IC39-R: New Perspectives on Distal Radius Fractures: Tips and Tricks to Improve Care
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

IC39-R: New Perspectives on Distal Radius
Fractures: Tips and Tricks to Improve Care
Moderator: Marc J. Richard, MD
Faculty: Jacob Wade Brubacher, MD, Mihir J. Desai, MD, R. Glenn Gaston, MD and Robin Neil
Kamal, MD
Session Handouts
OnDemand
76TH ANNUAL MEETING OF THE ASSH
SEPTEMBER 30 – OCTOBER 2, 2021
SAN FRANCISCO, CA
822 West Washington Blvd
Chicago, IL 60607
Phone: (312) 880-1900
Web: www.assh.org
Email: meetings@assh.org
All property rights in the material presented, including common-law copyright, are expressly reserved to the speaker or the ASSH. No statement
or presentation made is to be regarded as dedicated to the public domain.
7/27/2021
Distal Radius Fractures
Radiographic Evaluation for Distal • Attention to fracture
pattern and distal
Radius Fractures radius morphology
can inform
treatment approach
Robin Kamal MD MBA
• Attention to other
Medical Director I Value Based Care and Orthopaedic Surgery
Associate Professor
injuries
Department of Orthopaedic Surgery
Stanford University
1 2
Anatomy Outline
✓Imaging – to inform fixation technique and intraop
decision making
✓Bridge Plate? Fragment Specific?
✓Volar Plate? Dorsal Plate
✓Carpal instability?
3 4
Imaging
✓Preoperative imaging
✓Dynamic carpal instability (SL)?
✓Are the screws prominent dorsally?
✓How do I know whether I’ve captured the volar
lunate facet?
✓Are the screws in the DRUJ?
✓Are the flexor tendons at risk?
5 6
1
7/27/2021
Preoperative Imaging Anterior Posterior Views
1) Other injuries to carpus? • 22 degree radial inclination
2) Intraarticular comminution? • (Sigmoid notch)
1) Can I reliably fix parts? • Dorsal radius 3-5 mm beyond volar
2) Do I need to look in the joint? rim
3) Volar lunate facet fragment? • This relationship can be inverted in
4) Metaphyseal comminution? dorsally angulated fractures (need
5) Other injuries lateral)
7 8
Lateral View
• AP distance ~ 20 mm males, 18
females • How do I manage
• Concern for widened lunate facet dynamic SL instability?
when > normal
• Displacement informs approach – • Cadaveric study with
Dorsal vs Volar confirmed SLIL injury
• Intercarpal injuries (SL) • >1 mm of diastasis of SL
with thumb traction of
5lb compared to normal
9 10
Imaging
✓Are the screws prominent dorsally? JHS 2012
✓How do I know whether I’ve captured the volar
lunate facet? No difference
between 75%
✓Are the screws in the DRUJ? length and full-
✓Are the flexor tendons at risk? length unicortical
or bicortical screws
11 12
2
7/27/2021
Recommendations
1) Drill to but not through the dorsal cortex (use 16/18 mm
screws)
2) Unicortical screw placement at least 75% of the A→P
distance
3) If concerned for dorsal subluxation of the carpus, use a
dorsal approach
13 14
JHS-Eur 2011 Possible Long Screw Penetrating the Dorsal
Cortex?
• 83% success determining 1mm too
long with skyline view as compared
to 77% for lateral and 50% for
oblique
• Specific but not sensitive!
• You can get false negatives!
15 16
Skyline View Imaging
Long Screw Through Dorsal Cortex
✓Are the screws prominent dorsally?
✓How do I know whether I’ve captured the volar
lunate facet?
✓Are the screws in the DRUJ?
✓Are the flexor tendons at risk?
