The "Silver Tsunami" Are We Ready? - Melanie Thompson, MD Principal Investigator AIDS Research Consortium of Atlanta @drmt on Twitter - CECentral
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

The “Silver Tsunami”
Are We Ready?
Melanie Thompson, MD
Principal Investigator
AIDS Research Consortium of Atlanta
@drmt on Twitter
Financial Disclosures Dr Thompson's institution has received grants for research from CytoDyn, Cepheid, Frontier Biotechnologies, Gilead Sciences, GlaxoSmithKline, Merck & Co, and ViiV Healthcare. (Updated 04/1/21)
Learning Objectives By the end of this presentation, the learner will be able to: 1. Discuss 3 key challenges in the management of older people with HIV 2. Assess for frailty in older persons with HIV 3. Diagnose diabetes in a person with HIV
People with HIV are Living Longer!

CDC HIV Surveillance Report 2018 (updated 2020)

Aging is… “Being nibbled to death by goldfish” ‐ My father in law, Richard Morris
We’ve put more effort into helping
folks reach old age than into helping
them enjoy it.
– Frank Howard Clark
Considerations for Aging with HIV
• Multimorbidity
– Co‐morbidities including ASCVD, DM, frailty
– Mental health/substance use issues
– Organ demise: Hearing/vision loss, incontinence
• Polypharmacy
• Social isolation and loneliness
• Stigma
• Financial, housing, food insecurity; impact of social
determinants of health
What I’m Not Going to Talk About…
Multimorbidity is More Common in PWH
People With HIV People Without HIV
Cardiovascular
Diabetes mellitus
Chronic kidney ds
Neurologic
Osteoporosis
Malignancy
Depression
Schouten, CID, 2014People with HIV are Living Longer
But NOT Without Comorbidities
Marcus et al. JAMA Network Open. 2020 Jun (3)6Multimorbidity in PWH on ART in the US:
2030 Projections
• The PEARL Model: ProjEcting Age, multimoRbidity and
poLypharmacy
• NA‐ACCORD and CDC surveillance collaboration
• By 2030, 36% will have at least 2 comorbidities
– Differences by age
– Greatest increases among gay & bisexual men, esp Black/Hispanic;
Hispanic persons who inject drugs & heterosexual women
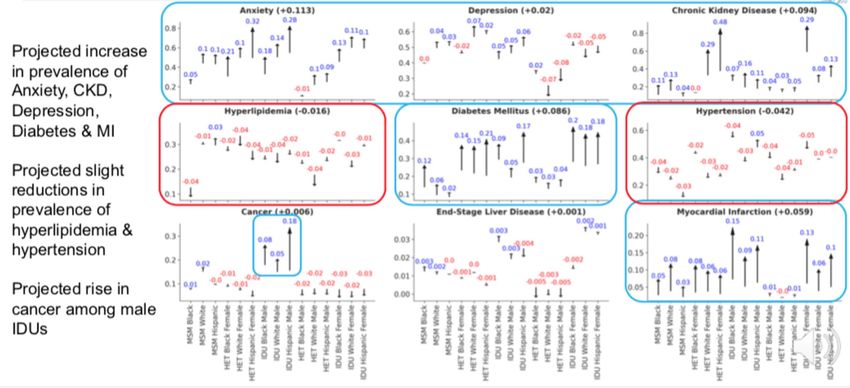
• Increases in anxiety, depression, CKD, DM, MI
• Limitation: excludes transgender & AAPI persons
Kasaie P et al. CROI 2021, Abstract 102.Projected Burden of Multimorbidity by Age, 2030
Kasaie P et al. CROI 2021, Abstract 102.Change in Prevalence of Comorbidities: 2020‐2030
Kasaie P et al. CROI 2021, Abstract 102.Rona • 69 yo African‐American woman who moved from Memphis and has not been to clinic since January 2020 “due to the pandemic.” • She is coming back to reestablish care. Last CD4 was 854/µL with HIV RNA < 50 c/mL. • She has taken her HIV meds “mostly” regularly, but has missed some other meds because of cost and access issues.
Rona • She has been observing coronavirus precautions, lives alone, is feeling increasingly isolated, and has not been vaccinated. • She is drinking more alcohol than usual, has started smoking again, and has gained 27 pounds. • She had one fall earlier this year, but had no injuries. • She has “no energy,” gets “no exercise,” and doesn’t sleep well.
