Hyaluronic Acid May Be a Predictive Biomarker for Thrombocytopenia and Liver Dysfunction After Oxaliplatin-based Chemotherapy
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
CANCER DIAGNOSIS & PROGNOSIS
2: 15-24 (2022) doi: 10.21873/cdp.10071
Hyaluronic Acid May Be a Predictive Biomarker
for Thrombocytopenia and Liver Dysfunction
After Oxaliplatin-based Chemotherapy
TAKASHI MIYATA, YASUTO TOMITA, YUTA SAN-NOMIYA, TAIGO NAGAYAMA,
RYOSUKE KIN, HISASHI NISHIKI, AKIFUMI HASHIMOTO, YORITAKA FUJII,
SEIKO MIURA, DAISUKE KAIDA, NAOHIKO NAKAMURA, TOMOHARU MIYASHITA,
HIDETO FUJITA, NOBUHIKO UEDA and HIROYUKI TAKAMURA
Department of General and Digestive Surgery, Kanazawa Medical University Hospital, Ishikawa, Japan
Abstract. Background/Aim: Following oxaliplatin-based treatment in stage III CRC (2). Oxaliplatin-based
chemotherapy, approximately half of all colorectal cancer chemotherapy is a key regimen for CRC, and oxaliplatin is
patients develop sinusoidal obstruction syndrome (SOS). SOS included in the capecitabine plus oxaliplatin (CapeOX)
can be monitored by measuring splenic volume; however, regimen (3). However, oxaliplatin may induce hepatic
obtaining this measurement is not a simple process. In this sinusoidal obstruction syndrome (SOS) (4).
study, we evaluated changes in hyaluronic acid (HA) Approximately 30% of patients with CRC develop
concentrations as a simpler marker of SOS. Patients and metachronous liver metastases, and hepatectomy is the only
Methods: We measured splenic volume and laboratory data, potentially curative treatment (5). Moreover, approximately half
including hyaluronic acid concentration, liver enzymes, and of patients treated with oxaliplatin develop SOS, which leads to
platelet counts, in 34 patients with colorectal cancer who significant postoperative adverse effects, especially after major
underwent radical resection and who received capecitabine liver resection (6-8). Early SOS assessment is necessary;
plus oxaliplatin (CapeOx) chemotherapy. Results: A strong however, an effective strategy remains to be determined.
correlation was identified between ≥30% increase in splenic Increasing splenic volume (SV) may predict the risk of
volume and significantly elevated HA concentrations. SOS (9); however, measuring SV is complicated. SOS may
Affected patients also had persistent thrombocytopenia and result from drug-induced injury to liver sinusoidal
liver dysfunction compared to patients without elevated HA endothelial cells (LSEC), and hyaluronic acid (HA), present
concentration. Conclusion: HA concentration may predict in LSEC, was a marker for SOS in a rat experimental
SOS in patients who receive CapeOx adjuvant chemotherapy. model (10). Therefore, we evaluated HA as a prognostic
marker for early SOS assessment. We measured HA before
Colorectal cancer (CRC) is the third most common cancer and after CapeOX adjuvant chemotherapy in patients with
and has the second highest cancer-related mortality rate (1); stage III CRC after curative surgical resection, and
postoperative adjuvant chemotherapy is the standard investigated the relationships and changes in treatment
progression between SV, platelets, and liver dysfunction, as
indicators of SOS.