17 18
3
7/27/2021
JBJS, 2004 JBJS, 2004
• Recognition of the critical • Recognition of the critical
anatomic areas of the anatomic areas of the
distal radius distal radius
• Outcomes linked to • Outcomes linked to
capture of the volar lunate capture of the volar lunate
facet facet
• Standard plates may not
capture → frag specific
• Attention to plate position
19 20
Anatomy Carpus → Distal Radius Kinetics
LRL SRL VRUL
21 22
Lateral View - Tear Drop (Angle)
• Volar projection of the lunate facet
seen on 10 degree lateral
• Serves as a mechanical buttress to
prevent lunate volar subluxation
• Projects at a 70 degree angle from
radial shaft
• Only 5 mm in width
• In this position, the AP distance is
similar to the AP distance of lunate
Fujitani et al JHS
23 24
4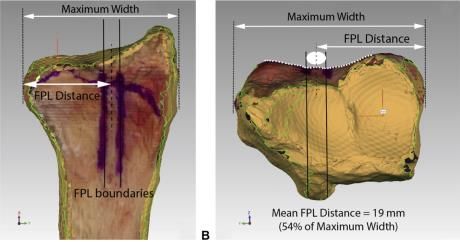
7/27/2021
• 15 mm size
• 5 mm initial displacement
• At Risk
• Consider fragment specific
plate or distal plate
Shapiro et al JOT
25 26
Imaging
✓Are the screws prominent dorsally?
✓How do I know whether I’ve captured the volar
lunate facet?
✓Are the screws in the DRUJ?
✓Are the flexor tendons at risk?
27 28
“Sigmoid Notch View”
• Live fluoroscopy until tangential
image of sigmoid notch is obtained
• Sigmoid notch view - cortical
overlap of the sigmoid notch
surfaces of the volar and dorsal
lunate facets
• Stripe of bone seen – “Sigmoid
Stripe”
29 30
5
7/27/2021
JHS 2018
CORRECT VIEW!
31 32
Imaging
✓Are the screws prominent dorsally?
✓How do I know whether I’ve captured the volar
lunate facet?
✓Are the screws in the DRUJ?
✓Are the flexor tendons at risk?
33 34
Volar Locking Plate Implant Prominence and Flexor Tendon
Rupture
Maximillian Soong, MD1; Brandon E. Earp, MD2; Gavin Bishop, MD3; Albert Leung, BS2; Philip
Blazar, MD JBJS
JHS 2014
Watershed line lies distally on the
intermediate column but
proximally on the radial column
35 36
6
7/27/2021
Flexor Tendon Injury
• Most reported instances of flexor tendon ruptures after
volar plating have involved
•Improper placement of the plate (radial column)
•Increased prominence of the distal edge of the plate bc of loss of reduction
• Use of non-anatomic plates
37 38
A plate that is placed too radial will create abnormal contact
between the plate and FPL
39 40
Plate Placement
Too Radial
Recommendations:
• Direct plate placement to the
volar lunate facet first
• Ensure plate is distal enough
based on lunate facet size
• Avoid distal and radial plate
placement
A plate that is placed too radial will create abnormal contact
between the plate and FPL
41 42
7
7/27/2021
Distal Radius Fractures Thank You
rnkamal@stanford.edu
• Use radiographic landmarks for planning
approach
• Use special fluoro views to assess for
other injuries – SL, carpal subluxation
• Use special fluoro vies for intraarticular
hardware
• Beware the small volar lunate facet
43 44
8
7/7/2021
The Osteoporotic Distal Radius Fracture: No disclosures
What Do I Do Next?
JACOB W B RUBACHER, M D
HAND AND UPPER EXTREMITY SURGERY
ASSISTANT PROFESSOR
UNIVERSITY OF KANSAS ORTHO AND SPORTS MEDICINE
1 2
Big Problem
The Osteoporotic Distal Radius Fracture:
▪ 2.1 million fractures per year
What Do I Do Next? ▪ 17 billion dollars health care spending
▪ 10 million Americans w/ osteoporosis
J A C OB W B R U B A CH E R , M D
▪ 1 out of every 2 Caucasian women
HAND AND UPPER EXTREMITY SURGERY will have osteoporosis-related fracture
ASSISTANT PROFESSOR
UNIVERSITY OF KANSAS ORTHO AND SPORTS MEDICINE
**The Joint Comission. Improving and Measuring Osteoporosis
Management [Monograph]. Oakbrook Terrace, IL: The Joint Commission; 2007.
