Hepatitis A - Arizona Department of Health Services
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Hepatitis A
Hepatitis A has a worldwide distribution1,2. In countries where sanitation is poor, infection
occurs at an early age; adults, however, are usually immune and outbreaks are rare1,3. In
developed countries, disease transmission can occur in child care settings with diapered
children and among household and sexual contacts of acute cases3. At-risk groups include
injection drug users, men who have sex with men (MSM), and travelers visiting endemic
countries3,4,5. Secondary attack rates of 15%–30% have been reported in households, with
higher rates of transmission occurring from infected children4. Attack rates among patrons
exposed to hepatitis A virus (HAV) infected food handlers are generally low3,4,5.
Hepatitis A became nationally reportable in 19662,6. During the pre-vaccine era, cases were
likely to report contact with another HAV case or childcare facilities, while post-vaccine era
cases indicated recent international travel7. The largest number of cases reported in one year
(59,606) was in 19712. Hepatitis A rates declined by over 95% from 1996 when the hepatitis A
vaccine was first introduced, through 2011, but re-emerged in 2016 in the United States due to
widespread outbreaks among persons reporting homelessness and drug use2.
A. Agent:
Hepatitis A virus, an RNA virus in the picornavirus family1,2,3,6.
B. Clinical Description:
Abrupt onset, with fever, malaise, anorexia, nausea, abdominal discomfort, vomiting, and
diarrhea1,2,3. Jaundice, dark urine and clay-colored stool follow a few days later1. Infections
range from asymptomatic to disabling illness that may last several months, but is seldom fatal
and not chronic1,5. Typically, symptom severity increases with age and duration of infection is
several weeks1,2. Prolonged, relapsing symptoms may occur for up to 6 months to 1 year in
about 15% of cases1,2,3.
▪ Differential Diagnosis: Clinically indistinguishable from other types of hepatitis and must
be diagnosed with laboratory tests2. Resources to consider:
- Diagnosis and Management of Foodborne Illnesses (CDC):
http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5304a1.htm
- Hepatitis A Differential Diagnoses (Medscape):
http://emedicine.medscape.com/article/177484-differential
C. Reservoirs:
Humans are the only natural host, rarely chimpanzees and other primates in laboratory
conditions1,2.
D. Mode of Transmission:
Direct and indirect person-to-person spread via the fecal-oral route1,2,5. Rarely, blood-borne
transmission can occur during the viremic phase of the disease2.
E. Incubation Period:
Range 15-50 days; average 28-30 days1,2,3,5,6.
F. Period of Communicability:
Hepatitis A Protocol
Last Revised: 3/28/2022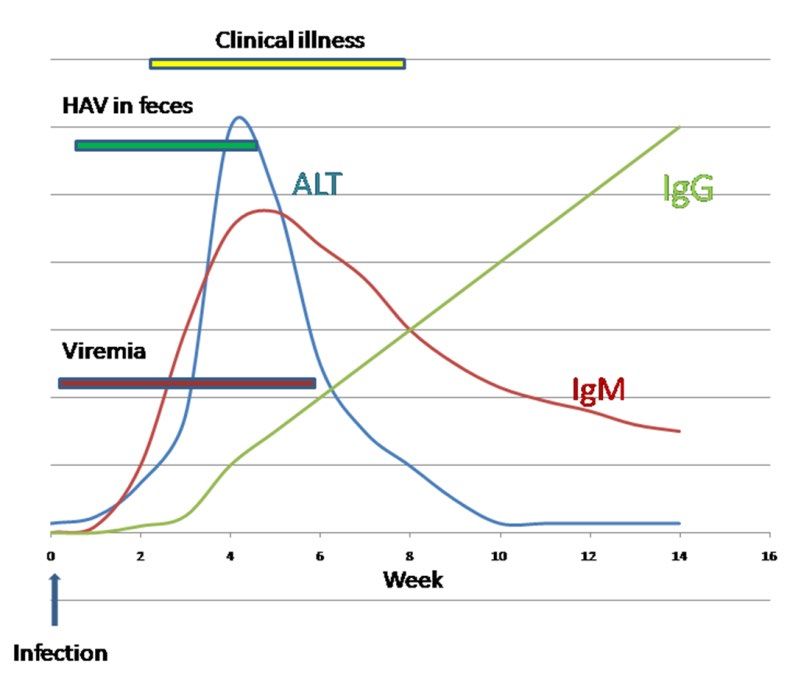
Most infectious from 1-2 weeks before symptom onset to about two weeks after non-jaundice
symptom onset or one week after onset of jaundice2,3. HAV replicates in the liver and is shed in
high concentrations in feces from 2 weeks before to 1 week after the onset of clinical illness2,3.
