HSIB maternity programme year in review 2020/21 - Summary of highlights, themes and future work
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

WWW.HSIB.ORG.UK HSIB maternity programme year in review 2020/21 Summary of highlights, themes and future work Independent report by the Healthcare Safety Investigation Branch NI-003748 August 2021

Providing feedback and comment on
HSIB reports
At the Healthcare Safety Investigation Branch (HSIB) we welcome feedback on
our investigation reports. The best way to share your views and comments is to
email us at enquiries@hsib.org.uk or complete our online feedback form at
www.hsib.org.uk/tell-us-what-you-think.
We aim to provide a response to all correspondence within five working days.
This document, or parts of it, can be copied without specific permission providing
that the source is duly acknowledged, the material is reproduced accurately, and
it is not used in a derogatory manner or in a misleading context.
© Healthcare Safety Investigation Branch copyright 2021.
2
About HSIB
We conduct independent investigations of patient safety concerns in NHS-
funded care across England. Most harm in healthcare results from problems
within the systems and processes that determine how care is delivered. Our
investigations identify the contributory factors that have led to harm or the
potential for harm to patients. The safety recommendations we make aim to
improve healthcare systems and processes, to reduce risk and improve safety.
We work closely with patients, families and healthcare staff affected by patient
safety incidents, and we never attribute blame or liability.
Considerations in light of coronavirus (COVID-19)
We have adapted some of our national and maternity investigations, reports and
processes to reflect the impact that COVID-19 has had on our organisation as well
as the healthcare system across England. For the period of this report, the way we
engaged with staff and families was revised.
About this report
This report provides a review of the HSIB maternity investigation programme
during 2020/21, including an overview of activity during this period, themes
arising from investigations and plans for the future. It is intended for healthcare
organisations, policymakers and the public to understand the work we have
undertaken. For readers less familiar with medical and healthcare terms relating to
maternity care, a glossary is included at the end of the review.
3
Our investigations
Our investigators and analysts have diverse experience of healthcare and other
safety-critical industries and are trained in human factors and safety science.
We consult widely in England and internationally to ensure that our work is
informed by appropriate clinical and other relevant expertise.
We undertake patient safety investigations through two programmes:
National investigations
Concerns about patient safety in any area of NHS-funded healthcare in
England can be referred to us by any person, group or organisation. We
review these concerns against our investigation criteria to decide whether to
conduct a national investigation. National investigation reports are published
on our website and include safety recommendations for specific organisations.
These organisations are requested to respond to our safety recommendations
within 90 days, and we publish their responses on our website.
Maternity investigations
We investigate incidents in NHS maternity services that meet criteria set out
within one of the following national maternity healthcare programmes:
• Royal College of Obstetricians and Gynaecologists’ ‘Each Baby Counts’ report
• MBRRACE-UK ‘Saving Lives, Improving Mothers’ Care’ report.
Incidents are referred to us by the NHS trust where the incident took place, and,
where an incident meets the criteria, our investigation replaces the trust’s own
local investigation. Our investigation report is shared with the family and trust,
and the trust is responsible for carrying out any safety recommendations made in
the report.
In addition, we identify and examine recurring themes that arise from trust-level
investigations in order to make safety recommendations to local and national
organisations for system-level improvements in maternity services.
For full information on our national and maternity investigations please visit
our website.
4Contents
1 Introduction 6
2 Highlights 8
3 HSIB strategic goals and objectives 10
4 Operational performance 12
5 Staffing and recruitment 19
6 Outcomes and impacts: emerging themes
from HSIB maternity investigations 21
7 Impact on trust learning and safety actions
for maternity services 31
8 Family and staff engagement 34
9 How the HSIB maternity investigation
programme is influencing national learning 40
10 Planned developments for 2021/22 44
11 Conclusion 47
12 Glossary 48
51 Introduction This report provides an overview of the operational performance, outcomes and achievements of the HSIB maternity investigation programme for the financial year April 2020 to March 2021. It also identifies themes in line with the requirement of our maternity Directions (secondary legislation that came into effect in 2018 that sets out our maternity investigation functions and responsibilities) and a high-level look at what we will focus on and hope to achieve during 2021/22. Since April 2018, HSIB has conducted safety investigations in NHS maternity services in England into occurrences of stillbirths, neonatal deaths or suspected brain injuries that meet the criteria of the Royal College of Obstetricians and Gynaecologists (RCOG) Each Baby Counts programme. In addition, HSIB also conducts safety investigations into the death of any woman while pregnant or within 42 days of the end of her pregnancy, from any cause related to or aggravated by the pregnancy or its management, but not from accidental or incidental causes and excluding suicides. By April 2019, the HSIB maternity programme was fully established in all 130 NHS trusts and 11 ambulance services delivering and supporting maternity services in England. The final RCOG Each Baby Counts programme report was published in March 2021 reflecting the important work RCOG has undertaken during the last five years. This work continues within the Each Baby Counts + Learn and Support programme, which is a collaboration between the RCOG and the Royal College of Midwives. This programme is currently supporting trusts to develop, test and evaluate new approaches to promote a more positive and supportive workplace environment. HSIB’s maternity investigation approach The maternity investigation programme draws on HSIB’s investigatory expertise to deliver a standardised, learning-orientated, and person-centred approach to safety investigations that produce insight to help reduce maternity safety incidents across the NHS. HSIB maternity investigations: • identify the factors that may have contributed towards death or injury • use the perception of events from families and staff to establish what happened and why Click here for contents page 6
• make safety recommendations to improve maternity care both locally and nationally
• identify safety themes of national significance to allow learning and
implement change.