*Watts NB, Lewiecki EM, Miller PD, Baim S. National Osteoporosis Foundation 2008
Image – Brilliant.com
3 4
Big Problem Big Problem – Small Response
▪ 2 million fractures ▪ Patients w/ fragility fracture
▪ 432,000 hospital admissions have 86% higher risk of a
second fracture
▪ 2.5 million medical office visits
▪ Only 20% with a fragility
▪ 180,000 nursing home admits fracture are screened
▪ Cost $25.3 billion by 2025 ▪ Once screened -> only 20%
get the needed therapy
Burge R, Dawson-Hughes B, Solomon DH, Wong JB, King AB, Tosteson A (2007) Incidence and economic burden of osteoporosisrelated
fractures in the United States, 2005–2025. J Bone Miner Res **The Joint Comission. Improving and Measuring Osteoporosis
22(3):465–475
Management [Monograph]. Oakbrook Terrace, IL: The Joint Commission; 2007.
Office of the Surgeon General (US) (2004) Bone health and osteoporosis: a report of the Surgeon General. Office of the Surgeon
General (US), Rockville (MD). *Watts NB, Lewiecki EM, Miller PD, Baim S. National Osteoporosis Foundation 2008 Clinician’s Guide to Prevention and Treatment of Osteoporosis and the World
Image – Ethendras - Wordpress
Health Organization Fracture Risk Assessment Tool (FRAX): what they mean to the bone densitometrist
and bone technologist. J Clin Densitom. 2008;11(4):473e477. Image – Study International
5 6
17/7/2021
MANDATE Why are you telling me this?
National Osteoporosis Foundation
Osteoporosis can be prevented, diagnosed, and treated
before fractures occur.
After the first fracture has occurred, there are effective
treatments to decrease the risk of further fractures.
Prevention, detection, and treatment of osteoporosis
should be a mandate of primary care providers.
https://fierceinc.com
7 8
• National post-fracture, systems-based, multidisciplinary fragility fracture
prevention initiative
• Quality improvement program to address the osteoporosis treatment gap
and prevent subsequent fragility fractures.
9 10
Know the Enemy
▪ Distal radius fractures - most common ▪ Low bone mass and disruption of bone
symptomatic fracture architecture
▪ Occur before potentially more debilitating hip ▪ Compromised bone strength, and an increase
or vertebral fractures. in the risk of fracture.
▪ Hand surgery clinic is valuable point of ▪ Most common bone disease in humans
intervention
▪ Only 5% to 20% of patient receive subsequent
medical consultation or pharmacotherapy
11 12
27/7/2021
Diagnosis
1. Measurement of BMD
▪ Bone remodeling - older bone replaced
with new bone. 2. Occurrence of adulthood hip or
vertebral fracture in the absence of
major trauma
▪ Bone loss – unbalanced, resulting in ◦ Laboratory testing is indicated to exclude secondary
greater bone removal than replacement. causes of osteoporosis
▪ Advanced age and menopause - the
rate of bone remodeling increases ->
magnifying the impact of the remodeling
imbalance.
13 14
What are the guidelines?
15 16
Who Should be Screened?
▪ Women age 65 and older and men age 70 and older
Retrospectively reviewed the medical records of ninety-five men and 344 women over the age of fifty years
who were treated for a distal radial fracture at a single institution over a five-year period.
▪ Postmenopausal women and men above age 50–69, based on risk
factor profile Assessed whether the patients had received (DXA) scan and osteoporosis treatment within six months
following the injury.
