
education. Disclosure of these commitments and/or relationships is included in these activity materials so that participants may
formulate their own judgments in interpreting its content and evaluating its recommendations.
This activity may include presentations in which faculty may discuss off-label and/or investigational use of pharmaceuticals or
instruments not yet FDA-approved. Participants should note that the use of products outside currently FDA-approved labeling should
be considered experimental and are advised to consult current prescribing information for FDA-approved indications. All materials
are included with the permission of the faculty. The opinions expressed are those of the faculty and are not to be construed as those
of UNMC.
The accredited provider has mitigated and is disclosing identified relevant financial relationships for the following faculty, planners,
and others in control of content prior to assuming their roles:
FACULTY
The faculty have nothing to disclose:
Matthew Donahue, MD Richard Starlin, MD Gary Anthone, MD
Sarah Stream, MPH, CDA, FADAA Rebecca Martinez, BSN, BA, RN, CIC Lacey Pavlovsky RN, MSN, CIC
PLANNING COMMITTEE
The planning committee members have nothing to disclose:
Kate Tyner, RN, BSN, CIC Jody Scebold, EdD, MSN, RN Jean Ellis, DHHS
Daniel Brailita, MD
Nebraska DHHS
Updates
Dr. Gary Anthone, MD
Chief Medical Officer, DHHS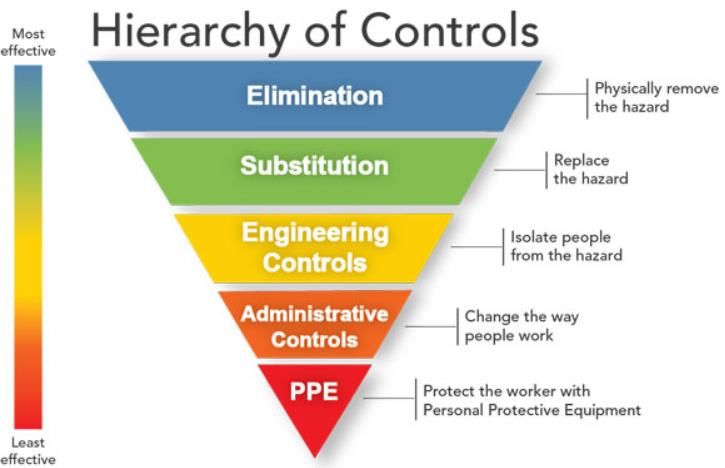
• Decrease 24 pts (-21,-17,+11,-44,0) • 7 day average of 2.%0 of staffed hospital beds occupied by Covid Pts (3.1,3.3,3.4,3.7,4.2) • 30% of COVID pts in ICU (31,29,30,36,24) • 59% of COVID ICU pts on Vents (50,29,25,36,41) • Average of 9 new covid pts admitted per day(12,12,16,16,22) • 7% of statewide ICU pts are COVID pts-9% was last week
Updates - Executive Order May 24th
• Link to 5/24/21 Governor Ricketts Press Release
• https://www.facebook.com/429619287192448/videos/491228182213000?__tn__=FNebraska DHHS
Updates
Dr. Matthew Donahue, MD
Medical Epidemiologist Intelligence Service Officer , DHHSVariants of Concern & Vaccinated vs.
