Impacts of COVID-19 on female genital cutting - ORCHID PROJECT - September 2020 - ReliefWeb
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

ORCHID PROJECT
WORKING TOGETHER TO END
FEMALE GENITAL CUTTING
Impacts of COVID-19 on
September 2020
female genital cutting

Summary
From March 2020, early in the global COVID-19 crisis, reports began to emerge from our partners and allies that they were witnessing
elevated rates of female genital cutting (FGC). In Kenya, a country making positive progress in ending the practice through political
leadership, a national and county-level governance structure and civil society action,1 we were hearing consistent reports of girls being
subjected to FGC, or fleeing their homes for fear of being cut, from various counties due to school closures and the implementation of
lockdown measures.
Since the start of the pandemic, a range of excellent reports have highlighted the ‘gendered impact’ of the COVID-19 crisis on women and
girls, which has brought pre-existing inequalities and gender-based violence into sharp focus.2 But at a global policy level there has been
less acknowledgement of how the pandemic is specifically affecting the practice of FGC.
In response, Orchid Project began conducting interviews and surveys with our grassroots partners and allies across West Africa, East
Africa and Asia to explore the impacts of COVID-19 on the practice of FGC and the organisations and activists working to end the practice.
KEY FINDINGS
● Increased rates of FGC are being reported across East and West Africa, where COVID-19 related lockdowns are being seen as an
opportunity to carry out FGC undetected
● Lack of FGC integration within COVID-19 response is leaving girls at risk and survivors with no recourse to essential prevention,
protection and support services
● Lack of essential health services and safe spaces for girls at risk and survivors of FGC is a serious concern
● Economic hardship is driving increased rates of FGC because of parents seeking ‘bride prices’ and, in some cases, cutters returning
to the practice having previously abandoned it
● Fear of the virus may be leading to a re-emergence of previously abandoned social norms around FGC in some rural communities
● Restricted access to communities for community-based organisations (CBOs) carrying out FGC programming may be resulting in
increased rates of cutting and lack of accurate data
● Shrinking civil society space to advocate for action to end FGC, alongside reduced funding for FGC
● Increased use of social media, behaviour change communications and digital technologies to reach communities with girls at risk
● CBOs are extending and expanding their service provision beyond FGC prevention efforts to respond to community needs in spite
of reductions in funding
● Grassroots and women-led organisations require urgent flexible, cash-based support to continue their work to protect girls.
Population Council (2020) ‘Lessons from a Five-Year Research Programme on FGM/C and the Relevance for Policy and Programmes in Kenya’
1
For example, see Gender and Covid 19 Working Group resources: https://www.genderandcovid-19.org
2
Impacts of COVID-19 on female genital cutting 1
Recommendations
Increase funding and support towards grassroots and women-led organisations and activists
1. Urgently increase funding to grassroots and women-led organisations working to end FGC, including greater provision for emergency,
flexible cash-based assistance during humanitarian crises
2. Significantly strengthen capacity building and technical assistance to grassroots organisations to support and expand new forms of
programmatic activity and innovation during COVID-19
3. Support community-led data collection, monitoring and reporting on the impact of COVID-19 on FGC to inform real-time crisis
response and recovery efforts
4. Technology and communications companies should scale up social and pro bono initiatives available to grassroots and women-led
organisations to enable them to access and effectively utilise technology to mitigate the impacts of COVID-19
Mainstream and integrate FGC interventions into development and humanitarian programming
5. Prioritise comprehensive mainstreaming of FGC into crisis response and recovery work, including GBV and SRHR programming in
both development and humanitarian contexts (the Humanitarian-Development Nexus)
6. Urgently call on UN OCHA to operationalize rhetorical, policy and financial commitments, including those made during the Oslo End
SGBV Conference, to ensure GBV is a key priority at field and country level during crisis response and recovery
Ensure essential service provision during crisis response and recovery
7. Recognise GBV and SRHR services as ‘essential’, including those accessed by girls at risk or survivors of FGC, to allow service providers
to continue to operate during emergencies
8. Harness learning from previous epidemics by working with medical professionals and health associations to identify opportunities
to disrupt the medicalisation of FGC
9. Governments should strengthen social protection measures, such as universal healthcare and universal basic income. High income
countries should support this agenda through debt cancellation, which will be critical to enable low and middle income countries
to mobilise domestic funds.
2 Impacts of COVID-19 on female genital cutting
Our Approach
At Orchid Project, given our focus on community-led change to end FGC, the onset of the COVID-19 pandemic compelled us to seek
answers to the following questions:
● Were community-based organisations able to function during lockdowns to ensure critical prevention work, or protection
interventions?
● Were grassroots groups able to adapt to ensure progress could still be maintained in ending FGC, or had they switched to fulfil other
urgent community needs?
● How could we ensure communities working to end FGC could get the support they needed to respond to the COVID-19 pandemic,
as well as future crises which put girls at heightened risk of being cut?
We know that data is critical to enabling evidence-based programming and advocacy. We wanted to contribute to establishing how the
pandemic is affecting trends in the practice to support effective crisis response, and improve preparedness for future emergencies and
humanitarian shocks.
Through this briefing we aim to share insights on FGC trends collected from community-based organisations in East and West Africa and
Asia-Pacific, the majority women-led,3 that are working to prevent and protect girls from undergoing FGC.
From March to July 2020, we reached out to our global network of grassroots organisations and activists and have carried out interviews
and surveys with 38 grassroots activists and organisations across 14 countries in order to monitor the impacts of the pandemic on FGC.4
As such, these findings cannot be generalised across all contexts in which FGC is practised, but they do provide important insights into
how COVID-19 is affecting FGC in specific communities.
3
At least 27 of the 38 respondents (71%) are women-led orgs to our knowledge (defined by having at least one women in senior leadership), though this data was not collected via the
surveys or interviews
4
Data was collected from CBOs in India, Indonesia, Iran (Islamic Republic of), Kenya, Liberia, Malaysia, Myanmar, Nigeria, Pakistan, Sierra Leone, Singapore, Somalia, Sri Lanka, United
Republic of Tanzania.
Impacts of COVID-19 on female genital cutting 3
Introduction
Female genital cutting (FGC), much like COVID-19, is a global issue that requires a global response. 200 million women and girls around
the world are affected by the practice.5 It is grounded in discriminatory gender norms, and has significant health and socio-economic
impacts on women throughout their lives. Ending the practice would have a transformative effect for women and girls, with accelerated
progress essential to achieving Sustainable Development Goal 5, on gender equality, and supporting all the other Agenda 2030 goals.
