HRT Prescribing -Made Easy in COVID pandemic & Case discussions - Dr Manju Navani 28th April 2021
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
HRT Prescribing –Made Easy in COVID pandemic & Case discussions Dr Manju Navani 28th April 2021
Discussion • Why menopause matters ? • HRT consultations during COVID • Risk Assessment before prescribing HRT • Basic Principles of HRT Prescribing HORMONES ➢ Choosing the right HRT- Why Progestogen matters? ➢Body identical HRT – When & Why? ➢Local HRT preparations ➢Case Studies (including Metabolic Syndrome) Take Home messages , resources Q&A
Why Menopause matters ?? Menopause is a CV risk factor Consequences ➢CVD and Metabolic Syndrome 1. Diabetes Mellitus 2. Hyperlipidemia 3. Hypertension 4. Central obesity 5. Prothrombotic state ➢Osteoporosis ➢Anxiety and Depression ➢Dementia Life style intervention
HRT Management during COVID • www.mims.co.uk • www.pcwhf.co.uk • www.bms.org.uk
Tele-Consultation History – New Diagnosis of menopause – clinical > age 45 • Symptoms • Menstrual Hx –Changes in cycles , Heavy periods ? • Obstetric Hx / Gynaecological Hx – Hysterectomy , BSO , Endometriosis • Does she need contraception? • Life style factors- BP, BMI, Alcohol, exercise • Indications for Transdermal HRT – Migraines +/- aura , BMI>30 , HT , Thyroxine , VTE risks etc • Medical History – Personal/Family History - Why??
Why & What Risk Assessment? Personal & Family Hx 1. Migraines +/- aura 2. CVS & metabolic risk factors 3. Venous Thrombo-embolism ( VTE) 4. Cancer – Breast , Bowel , Uterine, Ovarian 5. Risk of osteoporosis, DEXA scan Mental Health Exclude other causes of symptoms ( FBC, TFT s if required) www.bms.org.uk www.menopausematters.co.uk www.womans-health-concern.org.uk Green Climacteric scale chart
Benefits outweigh risks 50-60 ( NICE Guidance) BENEFITS of HRT ➢ Symptom Control ➢ Prevention and Rx of Osteoporosis ( under 60) ➢ Cardio –protection (window of opportunity in first 10 yrs) ➢Prevents metabolic Syndrome ➢ May prevent Alzheimer's Disease (July 2020) ➢ Reduces risk of colorectal cancer Rahman A, Schelbaum E, Hoffman K et al. First published June 14, 2020 Neurology Danish Osteoporosis Prevention Study (DOPS study) :2012, 17B E2 + NETA in early post menopausal years Finnish Study: Hodis HN et al. Vascular effects of Early v late post menopausal Rx with E . New Eng J of Med 2016;374(13)1221-31 ELITE study, KEEPS trial www.bms.org.uk, NICE Clinical Guidance (2015) Menopause Diagnosis and Management

ibis.ikinopedia.com

Refer to iFamilial Breast Cancer - NICE Guideline (CG164) • One relative – Female 1st degree with breast ca
Other RISKS Venous thromboembolism ➢Risk is increased with oral HRT 1 ( RR = 2) ➢Transdermal HRT has no greater risk than baseline risk 2 ➢Risk depends on type of Progestogen : Micronised Progesterone (Utrogestan) have lower risk of VTE compared with synthetic progestins2 Stroke ➢Risk increases with focal migraine, uncontrolled HT – consider transdermal HRT ➢Risk increases slightly over age 60 with oral HRT Ovarian Cancer ➢1 /5000 per year 1. Canonico Hormone replacement therapy and risk of venous thromboembolism in postmenopausal women: systematic review and meta-analysis. BMJ 2008; 336 (ESTHER study) 2. Vinogradova Y et al. Use of hormone replacement therapy and risk of venous thromboembolism: nested case-control studies using the Qresearch and CPRM databases. BMJ 2019; 364:k4810 http://dx.doi.org/10.1136/bmj.k4810,
Prescribing HRT Basic Principles
Check LIST for HRT prescribing 1. Uterus present - Oestrogen and Progestogens 2. Dose of Estrogen in HRT should be assessed & tailored on individual patient circumstances (see following slides) 3. Type of Progestogen in HRT matters due to CVS/Metabolic/ VTE/Breast cancer risks in individual patients 4. Transdermal HRT –Indications? 5 Regime: Sequential or Continuous Combined HRT ?