Unvaccinated COVID-19 Hospitalization Rates
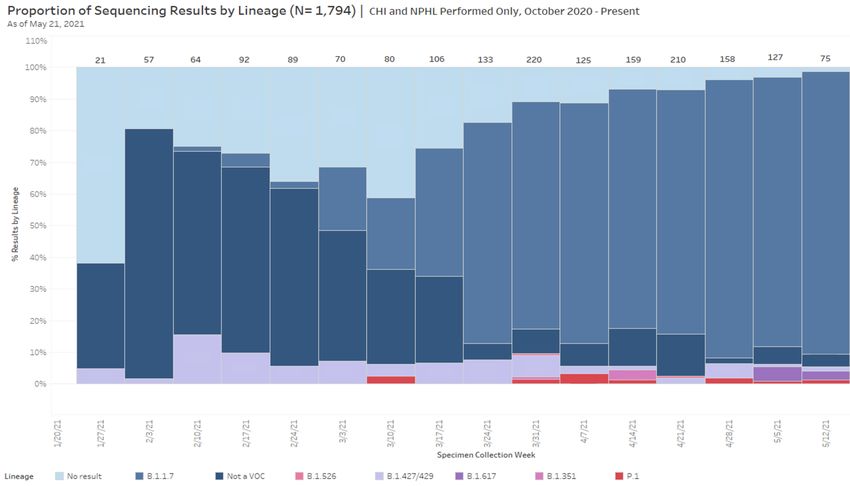
Variants of Concern & Sequencing
• 1,363 variants of concern (VOC) identified among Nebraska residents (1,205 B117,
18 P1, 10 B1.351, 11 B1.617, 102 B1.429/427, 17 B1.526); >90% of sequencing runs
are VOCs; B117 remains predominant
• 225 possible reinfections, one ”confirmed” reinfection identified (B117,
unvaccinated), no substantial trends relating to outcome or VOCs
• 537 possible vaccine breakthroughs (BTs), most confident in 228 of these that were
successfully sequenced; 14 hospitalized, 2 died
• P1, B1.526, B1.617 signals: potentially higher rates of vaccine BT (22-27%)
• B1.427/429 signal: potentially higher hospitalization rates (8%)
• Limitations: low numbers with proportions substantially impacted by small
changes in counts (directional trend, not statistically significant), selection bias
© Mc C h r y sta l G r ou p , 1
Public Health Fusion Cell |
LLC 4© Mc C h r y sta l G r ou p , 1
Public Health Fusion Cell |
LLC 5Current Applicable
Guidance for
Healthcare Settings
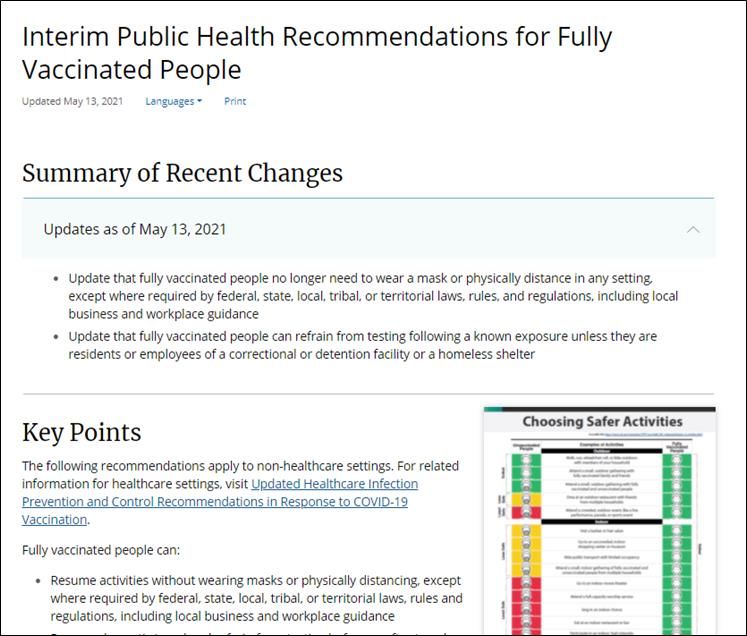
Rebecca Martinez, BSN, BA, RN, CICInterim Public Health Recommendations for Fully Vaccinated People | CDC
For NON-HEALTHCARE Settings Fully vaccinated people can: • Resume activities without wearing masks or physically distancing, except where required by federal, state, local, tribal, or territorial laws, rules and regulations, including local business and workplace guidance • Resume domestic travel and refrain from testing before or after travel or self-quarantine after travel • Refrain from testing before leaving the United States for international travel (unless required by the destination) and refrain from self- quarantine after arriving back in the United States • Refrain from testing following a known exposure, if asymptomatic, with some exceptions for specific settings • Refrain from quarantine following a known exposure if asymptomatic • Refrain from routine screening testing if feasible For now, fully vaccinated people should continue to: • Get tested if experiencing COVID-19 symptoms • Follow CDC and health department travel requirements and recommendations Interim Public Health Recommendations for Fully Vaccinated People | CDC
Acute and Outpatient – CDC Guidance & Updates
CDC Recommendations CDC Recommendations
– Last Updated February 23, 2021 – Last Updated April 27, 2021
Updated Healthcare Infection
Prevention and Control
CDC Interim Infection Prevention Recommendations in Response to
and Control Recommendations for COVID-19 Vaccination | CDC
Healthcare Personnel During the
COVID-19 Pandemic
Healthcare Facilities: Managing Operations During the COVID-19 Pandemic | CDCHierarchy of Controls
& Applied Horizontal
and Vertical Measures
Rebecca Martinez, BSN, BA, RN, CIC“Change is the only
constant.” - Heraclitus
Images by rawpixel.comControl exposure to hazards https://www.cdc.gov/niosh/topics/hierarchy/default.html
Eliminate the Hazard
• Elimination is the MOST effective and reliable at reducing hazards
• Get vaccinated
• Encourage others to get vaccinated
• Send home infected or potentially infected people from the workplace until they meet
CDC guidelines for ending isolation
• Clean and disinfect using a disinfectant that kill SARS-CoV-2 (on EPA’s List N)
“Vaccines will
MMR
help bring this
Vaccine pandemic to an
end.”