Problem List Medication List HIV Elvitegravir/cobicistat/TAF/FTC Hypertension Losartan/hydrochlorothiazide, metoprolol Hyperlipidemia Rosuvastatin, ezetimibe Diabetes mellitus Metformin (by endocrinologist) Chronic kidney disease, stage 2 Lisinopril 5mg Gastroesophageal reflux OTC omeprazole BID (by GI doctor) Osteoarthritis (knees) OTC acetominophen, Goody’s Powder (at bedtime) Osteopenia OTC calcium, magnesium, vitamin D Seasonal allergic rhinitis OTC diphenhydramine, fluticasone Past deep vein thrombosis Apixiban (by hospitalist in 2019) Depression, anxiety Escitalopram, clonazepam (by psychiatrist) Insomnia Zolpidem, OTC melatonin
AND…
And…
Multivitamin with iron
Zinc (to prevent COVID)
Turmeric (for arthritis)
Apple cider vinegar (for BP)
Vitamin C – 4000 mg/day
Two supplements advertised on TV to “help
the brain”Issues Associated with Polypharmacy • Inappropriate drugs, doses • Drug interactions: DON’T GUESS – LOOK IT UP! • Additive toxicities: nephrotoxic drugs, etc. • Risk of forgetting doses • Risk of missing prescriptions/skipping refills due to cost • Expense • “Overwhelmed” feeling of just too many pills!
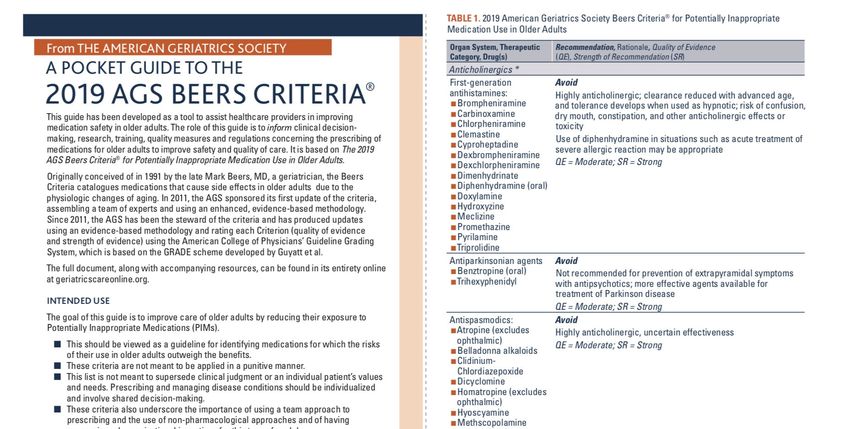
Resource: The Beers Criteria
• Potentially inappropriate medications for older adults
– Due to intrinsic effects
– Due to drug‐disease, drug‐syndrome interactions that may
exacerbate the disease or syndrome
– To be used with caution in older adults
• Medications that should be avoided or have their dosage
reduced with varying levels of kidney function in older
adults
• Potentially clinically important drug–drug interactions that
should be avoided in older adults
American Geriatric Society, 2019Pocket
Guide to
Beers
Criteria,
2019
http://files.hgsitebuilder.com/hostgator257222/file/ags_2019_beers_pocket_printable_rh.pdfResource:
STOPP and
START!
https://jamanetwork.com/journals/jamaintern
almedicine/fullarticle/227481Drug Interactions: Don’t Guess!