During times of crisis, states have a duty to prevent and mitigate gender-based violence, including FGC.6 Yet we are not seeing effective,
gender-based and intersectional policy-making in relation to COVID-19 pandemic, despite increased vulnerabilities for certain groups.7
Despite significantly higher rates of death amongst men, the innumerable short-term and long-term impacts of COVID-19, and the
responses to contain it, have fallen disproportionately on the burden of women and girls worldwide.8
Alongside this, the rise of a ‘shadow pandemic’ of gender-based violence (GBV) lays bare the stark realities of systemic inequality and
discrimination, and the continuing failure at global, regional and national levels to effectively apply a gender and intersectional lens to
policy making, even in emergency response and recovery. Where COVID-19 response and recovery plans have been put in place in a
gender-inclusive way, these largely ignore or fail to account for the particular needs and lived experiences of women and girls that are at
risk of, or are survivors of, FGC.
FEMALE GENITAL CUTTING AND We are already witnessing the economic and societal impacts of
COVID-19 undoing years of progress by grassroots activists and
COVID-19: THE NEED FOR AN communities to end FGC. UNFPA has reported that an additional
INTEGRATED CRISIS RESPONSE two million cases of FGC will need to be averted to meet Agenda
2030 as a result of COVID-19’s delays to FGC programming.14 Loss
of livelihoods and economic hardship are leading some parents to
FGC is a violation of the human rights of women and girls,9
decide to marry off their daughters, resulting in increasing rates
which is held in place by, and reinforces discriminatory gender
of FGC as a prerequisite for marriage. Bride prices can then be
stereotypes and norms that define the limits of a girl’s aspirations
exchanged for food and basic supplies. Lockdowns and curfews
and sexuality, and cause serious health impacts across her life.
also mean that girls are kept out of school where they are at
Ending FGC requires the displacement of harmful gender norms,
greater risk of FGC, whilst protection, health and justice services
which would potentially transform the lives of millions of women
are diverted to deal with implementing curfews and responding
and girls and accelerate progress towards gender equality.
directly to the pandemic.
In certain contexts, FGC acts as a precursor to child marriage
and marks a girl’s transition into womanhood.10 This shift has
significant implications for girls’ access to education and future
economic empowerment.11
Applying a gender-lens to the COVID-19
response is vital in continuing and
Emergency situations and humanitarian crises, including health accelerating work to end FGC, and all
epidemics,12 have disproportionate impacts on women and girls
forms of gender-based violence, in order to
and exacerbate these existing structural gender inequalities,13
which lie at the heart of FGC. Applying a gender-lens to the
achieve SDG 5 by 2030.
COVID-19 response is vital in continuing and accelerating work
to end FGC, and all forms of gender-based violence, in order to
achieve SDG 5 by 2030.
5
UNFPA (2020) ‘Online resources on female genital cutting’
6
Inter-Agency Standing Committee (2015) ‘Guidelines for Integrating Gender-Based Violence Interventions in Humanitarian Action: Reducing risk, promoting resilience and aiding
recovery’
7
UN Women (2020) ‘Will the pandemic derail hard-won progress on gender equality?’
8
LSE (2020) ‘Gendering COVID-19: implications for women, peace and security’
9
UN Human Rights Council (2020) ‘Resolution on the Elimination of Female Genital Mutilation’
10
World Vision (2014) ‘Exploring the links: Female genital mutilation/cutting and early marriage’
11
GIZ (2011) ‘Female Genital Mutilation and Education’
12
The Lancet (2020) ‘COVID-19: the gendered impacts of the outbreak’
13
Julie Lafrenière, Caroline Sweetman & Theresia Thylin (2019) ‘Introduction: gender, humanitarian action and crisis response’, Gender & Development 27/2: 187-201
14
UNFPA (April 2020) ‘Impact of the COVID-19 Pandemic on Family Planning and Ending Gender-based Violence, Female Genital Mutilation and Child Marriage’
4 Impacts of COVID-19 on female genital cutting
In order to mitigate the deeply gendered impacts of COVID-19, programming requires the provision of quality, survivor-centred
the global community must implement a response and recovery health, creation and maintenance of referral systems and
plan that applies a comprehensive gender lens at all levels of pathways, and safe spaces for women and girls.22 Equally, the
programming and implementation. But we need to do more than Minimum Standards for Child Protection in Humanitarian Action
mitigate the impacts. The global response to COVID-19 should (Standard 9), requires that “all children are informed about and
use this opportunity to ‘build back better’ by championing and protected from sexual and gender-based violence and have
funding grassroots, women-led local organisations to lead the access to survivor-centred response services”, and makes explicit
change on the ground.15 reference to FGC as a form of GBV.23
Centralising and supporting grassroots activists and organisations Nevertheless, only 0.12% of global humanitarian funding went to
will allow us to fundamentally disrupt systemic inequalities by essential GBV services from 2016-18.24 The Global Humanitarian
reinforcing and empowering women as agents of change, to Response Plan for COVID-19 has failed to include a single
ensure responsive and contextually relevant interventions,16 and standalone objective on responding to GBV during the pandemic,
to foster sustainability and scalability in the longer term. and GBV itself remains the most underfunded response service at
this time.25 Whilst availability and access to essential GBV services
are currently being curtailed, efforts to respond to COVID-19
Only 0.12% of global humanitarian funding must prioritise and integrate these services as essential and life-
went to essential GBV services from 2016-18. saving, and should consider and respond to the unique needs of
women and girls at risk or survivors of FGC.
FGC AND GBV IN EMERGENCIES
We need to do more than mitigate the
Emergency situations routinely lead to increased rates of gender- impacts. The global response to COVID-19
based violence (GBV) including FGC,17 and UNFPA Minimum should use this opportunity to ‘build
Standards on GBV in Emergencies require an assumption that back better’ by championing and funding
violence increases during these periods.18 Comprehensive grassroots, women-led local organisations to
evidence and information confirms that COVID-19 has intensified lead the change on the ground.
domestic and gender-based violence globally.19
Curfews and ‘stay at home’ orders have resulted in the shutting
down of schools, safe houses, churches, and other forms of
refuges for girls at risk of FGC. Most lockdown orders have been
implemented in high-prevalence FGC areas without exemption
for girls at risk, reducing access to essential GBV and protection
services, and disrupting vital and life-saving referral pathways.