https://debeaumont.org/wp-
content/uploads/2021/01/VaccineToolki
t_1pger.pdf
https://www.historyofvaccines.org/index.php/content/
graph-us-measles-cases
https://www.osha.gov/coronavirus/
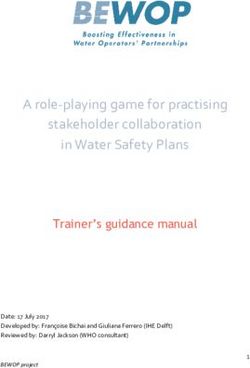
safeworkVaccination is key to ending this pandemic and moving forward https://www.historyofvaccines.org/index.php/content/1963-polio-campaign
Question – What Eliminated Polio? Answer – Vaccination https://www.cdc.gov/polio/progress/index.htm
Substitution – Reduce Risk
• Substitution involves replacing something that is hazardous, with something that is
not hazardous or less risk.
• Example- location of testing, such as outdoor/ drive-through testing sites
• Example- Sick versus well clinic locations/ appointment blocks
• COVID-19 disease is HIGH risk.
• COVID-19 vaccine is LOW risk.
• “At 95% efficacy, the vaccine is extraordinarily effective at protecting you
from the virus.”
• “If you’re concerned about side effects, we hear you. The likelihood of a
severe side effect is less than 0.5%. When mild side effects occur, they are
a normal sign your body is building protection to the virus, and most go away
in a few days. ”
• “The groundbreaking cooperation between leading medical experts here in
America and pharmaceutical companies globally has made a return to
normal possible thanks to the COVID-19 vaccine. The speed of
development was due to the sharing of research on a scale never attempted
before – and every study, and every phase of every trial, was carefully
reviewed and approved by a safety board at the FDA. The process was
transparent and rigorous throughout, with continual oversight and expert
approval.”
https://debeaumont.org/wp-content/uploads/2021/01/VaccineToolkit_1pger.pdfEngineering Controls
• Engineering controls are designed to remove the hazard at the
source, before it comes in contact with the worker / other patients.
• Well-designed engineering controls can be highly effective and
reliable in protecting workers and will typically be independent of
worker interactions to provide this high level of protection.
• Examples of engineering controls:
• Having dedicated airborne infection isolation rooms (AIIRs)
• Configuring the HVAC system to have negative pressure
typically where those with COVID-19 symptoms are cared for
• Improving central filtration (HEPA filters)
• Increasing the air exchanges per hour (ACH) in the facility
• Physical barriers such as plastic/glass walls or shields
Be sure to thank your
engineering (HVAC) staff
members for their dedication and
ingenuity
https://www.osha.gov/coronavirus/safeworkAdministrative Controls
• Administrative controls involve changing the way people work
• Used when hazards are not particularly well controlled
• Are less reliable than other measures and require significant effort
• Example of Administrative Controls:
• Written operating procedures to direct how work will be done
• Dedicated COVID-19 units
• Dedicated staff to care for COVID-19 patients
• Signs and Posters
• Training and refresher training
• Controlling facility entrance points
• Screening staff, patients, and visitors
• Visitor restriction procedures
• Communal dining policies
• Implementing remote work
• Capacity limits
• Universal masking
• Universal eye protection
https://www.osha.gov/coronavirus/safeworkPersonal Protective Equipment (PPE)
• PPE requires a lot of effort and should be used with more reliable control measures
• PPE can be costly in the long-term
• PPE is essential for COVID-19 patients and persons under investigation (PUI)
• When universal source control and universal eye protection is worn, it does
help reduce the risk of exposure if worn correctly
• Compliance with wearing the PPE is the first step
• Compliance with wearing the PPE correctly is critical
• PPE is needed when hazards are not well controlled
• As facilities determine how to move forward especially regarding PPE, they are
encouraged to assess their level of community transmission and what control
measures they are utilizing or will be utilizing to control risk.