HSIB’s investigations replace local trust incident investigations. Trusts are
encouraged to complete an initial review (historically referred to as a review
completed within 72-hours of the incident) to identify and act on any immediate
safety concerns. Confidentiality of all staff and families is protected in line
with our ‘just culture’ approach, which strives to supports a culture of fairness,
openness and learning in which people feel confident to speak up when things
go wrong, rather than fearing blame.
72 Highlights • The HSIB maternity investigation programme commenced 760 investigations during 2020/21. At the end of March 2021 fewer than 5% of our investigations had exceeded the designated 6-month timescale. • Where investigations exceed this timeframe, we have a detailed understanding of the reasons why and work closely with trusts and families to support their completion. • When the COVID-19 pandemic was declared in March 2020, HSIB’s maternity programme had almost completed one year of full operation. In line with NHS-wide efforts to reduce pressures on trusts, HSIB, in agreement with the Department of Health and Social Care, made amendments to the maternity programme criteria. • Families are central to our work. Without good, effective family engagement, we would be unable to hear a family’s story, reflect their voice and answer their questions. All families are invited to be part of their investigation and to date 87% have consented. • Families have described how HSIB investigations have helped them to fully understand the circumstances of their case; to trust that the knowledge generated is fair, transparent, and independent; and to feel reassured that they have been an important part of the investigation. • Non-English-speaking families have benefited from HSIB’s inclusive approach – we have produced our information resources in 25 languages other than English, used interpreters and translated 57 investigation reports into the family’s preferred language. We produce reports in other formats, such as audible, at a family’s request. • HSIB has adjusted the way we engage with families because of the pandemic. If appropriate and where technology allows, we will undertake trust, staff and family interviews remotely by phone or video rather than face-to-face visits. Where families feel unable to discuss their investigation or review a report using this approach a detailed risk assessment is completed to support a face-to-face meeting. • Trusts tell us that HSIB investigations and recommendations are positively influencing safer maternity care. We support trusts to take ownership of the recommendations from our reports and instigate responsive changes. The regular information we produce for trusts about our maternity investigations has helped to improve the flow of patient safety communication across perinatal teams. Click here for contents page 8
• The benefits of the HSIB maternity programme extend beyond learning and change for safer NHS maternity care. Improvements to NHS safety culture are being supported through HSIB’s family engagement model. Our learning focus in safety investigations enables staff to speak freely about their experiences. Our approach provides a unique insight into the relationship between engaged leadership and a positive safety culture. • HSIB works in collaboration with NHS England and NHS Improvement’s Maternity Transformation Programme to support the national maternity safety ambition to reduce the rate of stillbirths, neonatal and maternal deaths and brain injuries that occur during or soon after birth by 50% by 2025. • HSIB has been running a continuous survey of NHS staff who have been interviewed for maternity investigations, to drive improvement in the programme. The figures for April 2020 to March 2021 demonstrate that 86.8% of staff who responded strongly agree that HSIB investigations will help to improve the safety of maternity care at their trust. • In addition to the individual reports we have provided to families and trusts, during the last year we have published four national learning reports. We worked in collaboration with the wider HSIB investigation team to highlight areas for national investigation. Click here for contents page 9
3 HSIB strategic goals and objectives
Maternity investigation programme
HSIB Strategic Goal
contribution
1. Undertake independent safety We have commenced 760 maternity
investigations with objectivity investigations. At the end of March 2021
underpinned by competence fewer than 5% had exceeded the 6-month
credibility and integrity
timeframe for completion. The completed
investigations have provided families
with a full account of what happened,
and informed them of where we have
made safety recommendations to trusts.
All families are invited to be part of
their investigation and to date 87% have
consented. We receive positive feedback
from staff involved in our investigations.
2. Value and prioritise All HSIB maternity investigators undergo
professional development a comprehensive training programme
for staffing that includes upon joining the organisation. HSIB offers
internationally renowned safety
maternity programme staff ongoing
investigation techniques and
cutting-edge technology training and professional development
from national experts in human factors,
safety science and relevant clinical
specialities for maternity services. In
2020/21 we trained 22 new maternity
investigators to join our existing team.
The teams work closely with trusts and
our approach is influencing investigations
outside the HSIB criteria.
3. Provide learning to the wider The maternity programme has published
healthcare community and four maternity-themed reports in
promote professional safety 2020/21 and supported several national
investigations by improving
investigations, some of which are now
investigation skills and
techniques throughout the NHS complete and some ongoing. HSIB has
piloted a regional newsletter in the London
region with planned roll-out across England
in 2021/22. We contribute to learning
with local maternity systems and clinical
networks. In addition, our learning is shared
with NHS England and NHS Improvement
as part of the perinatal quality surveillance
model. HSIB’s investigations, reports
and family engagement approach are
influencing the way trusts approach their
local investigations
Click here for contents page 10Maternity investigation programme
HSIB Strategic Goal
contribution
4. Be financially sustainable, well The maternity programme remained within
governed and legally constituted budget and has optimised innovative ways
to support our independence of working to support families, trusts and
the wider maternity system. Governance
structures have been strengthened through
the development of the investigation
directorate. The maternity programme
has implemented a quality improvement
process to support further developments in
our work.