17 ℬ Estradiol Oral : Tablets – 0.5 mg, 1mg , 2 mg Transdermal (2/week, 1/wk ) Advantages 25, 37.5 mcg , • Improves Insulin sensitivity 40 mcg , 50 mcg , >transdermal E2 75 mcg , 80 mcg, 100 mcg • Lipid friendly Gels Oestrogel ™ Sandrena™ gel Disadvantages Higher risk of VTE >transdermal E2/no HRT Spray ↑binding proteins : TBG, SHBG Lenzetto ™(Estradiol1.53 mg/spray) ↑Triglycerides Drug interactions : Liver enzyme inducers
Considerations for transdermal HRT (17-ℬ Estradiol) ❖Poor relief with oral HRT ❑Cardiovascular risk factors ❖Absorption problems ( Metabolic syndrome) BMI >30, Central Obesity ❖Migraines, +/-focal Hypertension Dyslipidaemia ❖Interacting medications Diabetes Thyroxine Hypertriglyceridemia Anti-epileptics ( liver enzyme inducers) ❑Hx of VTE, risk factors for VTE ❖Gall Bladder disease, gall stones (Transdermal is Thrombogenic neutral)
Estradiol Equivalent doses (Conversion /interchangeable formulation table) LOW (50-60 yrs) STANDARD (40-50 yrs) HIGH (
What is Lenzetto? Lenzetto® is a novel transdermal HRT spray, delivering metered doses of estradiol. Each spray or actuation delivers 90 µL of transdermal spray and consists of:1,2 Lenzetto2 1 spray 2 sprays 3 sprays 21 mcg 29 mcg 40 mcg Matrix Patch 2 25 mcg ug/d 37.5 mcg ug/d 50 mcg ug/d Each Lenzetto device costs £6.90 and contains 56 sprays 2 min to dry 1. Estradiol (1.53 mg) 2. Octisalate (permeation enhancing) 3. Ethanol X1- 3 2. Invisible, no residue /irritation like with patches HRT, hormone replacement therapy; mg, milligram; µL, microlitre 1. Morton TL, et al. J Clin Pharmacol. 2009;49(9):1037–1046. 2. Lenzetto summary of product characteristics. 2018. Available from: https://www.medicines.org.uk/emc/product/11175. Accessed June 2020. 2 Kovács G, et al. Climacteric. 2016;19(5):488–495.
Progestogens in HRT 1. PROGESTERONES - Retroprogesterone: Dydrogesterone - Micronised Progesterone : Utrogestan 2. PROGESTINS (Androgenic) Norethisterone (NET) Medroxyprogesterone acetate (Provera™) 3. Mirena™: Levonorgestrel (52mg)
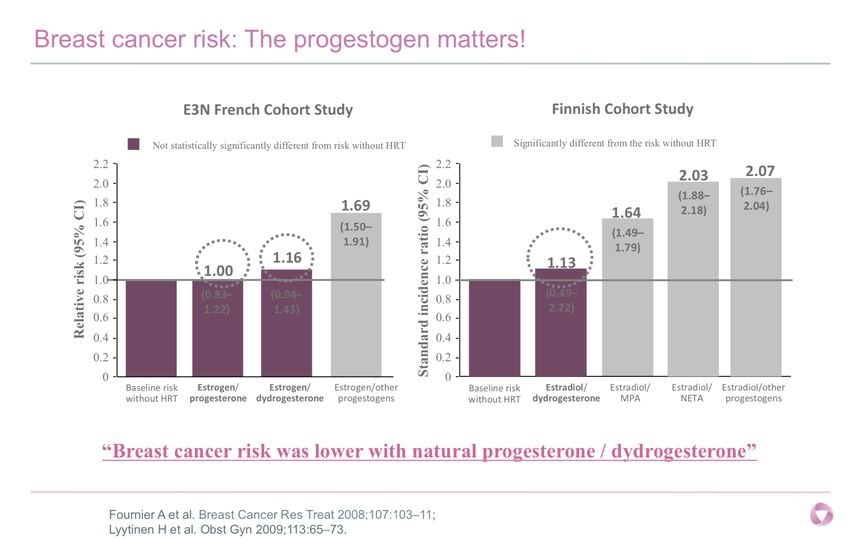
Why Progestogen matters? Type of PMS/ VTE Risks Metabolic Breast Cancer Progestogen Androgenic effects1 risk effects Dydrogesterone Lower Lower Neutral Lower Utrogestan Androgenic Thrombogenic Unfriendly Higher Norethisterone (Neutralises (oral) Higher Higher beneficial effect of E2 on insulin , MPA lipids) LNG Local effect , Local effect Local Effect Local effect (MirenaTM ) minimal (lack of safety data) 1. Stevenson J. Gray S. Hormone replacement therapy (HRT) shortage: switching to Femoston® (estradiol/dydrogesterone) from an alternative combination oral or transdermal HRT. Guidelines Nov 2019. 2. EMAS Position statement on Diabetes
Odds ratio for VTE with different oral HRTs 1.Vinogradova Y, Coupland C, Hippisley-Cox J. Use of hormone replacement therapy and risk of venous thromboembolism: nested case-control studies using the QResearch and CPRD databases. BMJ 2019; 364: k4810.