• There are NO changes
in the PPE required for
COVID-19 patients or
persons under
investigation (PUIs).
https://www.cdc.gov/coronavirus/2019-ncov/downloads/COVID-19_PPE_illustrations-p.pdfHorizontal vs. Vertical Control
Measures (COVID-19 examples)
• There are two approaches to infection prevention and control measures; horizontal
approach and vertical approaches.
• The approaches are not mutually exclusive and can be used concurrently.
• Horizontal measures
• Broad-based approach
• Tend to be more universal and applied across an entire population
• Reduces infection from a broader range of pathogens
• Specific COVID-19 examples include; hand hygiene reinforcement, universal
source control masking, universal eye protection, universal screening etc.
• Vertical measures
• Focused on a single pathogen such as SARS-CoV-2
• Generally indicated when standard measures and precautions have failed
• Focused on a specific patient or subset of a population group
• Encompasses active surveillance
• Assesses vaccination of healthcare workers
• Specific COVID-19 examples include: COVID-19 PPE, PUI PPE, procedures
such as masking dependent upon vaccination status etc.
https://www.infectioncontroltoday.com/view/horizontal-versus-vertical-two-approaches-hai-preventionEyewear
Horizontal Measures
Sarah Stream, MPH, CDA, FADAAEye Protection
The use of eyewear is currently evolving
• HCP working in facilities located in areas
with moderate to substantial community
transmission
• Eye protection should be worn
during patient care encounters to
ensure the eyes are also protected
from exposure to respiratory
secretions.
• HCP working in areas with minimal to no
community transmission
• Continue to adhere to Standard and
Transmission-Based Precautions
based on anticipated exposures and
suspected or confirmed diagnoses.
• This might include use of eye
protection, an N95 or
equivalent or higher-level
respirator, as well as other PPE
Infection Control: Severe acute respiratory syndrome coronavirus 2
(SARS-CoV-2) | CDC Thi s Photo by Unknown Author i s licensed under CC BY-SACommunity Mitigation Framework | CDC
Why Do Staff Need Eye Protection?
• When caring for patients with communicable infections, transmission-
based equipment including gloves, gowns and eye and mouth protection
is used to interrupt the transmission of a pathogen in addition to standard
precautions such as hand hygiene
• The eyes, mouth, and nose all contain mucosal surfaces that are potential
routes of acquisition of SARS-CoV-2 due to the presence of the ACE2
receptor (the receptor that SARS-CoV-2 uses to enter the body).
• In healthcare settings, where reliable physical distancing may not be
possible and workers may be exposed to individuals with SARS-CoV-2
infection, including those who are asymptomatic or presymptomatic, CDC
recommends the use of eye protection such as face shields during
patient care encounters.
https://www.idsociety.org/covid-19-real-time-learning-network/infection-prevention/eye-protection/Masking for Healthcare Workers: Source Control vs. Droplet/ Contact PPE Source Control Contact/ Droplet Precautions Worn by an individual to keep potential Worn by HCW to prevent exposure from infections from spreading to others an infected individual Well-fitting cloth or surgical mask Fluid resistant, well fitting, surgical mask Worn by HCW in the facility for an Prevents droplets from entering mouth extended period of time (extended use) and nose (mucous membranes) Should be doffed and discarded by HCW Influenza, Pertussis and Mumps are before leaving the facility at the end of examples of when surgical masks should their shift be worn as a droplet precaution If a HCW treats a patient that is under Droplet precautions should be taken any droplet precautions, the mask used for time exposure to droplets could be the patient encounter should not be encountered used as source control after that patient Should be doffed after every patient encounter exposure (don’t practice extended use) https://www.cdc.gov/coronavirus/2019-ncov/hcp/infection-control-recommendations.html#useppe https://www.cdc.gov/infectioncontrol/basics/transmission-based-precautions.html#anchor_1564057963
Transmission Based Precautions
Droplet Precautions
• Precautions for patients known or suspected to be infected with pathogens
that are transmitted by respiratory droplets generated when coughing,
sneezing or talking (ex: Influenza, Pertussis, Mumps)
• Used in addition to Standard Precautions
Things to consider
1. Appropriate PPE use: Don surgical
masks before entering the patient
room
2. Source Control for patients during
treatment
3. Patient Placement based on patient
status (assess isolation needs) https://aricjournal.biomedcentral.com/articles/10.1
4. Limit transport and movement of 186/s13756-019-0629-9#Fig8
patient in facility
Centers for Disease Control and Prevention. (2020). Transmission Based Precautions. Retrieved from
https://www.cdc.gov/infectioncontrol/basics/transmission-based-precautions.html#anchor_1564057963Selecting Eyewear
- content added based on audience feedback -
• The ANSI/ISEA Z87.1:2020 standard provides
criteria and requirements for selection, use, and
maintenance of the different face and eye
protectors to promote the most effective
materials and methods of use. American
National Standard For Occupational And
Educational Personal Eye And Face Protection
Devices.