Emergency situations resulting in increased sexual violence also
place survivors of FGC at greater risk of compounded physical
and mental health impacts as a result of existing trauma20 and
physical health impacts of FGC.21
The Inter-Agency Minimum Standards for GBV in Emergencies
15
ActionAid (2020) ‘Creating lasting impact: The power of women-led localised responses to COVID-19’. See also: CARE (2020) ‘Where are the women? The Conspicuous Absence of
Women in COVID-19 Response Teams and Plans, and Why We Need Them’
16
Ibid - ActionAid (2020) ‘Creating lasting impact: The power of women-led localised responses to COVID-19’
17
Inter-Agency Standing Committee (2015) ‘Guidelines for Integrating Gender-Based Violence Interventions in Humanitarian Action: Reducing risk, promoting resilience and aiding
recovery’
18
UNFPA (2015) ‘Minimum Standards for Prevention and Response to Gender-Based Violence in Emergencies’
19
UNDP (2020) ‘UNDP Brief: Gender-based Violence and COVID-19’
20
Behrendt, A., and Moritz, S. (2005) ‘Posttraumatic Stress Disorder and Memory Problems After Female Genital Mutilation’ The American Journal of Psychiatry 162/5: 1000-1002; Berg,
R. and Denision, E. (2012) ‘Does female genital mutilation/ cutting (FGM/C) affect women’s sexual functioning? A systematic review of the sexual consequences of FGM/C’, Sexuality
Research and Social Policy 9/1: 41-56
21
PopCouncil (2016) ‘Health impacts of FGM/C: A synthesis of the evidence’
22
UNFPA (2015) ‘Minimum Standards for Prevention and Response to Gender-Based Violence in Emergencies’
23
The Alliance for Child Protection in Humanitarian Action (2019) ‘Minimum Standards for Child Protection in Humanitarian Action’, Standard 9
24
IRC (2019) ‘Where is the money? How the humanitarian system is failing in its commitments to end violence against women and girls’
25
At end June, funding requirements for GBV in 16 countries with humanitarian response plans amounted to $487 million (including COVID-19 related-responses), of which only $34
million (7 per cent) were funded, leaving a gap of $453 million.
Impacts of COVID-19 on female genital cutting 5
FGC AND SRHR IN EMERGENCIES
SEXUAL AND REPRODUCTIVE HEALTH
The practice of FGC directly impacts the sexual and reproductive IMPACTS OF FGC
health and rights (SRHR) of women and girls affected by it. Whilst
the short-term health risks of FGC include haemorrhaging, • Genital tissue swelling
infection, and death, FGC is also associated with a number of • Problems with urination, including urinary
long-term health risks. Survivors of FGC experience a number of retention and painful urination
sexual, urological and mental health problems as well as obstetric
• Excessive scar tissue (keloids)
complications. This includes increased risk of caesarean section,
postpartum haemorrhage (excessive bleeding after childbirth), • Problems menstruating, often caused by
and higher incidences of intrapartum stillbirth (stillbirth occurring obstructing the vagina as a result of infibulation
between onset of labour and delivery) and neonatal death • Vaginal problems including discharge, bacterial
(death during the first 28 days of life).26 Experiences from past vaginosis and other infections
epidemics including Ebola and Zika demonstrate that essential • Removal of, or damage to the clitoris, can affect
SRHR services are routinely diverted or shut down in favour of sexual sensitivity and lead to decreased sexual
responding directly to the immediate health impacts of the virus. desire and pleasure, pain during sex, difficulty
As a result, in Liberia during the 2013-16 Ebola epidemic, more during penetration, decreased lubrication during
women died of obstetric complications than from Ebola itself.27 In intercourse, and reduced frequency or absence of
countries with high FGC prevalence, the risks of denying essential orgasm
and lifesaving SRHR services to survivors of FGC are exacerbated. • Childbirth complications including associations or
The Minimum Initial Services Package (MISP) for Sexual and links with
Reproductive Health guarantees a minimum immediate ◦ Increased risk of caesarean section
package of essential SRHR services in crisis situations, including
◦ Postpartum haemorrhage
responding to the needs of survivors of sexual violence, providing
emergency obstetric care, and requiring health care providers in ◦ Recourse to episiotomy
relevant FGC WHO Type III (infibulation) contexts to be aware and ◦ Difficult labour
able to perform de-infibulation where necessary.28 In contrast,
◦ Obstetric tears/lacerations
numerous reports from FGC-practising countries, including
Nigeria, India and Malaysia, indicate that SRHR services are being ◦ Instrumental delivery
defunded, deprioritised, and even rolled back in favour of directly ◦ Prolonged labour
responding to COVID-19.29
◦ Extended maternal hospital stay
◦ Perinatal risks including infant resuscitation at
delivery, intrapartum stillbirth, and neonatal
death
• Obstetric fistula, likely as a result of prolonged and
obstructed labour in women with FGC.
26
WHO ‘Health risks of female genital mutilation (FGM)’. Accessed in August 2020.
27
McQuilkin, Udhayashankar, Niescierenko & Maranda (2017) ‘Health-Care Access during the Ebola Virus Epidemic in Liberia’, The American Journal of Tropical Medicine and Hygiene,
97/3: 931-936
28
Inter-Agency Field Manual on Reproductive Health in Humanitarian Settings (2010) Revision for Field Review.
29
Gender in Humanitarian Action (GiHA) (2020) ‘The COVID-19 Outbreak and Gender: Key Advocacy Points from Asia and the Pacific’
6 Impacts of COVID-19 on female genital cutting
Regional Impacts of COVID-19 on FGC
Through our advocacy, knowledge sharing, and communications work, Orchid Project works with communities and local champions to
bring global attention to the issue of FGC, and to secure the prioritisation of greater policy commitments and financial resources to bring
an end to this practice. The impacts of COVID-19 on FGC are understood most starkly by those who are working at the forefront of efforts
to end the practice.
West Africa
OVERALL TRENDS
Across West Africa, national lockdowns and stay-at-home
orders responding to COVID-19 have resulted in restricted
freedom of movement, with the unintended consequences
that access to prevention, protection and care services,
including psychosocial support, have been seriously
curtailed. Nationwide lockdowns have resulted in girls
staying at home where they are at greater risk of FGC, with
no exemptions in place for girls at risk or survivors of the
practice. In Abuja, Nigeria, local organisations have reported
an increase in numbers of girls being cut across South-West
Nigeria as a result of school closures, whilst prevention and
protection efforts are unavailable due to social distancing
and travel restrictions. Across Ilorin, Kwara State, and North
Central Nigeria, grassroots organisations are also reporting
a re-emergence of socio-cultural norms, prompting a rise in
FGC.