Under 2 years
Which HRT? Systemic HRT Local HRT Has UTERUS – needs endometrial protection YES E+P Periods1 yr or age 54/55 Sequential HRT Cont Combined HRT-no period (Period HRT) After 2 years – 50 E+IUS
Types of HRT Estrogen Oestrogen Only( no uterus) Oestrogen (Sequential HRT) Monthly bleeds 17-28 Oestrogen Continuous combined HRT (CCHRT) but irreg bldg. x 6 Progestogen months No Bleed HRT Estrogen Progestogen Bleedd d
HRT Preparations ( Combined) E2 + P ORAL(ELESTE DUET ™ ) Oral ORAL ( FEMOSTON ™ ) E2+ Norethisterone (NET) Tibolone E2 + Dydrogesterone CONTINUOUS COMBINED HRT 1. SEQUENTIAL HRT 1. SEQUENTIAL HRT ● Oestrogenic, progestogenic, • Femoston ™ 1/10 • Elleste Duet ™ 1/10, NovofemTM androgenic effect • Elleste Duet ™ 2/10 ● Improves sex drive • Femoston ™ 2/10 ● Endometriosis ● Increased risk of stroke above 60 2. CONTINUOUS COMBINED HRT 2. CONTINUOUS COMBINED HRT • Femoston Conti ™ 1 mg • Elleste Duet Conti ™ 2 mg KliofemTM KliovanceTM/ • Femoston Conti ™ 0.5 mg • Kliofem ( 1 mg ) (PATCHES ) E2+ NET (PATCHES) E2+ LNG www.bms.org.uk. BMS update twice a week once a week on HRT supply shortages (2021) 1.Evorel Sequi ™ (50 Ug) 1. Femseven Sequi ™ (50 Ug) 2. Evorel Conti ™ 2. Femseven Conti ™
Tailor made HRT ( Mix& Match) ESTRADIOL Estradiol patch Estrogel ™ Sandrena gel ™ Lenzetto spray™ (Transdermal) Bioidentical HRT * Not licensed ➕ ➕ ➕ for use as part of HRT MICRONISED PROGESTERONE MIRENA™ Medroxy Progesterone acetate
SEQUENTIAL HRT CONTINUOUS COMBINED HRT Bio-identical HRT • Transdermal E2 + Micronised • Transdermal E2 + Micronised Progesterone (Utrogestan)capsule Progesterone(Utrogestan) daily • 100mg x 2(200mg) for 12 days • 100 mg (daily) • Licensed use – D15-D26 • Licensed use – D1-D25 MIX & MATCH • E2 + MPA (medroxyprogesterone • E2 + MPA ( 5 mg ) daily, if side effect acetate) can reduce to 2.5 mg daily monitor • 10 mg for 2 wks x month bleeding • Unlicensed use • Unlicensed use D1 Oestrogen D28 Oestrogen D14 Progestone Progestogen www.bms.org.uk
BIO IDENTICAL HRT- Recommended Indications Transdermal E2 + Micronised Progesterone https://thebms.org.uk/publications/consensus-statements/bioidentical-hrt/ 1. Patients with poor symptom control Cardiovascular risks , 2. Androgenic s.e with other Stroke risks e.g. Q Risk score VTE Risks 2, 3 HRT (PMS, acne, weight gain) 5-10%, metabolic syndrome , 3. Can help with Insomnia Diabetes with BMI>304 4. If shortages – of other HRT Breast Cancer Risk factors1 Patients on hepatic enzyme History of focal migraines, Limited 5 yr data