• This standard should be applied when the
equipment is first placed in service, so that any
applicable protectors will be stamped with
the marking “Z87” to demonstrate that the
meet the minimum guidelines laid out in the
standard.
• Those who make use of this standard often pair
its requirements with that of other essential
documents. For example, ANSI Z87.1 is often
used alongside ANSI Z358.1, the standard for
emergency eyewashes and shower equipment.
These standards are available together as the
ANSI/ISEA Z358.1 / ANSI/ISEA Z87.1 –
Eyewash and Eye Protection Package.
Read more at the ANSI Blog: ANSI Z87.1 Eye
and Face Protection Devices
Standard https://blog.ansi.org/?p=163275Exposure Possibilities You can look at your specific possible exposures: % County Positivity Rate x # Pt. Encounters = Possible Exposures Examples: 30% County Positivity x 20 Pt. Encounters = 6 Possible Exposures 10% County Positivity x 15 Pt. Encounters = 1.5 Possible Exposures **Remember that there is still the possibility of asymptomatic COVID- 19 shedding and there are some people that are vaccinated, you can assess your personal exposure risk by taking all these things into account regarding PPE use during patient encounters
https://theindependent.com/news/state-and-regional/health-experts-multiple-efforts-best- defense-against-covid-19/article_2a11c137-bf9c-5398-9ba3-821482c9419c.html
Nebraska Medicine
Updates to Masking &
Eye Protection
Guidance
Richard Starlin, MD
Assistant Professor, Division of Infectious Diseases
Medical Director, Employee Health, Nebraska MedicineNebraska Medicine
- Updated Mask Guidance
Image by rawpixel.com
• Nebraska Medicine adjusted its universal PPE policy to align with recent revisions to
the CDC mask guidance. The updates listed below are now in effect throughout
the organization.
• Fully vaccinated individuals, those who have completed their vaccine
series and are at least two weeks out from their final dose, can choose to
take off their mask in the following areas:
• Non-public and non-patient care areas, such as break rooms,
conference rooms, offices, ECCP etc.
• There is no requirement for physical distancing
• People may choose to continue to wear a mask in these settings to
minimize risk. Just because someone is wearing a mask in the
organization does not mean they have not been vaccinated.
• Unvaccinated individuals
• Must continue to comply with current masking and physical distancing
recommendations.
• Should not have unmasked interactions with other personnel.
https://www.nebraskamed.com/sites/default/files/documents/covid-
19/universal-ppe-policy-and-faq.pdf?date=5212021Nebraska Medicine – When Masks Are Required When masks are required Image by rawpixel.com • Masks remain required when in a public space and/or patient-facing areas, such as the cafeteria and hallways • Visitors should continue to wear their mask during the entirety of their visit, and our visitor policy remains as is • If you have any potential COVID-19 symptoms, even if vaccinated, wear a mask and contact Employee Health • A good rule of thumb to follow is if you are in an area the public can access easily, you should wear a mask, regardless of whether you have been vaccinated https://www.nebraskamed.com/sites/default/files/documents/covid- 19/universal-ppe-policy-and-faq.pdf?date=5212021
Nebraska Medicine
- Transitions Back to Standard Eye Protection
• Eye protection must be worn by colleagues when splash
or body fluid is anticipated.