Whilst recent analysis of COVID-19’s likely impacts has
pointed towards potential similarities with previous Ebola
epidemics in West Africa, local organisations instead point
to a community perception that COVID-19 is not as serious
“The longer girls stay home, the higher the
as Ebola, which has resulted in a weaker adherence to
risks for home initiation [of FGC]” lockdown rules. Social norms-based harmful practices are
– Chernor Bah, CEO & Co-Founder, Purposeful, therefore likely to continue secretly during COVID-19. In
Sierra Leone Sierra Leone, whilst a government ban on Bondo (secret
societies) gatherings has been put in place, where initiation
rites include FGC, activists note that it is unlikely that society
leaders will abide by lockdown rules and will instead perform
undercover initiations.
Impacts of COVID-19 on female genital cutting 7CLOSURE OF SAFE SPACES MONITORING AND REPORTING OF
Blanket lockdowns and stay-at-home orders have also resulted in
FGC
the closure of safe spaces for girls at risk and survivors of FGC. Local
Measures for monitoring and reporting suspected cases of FGC
organisations have reported a diversion of medical services and
for girls at risk have also come under considerable strain during
resources towards direct COVID-19 responses at the expense of
lockdown. Hotlines and helplines are unavailable in Liberia and
GBV and SRHR services. Mental health and psychosocial support
Sierra Leone, where FGC remains legal, although a helpline is
services have also failed to be classified as essential services
available in Sierra Leone for domestic violence and rape. In Nigeria,
during this period. Local organisations in Nigeria point to higher
some civil society organisations (CSOs) are running and upscaling
incidence rates of intimate partner violence during lockdown, and
their own hotline initiatives, with one local organisation in Enugu
stress the considerable implications for survivors of FGC without
State, Nigeria, reporting over 2,000 calls. Beyond telephone
access to vital services. Some shelters have also been closed in
services, organisations are reporting that community-based
Nigeria without provision of alternatives for women and girls at
surveillance methods have been curtailed during lockdown, with
risk of FGC. Where shelters or alternative options are available
a disproportionate effect on women and girls in hard to reach
across Nigeria and Sierra Leone, they are seriously hampered by
or rural areas. In Enugu state, Nigeria, activists and organisations
a lack of funding and limited spaces available.
are also relying on an increased presence of ‘Neighbourhood
Watch Group’ members in communities to provide an informal
ESSENTIAL SERVICES policing system and deterrent effect, noting that formal policing
is overburdened with COVID-19 and unable to provide protection
Health services are said to have been heavily reduced in Nigeria, to girls and women at risk of FGC.
Liberia and Sierra Leone. Reports from Abuja, Nigeria, note that
health care providers are providing ‘essential’ services only, which
has not included vital SRHR or broader health services for women
ECONOMIC IMPACTS
and girls at risk or survivors of FGC. These so-called ‘essential’
Whilst lockdown orders have broadly impacted economies and
services were also inaccessible during lockdown due to travel
have led to shortages and price rises on basic necessities, local
restrictions. Grassroots activists have also cited a lack of medical
livelihoods have also been seriously impacted. Anecdotal reports
supplies, closures and reduced services across Ilorin, Kwara State
from Nigeria suggest that former cutters may be returning to
and North Central Nigeria. Similar reports have also been made
providing FGC services as a way of making money whilst more
from Sierra Leone, where health services have been particularly
formal economic roles and opportunities are limited.
difficult to access by women and girls in remote areas, and as
a result of public curfews and limited transportation options,
including ambulances.
8 Impacts of COVID-19 on female genital cuttingSOCIETY FOR THE IMPROVEMENT OF RURAL PEOPLE (SIRP), NIGERIA
SIRP works across Enugu State to advocate for and provide community-based development programming for people living in
rural conditions, including to end FGC. Since the first documented cases of COVID-19 in Nigeria in February 2020, restrictions
on movement meant that SIRP’s community outreach programmes to end FGC stalled across Enugu State. SIRP initiated
and strengthened hotline reporting on FGC for girls at risk, and expanded the use of mass and social media, including radio
programming, to raise awareness of the regional Violence Against Persons Prohibition Law to a reported 1,250,000 listeners. SIRP
have also been supporting community-based women’s and youth groups to lead prevention and protection activities by using
WhatsApp to support community surveillance programmes. Most recently, SIRP have trained FGC and child marriage survivors on
effective COVID-19 prevention guidelines, whilst providing personal protective equipment (PPE) and essential food items.
“Because of the restriction of movement during this pandemic, more than 85% of women and
girls, particularly in rural communities, are exposed to the practice; making it difficult to track the
practice and create more awareness on the devastating effects on the survivors.”
- Dr Chris Ugwu, Executive Director, SIRP.
A SIRP team member teaches hand washing techniques. SIRP, Enugu State, Nigeria, 2020.
Impacts of COVID-19 on female genital cutting 9East Africa and the Horn
who are aware of at least 10 cases of FGC during the three
month lockdown period, although they also caution substantial
underreporting of the practice due to a shift of focus away from
FGC towards COVID-19. In communities who traditionally carry
out FGC during a ‘cutting season’, activists and organisations have
expressed fears and concerns for the increased number of girls
that will now be at risk of the practice when the season arrives.
CLOSURE OF SAFE SPACES
Local reports from across the East Africa region again emphasise
that stay at home orders and lockdowns are increasing the risk
of girls being cut, noting that some communities are viewing the
lockdown as an extended holiday to take advantage of decreased
surveillance and extended recovery time for girls to avoid
detection. The closure of schools, including boarding schools,
and churches across Kenya, Somalia and Somaliland and Tanzania
has resulted in the closure of de facto safe spaces.
Girls locked down at home are far more likely to be subjected
to FGC, where communities have the opportunity to conduct
ceremonies in secret. In Rift Valley and Samburu, Kenya, local
activists have reported that communities are using male
OVERALL TRENDS circumcision ceremonies to secretly cut girls during lockdown.
In Hargeisa and Puntland, Somalia, the arrival of the rainy
season has compounded the increased risk for girls at this time.