5. Support and uphold HSIB maternity investigations provide
equality across all our work information in multiple languages and
areas ensuring equitable and formats to support families to be a
fair treatment, access and
central part of all the work we undertake.
opportunities
Our family engagement model ensures
our teams are supported in all aspects
of communication with families. Our
investigators represent HSIB as equality
and diversity champions and Freedom
to Speak Up Guardians. Equality and
diversity is integral to our approach to
recruiting our teams.
Click here for contents page 114 Operational performance Maternity care in England is provided and supported by 125 acute trusts (reduced from 130 due to trust mergers) and 11 ambulance services. These are covered by 14 HSIB regional maternity investigation teams. The trusts refer maternity incidents (‘cases’) which appear to meet the HSIB referral criteria. Once a referral is received, an HSIB investigation team from the relevant region contacts the trust within 24-hours. This is to ensure the case meets HSIB’s criteria for investigation and to obtain the family’s contact details with their agreement. HSIB cannot commence an investigation without family consent to access the mother’s and baby’s healthcare records. We aim to initially contact families within five working days of the referral and provide them with detailed information about an HSIB investigation. This ensures they can make an informed decision when consenting for us to access medical records. The investigation team then scopes the case, working with the family and trust to establish the investigation’s terms of reference. Once the investigation has commenced, the team ensures that the family and the trust remain updated throughout. This enables the family and trust to be made aware of any delays. Ongoing communication with trusts during investigations ensures that any early learning is rapidly shared to support safer care. Impact of the COVID-19 pandemic When the COVID-19 pandemic was declared in March 2020, HSIB’s maternity programme had almost completed one year of full operation. In line with NHS- wide efforts to reduce pressure on trusts, HSIB (with the agreement of the Department of Health and Social Care) made amendments to the maternity investigation programme criteria. Under the amended criteria, trusts would continue to refer all cases in line with the existing criteria, and HSIB would temporarily cease investigations of cases relating to babies who had received cooling therapy where there was no apparent neurological injury (brain damage). In these cases, if a family or trust reported concerns about care, the case would be individually reviewed, and an investigation progressed where appropriate. Adjusting the criteria in this way reduced the overall investigation caseload by 15% during 2020/21. This also enabled HSIB to release some clinical staff to frontline duties in support of the response to the pandemic. In addition, HSIB worked collaboratively with NHS Resolution to reduce the burden of reporting for trusts by becoming the main reporting portal for HSIB and NHS Resolution Early Notification scheme cases. Click here for contents page 12
Involving families
Families remain central to our work. The time HSIB investigators take to develop
relationships and provide support is reflected in the positive feedback we receive
from families about their experience of an HSIB investigation. Without these
relationships we would be unable to hear a family’s story, reflect their voice and
answer the questions they ask of us. An HSIB maternity investigation cannot
proceed without a mother or family’s consent to be contacted and allow us
access to their healthcare records. In 2020/21, all families were invited to be part
of their investigation and 87% consented.
HSIB is doing further work to understand the reasons behind families not wishing
to be contacted by HSIB or progress an investigation. Table 1 demonstrates
improvements in consent following HSIB contact. This ongoing work has
identified themes relating to language, culture and faith, literacy, and age. Further
ongoing work is being undertaken in 2021/22.
Table 1 Improvements in gaining family participation in investigations
Families agreeing
Families not to be contacted Families
agreeing to be by HSIB but participating
Date range
contacted by not agreeing to in an
HSIB participate in an investigation
investigation
Quarter 1 2020/21 7.7% 8.1% 84.2%
Quarter 2 2020/21 7.3% 10.5% 82.2%
Quarter 3 2020/21 7.4% 7.5% 85.1%
Quarter 4 2020/21 7.9% 3.0% 89.2%
Because of the pandemic we have adjusted the way we engage with families. For
example, we have conducted staff and family interviews via telephone and video
conferencing, something we hadn’t done extensively before the pandemic. This
has enabled us to plan future working models to embrace a mix of IT solutions
and face-to-face interactions with trusts and families post COVID-19.
Click here for contents page 13Caseload statistics During 2020/21 the HSIB maternity investigation teams completed 1,024 reports, a number of these reports were part of the dedicated work undertaken to reduce the number of investigations exceeding the 6-month timeframe. HSIB received 1,269 maternity investigation referrals from trusts. Of these referrals: • 760 progressed to investigation • 509 were not progressed for the following reasons: - 170 were duplicate referrals from trusts - in 124 cases the family did not give consent to access healthcare records - 80 cases did not meet HSIB’s referral criteria - 135 were not progressed due to our COVID-19-related criteria adjustment. Except in the case of duplicate referrals, to ensure opportunities for learning were not lost, trusts would be expected to conduct a local investigation into cases that did not proceed to an HSIB investigation. Progress of referrals Of the 760 referrals that progressed to investigation, 381 investigations have been completed, meaning that the final report has been provided to the family and the trust. As at the end of March 2021, the remaining 379 ongoing cases were at varying stages of completion: • 268 were live investigations • 33 were undergoing internal quality assurance • 78 were with the trust or the family for a review of factual accuracy prior to completion • Over the course of the year we have reduced the number of active cases exceeding a six-month time frame from 283 (40 percent) to 15 cases (4 percent). Click here for contents page 14
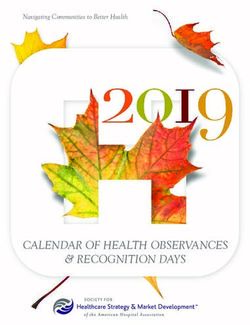
Categories of referrals
Referrals accepted for investigation across the four main criteria categories
for the maternity investigation programme are set out in figure 1.