• Cobicistat, ritonavir: strong CYP3A4 inhibitors, but somewhat
different interactions (RTV also an inducer)
• PIs: darunavir, atazanavir: lots of interactions
• NNRTIs other than doravirine: CYP3A4 inducers; rilpivirine lowered
by PPIs
• INSTIs: Polyvalent cations decrease absorption: Ca, Mg, Fe, Zn, Al
especially when given together on empty stomach
– Bictegravir: CYP3A4, UGT1A1; dolutegravir: minor CYPA4, UGT1A1
• Rifampin/rifabutin (don’t use BIC; increase dose with DTG)
• Metformin increased by BIC and DTG
• Look it up: www.hiv‐druginteractions.orgDrug‐Drug Interactions by Class
ARV Absorption Metabolism
Incr Gastric pg‐P CYP CYP CYP UGT1A1
pH Substrate Inhibitor Inducer
INSTI Most Not RAL EVG/c EVG/c Substrate
b/PI* ATV YES YES YES Not COBI Mixed
NNRTI RPV YES EFV, ETR EFV, ETR, NVP
NRTI TAF, TDF ABC
*bPI = ATVr/c, DRVr/c
INSTIs only: Decreased concentrations with polyvalent cations: Ca, Mg, Fe, Zn, Al
Maraviroc: pg‐P & CYP substrate
Fostemsavir: Substrate of CYP inducers; inhibits OATP1B1/3 and BRCP
Adapted from DHHS ART Guidelines, Table 20Resource: Liverpool HIV Drug Interactions
www.hiv‐druginteractions.orgAnd back to Rona..
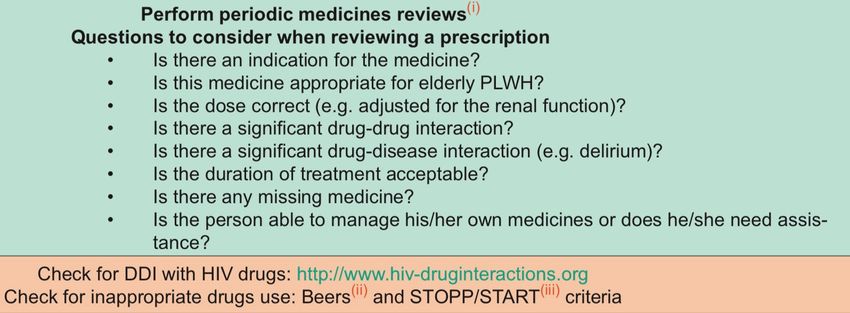
• Review meds: doses, schedule, prescribers
– OTC meds, & supplements; alcohol
• Look for inappropriate or risky meds, doses
– Clonazepam, zolpidem, diphenhydramine, alcohol increase risk of falls
– Apixaban no longer needed
– Supplements probably not needed
• Look for drug‐drug, drug‐supplement, drug‐disease interactions
– COBI increases metformin, rosuvastatin, fluticasone, apixiban, zolpidem,
clonazepam (BIC & DTG also increase metformin!)
– Polyvalent cations (Ca++ etc.) lower INSTI concentration when taken together
– Chronic PPI increases bone loss
– Goody’s powder = acetominophen + aspirin + caffeine: risk of bleeding,
gastritis, and insomnia (and too much acetominophen!)Medication List Changes/Strategy
Elvitegravir/cobicistat/TAF/FTC Change to BIC/TAF/FTC
Losartan/hydrochlorothiazide, metoprolol Monitor to adjust doses; lifestyle changes
Rosuvastatin, ezetimibe Monitor to adjust doses; lifestyle changes
Metformin (by endocrinologist) Monitor glucose to adjust dose
Lisinopril 5mg
OTC omeprazole BID (by GI doctor) H. pylori diagnosed & treated; address alcohol,
dietary interventions
OTC acetominophen, Goody’s Powder (at HS) Stop Goody’s Powder
OTC calcium, magnesium, vitamin D3 Proper spacing of Ca++, Mg++ re ART
OTC diphenhydramine, fluticasone Loratadine (less sedative), stop fluticasone
Apixiban (by hospitalist in 2019) D/C: no longer needed
Escitalopram, clonazepam (by psychiatrist) Wean clonazepam; social interaction/therapy?
Zolpidem, OTC melatonin Avoid zolpidem; exercise & sleep hygieneAND…
And…
Multivitamin with iron
Zinc (to prevent COVID)
Turmeric (for arthritis)
Apple cider vinegar (for BP)
Vitamin C – 4000 mg/day
Two supplements advertised on TV to “help
the brain”Also Remember… • General health assessments and screenings • Cancer screening: breast, colon, lung, cervical, anal, prostate • Vaccines! (SARS CoV‐2, flu, pneumonia, HAV, HBV, HPV) – Check CDC ACIP recommendations • Special attention to social isolation, mental health, substance use • Assess ability to participate in telehealth?