This article is freely accessible online. Patients and Methods
Correspondence to: Takashi Miyata, MD, Department of General Patient selection. We identified 34 patients with stage III CRC in
and Digestive Surgery, Kanazawa Medical University Hospital, our hospital database who underwent radical resection between
Ishikawa, Japan. Tel: +81 762862211, Fax: +81 762864626, e-mail: January 2017 and June 2020, and who received CapeOX adjuvant
ryutami5383917@gmail.com chemotherapy. We excluded patients with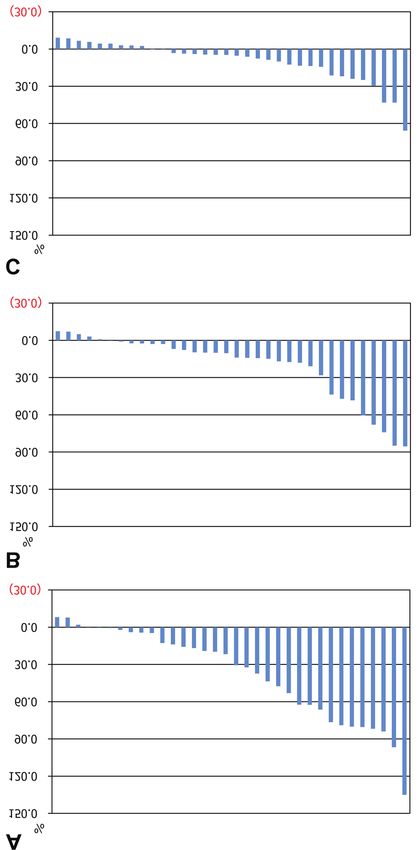
CANCER DIAGNOSIS & PROGNOSIS 2: 15-24 (2022)
Table I. Patient characteristics.
Characteristic Group A (n=17) Group B (n=17) p-Value
Median age (years) 64 65 0.890
Range 38-93 44-83
Gender (Male) 10 13 0.465
BMI 0.326
Median, kg/m2 22.9 22.0
Range 17.1-27.2 15.8-27.5
Primary colorectal cancer location 0.688
Right 3 5
Left 14 12
Surgery 1
Open 4 4
Laparoscopic 13 13
Postoperative complications 2 1 1
Pathology 0.162
tub 1, tub 2 14 14
pap 2 3
muc 1 0
Group A: Patients who experienced ≥30% increase in SV at time ii (immediately after completing oxaliplatin-based chemotherapy) compared with
time i (immediately before oxaliplatin-based chemotherapy). Group B: patients who did not experience ≥30% increase in SV at time ii compared
with time i. BMI: Body mass index; tub 1: well differentiated tubular adenocarcinoma; tub 2: moderately differentiated adenocarcinoma; pap:
papillary adenocarcinoma; muc: mucinous adenocarcinoma.
Clinical data. We retrospectively collected the patients’ sex, age, Results
body mass index, characteristics of the primary cancer and
surgical procedure, postoperative course, number of
Thirty-four patients were included; Group A (splenomegaly)
chemotherapy cycles, pathological factors, SV, and laboratory
data, namely hepatobiliary system enzymes, platelets, and HA comprised 17 patients, and Group B (no splenomegaly)
concentration. SV and laboratory data were measured four times: comprised 17 patients. There were no differences in the
i: before, ii: immediately after, iii: 6 months after, and iv: 1 year groups’ clinical characteristics (Table I).
after adjuvant CapeOX therapy. Changes in SV were determined Analyzing all patients, adjuvant CapeOX resulted in a
by comparing the value at each time point with the value before significant increase in HA at ii vs. i (pMiyata et al: Hyaluronic Acid as a Marker of SOS
Figure 1. Continued
17CANCER DIAGNOSIS & PROGNOSIS 2: 15-24 (2022)
Figure 1. Continued
1819
Miyata et al: Hyaluronic Acid as a Marker of SOS
Figure 1. Changes in laboratory data. (A) Changes in laboratory data for all patients. (B) Patients in whom splenic volume (SV) increased ≥30% after adjuvant chemotherapy compared with
before treatment. (C) Patients in whom SV did not increase by ≥30%. HA: Hyaluronic acid, PLT: platelet count, AST: serum aspartate aminotransferase, ALT: alanine aminotransferase, γ-
GT: γ-glutamyl transpeptidase.CANCER DIAGNOSIS & PROGNOSIS 2: 15-24 (2022)
significantly at ii (p=0.008), and improved at iii and iv. AST
levels increased significantly (p=0.004) at ii compared with
i; however, values improved, and did not change significantly
at iii (Figure 1C). Mean SV did not increase at any time after
chemotherapy, compared to i (Table II). Thrombocytopenia
(cut-off:Miyata et al: Hyaluronic Acid as a Marker of SOS
Figure 3. Magnitude of the percentage change in splenic volume in relation to the magnitude of the percentage change in HA levels after adjuvant
chemotherapy.
