Impact of Kangaroo Mother Care Intervention on Immunological and Pulmonary Functions of Preterm Infants during Breastfeeding
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Hindawi
Evidence-Based Complementary and Alternative Medicine
Volume 2022, Article ID 3180871, 7 pages
https://doi.org/10.1155/2022/3180871
Research Article
Impact of Kangaroo Mother Care Intervention on
Immunological and Pulmonary Functions of Preterm
Infants during Breastfeeding
Juan Yang ,1 Yanan Guo,2 and Yuying Dai3
1
Department of Children Health Care & Breast-feeding, The Fourth Hospital of Shijiazhuang City, Shijiazhuang, China
2
Department of Pathogenic Biology, Chongqing Medical University, Chongqing, China
3
Obstetrics Department, Wei County Hospital of Traditional Chinese Medicine, Kaifeng, China
Correspondence should be addressed to Juan Yang; yangjuan@sjzhospital.net
Received 6 April 2022; Revised 7 May 2022; Accepted 11 May 2022; Published 19 May 2022
Academic Editor: Fenglin Liu
Copyright © 2022 Juan Yang et al. This is an open access article distributed under the Creative Commons Attribution License,
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Objective. Preterm infants (PTIs) are prone to respiratory failure or other diseases due to immature organ development and poor
immunological function. Herein, the effects of Kangaroo Mother Care (KMC) on the immunological and pulmonary functions of
PTIs during breastfeeding were investigated in this study. Methods. The study recruited 86 delivery women and their PTIs with
preterm pregnancy outcomes, consisting of 46 cases receiving breastfeeding plus KMC intervention (KMC group) and 40 cases
receiving breastfeeding plus routine care (control group). The time of first lactation, time of first breastfeeding, and duration of
first breastfeeding were observed in both cohorts. The breastfeeding status was assessed using the LATCH system. Maternal
psychological status was evaluated by the breastfeeding self-efficacy scale (BSES) and self-rating anxiety/depression scale (SAS/
SDS). The growth and development of PTIs were recorded, and the levels of postalbumin (PA), transferrin (TRF), plasma albumin
(ALB), immunoglobulin (Ig) A, IgG, IgM, and complement C3 and C4 were measured. The tidal volume (VT), tidal volume per
kilogram (VT/kg), minute volume (MV), and minute volume per kilogram (MV/kg) were detected using a pulmonary function
tester. Results. The KMC group presented shorter time of first lactation and first breastfeeding than the control group, with longer
duration of first breastfeeding (P < 0.05). After intervention, the BSES scores of delivery women were increased, while the SAS and
SDS scores were decreased, with more notable improvements in the KMC group (P < 0.05). The levels of PA, TRF, ALB, IgA, IgG,
VT, and MV were elevated in PTIs in both groups, with more evident increase in the KMC group than in the control group
(P < 0.05). A better growth of PTIs was found in the KMC group than the control group (P < 0.05). Conclusions. The study
demonstrated that KMC intervention during breastfeeding could benefit PTIs specifically regarding their immunological and
pulmonary functions.
1. Introduction others have adverse outcomes due to various diseases or
improper nursing, which is an important factor causing
Unlike normal infants, preterm infants (PTIs) have a shorter premature infant death [3]. According to statistics, the global
gestational age, lower weight, and immature organ devel- mortality rate of PTIs has reached 20.8%, showing an in-
opment, which predispose them to be complicated with creasing trend [4]. PTIs with very low birthweight have an
other diseases, threatening the healthy development of increased risk of abnormal lung function, particularly ob-
newborns [1]. With the change of policies as well as some structive type and thoracic musculoskeletal abnormalities,
incentives such as the increase of elderly pregnant women which were related with alternations in lung function [5].