• Recognizes increased ASCVD risk in persons with
HIV
– 1.5‐2x increase in MI, stroke, heart failure
– Increased pulmonary HTN, blood clots, sudden death
• Addresses pathophysiology, screening, treatment
• Includes link to patient perspective from PLWH
Feinstein, Circulation, 2019Contribution
to MI Risk in CKD, Stage 4
PWH CD4 < 200/µL
(NA‐ACCORD) HIV‐RNA > 400c/mL HCV
When obesity
included:
DM significant Elev
HIV‐RNA not Smoke? Tot HTN
significant Chol
Althoff, Lancet HIV, 2020ASCVD Risk
Assessment and
Treatment
Two approaches
• High risk
• Low‐moderate risk
Feinstein, Circulation, 2019High Risk Approach
• Known clinical ASCVD, or
• LDLc ≥ 190 mg/dL (untx), and/or
• Age 40‐75 with diabetes
mellitus
OR
• Calculated high ASCVD risk by
risk calculator tools
• Presence of HIV‐related or 2018
ACC/AHA “risk enhancers”
Feinstein, Circulation, 2019If YES: Consider adjusting risk upward; may be 1.5‐2x higher
Feinstein, Circulation, 2019But also… • Control risk factors other than lipids – Smoking, smoking, smoking! – Diabetes mellitus – Hypertension – Obesity ‐ encourage exercise and diet: education! • Statin (without hyperlipidemia)? – Wait for REPRIEVE trial… • Consider role of mental health in being able to address general health issues: holistic approach needed
Oahunbade, et al, JAHA, March 23, 2021
Smoking and Cancer in PLWH
• Smoking: up to ¾ of PLWH
• Cancer burden attributable to
smoking
– Lung cancer: 94%
– Other ‘smoking related’ cancers
(esophageal, oral, etc.): 31%
– Anal cancer: 32%
– All cancer: 9%
Altekruse, AIDS, 2018Diabetes Mellitus: ADA Definition (2021)
• Hemoglobin A1C ≥ 6.5%
– "In conditions associated with an altered relationship between A1C
and glycemia, such as …HIV….only plasma blood glucose criteria
should be used to diagnose DM.” Likely only applies when on ART.
• Fasting plasma glucose ≥ 126 mg/dL, confirmed by repeat
• Plasma glucose ≥ 200 mg/dL 2 hrs after 75 g oral glucose
tolerance test
• Random plasma glucose ≥ 200 mg/dL with polyuria and
polydipsia
ADA. Diabetes Care 2021;44(Suppl. 1):S15–S33.A1C May Under‐ or Overestimate Glycemia Depending on ART
• A1C underestimated glycemia on NNRTIs, but overestimated on PIs
• Tenofovir (TDF) had no effect; INSTIs were not tested
• Unlike in MACS study, HIV itself did not affect A1C levels in this cohort
Eckhardt, et al. AIDS Patient Care & STDs, 2012Patel, Epidemiology of Sarcopenia and Frailty, 2016
Three Tools for Assessing Frailty • Fried’s Frailty Phenotype – 5 physical variables • Short Physical Performance Battery (SPPB) – 3 physical tasks • Frailty Index – 40 physical, psychological, social/functional variables
Fried’s Frailty Phenotype
Requires dynomometer
Fried, J of Gerontology, 2001Frailty Phenotype as a Predictor
Frailty phenotype
predicts
• Death
Fried, J of Gerontology, 2001Frailty Phenotype as a Predictor
Frailty phenotype
predicts
• Death
• Worsening
disability
• Incident fall
• 1st hospitalization
Frailty phenotype was more common in
women and African‐Americans
Fried, J of Gerontology, 2001Frailty: Short Physical Performance Battery
(SPPB)
3 physical tasks:
• Repeated chair
stands (sit then
stand 5 times)
• Balance tests
• 4‐meter (10‐foot)
walk test
geriatrictoolkit.missouri.edu/SPPB‐Score‐Tool.pdf; Greene, AIDS, 2014Frailty Index
• Relates deficit accumulation to risk of death
• 40 variables
– Physical: e.g. walk outside < 3d/wk; wt loss > 5 kg/yr
• Comorbid diseases, without regard to severity
– Psychological: feel depressed, happy, lonely, etc.
– Social/Functional: help bathing, dressing, eating, etc.