Table II. Change in SV in each group.
Patients SV data Time
i ii iii iv
All patients SV mean (ml) 147.2 202.6 181.0 166.3
Mean SV ratio compared with time i (%) --- 137.3 121.0 110.1
Group A SV mean (ml) 160.8 262.0 223.4 198.6
Mean SV ratio compared with time i (%) --- 163.4 136.5 119.4
Group B SV mean (ml) 138.3 147.4 144.1 139.7
Mean SV ratio compared with time i (%) --- 107.0 104.1 100.5
Time i: before; ii: immediately after; iii: 6 months after; iv: 1 year after adjuvant CapeOX therapy; SV: splenic volume.
We found a strong correlation between patients with and a persistent increase in HA compared to patients without
significantly elevated HA and those with a ≥30% increase in increased HA during and after chemotherapy. There is a strong
SV after CapeOX. In these patients, there was also marked correlation between splenomegaly and thrombocytopenia or
and persistent thrombocytopenia, persistent liver dysfunction, increased liver function caused by SOS in patients receiving
21CANCER DIAGNOSIS & PROGNOSIS 2: 15-24 (2022)
Figure 4. The hyaluronic acid (HA) cutoff value was 183 ng/ml, calculated using a receiver operating characteristic curve in a predictive model
for sinusoidal obstruction syndrome, shown as the boundary between Groups A and B.
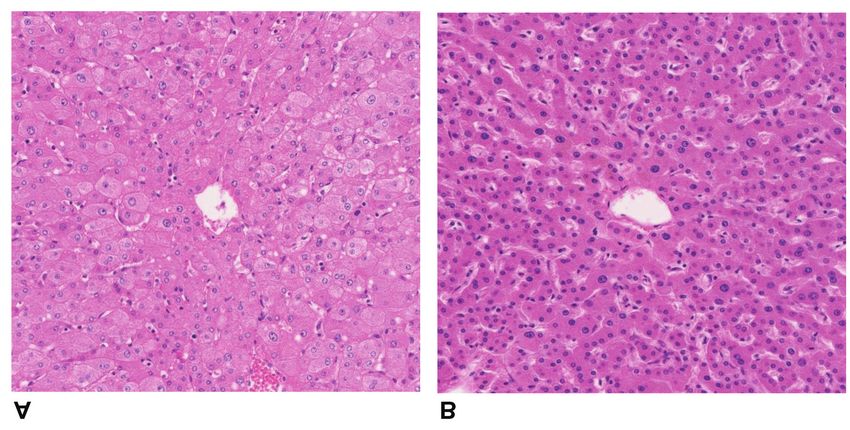
Figure 5. Liver histology showing atrophic hepatocytes with moderate sinusoidal injury and lymphocyte infiltration in a patient with an HA level
of 246 ng/ml (A). However, the liver tissue was almost normal in a patient with an HA level of 92 ng/ml (B) (magnification ×100, hematoxylin &
eosin (H&E) stain, for both images).
22Miyata et al: Hyaluronic Acid as a Marker of SOS
oxaliplatin-based-chemotherapy (4, 6, 8, 9); however, our 2 Sargent DJ, Wieand HS, Haller DG, Gray R, Benedetti JK, Buyse
results suggest that SOS evaluation is possible using HA M, Labianca R, Seitz JF, O'Callaghan CJ, Francini G, Grothey A,
instead of SV. Oxaliplatin-induced SOS may continue for O'Connell M, Catalano PJ, Blanke CD, Kerr D, Green E, Wolmark
N, Andre T, Goldberg RM and De Gramont A: Disease-free
more than a year after chemotherapy (9, 11), consistent with
survival versus overall survival as a primary end point for adjuvant
our results. colon cancer studies: individual patient data from 20,898 patients
The results of this study are important because they support on 18 randomized trials. J Clin Oncol 23(34): 8664-8670, 2005.