While 184 (53%) of the women had a DXA scan after injury, only seventeen (18%) of the men were evaluated
▪ Postmenopausal women and men age 50 and older who have had (p7/7/2021
DRF patients were offered a DXA scan and
endocrinology referral at initial hand surgery clinic visit.
Results • Medicare Standard Analytic File 2005-2014
Baseline period - 7 patients (15%) were screened, and
41 (85%) were not screened. • 37,473 patients w/ DRFx
- (26%) underwent BMD testing after fracture
35 patients met inclusion criteria. - Males (9%) less likely to be tested vs. females (30%)
80% - agreed to osteoporosis screening
64% were diagnosed with osteoporosis/osteopenia as • 1 in 5 patients went on to subsequent hip or vertebral compression fracture
a result of completing screening
• Patients who had testing had later time to fracture (819 versus 579 days)
• Females in BMD testing group had longer fracture-free interval
19 20
Who gets Pharmacotherapy? FRAX and Pharmacotherapy
Hip or vertebral (clinical or asymptomatic) fractures FRAX® calculate the 10-year
probability of a hip fracture AND major
T-scores ≤−2.5 at the femoral neck, total hip, or lumbar spine by DXA osteoporotic fracture
Postmenopausal women and men age 50 and older with: Cost-effective to treat individuals with
- low bone mass (T-score between −1.0 and −2.5 (osteopenia) a prior hip or vertebral fracture and
those with a DXA femoral neck T-score
- 10-year hip fracture probability ≥3 % or a 10-year major osteoporosis- ≤−2.5.
related fracture probability
Lumbar Spine T-score ≤−2.5 also
warrants treatment
21 22
Recommend treating postmenopausal women at high risk of fractures, especially those who
have experienced a recent fracture, with pharmacological therapies, as the benefits outweigh Routine treatment all women over age of 65 with DRFX with bisphosphonates:
the risks. - Avoid 94,888 lifetime hip fractures
- 19,464 atypical femur fractures
- $2 billion annually, which translates to costs of $205,534 per hip fracture avoided.
In postmenopausal women at high risk of fractures, we recommend initial treatment with
bisphosphonates (alendronate, risedronate, zoledronic acid, and ibandronate) to reduce - Breakeven price point of annual bisphosphonate therapy would be $70
fracture risk.
- Conclusion: To optimize efficiency of treatment either patients may be selectively
treated, or the cost of annual bisphosphonate treatment should be reduced to cost-
effective margins.
23 24
47/7/2021
Conclusion:
• Osteoporosis - Big problem, poorly diagnosed and treated
• Hand Surgeons are at a valuable point of intervention
• Distal radius fracture over 50 meet should be screened
• How will your practice/system manage these patients?
25 26
57/26/2021
Disclosures
Beyond the FCR: • Acumed
Other Surgical Approaches to the • Consulting
Distal Radius •Axogen
• Consulting/Research Support
Mihir J. Desai, MD • No support received for this presentation
Associate Professor of Orthopaedic Surgery
Vanderbilt University Medical Center
V A N D E R B I L T Orthopaedics V A N D E R B I L T Orthopaedics
1 2
V A N D E R B I L T Orthopaedics V A N D E R B I L T Orthopaedics
3 4
Now What?
V A N D E R B I L T Orthopaedics V A N D E R B I L T Orthopaedics
5 6
17/26/2021
How to treat? What’s the Best Technique?
• “Short” Answer: Depends on the
fracture
• Comes down to the surgeon’s:
• Training
• Comfort
• Experience
V A N D E R B I L T Orthopaedics V A N D E R B I L T Orthopaedics
7 8
• 100 patients
• Randomized to VLP or Fragment Specific Fixation
• Comminuted fractures
• Plate removed at 3 months (2nd
• At 12 months: Surgery)
• No difference in grip strength, ROM, DASH
• 1 year follow-up
• 56% vs. 21% complications in Fragment Specific vs. VLP • Functional outcomes similar to
• CRPS, painful hardware, tendon injury historical data
• No infections, tendonitis, tendon
rupture
V A N D E R B I L T Orthopaedics V A N D E R B I L T Orthopaedics
9 10
What is the “Critical Corner”?