Referrals not investigated due to our COVID-19 criteria adjustment are
shown, categorised as ‘COVID-19 rejections’. The diagrams show that in the
first two years of the programme, ‘cooled babies or babies diagnosed with
brain injuries’ was the largest category.
The change in HSIB criteria has led to a change in the proportion of cases
within each category. We also observed at the start of the pandemic an
increase in intrapartum stillbirth and maternal death referrals, with both
representing a greater proportion of referrals from April to July 2020
compared with previous years of the programme’s operation.
In February 2021 HSIB published a national investigation report which
highlighted the patient safety risks and contributory factors that emerged
from our review of maternal deaths during wave 1 of the pandemic.
Figure 1: categories of accepted referrals to HSIB’s maternity
investigations programme
1 April 2020 - 31 March 2021
Maternal deaths 66,
135, 7%
Early neononatal deaths 15% 101,
11%
Intrapartum stillbirths
Cooled babies or diagnosed
with brain injuries
COVID-19 rejected 147,
17%
446,
50%
Click here for contents page 15Investigation timescales
A key priority in the last year has been to resolve the number of investigations
exceeding the 6-month timescale for completion, as set out in the 2018 maternity
Directions. Investigation pathway development and close internal monitoring has
led to the reduction in the number of cases exceeding this timeframe. At the end
of March 2021 fewer than 5% of our live cases exceeded the 6-month timeframe.
Where cases have taken longer than 6 months to complete, this can be due to
investigations being unable to progress because of:
• A requirement for another agency to complete an initial review
• investigations needing additional clinical information from trusts and staff
• the requirement to investigate care provision by a number of different
healthcare providers.
In addition, some families require more time to feel ready to engage with the
investigation. It is important that HSIB respects and accommodates these requests.
The investigation team ensures that the family and the trust remain updated throughout.
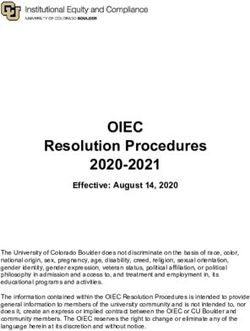
Figure 2: Progress of active cases against the six-month timescale
1 April 2020 - 31 March 2021
100 92 94
90 89 7 86
90 84 85 84
80 79 1 79
80 76
70 32
60 67 51 67 51 48 64
50 70 65 59
57 74
40 32
1
30 3 10
1
20
32
10 25 19 22 26 21 25 20 22 20
17 10
0
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Rejected (consent Active Completed Total referred (excludes
and COVID-19) rejected duplicates/standard
outside HSIB criteria
At the point of publication the number of reports that remain active over 6 months
has changed, this data is monitored and reported monthly to DHSC.
Click here for contents page 16Operational engagement with trusts and local maternity systems Ongoing communication with trust maternity service leaders is a key feature of HSIB’s investigations. Close collaboration with trusts is necessary for the HSIB maternity investigation programme to be effective, and its operational structure ensures that every trust has regular, productive engagement with their local team of HSIB staff. Each team includes a regional lead, team leader and a link investigator aligned to the trust. This is alongside the investigatory team. We share intelligence from our investigations with trusts through an ongoing programme of meetings and communications which are designed to facilitate a rapid response to safety concerns that require urgent attention. Awareness of emergent and recurring themes enables trusts to communicate effectively with frontline staff about risks and support their learning from HSIB’s work. We offer each trust a scheduled quarterly review meeting (QRM) with our HSIB team leader and link maternity investigator. We encourage the attendance of all clinicians involved in the provision of perinatal care, including obstetricians, midwives, neonatologists and obstetric anaesthetists (the perinatal team) to discuss the themes and possible actions being undertaken. We also encourage the attendance of staff from all levels of the trust, from the ‘ward to the board’. There may be external representation from the regional chief midwife or commissioners. At the QRM, the HSIB team presents referral data and reviews cases, identifying evolving and recurrent themes along with any evidence of safety improvement based on previous HSIB recommendations. This information remains with the trust for them to share with internal or external stakeholders including clinical commissioning groups (CCGs) and local maternity systems. We also share national themes to allow trusts to learn from incidents that have occurred in other trusts. HSIB receives positive feedback on this approach. HSIB is in a unique position to influence and observe the changes implemented by a trust due to the ongoing engagement our teams have at trust level. On occasion, including when there are serious safety concerns or when HSIB considers there to be insufficient urgency in a trust’s response to previously identified issues, senior HSIB maternity team members also attend the QRM meeting. A member of the trust executive team and the board-level maternity safety champion are encouraged to attend. Click here for contents page 17
A trust that is responding effectively to HSIB’s investigations will keep their HSIB team informed and updated on actions being taken to address recommendations. Similarly, trusts will be open with their CCGs and use HSIB reports to reinforce their prioritisation of safety actions. For example: A trust used the findings of an HSIB investigation to support a business case to acquire a piped (continuous) medical gas supply to neonatal resuscitaires, instead of reliance on oxygen cylinders. By addressing this issue, the trust reduced the future risk of interruption in the availability of medical gases during resuscitation, which had occurred and had impacted on a baby’s care. It is HSIB’s experience that most trusts welcome our reports and act promptly to respond to our recommendations. For various reasons some trusts have taken longer to recognise or prioritise the actions necessary to address risks. We understand the many pressures on trusts and that maternity services are a product of systems not all within the full control of individual organisations; sometimes solutions do not appear easily achievable. In the event we are unable to resolve variation in opinion in relation to a safety recommendation we will ensure the trust board maternity safety champion is aware to support further discussion at executive board level. HSIB has a duty under the 2018 maternity Directions to ensure that identified patient safety risks are known to relevant parties, including escalation to relevant regulatory agencies when there is evidence that the risks may, for whatever reason, be persisting. On the rare occasions HSIB has done this, it has only taken place after detailed consideration and discussion with the trust. Click here for contents page 18
5 Staffing and recruitment Maternity investigators In November 2020, we welcomed 22 new maternity investigators. Our investigators come from both clinical and non-clinical investigatory backgrounds. This was the 11th group of maternity investigators to join the organisation, bringing the total maternity investigator workforce to 130 investigators across the 14 regional teams; this is equivalent to one investigator per trust. All maternity investigators receive a comprehensive 3-week induction and training programme. The training focuses on developing the skills required to work effectively as an HSIB healthcare safety investigator in NHS maternity services, drawing from the knowledge and experience of practitioners and academic staff. This includes the application of safety science and analysis tools to identify the systems and processes that impact on safe maternity care. Subjects delivered during the training programme include: • learning from investigations • human factors • the System Engineering Initiative for Patient Safety (SEIPS) (a model used in safety investigations) • culture • working with families • working with staff • organisational and safeguarding • interviewing • analysing evidence • understanding health providers’ responsibilities after an incident has happened. Click here for contents page 19
Clinical advisors
We recruited 12 additional clinical advisors to the maternity programme in
October 2020, specialising in obstetrics, neonatology, obstetric anaesthetics, and
intensive care.