The greatest amount of viral shedding occurs 2 weeks prior to symptom onset2,3. Infants and
children, however, may shed virus for up to 6 months after infection2,3.
G. Susceptibility and Resistance:
Groups at increased risk for hepatitis A or its complications include international travelers,
MSM, and users of drugs2,3,5. Outbreaks of hepatitis A have also been reported among persons
working with hepatitis A–infected primates2. Other risk factors include sexual or household
contact with an infected person, and contact with a child or employee in child care3. Immunity
after infection lasts for life1,2,5.
In recent years, outbreaks have occurred primarily among individuals experiencing
homelessness/ unstable housing and those who use drugs, both injection and non-injection.
From November 2018 - December 2019, Arizona saw a hepatitis A outbreak with a total of 598
total cases16.
The Advisory Committee on Immunization Practices (ACIP) recommends that children receive
the Hepatitis A vaccine at 12-23 months of age2,3,6. Persons at increased risk for Hep A should
be identified and vaccinated, including international travelers, those with close contact with an
international adoptee from a country of high or intermediate endemicity, MSM, persons who
use illegal drugs, persons experiencing homelessness, persons who have a clotting factor
disorder, persons with occupational risk such as those who work with HAV-infected primates or
with HAV in a laboratory setting, and persons with chronic liver disease3,6. Refer to Pink Book,
14th edition, or CDC guidance for vaccination options2.
H. Treatment:
No specific therapy is available - only supportive care1,2,3,6.
Disease Management
I. Clinical Case Definition9:
An acute illness with a discrete onset of any sign or symptom consistent with acute viral
hepatitis (e.g., fever, headache, malaise, anorexia, nausea, vomiting, diarrhea, abdominal pain,
or dark urine), AND
● Jaundice or elevated bilirubin levels (total biliruin levels >3.0 mg/dL), OR
● Elevated serum alanine aminotransferase (ALT) levels (>200 IU/L), AND
● Absence of a more likely diagnosis.
J. Laboratory Criteria for Case Classification9:
● Immunoglobulin M (IgM) antibody to hepatitis A virus (anti-HAV) positive or reactive, OR
● Nucleic acid amplification test (NAAT; such as PCR or genotyping) for hepatitis A virus RNA
positive or detected.
Epidemiologic linkage
Contact (e.g., household or sexual) with a laboratory-confirmed hepatitis A case 15-50 days
prior to onset of symptoms.
Hepatitis A Protocol
Last Revised: 3/28/2022Case Classification9
Confirmed ● A case that meets the clinical description and is IgM anti-HAV positive/reactive*, OR
● A case that has hepatitis A virus RNA detected by NAAT (such as PCR or
genotyping), OR
● A case that meets the clinical description and occurs in a person with an
epidemiologic linkage, as defined above.
Probable A case that is IgM anti-HAV positive* but for which clinical illness information is
unavailable. If an investigation indicates the absence of clinical illness, the case should
be ruled out rather than classified as probable.
*And not otherwise ruled out by IgM anti-HAV or NAAT for hepatitis A virus testing
performed in a public health laboratory.
K. Classification of Import Status:
Import status reflects where the HAV infection was acquired: in county, in state, international,
out of county but in Arizona, out of state but in U.S., or location of infection is unknown.