and pregnancy complications in recent years, the premature Additionally, PTIs born before 32 weeks’ gestational age
birth rate has gradually increased, accounting for 5%–15% of have high rates of late onset sepsis and necrotizing en-
the total number of deliveries [2]. Some premature babies terocolitis, which may be associated with both the infant’s
have a good prognosis after positive treatment, while some immune system and the developing gut microbiota [6].2 Evidence-Based Complementary and Alternative Medicine
Breast milk, the best natural nutritional supplement for semi-recumbent position, the child was placed naked be-
newborns and the first choice for clinical treatment of PTIs, tween the mother’s bare breasts. The mother placed one
is of great significance to increase neonatal immunity and hand on the patient’s back covered with a clean thin back,
promote neonatal growth and development [7]. However, and the other hand supported the patient’s buttocks to
due to the poor condition of the child, pregnant women tend prevent the patient from sliding down. In this way, the child
to develop anxiety and other negative emotions after de- can fully feel the mother’s smell and body temperature,
livery, which directly affects the maternal lactation function, thereby enhancing the emotional communication between
leading to the reduction of the success rate of breastfeeding the mother and the child, and stimulating the maternal
[8]. As the research deepens, the combination of effective lactation function. In addition, the medical staff paid close
interventions on the basis of conventional treatment has attention to the vital signs of the child, corrected the
been found to exert a positive impact on the health level of mother’s practice in a timely manner, and encouraged the
delivery women and newborns. Kangaroo Mother Care mother to communicate with the child softly. Finally, under
(KMC), a way to imitate the animal kangaroo to take care of the guidance of medical staff, the infant was helped to suck as
children, allows the delivery women to get in close contact early as possible. The initial KMC intervention lasted for half
with their infants as early as possible to shorten the inter- an hour, followed by two periods of 2 h at noon (generally 9:
dependent relationship between them, which is extremely 00–11:00) and 2 h in the afternoon (14:00–16:00). In the case
suitable for PTIs. At present, it has been fully put into clinical of blood collection of children, the duration of KMC in-
use in many countries with excellent application results tervention was extended. The sucking reflex was established
[9, 10]. However, the research on KMC is in the theoretical as early as possible, and the child’s health was gradually
guidance stage in China due to study on starting late, and restored. The control group: after birth, the nursing staff
there is still no comprehensive and abundant experimental carried out airway cleaning, body cleansing, infection pre-
evidence on the specific function improvement of KMC in vention, and measurement of body length, weight, and head
PTIs, resulting in it not being widely used in clinical practice. circumference for the baby. The PTIs were placed in in-
Based on this, this study studies the improvement effect of cubators at 32–34°C for real-time monitoring of vital signs.
KMC on the immunological function and pulmonary As for the mothers, health education and psychological
function of PTIs under breastfeeding, laying a reliable counseling were provided so that they could understand the
foundation for future application of KMC. importance of breastfeeding until they could breastfeed. The
treatment lasted for two weeks in both cohorts.
2. Methods
2.3. Detection Methods. The venous blood (3 mL) was
2.1. Enrollment of Study Subjects. After being reviewed and extracted from included PTIs before and after intervention
approval by the Ethics Committee of our hospital, 86 cases of for the measurement of albumin (PA), transferrin (TRF),
delivery women and their PTIs with premature pregnancy plasma albumin (ALB), immunoglobulin (Ig) A, IgG, IgM,
outcomes in our hospital from March 2019 to August 2021 and complement C3 and C4 levels with the use of an au-
were selected for the study. Among them, 46 cases receiving tomatic biochemical analyzer. Besides, the tidal volume
KMC intervention during breastfeeding were assigned to the (VT), tidal volume per kilogram (VT/kg), minute volume
KMC group and 40 cases receiving routine intervention (MV), and minute volume per kilogram (MV/kg) were
during breastfeeding were assigned to the control group. We detected using a pulmonary function tester.
obtained informed consent from all family members. In-
cluded PTIs must fulfill the following criteria: (i) gestational
age of 28 to 37 weeks; (ii) birth weightEvidence-Based Complementary and Alternative Medicine 3
complement C3 and C4. The pulmonary function of PTIs Table 1: Baseline data of delivery women and their PTIs.