• Scored between 0‐1 = deficits/variables
– < 0.08 = robust; ≥ 0.25 = frail
Searle, BMC Geriatrics, 2008.CDC STEDI
https://www.cdc.gov/steadi/index.htmlFrailty is Dynamic!
Interventions to Prevent Frailty
• Exercise, strength and balance training
• Social interaction
• Healthy diet
• Preventative health care and screening
• Management of medications
• Smoking cessationScreening for HIV‐Associated Neurocognitive Disorders
Screening tools have variable sensitivity/specificity
• Mini‐mental state examination (MMSE)
• International HIV dementia scale (IHDS)
• Montreal cognitive assessment (MoCA)
• Simioni symptom questionnaire (SSQ)
• Cognitive assessment tool‐rapid version (CAT‐rapid)
Joska, AIDS Behavior, 2016Screening for HIV‐Associated Neurocognitive Disorders
Screening for HIV dementia
– IHDS + CAT‐rapid = most sensitive/specific
Screening for asymptomatic/mild HAND
– No screener had adequate sensitivity/specificity: need
full neuropsych testing
– MoCA often used in clinic
Don’t forget reversible causes … syphilis, thyroid
disease, B12 deficiency, depression
Joska, AIDS Behavior, 2016Screening for Mental Health and Substance Use Issues
• Depression and substance use are common; screening is
uncommon
• Easy screening tools available (and reimbursable!)
• Depression ‐ PHQ 2 and 9; Anxiety ‐ GAD‐2 and 7
– PHQ‐2: Over the last 2 weeks, how often have you been bothered by
the following: (score 0‐3)
• Little interest or pleasure in doing things
• Feeling down, depressed or hopeless
• Alcohol Use: CAGE and AUDIT
• Drug Use: TICS, opioid risk tool
National HIV Curriculum: https://www.hiv.uw.edu/page/mental‐health‐screening/phq‐2Tools for Screening
National HIV Curriculum
• https://www.hiv.uw.edu
https://www.hiv.uw.edu/page/mental‐health‐screening/phq‐2The Social Isolation Score (SIS)
Visits from close family
Visits from close friends
Number of close family/friends
Use of self‐help or support group in last year
Volunteer work or involvement in community organization
Frequency of attendance to religious events
Relationship status
Living alone
Greysen et al., Journal of American Geriatrics Society, 2013PLWH ≥ 65 yo
are 2‐7 times
more likely to
experience
social
isolation than
those who are
HIV ‐
Greysen et al., Journal of American Geriatrics Society, 2013Social Isolation Is Associated with Increased Mortality
Not Isolated
SIS < 4
Isolated
SIS ≥ 4
Greysen et al., Journal of American Geriatrics Society, 2013Stigma Kills! • HIV status • LGBTQ+ discrimination • Ageism • Substance use • Race/ethnicity
What Do
Guidelines
Say?
IAS‐USA 2020
JAMA. doi:10.1001/jama.2020.17025What Do Guidelines Say?
EACS 2020
• Manage polypharmacy
• Assess for and manage frailty: Frailty Phenotype (Fried) and Frailty Index
https://www.eacsociety.orgWhat Do Guidelines Say?
DHHS 2021 (from 12/2019)
• Section on “HIV and the Older Person”
• Attention to polypharmacy & multimorbidity
management
• Refer those with progressive neurocognitive
defects for neurologic assessment and
neuropsychiatric testing
• Drug‐drug interactions tables focused on ART
DHHS. Guidelines for the Use of Antiretroviral Agents in Adults & Adolescents Living with HIV
https://clinicalinfo.hiv.gov/en/guidelinesFINALLY! An Update!
Thompson M, et al. CID, 6NOV2020 ; also
www.hivma.org under “Guidelines”What Do Guidelines Say?
HIVMA/IDSA Nov. 2020
• Recommendations focused on preventing,
detecting & managing multimorbidity
• Section on metabolic & noncommunicable
comorbidities including drug interactions
• Neurocognitive assessment recommended
based on symptoms
Thompson M, et al. CID, 6NOV2020 ; also
www.hivma.org under “Guidelines”Patient
Centered Care
Coordination
for Older
PLWH
Slide: HealthHIVThank You!
• Colleagues whose research I have presented
• Research participants
• Guidelines panels
• People living with HIV who have had the
resilience to become the survivors who inspire
us today!You can also read