L. Laboratory Testing:
Gold Standard – Detection of IgM anti-HAV. Serology, or anti-HAV tests, such as the enzyme
immunoassay (EIA), are available commercially. Since 2011, testing is no longer available at the
Arizona State Public Health Laboratory (ASPHL). Samples may be tested at CDC under certain
circumstances with prior approval by CDC.
TEST SPECIMEN & TRANSPORT COLLECTION TIME
Serology (IgM) Serum, EDTA-treated plasma (purple-top). During the acute phase of
1mL; 2mL preferred the disease.*
After collection, specimens may be stored at
room temperature (15-25°C) for up to 8 hours
or refrigerated (2–8°C) for up to 48 hours.
Specimens stored beyond these time points
must be frozen at or below -20 °C. Frozen
specimens should undergo no more than one
freeze-thaw cycle.
EIA Whole blood or serum, transported in a serum During the acute phase of
(Enzyme separator tube or red top vacutainer tube. the disease.*
Immunoassay) 1.0 mL (minimum 0.5 mL)
Keep refrigerated.
*IgM anti-HAV is detected 5-10 days before onset of illness and can be detected up to 6 months after illness onset2,3,6.
Polymerase Chain Reaction (PCR) – Can be used to amplify and sequence viral genomes,
particularly for outbreaks2. Consult with the state health department if specialized testing (e.g.,
molecular testing) at CDC is warranted. CDC will not accept any hemolyzed samples.
Hepatitis A Protocol
Last Revised: 3/28/2022M. Assessing Laboratory Results:
MARKER INTERPRETATION
HAV IgM 3
A reactive result indicates current or recent infection. A negative result indicates
absence of infection. False positive results may occur. Serum IgM anti-HAV is
detectable 5-10 days before symptom onset and declines to undetectable
concentrations within 6 months after infection; although people who test positive for
IgM anti-HAV more than 1 year after infection have been reported. IgM anti-HAV is
detectable in up to 20% of vaccines when measured 2 weeks after hepatitis A
immunization. (Confirmed case if also meets clinical criteria)
HAV IgG 2 IgG anti-HAV appears in the convalescent phase of infection, remains present in
serum for the lifetime of the person, and confers enduring protection against disease.
(If only IgG result case should be ruled out)
HAV total The antibody test for total anti-HAV measures both IgG anti-HAV and IgM anti-HAV.
Ab2 Persons who are total anti-HAV positive and IgM anti-HAV negative have serologic
markers indicating immunity consistent with either past infection or vaccination. (If
only HAV total Ab result case should be ruled out)
http://www.cdc.gov/hepatitis/Resources/Professionals/Training/Serology/training.htm
Criteria to Distinguish a New Case from an Existing Case
A case should not be counted as a new case if laboratory results were reported within 6 months
of a previously reported infection in the same individual. Although hepatitis A is usually self-
limiting and does not result in chronic infection, up to 10% of persons with hepatitis A may
experience a relapse during the 6 months after acute illnesses.
N. Outbreak Definition:
Diagnosis or detection of two or more individuals from different households and families who
experience an illness clinically compatible with hepatitis A virus infection, at least one with
confirmed HAV, after exposure to a common food or a shared experience; OR
An unexplained, unexpected increase in cases of confirmed HAV infection that is clustered by
time, place, or person.10.
Hepatitis A Protocol
Last Revised: 3/28/2022Investigation Guidelines
O. Time Frame11:
Begin investigation as soon as possible. Control measures should be initiated within 24 hours of
initial report and must be completed within 2 weeks of a contact’s last exposure to an
infectious case11. Outbreaks should be entered into the MEDSIS Outbreak Module within 24
hours of receipt of report.
Providers - Submit a report to the local health department within 5 working days
after a case or suspect case is diagnosed, treated, or detected11.
- Submit a report to the local health department within 24 hours after
detecting an outbreak11.
Schools, Childcare Submit a report to the Local Health Department within 24 hours after
establishments, detecting a case or a suspect case11.