the hypothesis that systemic indicators of drug-induced injury PMID: 16260700. DOI: 10.1200/JCO.2005.01.6071
to LSEC may serve as simple biomarkers of SOS in CRC 3 André T, de Gramont A, Vernerey D, Chibaudel B, Bonnetain F,
patients receiving oxaliplatin-based chemotherapy. However, Tijeras-Raballand A, Scriva A, Hickish T, Tabernero J, Van
in order to prove the specificity of measured HA levels for Laethem JL, Banzi M, Maartense E, Shmueli E, Carlsson GU,
Scheithauer W, Papamichael D, Möehler M, Landolfi S, Demetter
oxaliplatin-induced injury of liver sinusoidal endothelial cells,
P, Colote S, Tournigand C, Louvet C, Duval A, Fléjou JF and de
further studies are required that take into account the tumor as Gramont A: Adjuvant fluorouracil, leucovorin, and oxaliplatin in
a source of systemic HA. stage II to III colon cancer: Updated 10-year survival and outcomes
As a limitation, we evaluated the records of only 34 patients according to BRAF mutation and mismatch repair status of the
who received CapeOX chemotherapy for stage III CRC. MOSAIC study. J Clin Oncol 33(35): 4176-4187, 2015. PMID:
Additionally, this was a retrospective and non-randomized 26527776. DOI: 10.1200/JCO.2015.63.4238
study. Third, because liver biopsy was not performed, we chose 4 Rubbia-Brandt L, Audard V, Sartoretti P, Roth AD, Brezault C,
Le Charpentier M, Dousset B, Morel P, Soubrane O, Chaussade
increased HA as a possible biomarker of SOS. The correlation
S, Mentha G and Terris B: Severe hepatic sinusoidal obstruction
between liver dysfunction induced by chemotherapy and the associated with oxaliplatin-based chemotherapy in patients with
development of SOS in pathological examination remains metastatic colorectal cancer. Ann Oncol 15(3): 460-466, 2004.
unclear. However, this study does not require CT examinations, PMID: 14998849. DOI: 10.1093/annonc/mdh095
which are necessary for measuring spleen volume, and can be 5 Manfredi S, Lepage C, Hatem C, Coatmeur O, Faivre J and
done only by collecting blood, so it has the advantage of being Bouvier AM: Epidemiology and management of liver metastases
easily tackled in future prospective studies. from colorectal cancer. Ann Surg 244(2): 254-259, 2006. PMID:
16858188. DOI: 10.1097/01.sla.0000217629.94941.cf
In conclusion, splenomegaly, prominent thrombocytopenia,
6 Nakano H, Oussoultzoglou E, Rosso E, Casnedi S, Chenard-Neu
and liver dysfunction were confirmed after oxaliplatin-based
MP, Dufour P, Bachellier P and Jaeck D: Sinusoidal injury
adjuvant chemotherapy, possibly owing to SOS. We believe increases morbidity after major hepatectomy in patients with
that increased HA after oxaliplatin-based chemotherapy is colorectal liver metastases receiving preoperative chemotherapy.
strongly associated with these outcomes and may predict SOS. Ann Surg 247(1): 118-124, 2008. PMID: 18156931. DOI:
10.1097/SLA.0b013e31815774de
Conflicts of Interest 7 Tamandl D, Klinger M, Eipeldauer S, Herberger B, Kaczirek K,
Gruenberger B and Gruenberger T: Sinusoidal obstruction
The Authors declare they have no financial or other conflicts of syndrome impairs long-term outcome of colorectal liver
interest. metastases treated with resection after neoadjuvant
chemotherapy. Ann Surg Oncol 18(2): 421-430, 2011. PMID:
Authors’ Contributions 20844968. DOI: 10.1245/s10434-010-1317-4
8 Nordlinger B, Sorbye H, Glimelius B, Poston GJ, Schlag PM,
Rougier P, Bechstein WO, Primrose JN, Walpole ET, Finch-
Takashi M and HT designed the study. TM, HT, YS, TN, RK, HN,
Jones M, Jaeck D, Mirza D, Parks RW, Collette L, Praet M,
AH, YF, SM, DK, YT, NN, TM, HF, and NU performed data
Bethe U, Van Cutsem E, Scheithauer W, Gruenberger T, EORTC
acquisition, analysis, and interpretation. Takashi M prepared the
Gastro-Intestinal Tract Cancer Group, Cancer Research UK,
manuscript. TM revised the paper critically. All Authors read and
Arbeitsgruppe Lebermetastasen und-tumoren in der
approved the final manuscript.