The new clinical advisors completed a two-day induction programme prior to
joining their clinical and midwifery advisory colleagues. The clinical advisor team
supports the work of the programme by providing multidisciplinary clinical
input to inform the analysis undertaken by maternity investigators throughout
investigations.
The clinical advisors work for HSIB one or two days a week. Most maintain active
clinical practice in their speciality, working in hospitals across the NHS in England,
in addition to their work for HSIB.
206 Outcomes and impacts: emerging themes from HSIB maternity investigations HSIB has a unique insight into local maternity services which informs our work at local, regional and national level to support joined-up learning. Our investigations provide us with granular detail of the safety, risks and culture within individual maternity units, and the recurrent safety themes at trust level and across the country. We have made over 1,500 safety recommendations to trusts addressing a wide array of issues. The most frequently recurring themes, which will be explored in more detail, include: • effective escalation of safety concerns about mothers and babies • clinical oversight • clinical assessment and monitoring. In addition, our investigations have highlighted: • how the use of clinical guidelines influence the care provided • the impact of pathways of care crossing healthcare boundaries on the care provided to mothers and babies. Effective escalation of safety concerns about mothers and babies Our investigations have identified recurring recommendations relating to effective escalation. A lack of effective escalation can impact on the outcome for mothers and babies, for example: • when concerns about mothers and babies are not effectively communicated to more senior or more specialist clinicians • where the response to escalation does not influence a change in a mother’s or baby’s clinical condition. The themes identified in the recommendations included timeliness of escalation, the environment in which the care was being given, anticipation of events and communication within and outside of the clinical team. Click here for contents page 21
Our investigations explore the reasons behind these issues and particularly the human factors related to team working and communication. HSIB has observed that effective escalation can be supported by: • Mechanisms that enable early recognition and correct identification of a concern Early warning physiological scoring tools that are adapted for use with pregnant women should be used in any environment a mother attends, such as the emergency department. These tools are often only applied within maternity services. This means that thresholds for escalation may not be identified. Early warning physiological scoring tools should be supported with clear escalation pathways that enable maternity expertise to be supported by those with critical care skills. HSIB receives feedback on improvements trusts are undertaking. For example, one trust has implemented a requirement for mothers to be reviewed by a consultant obstetrician and anaesthetist, and physically examined, if their observations are outside the expected ranges or if their early warning scores for sepsis are above an agreed score. • Effective and timely communication between individuals and teams Sharing of accurate information with the right people at the right time is essential for effective escalation. This needs to ensure the key pieces of information about a mother’s or baby’s condition are communicated, to enable the clinician receiving the information to make an informed decision about next steps. Once a mother or baby has been assessed, detailed documentation and clear management plans need to be completed to support the clinicians caring for the mother or baby to provide ongoing care. These plans need to include when further escalation should be undertaken and to whom. HSIB investigations have highlighted the importance of continuity of care and oversight of mothers’ or babies’ care, particularly when multiple clinical specialities are involved. Examples of actions trusts have implemented include: • A trust with multiple hospital sites that introduced a series of meetings between key staff at all its sites (known as ‘safety huddles’). The introduction of cross-site safety huddles improved communication and raised awareness of workload and complexity of clinical issues, particularly out of hours. Click here for contents page 22
• The implementation of an operational co-ordinators role to oversee workforce and activity. This role builds resilience into services by enabling oversight of the current situation, and forward planning for future shifts. This supports recognition of potential safety concerns and supports escalation across the perinatal service. • A trust culture that supports individuals and teams to raise concerns when the initial actions and decisions in response to a mother’s or baby’s deteriorating clinical condition are ineffective Clinical oversight is essential to ensure escalation is actioned and effective. The culture of a trust and clinical environment should support staff at all levels to challenge decisions. This means that staff should be empowered to escalate concerns when decisions relating to care have not been effective. In scenarios where there is difference of clinical opinion, a second opinion should be sought to ensure the mother or baby remain central to ongoing decisions and a dynamic approach is taken to care planning. HSIB has observed the development of a communication tool in a trust for use in complex situations. The tool allows all members of the multidisciplinary team to challenge a situation where they feel that the safety of a mother or baby could be compromised. Another trust has been creating an environment that supports ‘psychological safety’ as part of multidisciplinary training, ensuring that all members of the team feel safe and empowered to speak up and share ideas, questions and concerns. Clinical oversight The care a mother and baby receive involves many members of staff who may be involved at particular stages during the pregnancy, labour, birth, and in the immediate postnatal care. Above we have highlighted where clinical oversight can impact on escalation; this section provides more detail on clinical oversight throughout a mother’s pregnancy pathway. Throughout a mother’s pregnancy, effective multi-professional working requires open channels of communication and effective documentation of care plans. Co-ordinating care prevents ‘silo working’ and ensures staff and mothers have a clear understanding of care plans. This is particularly important when mothers have complex care needs, or care is delivered across multiple healthcare providers. HSIB has observed situations where a mother or family has had to take responsibility for updating clinical teams. Click here for contents page 23