was reflected by VT, VT/kg, MV, and MV/kg. When the KMC Control
delivery women were discharged from the hospital, they t or χ2 P
(n � 46) (n � 40)
were given anonymous nursing satisfaction surveys to show Maternal age (year) 28.37 ± 3.16 28.90 ± 3.20 0.771 0.443
their nursing satisfaction. The survey was conducted on a 10- Sex of newborn,
point scale, with 10 being very satisfied, 7–9 being basically 0.086 0.769
n (%)
satisfied, 4–6 being improvement needed, and 1–3 being Boy 25 (54.35%) 23 (57.50%)
dissatisfied [15]. Girl 21 (45.65%) 17 (42.50%)
Maternal BMI
28.19 ± 1.96 28.62 ± 1.15 1.217 0.227
(kg/cm2)
2.5. Statistics Processing. Data processing was made by Gestational age
SPSS23.0 (IBM, USA). Count data (expressed as percentage) 30.37 ± 1.78 30.63 ± 1.81 0.670 0.505
(week)
were analyzed by Chi-square test. Measurement data Weight at birth (g) 1742 ± 123 1723 ± 121
(expressed as mean ± standard deviation) were tested by Primiparity, n (%) 0.024 0.878
either paired or unpaired t-test. Statistical significance was Yes 28 (60.87%) 25 (62.50%)
assumed at P < 0.05. No 18 (39.13%) 15 (37.50%)
Nationality, n (%) 0.090 0.764
Han nationality 43 (53.48%) 38 (95.00%)
3. Results Minority 3 (6.52%) 2 (5.00%)
3.1. Baseline Data of Delivery Women and Their PTIs.
Demographic and clinical data of two groups of delivery
women and their PTIs were compared with regard to ma-
Table 2: KMC intervention benefits breastfeeding status of PTIs.
ternal age and BMI, gender distribution of newborn, ges-
tational age, weight at birth, primiparity, and nationality. It KMC Control
t P
was found that the KMC and control groups showed no (n � 46) (n � 40)
significant difference in terms of maternal age and BMI, The time of first
39.14 ± 3.97 45.71 ± 5.43 6.46 0.05), but all elevated significantly monary Functions of PTIs. It was found that the levels of IgA,
after intervention (P < 0.05). This elevation was more sig- IgG, IgM, C3, and C4 exhibited no notable differences be-
nificant in the KMC group than the control group (P < 0.05, tween the KMC group and the control group before in-
Figure 1). In comparison with the control group, the KMC tervention (P > 0.05), but all increased notably after
group presented a better growth status, showing in weight intervention (P < 0.05), with higher levels in the KMC group4 Evidence-Based Complementary and Alternative Medicine
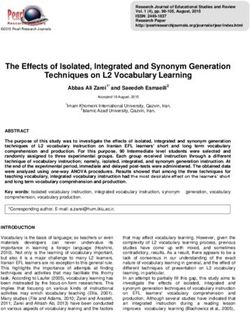
30 *# 50 50
*# *#
The TRF level (mg/L)
The PA level (mg/L)
The ALB level (g/L)
40 * 40
* *
20
30 30
20 20
10
10 10
0 0 0
Before After Before After Before After
KMC KMC KMC
Control Control Control
Figure 1: The serum levels of PA, TRF, and ALB in the PTIs after KMC intervention. ∗ P < 0.001 versus before intervention and #P < 0.001
versus the control group.
Table 4: The growth status of PTIs after KMC intervention. limits the effective implementation of breastfeeding [17].
KMC Control And as premature mothers have just completed pregnancy,
t P there are generally varying degrees of anxiety, depression,
(n � 46) (n � 40)
Weight gain (g/d) 4.29 ± 0.58 3.78 ± 0.42 4.61Evidence-Based Complementary and Alternative Medicine 5
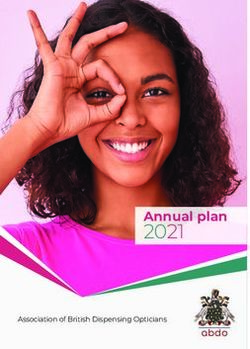
1.5 400
*#
*#
300 *
The IgG level (mg/dl)
The IgA level (mg/dl) *
1.0
200
0.5
100
0.0 0
Before After Before After
KMC KMC
Control Control
60 80
*#
*#
*
60
The IgM level (mg/dl)
The C3 level (mg/dl)
*
40
40
20
20
0 0
Before After Before After
KMC KMC
Control Control
40
*#
30 *
The C4 level (mg/dl)
20
10
0
Before After
KMC
Control
Figure 2: The serum levels of IgA, IgG, IgM, C3, and C4 in the PTIs after KMC intervention. ∗ P < 0.001 versus before intervention and
#
P < 0.001 versus the control group.