from inducing agents (e.g. aura 5 anticonvulsants) observational study 1.Fournier A, Berrino F, Clavel-Chapelon F. Unequal risks for breast cancer associated with different hormone replacement therapies: results from the E3N cohort study. Breast Cancer Res Treat 2008; 107(1): 103-11 2. Vinogradova Y, Coupland C, Hippisley-Cox J. Use of hormone replacement therapy and risk of venous thromboembolism: nested case-control studies using the QResearch and CPRD databases. BMJ 2019; 364: k4810 3. Scarabin PY. Progestogens and venous thromboembolism in menopausal women: an updated oral versus transdermal estrogen meta-analysis. Climacteric 2018; 21(4): 341-5 , 4. Slopien R, Wender-Ozegowska E, Rogowicz-Frontczak A, et al. Menopause and diabetes: EMAS clinical guide. Maturitas 2018; 117: 6-10 KEEPS, ELITE study 5.Migraines and HRT. https://thebms.org.uk/publications/tools-for-clinicians/migraine-and-hrt/
When to Say No…..No to HRT? • Breast Cancer • E2 dependent cancers- Endometrial Cancer beyond Stage 1 • Current thromboembolic disease/ IHD • Active severe liver disease CAUTION • Migraine with aura • Hypertension. DM , Hyperlipidaemia • Past Hx of VTE/Family Hx of VTE • Endometriosis • Over 60 yrs
1. Sandra • Age 52, Para 2 , actor, upset , tearful , mood worsened, insomnia, low self esteem, - 12 months • Citalopram x 12 months , no effect • Periods are irregular, every 2-3 months in last year • Past Hx of PMS , Post natal depression , NIDDM on Metformin x 2 years BP-120/80, BMI=26, non smoker Drinks 10 units /week She requests a blood test for menopause
Decides to start oral HRT Why Sequential HRT? Month 1 Month 2 Month 3 Oestrogen Oestrogen Oestrogen 17-28 Prog 17-28 (E2 1mg + Dydrogesterone) (E2 + NETA) Elleste Duet TM Why? 1. Femoston™ 1/10 2. Mirena ™ and oral Estradiol tablet 1mg/ patches 1. Started Femoston- 1/10 ( 1mg E2 + 10 mg DG) Contraception: add a mini pill (DSG/levonorgestrel), barrier Ref: https://thebms.org.uk/wp- content/uploads/2018/08/HRT- Practical-Prescribing-AUG2018.pdf ( for doses)
Follow up Yearly • Age 54 Femoston Age 52 FU-3 months FU Age 59-60 Conti 1 mg Femoston • Still hot • Fed up Femoston 1/10 Check BP with Irreg bldgx 4 Conti 0.5 periods /12 mg Before starting HRT • Side effects Can change from Seq to CCHRT after 1-2 yrs • Benefits/Risks Sandra asks how long can I take HRT for? Femoston Yearly FU, BP check , Review changes in Hx 2/10 Benefit/Risk Analysis , Life style, Ca & Vit D