Collective reports from CSOs and activists operating across East
In Kenya and Tanzania, links between FGC and child marriage
Africa and the Horn of Africa have noted a considerable rise in FGC
across the region also mean that girls undergoing FGC are likely
cases across Somalia and Somaliland, Kenya, Tanzania and Sudan.
to be married during this period, and expected high rates of
According to a recent UNFPA rapid assessment, 31 percent of
early pregnancy mean that girls are unlikely to return to school
community members across Somalia and Somaliland stated that
following lockdown.
there has been an increase in FGC incidents compared to the
pre-COVID-19 period.30 Additionally, NAFIS (Somaliland National In addition to schools and churches, lockdown orders have also
Network Against FGM/C) are reporting a sustantial increase resulted in the closure of essential safe spaces in relation to GBV
in calls reporting FGC incidents,31 which are usually carried including refuges, safe houses, and women’s shelters across the
out during school holidays or the rainy season, indicating that region, which provided vital alternatives for women and girls
communities are using lockdown as an opportunity to cut girls at risk of GBV including FGC. In Kenya, a circular issued by the
and provide adequate healing time. Restrictions on movement Ministry of Labour and Social Protection, in response to COVID-19,
and lockdown in Puntland, Somalia have reportedly enabled FGC ordered the blanket closure of safe houses and refuges across
to take place more easily, whilst a lack of lockdown enforcement Kenya without consultation of NGOs and CSOs providing such
in Hargeisa has reportedly allowed ‘cutters’ to visit up to seven services. Whilst some rescue homes have remained open across
houses a day to perform FGC.32 Kenya, including in Nairobi, most centres are unable to admit
new cases and cope with current increased demand for services
In Kenya, media accounts from West Pokot have also recorded
whilst also struggling with limited funding. As few alternatives for
a “dramatic” rise in FGC cases, with 500 cases of FGC reported
girls at risk are currently available, one organisation in Kuria has
during the lockdown period.33 An increase in girls being cut in
reported that local activists have to care for girls at risk in their
Tanzania has also been noted by the Pastoral Women’s Council,
own homes, despite the already increased strain on financial
10 Impacts of COVID-19 on female genital cuttingresources. A similar situation has been reported in the Arusha
region of Tanzania, where most safe houses and rescue centres
IMPACT ON SOCIAL AND GENDER
are either closed or lack funding, leading to one rescue centre NORMS
having to shut down entirely.
Activists have reported that the rise of COVID-19 is resulting in
the reemergence of harmful social norms underpinning gender
ESSENTIAL SERVICES inequality and practices including FGC. In Narok county, Kenya,
organisations are reporting that a rise in teenage pregnancy
Activists and organisations across the region are also reporting rates is reinforcing beliefs that FGC reduces sexual urges of
significant barriers to accessing essential sexual and reproductive women, leading many communities to embrace FGC as a
health services across Kenya and Tanzania. The practice of FGC means of reducing early pregnancy during COVID-19. In Kuria
can often lead to acute infection in survivors, but supply chains East, partners have cautioned that community elders believe
and access to medical commodities have been substantially COVID-19 is a punishment sent by the Kurian gods, who are angry
interrupted owing to lockdown and a centralised approach to at the perceived abandonment of traditional culture, including
commodity procurement based in Nairobi. Access to services FGC. Elders are now spreading the message to communities
is also being reduced across Kenya to telephone consultations, that a return to cultural rites including FGC will appease the
which present accessibility issues for women and girls in remote gods and prevent COVID-19. Local activists are concerned that
and rural areas, who may not have access to a telephone. Equally, these messages are likely to be spread and received across Kuria.
a lack of PPE for women and girls trying to access services has Communities have also cited beliefs that COVID-19 is “only for the
created an additional barrier, whereby both service providers and poor” or those who live in cities who have abandoned traditional
patients lack adequate resources to carry out services in a safe gods and culture.
environment. Local activists across both Kenya and Tanzania have
reported a general de-prioritisation of FGC services in favour of
responding directly to COVID-19.
ECONOMIC IMPACTS
The economic impacts of COVID-19 are also contributing to an
increase in FGC practices across Kenya in particular. In the Rift
Valley, a general loss of livelihoods across communities has
triggered an increase in FGC as a precursor to child or early
marriage to fetch a higher bride price. Concerns have also been
raised that former cutters whose incomes are also at risk may
return to cutting, with reports from Plan International in Somalia
noting that former cutters are reportedly going from house to
house to perform FGC services in Mogadishu.35
Monitoring and reporting of FGC cases has also been significantly
impacted by COVID-19. Whilst specific hotlines are available and
run by either NGOs or the government across Kenya and Tanzania,
activists are reporting increased usage of hotlines, but limited
or ineffective means of following up reports with verification or
enforcement action. Activists in Kenya note that there is poor
coordination of hotlines and reporting at county level, including
case management mechanisms and referral pathways, whilst a
reliance on telephone reporting presents accessibility issues for
women and girls in remote or rural areas. Courts in Kenya are
either not in session or have a substantial backlog of cases, and
in Kuria, law enforcement is being redirected to enforce curfews
and COVID-19 responses. Reports from Rift Valley note that
government child protection officers are becoming hostile to
anyone reporting FGC, and that police officers are overwhelmed.
30
UNFPA (2020) ‘GBV/FGM Rapid Assessment Report: In the Context of COVID-19 Pandemic in Somalia’
31
Plan International (2020) ‘Girls in Somalia subjected to door-to-door FGM’
32
The Guardian (2020) ‘Huge FGM rise recorded in Somalia during coronavirus lockdown’
33
Daily Nation Kenya (2020) ‘West Pokot records dramatic rise in FGM cases’
Impacts of COVID-19 on female genital cutting 11NATALIE ROBI TINGO, FOUNDER OF MSICHANA EMPOWERMENT,
KURIA, KENYA
Natalie lives and works in Kuria, a rural area of southern Kenya, where prevalence of FGC may be as high as 96%.34 Under the
increasing pressure of a global pandemic, Natalie is continuing her work to empower girls by providing sanitary products and
preventing FGC.
“Where I am, calamities such as COVID often make cutting ceremonies of girls and boys much bigger because of the belief that
we need to appease the gods. Usually, the cutting season starts around August, but I heard young men chanting just this last
week (June), which signals that the elders have said the cutting season should begin already.
We are staying open because it’s more important than ever to break the cycle. If a girl has access to menstrual care, she has
better options than trading sex for a sanitary pad. If we break the cycle of undergoing FGM/C, the risk of child marriage slowly
goes away.