intervention [23], which can also corroborate the results of infants can stimulate skin receptors into the cerebral cortex,
this experiment. The main reasons for the difference in reduce nerve tension, and promote the secretion of neonatal
growth and development between groups, we speculate, may neurotransmitters, thus regulating the metabolism of growth
be the following: (1) early skin contact between mothers and hormone, thyroxine, and insulin levels. Besides, it can6 Evidence-Based Complementary and Alternative Medicine
Table 5: KMC intervention benefits the pulmonary function of PTIs after KMC intervention.
Time point KMC (n � 46) Control (n � 40)
Before intervention 15.01 ± 4.18 15.85 ± 4.61
VT (mL)
After intervention 24.79 ± 4.91∗# 20.91 ± 2.75∗
Before intervention 5.22 ± 0.74 5.38 ± 0.81
VT/kg (mL)
After intervention 7.74 ± 1.51∗# 6.43 ± 1.02∗
Before intervention 0.69 ± 0.08 0.68 ± 0.07
MV (L)
After intervention 1.55 ± 0.16∗ # 1.15 ± 0.08∗
Before intervention 0.23 ± 0.06 0.24 ± 0.05
MV/kg (L)
After intervention 0.46 ± 0.08∗ # 0.38 ± 0.07∗
∗
P < 0.001 versus before intervention and #P < 0.001 versus the control group.
Table 6: Maternal satisfaction survey results.
Very satisfied Basically satisfied Improvement needed Dissatisfied
KMC (n � 46) 39 (84.78) 7 (15.22) 0 (0.0) 0 (0.0)
Control (n � 40) 21 (52.50) 14 (35.00) 3 (7.50) 2 (5.00)
χ2 10.570 4.537 3.575 2.355
P 0.001 0.033 0.059 0.125
increase the catecholamine in newborns, promote the lung tissue and helping the lungs to achieve the optimal level
synthesis of glycogen, protein, and fat, and increase the of expansion and compliance [28]. This state can not only
intake of newborns [24]. (2) PTIs tend to lose heat easily due more reliably maintain the normal operation of pulmonary
to thin subcutaneous fat and rich and sensitive blood vessels function, but also enable the newborn to obtain a more
[25], while under the intervention of KMC, the amount of stable respiratory cycle, contributing to a higher quality of
autonomic activity and the consumption of oxygen and heat sleep and rest. Similarly, when Aagaard et al. performed
are decreased. At the same time, skin contact can transfer the KMC on neonates in the intensive care unit, they found
mother’s temperature to the newborn and keep the body more effective improvements in pulmonary function [29].
temperature constant, which is also conducive to physical Finally, the nursing satisfaction survey results of the two
growth. (3) Finally, the safe, stable, and warm environment groups demonstrated that the implementation of KMC in
created by KMC can stimulate the brain function devel- breastfeeding has gained higher recognition of the delivery
opment of neonates, which is conducive to the formation of women, which once again confirmed its potential for clinical
synapses. Therefore, the implementation of KMC in application.
breastfeeding can improve the growth and development of While providing a good guarantee for the immuno-
PTIs from multiple perspectives. logical function and pulmonary function of PTIs, the
Among the organ dysfunctions of PTIs, abnormal im- implementation of KMC under breastfeeding can effectively
munological function and pulmonary function are the most improve the efficiency of maternal breastfeeding and the
common manifestations, and their abnormality is usually growth and development of PTIs, which is worth promoting
the key to the occurrence of major infectious diseases, re- in clinical use. In the follow-up study, we will carry out a
spiratory arrest, and respiratory failure in PTIs [26]. In this longer follow-up investigation on delivery women and PTIs
study, we found effectively improved immunological in this study to analyze the long-term prognostic impact of
function and pulmonary function of both groups after in- KMC on PTIs. Second, it is necessary to increase the number
tervention, which highlighted the importance of breast- of research subjects so as to obtain more representative
feeding for the growth and development of PTIs. More results for clinical reference.
significant improvements were determined in the KMC
group, indicating that the implementation of KMC in Data Availability
breastfeeding has a more effective promotion effect. The
improvement, we speculate, may also be correlated with The data supporting the findings of this study are included in
prone sleep of KMC in addition to the above speculations. this article.