(Option 2) IUS + Estradiol IUS + E2 from age 52-57. Advantages of IUS • Unlicensed as part of HRT (x 5 yrs) • Reduces heavy periods • Local Hormonal effect with minimal side effects • Data on Breast safety are sparse At 57 , Remove IUS and change to Femoston Conti 1 mg ™ Mirena SPC: Bayer plc Lyytinen et al. A case control study on hormone therapy as a risk factor for breast cancer in Finland: IUS carries a risk as well. Int J Cancer.2010; 126:483-489
Daisy 51 yrs, very hot , insomnia, low mood tired , joint pains , gained weight – 2 years No Periods – 1 year Has tried herbal remedies – not seen much benefit CVS Risk factors BP - 130/88 , BMI=32 , non - smoker Past Hx : PCOS, pre-eclampsia HT on Rx Alcohol 2-3 bottles of wine/week NIDDM- Metformin Advise Life style interventions On statin No auto immune disease 1. Does she need contraception? VTE Risk factors 2. What are her HRT options ?? Personalise Risks and benefits BMI=32 Evaluate her CVS risks before starting HRT – Q Risk score = 7% If high risks – Alternatives to HRT Choice of HRT preparation depends on BMI , CVS/VTE risk factors Daisy has BMI= 32 , HT – Transdermal E 2 + Progesterone No periods x 1 yr - CCHRT
Why Bioidentical HRT? E2: Improves Insulin sensitivity , lowers Cholesterol , primary prevention of CVD (Cochrane review 2014 1) Moderate risk of CVD – Q Risk score is 5-10% HRT can be used with caution 1. Transdermal E2- thrombogenic neutral cf oral E2 2. Micronised Progesterone : insulin & lipid neutral, doesn’t increase her risk of thrombosis, lower risk of breast cancer 2 Low dose transdermal E2 + Micronised Progesterone(Oral Utrogestan TM 100 mg daily (unlicensed use) OR Mirena TM Counselling benefits & Risks, Ca and Vit D FACT sheet on bioidentical HRT https://thebms.org.uk/publications/consensus-statements/bioidentical-hrt/ 1. Boardman et al . Cochrane Database Syst Review 2015 . Hormone therapy for preventing CVD in post menopausal women . 2. An Endocrine Society Cl Practice Guideline . Wierman et al. JCEM2014, Climacteric, Maturitus 2/9/19
Effect of E2 HRT – in early and established atherosclerosis ( Menopause & CVD ) Menopause and CVD : Dr Louise Newson , Post Reproductive Health J, 17.01.2018
Unregulated Bio-identical /Body identical (Regulated) Oestrogel ™ Sandrena gel™ Lenzetto spray ™ Estradiol patches Utrogestan™ 1 measures daily (0.5 mg ) 1 spray can ↑2 sprays in (17B oestradiol) (Micronised 4-6 weeks if required 25, mcg twice a week Progesterone) CONTIUOUS COMBINED Licensed 100 mg cap D1-D25 Unlicensed ( daily) At bedtime, on empty stomach Vaginal insertion if s.e Drowsy, somnolence