Under COVID, the global conversation has been about ‘how do we use technology to mitigate these things.’ But many of the girls
we work with are not online. We need to strengthen the systems we already have. Make services affordable and accessible, and
ensure the community is responsive.
Natalie Robi Tingo stands with a group of Kurian schoolgirls. Msichana Women’s Empowerment, Kuria, Kenya, 2020.
Feed the Minds (2014) ‘Female Genital Mutilation practices in Kenya: The role of Alternative Rites of Passage. A case study of Kisii and Kuria districts’
34
Plan International (2020) ‘Girls in Somalia subjected to door-to-door FGM’
35
12 Impacts of COVID-19 on female genital cuttingAsia
MONITORING AND REPORTING
Where activists and organisations were carrying out programmatic
activities with communities to end FGC, lockdown and stay-at-
home orders have prohibited further work at this time. Travel
restrictions mean that carrying out community-based activities
is extremely difficult, whilst organisations with monitoring and
reporting mandates have been unable to verify information
and collect real-time data. The reality across Asia is that most
organisations and activists don’t have access to vital information
about the situation facing women and girls at risk of FGC.
Conversely, anecdotal reports made by activists across Indonesia
OVERALL TRENDS and Malaysia suggest that lockdowns may have resulted in
the cancellation or postponement of large, ritualistic FGC
The reality across Asia is that most organisations and activists ceremonies, for example in Gorontalo province, as the economic
don’t have access to vital information about the situation impacts of COVID-19 lead communities to re-prioritise resources
facing women and girls at risk of FGC. No country across Asia away from expensive ceremonies towards basic needs. However,
has legislated to ban FGC, despite significant incidence rates in activists and organisations stress that verifying these reports is
certain countries and credible evidence of the practice taking difficult if not impossible during lockdown, and note that a lack of
place across the region.36 As a result, protection and deterrence policing during COVID-19 may also mean that ceremonies simply
that would be provided by law enforcement are unavailable go ahead as normal.
to women and girls at risk or survivors of FGC. Advocacy and
programmatic work to end FGC in Asia is broadly hampered in
ordinary circumstances by considerable lack of recognition that
ESSENTIAL SERVICES
the practice exists by local governments, and to a lesser extent,
the international community. Resourcing and programming to Access to essential services is also heavily restricted across the
end the practice in Asia are extremely limited, so the impact of Asia region. In Malaysia, family planning clinics have had to scale
the COVID-19 pandemic on activities to end FGC have been less down or postpone their work indefinitely, as health services only
significant than in West and East Africa. offer COVID-19 related services, despite survivors of FGC being
reliant upon broader access to SRHR services. In Indonesia,
service providers and safe houses have been closed.
IMPACT ON SOCIAL AND GENDER
NORMS
The emergence of COVID-19 has, however, made it even more
difficult for activists and organisations working to end FGC in the
region. One partner based in a rural community in Sumatra Utara,
Indonesia, has raised concerns about the impact of lockdown on
social norms in rural or isolated communities, where traditional
and dominant views around FGC - such as it controlling women’s
sexuality - are not being challenged as a result of community
isolation during this period.
36
Orchid Project (2020) ‘Asia Network to End FGM/C Consultation report’
Impacts of COVID-19 on female genital cutting 13Impact of COVID-19 on trends in FGC
IMPACT OF COVID-19 ON COVID-19 may provide an opportunity to
MEDICALISATION OF FGC interrupt increasing trends of medicalisation
by capitalising on the perceived understanding
Whilst lockdowns and stay-at-home orders have widely resulted that FGC is not ‘essential’, and is in fact a
in a loss of prevention, protection and support services to women
and girls at risk or survivors of FGC, a lack of access to services may violation of the rights of women and girls.
be driving down rates of medicalised FGC (FGC performed by a
medical professional). Reports from organisations across Nigeria,
where 12.7% of FGC is carried out by a medical professional,37 IMPACT OF COVID-19 ON CROSS-
note that lockdown orders and restrictions on movement mean
that families across Enugu State have been unable to travel to
BORDER CUTTING
clinics or health facilities to access FGC services.
Varying levels of response to COVID-19 across international
borders is likely to have impacts on cross-border cutting. The
phenomenon of cross-border cutting is well-documented and of
“People are unable to go to the hospitals particular concern in normal circumstances where communities
where medicalised FGM is practiced and cross national borders to carry out FGC in a country where the
even if they can find their way to the hospitals, practice is legal or in hopes of avoiding authorities.38 Kenya’s Anti-
the attention of the health care providers have FGM Law is well regarded as one of the most robust and stringent
been diverted to focusing on the pandemic. pieces of legislation making the practice illegal to carry out,
with mandatory reporting requirements and the application of
If this happens, efforts should be made to extraterritorial jurisdiction. Border communities routinely cross
maintain this positive achievement even into neighbouring countries to carry out the practice.
beyond this pandemic.” Local activists working in communities along the Kenya-Tanzania
- HACEY Health Initiative, Nigeria border have noted the impact that different national approaches
towards COVID-19 have had on the practice of FGC. Whilst
Kenya moved to enact stricter forms of lockdown and issued
In cases where families do arrive at medical facilities, one partner stay-at-home orders, Tanzania’s President Magufuli has advised
notes that the prioritisation of COVID-19 by healthcare workers citizens that religious faith can prevent or cure COVID-19, whilst
means that FGC services are unlikely to be provided in a medical encouraging public gatherings.39 Subsequent higher rates of
setting. Equally, reports from Malaysia and Indonesia, where infection across the Tanzanian border have led to fears within
FGC is routinely offered by midwives as part of ‘birth packages’, the Kenyan Loita community that Tanzanians will bring COVID-19
suggest that clinics where such services are offered are closed or across the border.
offering ‘essential’ services only. In such circumstances, COVID-19
may provide an opportunity to interrupt increasing trends of
medicalisation by capitalising on the perceived understanding
that FGC is not ‘essential’, and is in fact a violation of the rights
of women and girls. COVID-19 may provide an opportunity to
interrupt increasing trends of medicalisation by capitalising on
the perceived understanding that FGC is not ‘essential’, and is in
fact a violation of the rights of women and girls. However, the
possibility of health service providers switching to private
settings - such as homes - to carry out the practice cannot be
ruled out.