• Volar, ulnar lunate facet
• Emphasized by Melone in 1984
• Origin of SRL
V A N D E R B I L T Orthopaedics V A N D E R B I L T Orthopaedics
11 12
27/26/2021
Requirements for Good Reduction Approach
Approach Radiographs
• FCR • Good DRUJ view
• Between ulnar bundle and FDS/FDP • Supinate radius
• Dorsal
• Dorsal Plate
• Bridge Plate
• Combination
V A N D E R B I L T Orthopaedics V A N D E R B I L T Orthopaedics
13 14
V A N D E R B I L T Orthopaedics V A N D E R B I L T Orthopaedics
15 16
Dorsal Plating
• Dorsal metaphyseal comminution
• Dorsal shear
• Direct visualization of articular surface
Problems:
• Extensor tendon irritation
• Difficult to correct volar tilt
Yu et al. (2011)
• Newer lower profile dorsal plates
• Less tendon irritation
• Less neuropathic pain than volar plates
V A N D E R B I L T Orthopaedics V A N D E R B I L T Orthopaedics
17 18
37/26/2021
• Use standard dorsal approach Dorsal
• Between 3 and 4 ext compt.
V A N D E R B I L T Orthopaedics V A N D E R B I L T Orthopaedics
19 20
Indications for Bridge Plating
• Severely Comminuted Fractures
• Distal fractures
• Radiocarpal dislocations
• “Position hand on wrist”
• Still unstable despite fixation
• Plate removal at 3-4 months
V A N D E R B I L T Orthopaedics V A N D E R B I L T Orthopaedics
21 22
Bridge-Plating Technique
V A N D E R B I L T Orthopaedics V A N D E R B I L T Orthopaedics
23 24
47/26/2021
V A N D E R B I L T Orthopaedics V A N D E R B I L T Orthopaedics
25 26
6 weeks after plate removal
Choice of Approach
•Fracture Characteristics
•Surgeon Preference
V A N D E R B I L T Orthopaedics V A N D E R B I L T Orthopaedics
27 28
Thank You
• Mihirjdesai@vumc.org
V A N D E R B I L T Orthopaedics
29
5Marc J. Richard, M.D.
ASSH ICL#39-R
New Perspectives on Distal Radius Fractures: Tips and Tricks to Improve Care
Tips and Tricks for Challenging Fracture Patterns
I. Instruments to broaden the armamentarium
- Lobster claw (serrated bone holding clamp)
- Large pointed tenaculum
- 16g needle
- Lamina spreader
- Finger traps/traction
II. Patterns/Techniques
- Small lunate facet fragment
o Suture of long/short radiolunate ligament
o Hook plate
o K-wires
o Spanning plate
- Previous distal radius fracture
o Radial column plate
o Non-anatomic plate
o Spanning plate
- Persistent radial translation
o Release of brachioradialis
o Lamina spreader in interosseous space
- Delayed fixation
o Pronation of proximal shaft
o Dorsal periosteal release7/20/2021
Disclosures
• Physician Advisory Board
Distal Radius Fractures: – Auxillium
– Smith & Nephew
– BME
Managing Associated Injuries – Zimmer Biomet
R. Glenn Gaston, MD – Restor3D
– PBC Biomedical/Mochida
OrthoCarolina Hand Fellowship Director
• Hand Consultant
Atrium Health Chief of Hand Surgery – Carolina Panthers
– NASCAR
– Charlotte Hornets
1 2
Associated Injuries Median Nerve Dysfunction
• Contusion
• Median nerve • Associated fractures – Present at time of injury
– Neurapraxia – Nonprogressive
– Acute CTS • Ligamentous injury • Acute CTS
– CRPS – SL, LT – Tends to worsen with time
• Reduce fx and re-eval
• Document 2 pt discrimination
• DRUJ instability • Osteoporosis – 5.4% incidence, risk factor
– TFCC displacement >35% (Dyer JHS 2008)
– Ulnar styloid
• Pre-existing or subclinical worsened by
swelling/hematoma
3 4
Median Nerve Dysfunction Post-operative Median Nerve Dysfunction
• Failure to improve • CTS
– To OR for ORIF and CTR – Reported 10% s/p VLP
– Standard CTR +/- HW
– I prefer 2 incisions removal
• Dealers choice
– No benefit to “prophylactic”
CTR at time of ORIF
5 6
17/20/2021
Post-operative Median Nerve Dysfunction DRUJ Instability
• Principles: after DR ORIF
• CRPS after DR Fx – Always compare to opposite
– This is CTS until proven side intra-op
otherwise – Stable in one position?