Migraines and HRT • 2 fold increased risk of ischemic stroke, higher risk with oral E • Diagnosis of migraine +/- aura • Increased prevalence- fluctuating E levels, transdermal HRT advised • HRT is not a CI – migraine with aura • Continuous HRT preferred to cyclical • Preferred Progestogens- MirenaTM, UtrogestanTM, transdermal norethisterone in combined patches • Use lowest effective dose www.bms.org.uk FACT sheet • Anne MacGregor . Migraine, menopause & HRT . Post Reprod Health 2018 ; Vol 24(1) 11-18
When to refer for an Expert Opinion • Multiple Rx failures • Premature Ovarian Insufficiency ( POI)
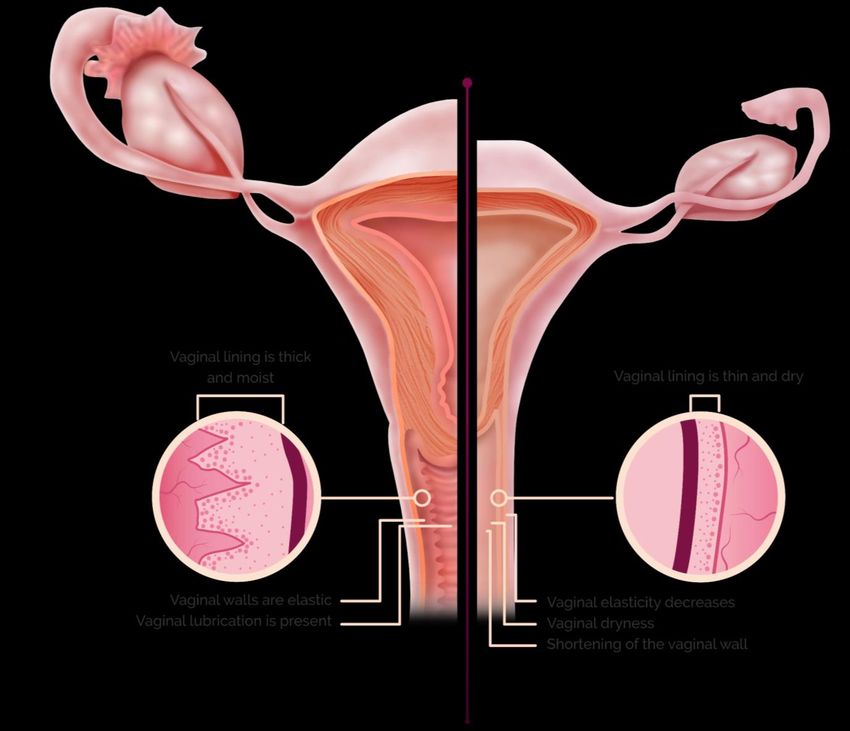
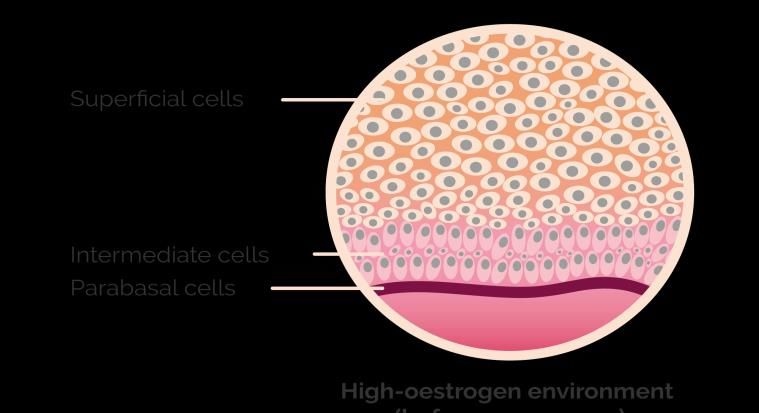
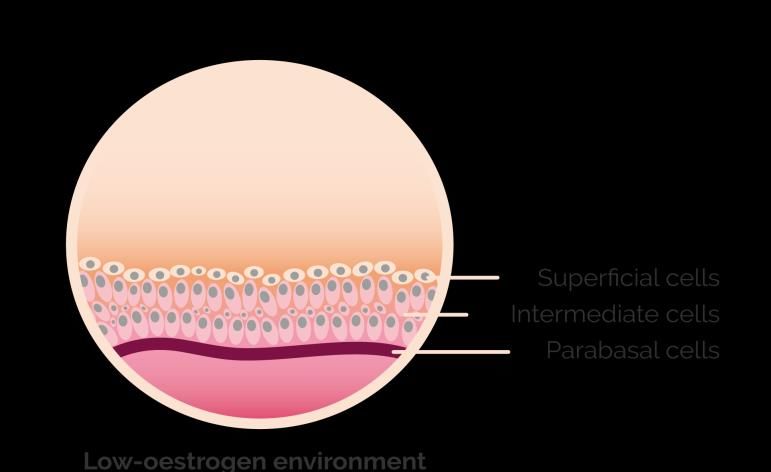
Genitourinary Syndrome of menopause ( GSM) Vagina before menopause Vagina after menopause 1. Johnston SL. Geriatrics & Aging. 2002;5(7):9-15. Adapted from Johnston 2002 2. Reiter S. International Journal of General Medicine 2013:6 153–158
Non Hormonal Therapies Lubricants • Pjur Med ( silicone based) • Yes: oil based , water based lubricant • Water based – Sylk, not so effective Moisturisers • Regelle, Replens, Hyalofemme , Yes Vaginal Moisturiser Laser Rx – CO2 , Erbium laser
Treatment OF GUS ( Genitourinary syndrome) • 17 B Estradiol ➢Vagifem (10 mcg) daily x2 w, foll by twice a week TM ➢Vagirux is therapeutically equivalent to Vagifem, single applicator, TM cheaper ➢Estring (trademark of Pfizer) ( 3 months) • Estriol (weaker than Estradiol) ➢Cream – Ovestin (0.1%- 500mcg /applicator)TM ➢Gel - Blissel (50 mcg) daily x 3 wks foll by twice a week TM ➢Pessary – Imvaggis (30 mcg) TM • Prasterone 6.5 mg : Intrarosa (DHEA)daily TM • Ospemifene (SERM) Oral tablet 60 mg daily TM 1. NICE Guidelines NG23; 2. BMS Consensus Statement 2018-Urogenital Atrophy 2. Public Assessment Report: Vagirux 10 micrograms vaginal tablets PL 04854/0184. October 2020. 2. Novo Nordisk. VAGIFEM (estradiol 10 microgram) vaginal tablets. Summary of Product Characteristics. September 2018. 3. Gedeon Richter. VAGIRUX (estradiol 10 microgram) vaginal tablets. Summary of Product Characteristics. 4. Gedeon Richter Plc. Data on File: Vagirux 2 – Therapeutic equivalence and systemic exposure study. September 2020. 5. Sturdee DW, Panay N, on behalf of the IMS Writing Group. Climacteric 2010;13:509–22. 6. NHS Sustainable Development Unit. Reducing plastic in the NHS. Available at: https://www.sduhealth.org.uk/nhs%20long%20term%20plan/single-use-plastics/reducing-plastic-in-the-nhs.aspx (Last accessed: November 2020).