Shelters
Laboratories - Submit a report to ADHS within 5 working days after obtaining a positive
test result11.
P. Forms:
N/A
Q. Investigation Steps:
Confirm Diagnosis12
▪ Contact the medical provider who reported or ordered testing of the case. Obtain
information from provider or medical chart.
o Obtain the reason for testing.
o If the patient is pregnant, obtain the due date.
o If patient is hospitalized, obtain medical records, including admission notes, progress notes, lab
report(s), discharge summary, and outcome status (survived or date of death).
▪ Record any acute hepatitis symptoms or signs, especially:
o Jaundice (if present, record date of jaundice onset).
o Elevated serum alanine aminotransferase (ALT) or bilirubin (total bilirubin).
o Clay-colored bowel movements or dark colored urine.
o Nausea, vomiting, abdominal pain, fever, fatigue, joint pain.
o With no jaundice, onset date of earliest acute symptom or if unavailable, collection date of first
elevated aminotransferase serum.
▪ Collect case’s demographic data and contact information:
o Birth date, county, sex, race/ethnicity, address, phone number(s).
▪ Through a credible immunization registry (ASIIS) or medical record, obtain information on
history of hepatitis A vaccine or immune globulin receipt.
Conduct Case Investigation12
▪ Attempt to interview the case as soon as possible.
o The investigator will attempt three phone calls, or text messages following unreturned voicemails,
before sending a letter to patient’s address.
o All interview attempts, even if unsuccessful (i.e., leaving a voicemail or text message), should be
entered into the Case Contacted & Interviews table in MEDSIS as close to real time as possible.
o If phone numbers appear invalid or non-functioning, fill out LexisNexis Request form to request a
LexisNexis search. This can be conducted for individuals 18 years and older. For those younger than
18 check in ASIIS for demographics. If ASIIS does not contain information, please have a
parent/guardian name available when requesting LexisNexis help..
▪ Collect information as specified on the investigation form and DSO.
Hepatitis A Protocol
Last Revised: 3/28/2022▪ Onset date used for the investigation is date of jaundice onset or, if no jaundice is present,
use the onset date of earliest reported symptom.
o If acute symptoms were present without jaundice but the onset date is unclear, use the collection
date of first abnormal aminotransferase.
▪ Inquire about activities 2-6 weeks prior to onset date:
o Number of male and female sex partners.
o Use of injection or non-injected drugs not prescribed by a doctor.
o Housing situation, to assess for housing instability or homelessness. Ask about any hotels or group
living situations.
o Travel history, including dates and places.
o Food history
o Exposure to a jaundiced person or a diagnosed or suspected case.
- List the name and address of contact or suspect case.
- Note relationship (non-sexual household member, sex partner, child cared for by case, babysitter
of case, playmate or other).
o Occupation, such as a child care worker, food handler, or health care worker.
▪ Inquire if anyone in household has traveled outside of the US or Canada in 3 months prior
to symptom onset.
Conduct Contact Investigation12
▪ Inquire about case’s activities and occupations during the communicable period (2 weeks
before illness onset until 2 weeks after jaundice onset).
o Record any child care association (including nursery school, preschool, or baby-sitting group), either
as attendee, employee, or household contact to attendee or employee. Include dates, location, and
activities.
o Record occupation and any other at risk activities such as food handling, child care, and/or direct
patient care with dates, descriptions, and locations.
▪ Consider case’s occupation and activities; identify the following contacts:
o Close personal contacts:
- Household and sexual contacts.
- Person who have shared illicit drugs with an infectious case.
- Person with other types of ongoing, close personal contact evaluated on a case-by-case basis
(e.g. regular babysitting of infectious child).
o High-risk contacts: those more likely to experience adverse outcomes from infection (people with
blood clotting disorder or chronic liver disease) and whose child care association, occupation, or
personal activities could result in further transmission of the virus.
o Child care facility contacts.
o Hospital/long-term care facility contacts.
o Food service contacts:
- Co-workers who work the same shift as infected food handler.