• A good reminder for yourself is that “when gloves
are on, goggles are on”
• Eye protection is a continued requirement for the care of
patients with or under investigation for COVID-19
• Outside the potential risks mentioned above, eye
protection is not required, however, you can elect to
continue to wear it during any patient interaction
Image by raw pixel.comQuestions and Answer Session Please use the QA box in the webinar platform to type a question Questions will be read aloud by the moderator in the order they are received A transcript of the discussion will be made available on the ICAP website Panelists: Richard Starlin, MD Daniel Brailita, MD Rebecca Martinez, BSN, BA, RN, CIC Sarah Stream, MPH, CDA, FADAA Kate Tyner, RN, BSN, CIC Lacey Pavlovsky RN, MSN, CIC Jody Scebold, EdD, MSN, RN Jean Ellis, RN, BSN
Resource recommendation: based on audience question CDC webpage: Key Things to Know about COVID-19 Vaccines a.k.a "What we know and what we are still learning about vaccines" https://www.cdc.gov/coronavirus/2019- ncov/vaccines/keythingstoknow.html
Nebraska ICAP
Updates
Nebraska ICAP Acute & Outpatient Assessments
Office Hours & Phone NumberAntimicrobial Stewardship Self-
Assessment Survey
• In partnership with Nebraska DHHS, Nebraska ASAP has developed a survey tool
to assess CDC Core Element implementation at your facility.
• Because of the need for the DHHS to better understand stewardship activities in
the state, we strongly encourage you to complete the below assessment survey.
• Nebraska ASAP will review your responses and reach out to offer targeted
feedback/interventions to help improve stewardship at your facility.
Acute Care Outpatient
Hospitals Clinics
https://redcap.nebraskamed.com/surveys/?s=D3
https://redcap.nebraskamed.com/surveys/?s=RTHMH HWL4LHRR
APKLAImplement infection-control
measures relevant to
construction, renovation,
maintenance, demolition,
and repair. Before the project
gets underway, perform an
infection control risk
assessment (ICRA) to define
the scope of the project and
need for barrier measures.
CMS requires this.
https://www.cms.gov/medicare/provider-
enrollment-and-
certification/surveycertificationgeninfo/do
wnloads/survey-and-cert-letter-15-12-
attachment-1.pdf
https://www.cdc.gov/infectioncontrol/pdf/g
uidelines/environmental-guidelines-P.pdfRespiratory Protection Taskforce https://icap.nebraskamed.com/nebraska-respiratory-protection-task-force/
Respiratory Protection Taskforce https://icap.nebraskamed.com/nebraska-respiratory-protection-task-force/
PPE Requests from NE DHHS
Use this link to request support with PPE:
•PPE Request from NE
DHHS https://form.jotform.com/Nebras
kaDHHS/PPERequestForm
•This form goes to both the local health
department and NE DHHS
•Requests are for PPE needs for next 2
weeks.
•Requests must be made by
Wednesday 11:59 AM for next week
delivery.
•Local Health Departments are
responsible for approving requests,
work with them directly for urgent
needsAcute and Outpatient Services by Ne ICAP
ICAR Reviews for Acute and OP
• Infection Control Assessment and Response (ICAR) tools are used to
systematically assess a healthcare facility’s infection prevention and
control (IPC) practices and guide quality improvement activities (e.g.,
by addressing identified gaps)
• ICAP is offering COVID-19 virtual assessments to both Acute and
Outpatient Settings
• ICAP is offering Full, on site, Infection Control ICAR Reviews for
Outpatient Settings
• Contact NE ICAP at 402.552.2881 to be connected with an IP
• ICAP Request for Assessment and
Email Distribution:
https://nebraskamed.formstack.com/forms/
add_me_to_email_distribution_listInfection Prevention and Control
Office Hours
Monday – Friday
8:00 AM – 10:00 AM Central Time
2:00 PM -4:00 PM Central Time
Call 402-552-2881
Like us on Facebook by
scanning this QR code!Webinar CE Process
1 Nursing Contact Hour is awarded by NE Medicine *
* Nebraska Medicine is approved as a provider of nursing continuing professional
development by the Midwest Multistate Division, an accredited approver by the
American Nurses Credentialing Center’s Commission on Accreditation.
1 AMA PRA Category 1 CreditTM for Physicians offered by UNMC
CNE Nursing Contact Hours: AMA PRA Category 1 Credit™
➢ Completion of survey is required. Completion of survey is required.
➢ The survey must be specific ➢ The survey must be specific to
to the individual obtaining the individual obtaining credit.
credit. (i.e.: 2 people cannot (i.e.: 2 people cannot be listed
be listed on the same survey) on the same survey)
➢ One certificate is issued monthly ➢ One certificate is issued monthly for
for all webinars attended all webinars attended
➢ Certificate comes directly from ➢ Certificate can be downloaded from
ICAP via email the UNMC CCE system directly, they
➢ Certificate is mailed by/on the 15th will email you access
of the next month ➢ Survey functionality is lost on mobile
➢ Survey functionality is lost on devices
mobile devicesYou can also read