For a mother with complex care needs, the importance of allocating responsibility for her care to a named consultant is often underestimated. There is a need to ensure a robust delegated approach is in place to provide consultant-led care when a named individual is not available. Without this approach care can be fragmented, ineffective and impact on the overall outcome for the mother or baby. HSIB has observed that clinical oversight can be supported by: • Effective documentation and communication with mothers and clinical teams providing care Healthcare records should include detailed documentation and communication which are accessible to the mother and clinical teams providing care. Detailed clinical records should be accessible and provide information that identifies changes at any point within a mother’s care pathway. This is particularly important when a mother receives care outside of the trust where she has booked for her maternity care. In emergency situations clinicians need to be able to access clinical information to support the care they provide. This cannot rely on the mother or family being in a position to accurately provide the information. Changes to a mother’s care plan can occur at any point in her pregnancy; it is important that these changes are effectively communicated to ensure they can be supported by the environment in which the care is being provided and the clinical team. HSIB has highlighted the importance of accurate, timely and repeated risk assessment to enable clinical oversight and management of ongoing care. The interim report of the Ockenden review of maternity services at the Shrewsbury and Telford Hospital NHS Trust, published in 2020, identified risk assessment throughout pregnancy as an essential action with the recommendation that formal risk assessment should be undertaken at every antenatal contact. HSIB investigations have observed the importance of this extending throughout the intrapartum and postnatal care of a mother and baby. HSIB has examples of trusts that have reinforced intrapartum risk assessments in birth centre settings to include senior midwifery oversight. These risk assessments, undertaken by the midwifery team, include hourly reviews of partograms. This supports a ‘fresh eyes’ review of a mother’s progress in labour and her uterine contractions, and leads to a regular holistic review of a mother’s and baby’s wellbeing. Click here for contents page 24
• Robust communication of changes to care plans To fulfil the essential requirement of safe care and meet the expectation of a mother during pregnancy requires effective and detailed communication. This is particularly important when the pathway of care is changed. Mothers who may initially be assessed as being low risk of complications can move between a low-risk and high-risk pathway during their pregnancy. Mothers considered suitable for a low-risk antenatal care pathway may develop conditions that require them to move to an obstetric-consultant led pathway, either temporarily or for the duration of their maternity care. This may subsequently influence birth planning choices, and requires skilled conversations to ensure safety, expectations and experiences are all supported following robust risk assessment. HSIB is aware of a trust that has introduced detailed, face-to-face holistic reviews that are undertaken when changes in a mother’s condition are identified. Another example includes the categorisation of all operative births to enhance clinical oversight and ensure timely delivery of babies. • Robust systems that support a named consultant to have overall responsibility for a mother’s care The lack of a named consultant can result in decisions being made around one particular aspect of a mother’s or baby’s care without consideration of the impact on another aspect. Clinical oversight in complex clinical situations is important to maintain situation awareness. Mothers may have pre-existing conditions that require support from clinical specialities outside of maternity during pregnancy. This requires planning and co- ordination to ensure care and information does not conflict or become confusing for the mother. It is also important when the health and wellbeing of a mother or baby changes rapidly that there is oversight and co-ordination of urgent decisions. A named consultant should be responsible for the oversight of care for mothers with complex care requirements. The on-call consultant should be informed in emergency situations. HSIB knows of an example where a trust that has implemented robust care planning and clinical oversight for mothers whose preferred place or method of plan to birth falls outside of national guidance. Other examples include the implementation of joint reviews with different clinical specialities during a mother’s antenatal and intrapartum care; and the involvement of multidisciplinary team ‘huddles’ to co-ordinate emergency care of the mother and ensure a named point of contact is provided to the family. Click here for contents page 25
Clinical assessment and monitoring The clinical assessment of mothers and babies incorporates many factors which influence ongoing monitoring and can affect subsequent actions taken as part of their care. The initial monitoring of a mother’s observations, measurement of the baby’s growth, the interpretation of cardiotocograph (CTG) monitoring, or assessment of progress in labour are just a few examples. Each clinical assessment is an opportunity to re-evaluate a mother’s care pathway and consider whether it needs to change. Such a change could be a referral for an obstetric review in the antenatal period, request for a review of a progress in labour or a move from one birthing environment to another. Decisions that are not fully informed can adversely influence both the outcome and experience for families and staff involved. • Examples of situations where HSIB has observed the influence of clinical assessment The importance of symphysis-fundal height measurements along with accurate plotting on growth charts to enable escalation for growth scans and review. Symphysis-fundal height measurement is used to assess a baby’s growth during pregnancy. When plotted on a chart, the measurements provide a visual indication of growth and can identify changes that need additional action. It is important that there is recognition when a baby is not growing as expected and that this is escalated for appropriate action. Babies whose growth is below the 10th centile require additional ultrasound scans and senior clinical review. If a baby’s growth exceeds the 90th centile this can also have implications when planning the birth. Information about a baby’s growth and size informs the clinical teams to anticipate a need for additional support at birth, such as neonatal resuscitation, or for larger babies the increased risk of the baby becoming stuck (shoulder dystocia). HSIB made safety recommendations following several undetected small for gestational age (SGA) babies at one trust. As a result, the trust reviewed the accessibility of customised growth charts alongside the information and support provided to clinicians relating to detection of SGA babies. This trust has reported a marked improvement in its SGA detection rates as a result. Click here for contents page 26