As is known to all, due to the incomplete development of the
respiratory system, PTIs may compress the lungs due to the Conflicts of Interest
heart, ribs, and other organs and tissues when they remain
supine or side lying, reducing the compliance of the lungs The authors declare that there are no conflicts of interest.
and making it more difficult for the originally incomplete
pulmonary function to operate [27]. By lying on the Authors’ Contributions
stomach, children can keep their lungs on top and their heart
on the bottom, thereby reducing the compression area of Juan Yang and Yanan Guo contributed to this work equally.Evidence-Based Complementary and Alternative Medicine 7
Acknowledgments [17] J. E. Harding, B. E. Cormack, T. Alexander, J. M. Alsweiler,
and F. H. Bloomfield, “Advances in nutrition of the newborn
The study was supported by Key Science and Technology infant,” The Lancet, vol. 389, no. 10079, pp. 1660–1668, 2017.
Research Plan of Department of Public Health in Hebei [18] C. L. Williams and C. J. Tann, “Global perspectives of pre-
Province (No. 20120230). mature birth across the life course,” The Lancet Child &
Adolescent Health, vol. 3, no. 6, pp. 370-371, 2019.
[19] G. J. Chan, B. Valsangkar, S. Kajeepeta, E. O. Boundy, and
References S. Wall, “What is kangaroo mother care? Systematic review of
the literature,” Journal of Global Health, vol. 6, no. 1, Article
[1] L. S. Owen, B. J. Manley, P. G. Davis, and L. W. Doyle, “The ID 010701, 2016.
evolution of modern respiratory care for preterm infants,” The [20] WHO, I. K. S. Group, S. Arya et al., “Immediate “kangaroo
Lancet, vol. 389, no. 10079, pp. 1649–1659, 2017. mother care” and survival of infants with low birth weight,”
[2] M. Brossard-Racine and C. Limperopoulos, “Cerebellar injury New England Journal of Medicine, vol. 384, no. 21,
in premature neonates: imaging findings and relationship pp. 2028–2038, 2021.
with outcome,” Seminars in Perinatology, vol. 45, no. 7, Article [21] A. Conde-Agudelo and J. L. Diaz-Rossello, “Kangaroo mother
ID 151470, 2021. care to reduce morbidity and mortality in low birthweight
[3] L. B. Boettcher and E. A. S. Clark, “Neonatal and childhood infants,” Cochrane Database of Systematic Reviews, vol. 8,
outcomes following preterm premature rupture of mem- Article ID CD002771, 2016.
branes,” Obstetrics & Gynecology Clinics of North America, [22] N. Charpak, R. Tessier, J. G. Ruiz et al., “Twenty-year follow-
vol. 47, no. 4, pp. 671–680, 2020. up of kangaroo mother care versus traditional care,” Pedi-
[4] J. L. Mehta and M. Bavineni, “Premature birth, infections, and atrics, vol. 139, no. 1, 2017.
atherosclerotic cardiovascular disease,” European Heart [23] M. Ramani, E. A. Choe, M. Major et al., “Kangaroo mother
Journal, vol. 40, no. 39, p. 3275, 2019. care for the prevention of neonatal hypothermia: a ran-
[5] A. S. Scavacini, J. Davidson, G. F. Wandalsen et al., “Asso- domized controlled trial in term neonates,” Archives of Dis-
ciation between thoracic musculoskeletal abnormalities and ease in Childhood, vol. 103, no. 5, pp. 492–497, 2018.