37
UNFPA (2013) ‘Female Genital Mutilation (FGM) Dashboard - Nigeria’
38
UNFPA (2019) ‘Beyond the Crossing: Female Gential Mutilation Across Borders’
39
Chatham House (2020) ‘Expert Comment: Tanzania Evades COVID-19 Lockdown, but Restrictions Persist’
14 Impacts of COVID-19 on female genital cuttingImpacts of COVID-19 on grassroots
organisations working to end FGC
Beyond the direct impacts of COVID-19 on rates and having to be drastically scaled back or reduced to accommodate
modalities of the practice of FGC itself, the pandemic and health and safety concerns around virus transmission. One
governmental responses to contain COVID-19 are largely organisation in Narok, Kenya notes that social distancing concerns
acknowledged to have had considerable negative impacts could be effectively managed if adequate PPE were provided and
on the functioning of CSOs and activists working to end the available, including face masks, soap and hand sanitizer.
practice. UNFPA has estimated that COVID-19 has resulted
Organisations and activists carrying out varying forms of vital
in a delay to one third of programmatic activities aimed at
work to end FGC are also being impacted in different ways
ending FGC,40 although grassroots activists and organisations
by lockdown. Despite the vital need for research and data
have also reported broader challenges in their work as a
collection - particularly across the Asia region, lockdown has led
result of the pandemic.
to research being put on hold or delayed as collection methods
are unsuitable for remote surveying. Organisations across East
RESTRICTIONS ON CSO ACTIVITIES Africa have also noted that rescue centres are unable to reach
out to girls at risk or to offer protection from FGC, whilst clinics
and health services operating in Malaysia have been shut down
Almost all grassroots organisations and activists across all regions
or have had to scale down services and training. Organisations
have reported severe restrictions placed on programmatic
with a monitoring or reporting mandate, including across Kenya
activities as a result of stay at home orders and social distancing
and Indonesia, have reported that restrictions on movement
measures. Restrictions on travel and movement are preventing a
prevent adequate monitoring of potential FGC cases, making it
wide range of organisations that are not community-based from
difficult to accurately assess and verify cases in real-time, creating
accessing communities to carry out vital social norms-based work
considerable impacts for urgent response requirements.
to end the practice, including Orchid Project partners; Tostan
(Senegal), Kalyanamitra (Indonesia), and COVAW (Kenya). Where
organisations and activists are community-based, social distancing
rules mean that their usual activities including women’s forums,
community dialogues, training and capacity building activities are
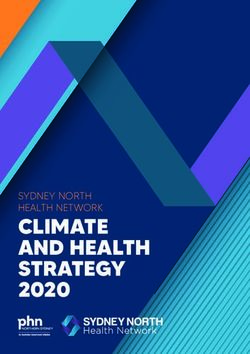
RESPONSES BY GRASSROOTS ACTIVISTS AND
ORGANISATIONAL AND INDIRECT IMPACTS OF ORGANISATIONS ON SUPPORT NEEDED TO RESPOND
Responses by grassroots activists and organisations on support
Organisational
COVID-19 REPORTEDand BYindirect impacts ofACTIVISTS
GRASSROOTS COVID-19 TO THE IMPACTS OF COVID-19 ON FGC
needed to respond to the impacts of COVID-19 on FGC
reported by grassroots activists
20 20
18 18
16 16
Number of responses
Number of responses
14 14
12 12
10 10
8 8
6 6
4 4
2 2
0 0
Restrictions on Reductions in Connectivity Staff Lack of basic Urgent Capacity Provision of Classifying Increased Integrating
programming funding problems wellbeing necessities, flexible building and PPE FGC media FGC within
e.g. PPE emergency technical prevention attention on crisis
funding assistance and FGC response and
response as recovery
'essential'
services
40
UNFPA (2020) ‘Impact of the COVID-19 Pandemic on Family Planning and Ending Gender-based Violence, Female Genital Mutilation and Child Marriage’
Impacts of COVID-19 on female genital cutting 15are unable to directly access communities to carry out
“COVID-19 has reduced physical access to programming activities such as community dialogues, a shift
communities and households as all individuals towards online communications is hampered by unequal access to
are advised to take responsibility. However, technology, including internet access. For example, organisations
operating in various parts of rural Kenya and Indonesia report
with funding and provision of PPE, community that communities have limited access to internet or technology
interventions can take place within proper such as mobile phones, and the gender digital divide in particular
WHO guidelines. Funding is also needed for limits access considerably for women and girls most at risk of
online advocacy, therapy, and counseling FGC. Organisations and activists themselves operating in rural or
services.” impoverished areas equally report a lack of internet access and
technology to carry out their own work online. Furthermore,
- One Voice Initiative For Women and Children shifting towards online communication methods are not cost-
Emancipation, Nigeria neutral. Whilst the use of radio-based communications has
worked well for a number of organisations in Kenya, many
grassroots activists report that they simply cannot afford to buy
radio airtime. In Nigeria, organisations working to end FGC have
been hampered in communicating with community activists due
to lack of mobile phones and inadequate funding to provide this.
URGENT LACK OF FUNDING
Underlying many of the factors preventing programmatic activity
is the reality that many grassroots organisations and activists are
experiencing a dire lack of funding to cope with the increased
risks of FGC, alongside a need for new ways of working to end the
The SAFE Samburu team pose for a photograph wearing PPE. Samburu, practice during a pandemic. The knock-on impacts of COVID-19
Kenya, 2020.
on local and national economies have led to price rises in food
and basic necessities, including essential commodities such as
PPE. Organisations are reporting a reduction in donor funding
S.A.F.E. KENYA at this time as donors shift attention away from FGC in favour
of responding directly to COVID-19 and its health impacts. One
SAFE Maa and SAFE Samburu have been working in organisation in Rift Valley, Kenya, has had to send staff home with
Loita Hills and Samburu during Kenya’s COVID-19 curfew half of their usual salaries amid depleting donor funding, whilst
whilst trying to mitigate social distancing impacts on vital staff are having to additionally accommodate girls at risk within
community-based activities. With authorisation from their own homes at personal cost. One organisation in Kenya has
local government, both S.A.F.E. teams have been able to had to close down due to lack of funding, whilst another two
continue their community workshops by sharing public organisations in Indonesia and Tanzania are also at imminent risk
health information on social distancing and handwashing, of closure as a result of diminishing funding.
alongside facilitating dialogue on FGC. To abide by social
distancing rules, capacity has been reduced for the
number of participants, which has led to full participation
of community members and a deeper dialogue on FGC. “Funding for grassroots organisations is now
S.A.F.E. have also adapted their flagship performance tours, key - if we are to reduce FGM prevalence
which usually encourage large audiences in marketplaces within the COVID-19 context. The Anti-
and school settings. Instead, they have utilised the power FGM Board, UN Organisations and other
of film to share their performances through screenings at
key stakeholders need to ensure that matters
local homesteads as a tool to engage families in dialogue on
FGC, as well as sharing on social media to reach national and pertaining to policy and advocacy is done at
international audiences. all levels to ensure integration of FGM within
current COVID-19 country responses.”