• Triage services being available 24-hours a day with dedicated and appropriately skilled clinicians Triage services are often the recommended point of contact given to families if they have concerns in relation to the pregnancy, or if a mother has gone into labour. It is important that trusts have a dedicated triage service that is available 24-hours a day and staffed by skilled clinicians. The clinicians need to have access to the mother’s records to ensure they provide informed, individualised advice. Each contact needs to be recorded accurately, with a process to support identification of multiple contacts so these can be escalated. HSIB has identified variation across England in the triage service model and associated resource; this has resulted in several safety recommendations to trusts to review the services they provide. HSIB made a safety recommendation to a trust identifying that the triage unit was not always accessible. The trust has now reviewed its service and introduced a new triage system, ensuring that it is open 24/7 with dedicated skilled staff. • Recognition of labour At the start of labour, a mother’s or family member’s first contact with maternity care is often by telephone. This initial telephone assessment at the start of labour informs decisions about the timing of admission for intrapartum care and may influence the care pathway. HSIB has observed that the timing of a mother’s transition from latent to active labour may be difficult to recognise and affects when one-to-one intrapartum care starts. A structured approach to telephone triage has been recommended, and documentation and handover of care has also been found to affect this period of care. When a mother goes into labour, clinicians undertake an assessment to establish how the labour is progressing and to inform them of the wellbeing of mother and baby. The initial assessment is often carried out over the telephone to advise the mother whether she should attend the maternity unit or can safely remain at home. Clinicians need to ensure the advice they provide supports mothers to receive assessment and monitoring throughout their labour. This needs to be individualised for each mother and informed by risk assessments undertaken during antenatal care. Click here for contents page 27
HSIB has highlighted through safety recommendations the importance of accurate recognition when a mother transitions from latent phase to established labour. This supports the decisions made in relation to the environment in which mothers are cared for. Our investigations have identified mothers’ and babies’ need to be in an appropriate environment to ensure they are monitored and receive one-to-one care when in established labour. HSIB has recognised that on occasion trusts have been unable to transfer mothers to a labour ward due to availability of beds or because the baby was going to be born imminently. HSIB has observed a number of examples where trusts have developed the ability to move clinicians and equipment to a mother’s location to support safe care and birth of the baby. • Accurate application, recording and interpretation of monitoring for a mother and baby during labour Intrapartum care requires clinicians to undertake ongoing assessments of a mother’s and baby’s wellbeing to ensure labour is progressing as planned. One key element is the assessment of fetal wellbeing throughout a mother’s labour. For mothers confirmed as being at low risk of complications, intermittent auscultation (IA) is suitable. IA allows mothers with non-complex pregnancies to be monitored using a Pinard stethoscope or handheld Doppler. Clinicians need to be trained to undertake IA effectively and to follow guidance, ensuring deviations from expected ranges are identified. Any changes require action, escalation, and commencement of continuous cardiotocograph (CTG) monitoring to assess a baby’s wellbeing. The monitoring of a mother and baby during labour (CTG monitoring) is used for more complex pregnancies, labour, maternal choice, and for other factors. Interpretation is complex and requires training, support, multi-professional input and tools to support clinical interpretation. Following HSIB safety recommendations a trust has successfully won a bid for funding, enabling it to appoint a fetal monitoring midwife and set up a CTG working group. The Ockenden report, identified an essential action that required the appointment of a lead midwife and obstetrician to champion best practice in fetal monitoring. Use of guidance The use of national policy and guidance to support staff to provide care to mothers and babies is variable. There is a significant volume of national guidance available, and at times it can be unclear or conflicting. Click here for contents page 28
Our investigations have highlighted these issues and made safety recommendations accordingly. Our investigations often identify that local guidance does not reflect the national perspective, or local interpretation is different or unclear. Where a trust has multiple sites, the guidance may be different at each site, which can be confusing for staff. In addition, where a trust has implemented guidance without a co-ordinated approach, staff can find it challenging to follow. HSIB recognises that the effective and appropriate use of national policy and guidance to support staff to provide care to mothers and babies is variable. HSIB has contacted the National Institute for Health and Care Excellence (NICE) regarding updates to its induction of labour guidance, and has responded to maternity-related NICE guidance consultations to share feedback and learning from our investigations. Pathways of care crossing healthcare boundaries To support improvement in local maternity units, our investigations have tackled challenges that are presented by care pathways that cross multiple healthcare boundaries. This can be internally within trusts across clinical settings such as intensive care, haematology, radiology and oncology services, and operating theatres. It also includes local system partners such as GPs, ambulance trusts, and external services for social care, pregnancy termination, substance misuse, learning disabilities, mental health and police forces. HSIB investigations regularly involve care provided by road and air ambulance services, highlighting the importance and complexities of pre-hospital care. HSIB has supported a systematic approach to investigations and opportunities for learning to be shared within this specialism of care. HSIB has recognised opportunities to develop this further and will be developing a quarterly review meeting approach similar to those that take place in trusts, and is undertaking a webinar with ambulance services in June 2021. Historically trusts have only been able to investigate aspects of care they have provided. This has meant that multiple providers investigate the aspects relevant to their service. These investigations are often not joined together or shared, resulting in families not being able to fully understand what happened during their whole journey or having to contact individual providers to have their questions answered. Families have told us that this can result in them reliving their experience multiple times, often without fully understanding what has happened. HSIB investigations are able to look at the whole care pathway and independently understand the Click here for contents page 29