Chirurgischen Arbeitsgemeinschaft Onkologie (ALM-CAO),
Australasian Gastro-Intestinal Trials Group (AGITG) and
Acknowledgements Fédération Francophone de Cancérologie Digestive (FFCD):
Perioperative chemotherapy with FOLFOX4 and surgery versus
We thank Jane Charbonneau, DVM, from Edanz (https://jp.edanz. surgery alone for resectable liver metastases from colorectal
com/ac) for editing a draft of this manuscript. cancer (EORTC Intergroup trial 40983): a randomised controlled
trial. Lancet 371(9617): 1007-1016, 2008. PMID: 18358928.
References DOI: 10.1016/S0140-6736(08)60455-9
9 Miyata T, Takamura H, Kin R, Nishiki H, Hashimoto A, Fujii Y,
1 Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA and Miura S, Fujita J, Kaida D, Tomita Y, Nakamura N, Fujita H,
Jemal A: Global cancer statistics 2018: GLOBOCAN estimates Kinami S, Ueda N and Kosaka T: Spleen volume as a predictive
of incidence and mortality worldwide for 36 cancers in 185 biomarker for thrombocytopenia and liver dysfunction after
countries. CA Cancer J Clin 68(6): 394-424, 2018. PMID: oxaliplatin-based chemotherapy. Anticancer Res 40(6): 3361-
30207593. DOI: 10.3322/caac.21492 3370, 2020. PMID: 32487632. DOI: 10.21873/anticanres.14319
23CANCER DIAGNOSIS & PROGNOSIS 2: 15-24 (2022)
10 Miyata T, Tajima H, Hirata M, Nakanuma SI, Makino I, Hayashi 14 Yao L, Yao ZM and Yu T: Influence of BOL on hyaluronic acid,
H, Oyama K, Miyashita T, Takamura H, Ninomiya I, Fushida S, laminin and hyperplasia in hepatofibrotic rats. World J
Iseki S, Harada SI, Wakayama T and Ohta T: Phosphodiesterase Gastroenterol 7(6): 872-875, 2001. PMID: 11854920. DOI:
III inhibitor attenuates rat sinusoidal obstruction syndrome 10.3748/wjg.v7.i6.872
through inhibition of platelet aggregation in Disse's space. J 15 Fried MW, Duncan A, Soroka S, Connaghan DG, Farrand A,
Gastroenterol Hepatol 33(4): 950-957, 2018. PMID: 28960464. Peter J, Strauss RM, Boyer TD and McDonald GB: Serum
DOI: 10.1111/jgh.14004 hyaluronic acid in patients with veno-occlusive disease
11 Iwai T, Yamada T, Koizumi M, Shinji S, Yokoyama Y, Takahashi following bone marrow transplantation. Bone Marrow
G, Takeda K, Hara K, Ohta K and Uchida E: Oxaliplatin- Transplant 27(6): 635-639, 2001. PMID: 11319594. DOI:
induced increase in splenic volume; irreversible change after 10.1038/sj.bmt.1702821
adjuvant FOLFOX. J Surg Oncol 116(7): 947-953, 2017. PMID:
28876454. DOI: 10.1002/jso.24756
12 DeLeve LD: Vascular liver disease and the liver sinusoidal
endothelial cell. In: Vascular Liver Disease. DeLeve LD, Garcia-
Tsao G (eds.). New York, Springer, pp 25-40, 2011.
13 Hirata M, Tajima H, Miyashita T, Miyata T, Nakanuma S,
Makino I, Hayashi H, Oyama K, Takamura H, Ninomiya I,
Fushida S, Nakata H, Iseki S, Harada S, Wakayama T and Ohta
T: Extravasated platelet aggregation in the livers of rats with
drug induced hepatic sinusoidal obstruction syndrome. Mol Med Received August 28, 2021
Rep 15(5): 3147-3152, 2017. PMID: 28358421. DOI: 10.3892/ Revised September 12, 2021
mmr.2017.6407 Accepted October 18, 2021
24You can also read