lung function in preterm infants,” The Clinical Respiratory [24] G. J. Chan, A. S. Labar, S. Wall, and R. Atun, “Kangaroo
Journal, vol. 14, no. 2, pp. 158–164, 2020. mother care: a systematic review of barriers and enablers,”
[6] T. Sproat, R. P. Payne, N. D. Embleton, J. Berrington, and Bulletin of the World Health Organization, vol. 94, no. 2,
S. Hambleton, “T cells in preterm infants and the influence of pp. 130–141, 2016.
milk diet,” Frontiers in Immunology, vol. 11, p. 1035, 2020. [25] A. G. Mekonnen, S. S. Yehualashet, and A. D. Bayleyegn, “The
[7] G. Mangili and E. Garzoli, “Feeding of preterm infants and effects of kangaroo mother care on the time to breastfeeding
fortification of breast milk,” La Pediatria Medica e Chirurgica, initiation among preterm and LBW infants: a meta-analysis of
vol. 39, no. 2, p. 158, 2017. published studies,” International Breastfeeding Journal,
[8] D. A. Gidrewicz and T. R. Fenton, “A systematic review and vol. 14, no. 1, p. 12, 2019.
meta-analysis of the nutrient content of preterm and term [26] R. D. Bogdan, L. Rusu, A. I. Toma, and L. Nastase, “Respi-
breast milk,” BMC Pediatrics, vol. 14, no. 1, p. 216, 2014. ratory outcome of the former premature infants,” Journal of
[9] E. O. Boundy, R. Dastjerdi, D. Spiegelman et al., “Kangaroo Medicine and Life, vol. 12, no. 4, pp. 381–394, 2019.
mother care and neonatal outcomes: a meta-analysis,” Pedi- [27] G. Erickson, N. R. Dobson, and C. E. Hunt, “Immature
atrics, vol. 137, no. 1, 2016. control of breathing and apnea of prematurity: the known and
[10] R. R. Kostandy and S. M. Ludington-Hoe, “The evolution of unknown,” Journal of Perinatology, vol. 41, no. 9,
the science of kangaroo (mother) care (skin-to-skin contact),” pp. 2111–2123, 2021.
Birth Defects Research, vol. 111, no. 15, pp. 1032–1043, 2019. [28] W. Durlak, M. Klimek, M. Wroński, A. Trybulska, and
[11] R. Romero, S. K. Dey, and S. J. Fisher, “Preterm labor: one P. Kwinta, “Multimodal longitudinal respiratory function
syndrome, many causes,” Science, vol. 345, no. 6198, assessment in very low birth weight 7-year-old children,”
pp. 760–765, 2014. Advances in Medical Sciences, vol. 66, no. 1, pp. 81–88, 2021.
[12] N. Altuntas, M. Kocak, S. Akkurt, H. C. Razi, and M. F. Kislal, [29] H. Aagaard, L. Uhrenfeldt, M. Spliid, and L. Fegran, “Parents’
“LATCH scores and milk intake in preterm and term infants: experiences of transition when their infants are discharged
a prospective comparative study,” Breastfeeding Medicine, from the neonatal intensive care unit: a systematic review
vol. 10, no. 2, pp. 96–101, 2015. protocol,” JBI Database of Systematic Reviews and Imple-
[13] M. Hines, N. Hardy, A. Martens, and E. Zimmerman, “Birth mentation Reports, vol. 13, no. 10, pp. 123–132, 2015.
order effects on breastfeeding self-efficacy, parent report of
problematic feeding and infant feeding abilities,” Journal of
Neonatal Nursing, vol. 28, no. 1, pp. 16–20, 2022.
[14] L. Gao, J. Qu, and A. Y. Wang, “Anxiety, depression and social
support in pregnant women with a history of recurrent
miscarriage: a cross-sectional study,” Journal of Reproductive
and Infant Psychology, vol. 38, no. 5, pp. 497–508, 2020.
[15] A. McNicholas, A. McCall, A. Werner, R. Wounderly,
E. Marinchak, and P. Jones, “Improving patient experience
through nursing satisfaction,” Journal of Trauma Nursing,
vol. 24, no. 6, pp. 371–375, 2017.
[16] Z. Z. Shen, Y. W. Wang, S. Ma et al., “Risk factors for preterm
birth, low birth weight and small for gestational age: a pro-
spective cohort study,” Zhonghua Liuxingbingxue Zazhi,
vol. 40, no. 9, pp. 1125–1129, 2019.You can also read