care provided at each stage by the relevant provider. This has enabled us to identify the opportunities in a mother’s or baby’s care where something different could have been done. For families, we explore all aspects of care, answer any questions they have and provide them with a detailed explanation of events. For staff, being involved in an investigation can enable them to recognise that they were unlikely to have been able to change the outcome in the situation they were presented with. An example is described below: A recent investigation highlighted safety risks associated with ineffective communication within and between trusts, for the identification and care of mothers with complex care needs. A mother with multiple risk factors was referred by one trust for further assessment by a specialist unit at a different trust. The assessment involved screening for two concerns: suspected placenta accreta spectrum (PAS – a condition where the placenta is firmly stuck to the uterus and can cause severe bleeding complications during birth) and potential complications with the baby. The assessment required separate appointments; the mother only attended for the checks relating to her baby. There was a misperception in and between the trusts that screening had also been undertaken for PAS with no problems identified, so the mother was referred back to the original trust for ongoing care. Following the birth of the baby, the mother experienced extensive bleeding caused by PAS which could not be stopped and resulted in her death. HSIB’s recommendations supported improved communication arrangements between the trusts, and the clarity of information provided to mothers about complex risks such as PAS. Click here for contents page 30
7 Impact on trust learning and safety actions for maternity services Trusts embraced the introduction of HSIB’s maternity investigation programme with differing levels of confidence. Most trusts are keen to work with us, although some required greater effort to build relationships that are open, engaged and encourage learning. After two years of full operation, we are confident that we have constructive, effective working relationships with all trusts and their staff. Visible engagement by senior leaders is a strong signal that a trust is willing to recognise the safety issues we have identified and respond to our safety recommendations. Trusts have supported HSIB to understand what ‘works well’ for both organisations and have actively shaped our approach to investigations. The regular information we produce for trusts about our maternity investigations has helped to improve the flow of patient safety communication across the perinatal teams (midwifes, obstetricians, obstetric anaesthesia, neonatologist and neonatal nurses). For example: • There is increasing representation at our quarterly review meetings from across the perinatal team and from the executive board. This is encouraging wider discussion around learning identified within our investigations. The benefits of the HSIB maternity programme extend beyond learning and implementation of change for safer NHS maternity care. Improvements to the safety culture within trusts are being supported by HSIB’s family engagement model. Our learning focus in safety investigations enables staff to speak freely about their experiences. This enables the unique insight our approach provides into the relationship between engaged leadership and a positive safety culture at trust level. We encourage trusts to meet with HSIB and the family on completion of an investigation. These tripartite (three way) meetings can be complex to arrange to ensure they provide a supportive environment to talk through the learning from the investigation and ongoing communication the trust may wish to undertake. For example, we have worked closely with a trust that in the past had limited communication with families during investigations. During our time working with the trust, we have seen a significant changes as it has adopted a proactive and collaborative approach for each family at the beginning and throughout Click here for contents page 31
the investigation. This has meant at the tripartite meeting on completion of the investigation we are confident that we can step back and leave the ongoing communication and care of the family with the trust. HSIB is influencing change at local and system levels A newsletter sharing changes that trusts have made in response to HSIB maternity investigations has been piloted in the London region, and we expect to roll this out to all regions in 2021/22. Below are some examples of local changes made in response to learning from HSIB maternity investigations. HSIB rapidly escalated concerns from an investigation about the pre-printed algorithm used by a trust’s maternity triage team to assist the home birth of a baby. The algorithm was not in line with national guidance and the discrepancies may have contributed to a delay in the baby’s birth. As a result of HSIB’s letter of concern to the trust, the breech birth algorithm was immediately withdrawn and replaced with one that aligned with national guidance. This action has ensured that mothers in a similar situation are given advice to reduce the risk of recurrence and of harm. A trust immediately relocated a resuscitaire from the maternity unit to the emergency department (and ordered a new resuscitaire to replace it), following an HSIB investigation which found that the lack of a readily available resuscitaire in the emergency department had delayed vital care for a baby born with no signs of life in an ambulance on the way to the hospital. This response ensures that in future, the required equipment will be available to enable safe and timely provision of emergency neonatal care. A trust had received repeated recommendations from six HSIB investigations relating to fetal monitoring, paying particular attention to intermittent auscultation and continuous fetal monitoring from the perspective of interpretation and escalation. The trust used the findings to establish a new fetal surveillance midwife post. The importance of this role is highlighted in both the ‘Saving Babies Lives’ care bundle’ (guidance published by NHS England to reduce the number of stillbirths) and the interim Ockenden report. Click here for contents page 32
You can also read