• Inject CT
• Splint in that position
• CTR
– Grossly unstable: address
boney injuries
– Plus standard CRPS Rx • Radius
– Radial translation
– Sigmoid notch
• Ulnar styloid/neck fracture?
7 8
DRUJ Instability DRUJ Instability
Distal Radius Malalignment Distal Radius Malalignment
• Dorsal • Radial translation
sigmoid – Displaced ulnar styloid fx of
notch 2mm
– If DOB present then DRUJ
becomes lax
9 10
DRUJ Instability
Ulnar Head & Neck Fractures
with Ulnar Styloid Fracture
• Numerous options for • ORIF ulnar styloid
stabilization – K-wires
– K-wires – Tension band
– Tension band – Screw
– Cannulated screws – Hook plate
– Plates*
• Typically my preference for • Re-assess for stability
instabiltiy
– Consider open TFCC repair
11 12
27/20/2021
Ligamentous Injuries
DRUJ Instabiltiy
SLIL & LTIL
• No ulnar styloid fx or • SLIL injuries • LTIL
persistent instability – Reported up to 45% – Reported up to 15%
– Rule out interposed tissue – Most partial tears – Most partial tears
(ECU)
– Open TFCC repair
– Arthroscopic?
32 pts. No difference subjective, objective or xrays even with
Grade 3 (10 pts) Always get contralateral films
*No grade 4 patients before going to the OR
13 14
Ligamentous Injuries Ligamentous Injuries
SLIL & LTIL SLIL & LTIL
Positive Watson’s shift
after ORIF styloid
15 16
Other Associated Fractures
Scaphoid Fracture
Always Joint Above and Below
• I tend to fix both • Carpus
• Fix scaphoid first to avoid
• Hand
displacement • Elbow
• I prefer 2 incisions
• Gurbuz et al: 22/22 healed 45 WF,
49 WE, PRWE 5, all returned to
pre-injury actrivity (J Wrist Surg
2018)
17 18
37/20/2021
Other Associated Fractures A Few Random Ones…
• Evaluate possible associated injuries
– Some easily missed… • Post-operative loss of
supination
• Volar DRUJ capsule tight
– Often missed/forgotten
19 20
A Few Random Ones…
Thank You
Osteoporosis
• These pts 2-4x risk of 2nd future fragility fx
» Malini H et al. Calcif Tissue Int 1993
» Lauritzen JD et al. Osteoporosis Int 1993
» Cuddihy MT et al. Osteoporosis Int 1999
» Klotzenbuetcher CM J Bone Miner Res 2000
» Foote JE et al. J Hand Surg 2012
• 50% ↑ relative risk future hip fracture
» Owen RA et al. Clin Orthop 1982
» Johansson C et al. Maturitas 1996 Don’t miss things right in front of you!
• 5x more likely to have 2nd DR fx
» Robinson CM. JBJS 2002
21 22
4You can also read