- GirlVanize, Kenya
UTILISING TECHNOLOGY
Grassroots organisations and activists have also reported
considerable challenges utilising or adapting to technology to
continue community-based programming. Where organisations
16 Impacts of COVID-19 on female genital cuttingDE-PRIORITISATION OF FGC
In addition to a diversion and reduction in funding for work to end FGC, activists are reporting a broader de-prioritisation of FGC in terms
of media attention and political will to engage with the issue, resulting in the issue all but disappearing from the public agenda. Despite
global recognition of the ‘shadow pandemic’ of GBV resulting from COVID-19, local authorities in Narok, Kenya have shifted their entire
focus to respond directly to COVID-19, with the result that “FGC is a non-issue at the moment”. This phenomenon has been particularly
striking across the Asia region, where activists have struggled for years to get governmental recognition of the practice onto political
agendas. Activists in Sri Lanka have noted a general difficulty in engaging with the police on violence against women, where complainants
are being turned away, and activists across Sri Lanka, Pakistan and Singapore note that advocacy on FGC is being scaled back as a result of
governments cautioning that “now is not the time” to be discussing FGC. In Iran, activists cannot speak openly about FGC in public, and
media outlets will no longer engage with the issue.
Dr Chris Ugwu stands with community members in facemarks with COVID-19 posters. SIRP, Enugu State, Nigeria, 2020.
“We need financial support to keep reaching communities with the sensitisation of COVID-19 and to
provide food to households, this is because poverty is the root cause of FGC and child marriage, and
now most households don’t go to work. We need financial support so that we can get the resources
required to hold forums on the need to end FGC, and to also keep educating the community on the
prevention measures of COVID 19.”
- Maasai Mara Women Empowerment Guide Organisation, Kenya
Impacts of COVID-19 on female genital cutting 17Mitigating strategies and best practices: How grassroots
organisations and activists are adapting to COVID-19
● Reducing the numbers of participants in community-based programme initiatives
SOCIALLY DISTANCED
● Holding community-based meetings in open, outdoor spaces
PROGRAMMING ● Provision and utilisation of adequate and effective PPE.
● Terrain tools to map rural areas and access to remote communities, such as
MAPPING OpenStreetMap and Missing Maps.
● UReport polling- free SMS-based technology for surveys and data collection.
REMOTE SURVEYING
AND DATA COLLECTION
● Greater usage of WhatsApp, social media and communication platforms to
DIGITAL organise, mobilise, and share key information
TECHNOLOGIES ● Creation of digital and mobile phone apps to stimulate dialogue and social norms
change
● Sharing pre-recorded podcasts through bluetooth for non-smartphone users.
Poverty is a key driver of FGC in some contexts. The economic shock from lockdowns has
HUMANITARIAN led grassroot activists to provide:
ASSISTANCE ● Food parcels
● Hand crafting face masks and PPE
● Provision of menstrual products
● Provision of soap and community advice on hygiene to avert COVID-19
● Housing girls at risk of FGC in activists’ own houses.
● Collating lists of service providers and maintaining updated referral pathways
SERVICE
PROVISION ● Hotlines for girls at risk of FGC and gender-based violence
● Community-based protection, community surveillance schemes, use of WhatsApp
● Rescue brigades42
● Shelters and refuges for women and girls at risk- activists are reporting housing
girls at risk in their own homes.
Many organisations have developed communications campaigns to promote FGC
BEHAVIOUR CHANGE abandonment to people subject to stay-at-home orders and curfews:
COMMUNICATIONS ● Use of radio time to promote messages on ending FGC
● Radio and TV ‘jingles’
● Poster campaigns
● Sponsored advertisements on social media.41
41
UNICEF Nigeria reached 1.1 million users in a 4 week period as part of the Spotlight Initiative in Nigeria during lockdown
18 Impacts of COVID-19 on female genital cuttingMITIGATING STRATEGIES EMPLOYED BY GRASSROOTS
ACTIVISTS
Responses byAND ORGANISATIONS
grassroots TO RESPOND
activists and organisations TO THE
on support “While girls and family members stay home,
IMPACTS
needed OF COVID-19
to respond ON
to the FGC of COVID-19 on FGC
impacts
the most immediate channel of getting
12 information is through radio. Parents are glued
10 to their radio to follow COVID-19 updates
8
6
from the government and children are taking
4 virtual classes through the radio teaching
2
program. This presents a huge opportunity
0
Using online Shifting to Adapting Providing Have not to use this same medium to transmit vital
communication behaviour programming humanitarian found it
tools change for social assistance possible to information about the impact of the practice
communications distancing adapt
and the importance of protecting and
upholding girls’ rights. Purposeful is currently
using this same channel to engage girls,
SAHIYO, INDIA & USA address issues and transmit vital information
to keep girls and their families safe from
Before the coronavirus pandemic hit, much of
COVID-19. The temporary ban on all secret
Sahiyo’s work involved working with activists and
community members through in-person retreats and societies presents an opportunity to hold the
Thaal Pe Charchas – conversations over food. In the community accountable in the event of secret
current climate, Sahiyo has needed to pivot and work initiation. Though we are not sure how this is
increasingly through technology and digital spaces. The monitored.”
organisation has been able to work to their strengths
as communicators at this time, and use digital spaces - Purposeful, Sierra Leone
to convey messages to great success. They’ve held
webinars with over 300 people in attendance and
continue to share survivor stories on their social
channels through a project with the StoryCentre;
Voices to End FGM/C.
Community members discuss FGC during a ‘Thaal Per Charcha’ (conversations over food). Sahiyo, India, 2018.
42
The rescue brigade model has proven effective in humanitarian crises and consists of women’s rights/anti-FGC activists and youth service providers responding to cases of GBV and FGC
through formal or informal referral mechanisms and providing referrals for survivors. Rescue brigades can play a critical role in raising awareness about GBV and FGC during the COVID-19
pandemic as well as provide referral pathways to communities.
Impacts of COVID-19 on female genital cutting 19You can also read