Vagirux has an environmentally sustainable design ✓ Vagirux tablets are packed in blister pack, accompanied by a Applicators and packaging as supplied CE-certified applicator for multiple use, giving: Vagirux packaging1 £11.34 1 applicator sealed in foil and 24 tablets in a blister pack Up to 24 uses before disposal of the applicator1 With 24-tablet packs of Vagirux and a reusable applicator Less waste than single use applicators1,2 per pack, this could save 15.6 million plastic applicators from landfill.†1,4,5 Vagifem packaging2 £16.724 A positive user experience, with handling rated as 24 applicator sealed in individually sealed foil and “problem-free” by the majority of users in a focus 24 tablets in a blister pack group*3 *In 12 of 13 participants.3 †Calculation based on 24-tablet pack sizes. Also supplied as 18-tablet packs where marketed. 1. Gedeon Richter. VAGIRUX (estradiol 10 microgram) vaginal tablets. Summary of Product Characteristics. 2. Novo Nordisk. VAGIFEM (estradiol 10 microgram) vaginal tablets. Summary of Product Characteristics. 3. Gedeon Richter Plc. Data on File: Vagirux 2 – Therapeutic equivalence and systemic exposure study. September 2020. 4. NHS Business Services Authority. Drug Tariff. November 2020. Available at: https://www.nhsbsa.nhs.uk/sites/default/files/2020-10/Drug%20Tariff%20November%202020.pdf (Last accessed: November 2020). 5. NHS Digital (UK) GP Practice Prescribing Presentation-level Data. Organisation Data Service, Health and Social Care Information Centre, licensed under the Open Government Licence v3.0 (Last accessed: November 2020).
Duration & F/U of systemic HRT • POI - until age 51 at least 1 At 3/12, followed by Annual • >51 yrs : Informed choices, review (QS4) No arbitrary time limit Discontinue gradually- 2. BP, BMI makes no difference 3. Check Bleeding pattern, symptom • Individualise Rx & Risks: control - 50-60 = Benefits 4. Risk Benefit Analysis outweigh risk 5.Any changes in Medical History - 60-70 Benefits = risk 6. Dose reduction with age - Over 70 Risk outweigh benefits
Take Home Messages 1. Menopause is a CV risk factor - Life style intervention 2. Over 45 : No need for Blood test (FSH) 3. HRT within 10 years of menopause or under 60 – benefits outweigh risks, cardioprotective 4. Oestrogen matters : Consider dose, Transdermal : BMI>30, HT , Thyroxine, Migraines , VTE /CVS risk factors 5. Progestogen matters : Advantages of Dydrogesterone and Utrogestan in DM, CVS risks , VTE Risk factors, Breast cancer risk factors 6. Local E2 for GSM – can be added to systemic HRT
Training • BMS Principles & Practice Menopause • Patient info leaflet ( NICE) care www.bms.or.uk • http://www.pcwhf.co.uk/(Primary • Menopause & me leaflet Primary Care Womans Health Forum) • www.menopausematters.co.uk • www.menopauseacademy.co.uk • www.womens-health- • www.emas-online.org concern.org.uk • IMPART online learning • www.bms.org.uk www.imsociety.org • www.managemymenopause.co.uk www.ims.org ( Excellent webinars) • mywayhub.co.uk - webinars • www.menopausedoctor.co.uk • BMJ learning • www.nice.org.uk • Management of The Menopause- 6th edition -BMS
Thank you for your attention Continue to Stay Safe International menopause society
You can also read

















