- Patrons of the establishment of an infected food handler if the infected food handler prepared
food that was not heated, the infected food handler had diarrhea, or if the facility’s/food
handler’s sanitation practices are deficient1.
▪ Identify and create a line list of primary contacts.
o Collect information of each primary contact’s hepatitis A immunization status, age, and any
symptoms of hepatitis.
o Collect information on the contact’s occupation.
o Note any child care attendance (include facility name and location).
o Note any high risk contacts (food-handler, child care attendee, health care worker).
▪ Follow up symptomatic contacts as suspected cases.
o A contact meeting the clinical case definition is considered a confirmed
Initiate Control and Prevention Measures
▪ Provide education that includes basic information about the disease and its complications
and ways to treat and prevent transmission of illness.
Hepatitis A Protocol
Last Revised: 3/28/2022o Emphasize hand washing, cleaning fingernails and personal hygiene especially after defecation and
diaper changing and before handling food12.
▪ If needed, notify appropriate administrative personnel to initiate investigation of the
facility to determine if others are at risk especially if case is a food handler or
establishment, a child care provider/attendee, and/or health care worker.
Arizona Food Code 2-201.11 requires that food employees must report to the “person in charge” information
about their health and activities as related to diseases transmissible through food (such as being diagnosed
with hepatitis A)17.
▪ Follow-up with case(s) and contacts to assure compliance with work and/or child care
facility restrictions.
▪ As appropriate, use notification letters and disease fact sheets to notify the case, contacts,
and other individuals and groups.
Isolation, Work and Child Care Restrictions
Per A.A.C. R9-6-343:
A. Case Control Measures - A local health agency shall:
1. Upon receiving a report under R9-6-202 or R9-6-203 of a hepatitis A case or suspect case, notify the
Department within one working day after receiving the report and provide to the Department the
information contained in the report;
2. Exclude a hepatitis A case or suspect case from working as a food handler, caring for patients or
residents in a health care institution, or caring for children in or attending a child care establishment
during the first 14 calendar days of illness or for seven calendar days after onset of jaundice;
3. Conduct an epidemiologic investigation of each reported hepatitis A case or suspect case; and
4. For each hepatitis A case, submit to the Department, as specified in Article 2, Table 4, the information
required under R9-6-206(D).
B. Contact Control Measures - A local health agency shall:
1. Exclude a hepatitis A contact with symptoms of hepatitis A from working as a food handler during the
first 14 calendar days of illness or for seven calendar days after onset of jaundice;
2. For 45 calendar days after exposure, monitor a food handler who was a contact of a hepatitis A case
during the infectious period for symptoms of hepatitis A; and
3. Evaluate the level of risk of transmission from each contact's exposure to a hepatitis A case and, if
indicated, provide or arrange for each contact to receive prophylaxis and immunization.
Contact Management
▪ PEP guidance can be found through CDC:
https://www.cdc.gov/mmwr/volumes/67/wr/mm6743a5.htm
▪ Contacts who are not immune to hepatitis A should be administered a single dose of
single-antigen hepatitis A vaccine or immune globulin (IG) within two weeks after
exposure3.
o Infants aged 40 years depending on the providers’ risk assessment For long-term immunity, the HepA vaccine
series should be completed with a second dose at least 6 months after the first dose; however, the
Hepatitis A Protocol
Last Revised: 3/28/2022second dose is not necessary for PEP. A second dose should not be administered any sooner than 6
months after the first dose, regardless of HAV exposure risk.
o Persons who are immunocompromised or have chronic liver disease and who have been exposed to
HAV within the past 14 days and have not previously completed the 2-dose HepA vaccination series
should receive both IG (0.1 mL/kg) and HepA vaccine simultaneously in a different anatomic site (e.g.,
separate limbs) as soon as possible after exposure. For long-term immunity, the HepA vaccination
series should be completed with a second dose at least 6 months after the first dose; however, the
second dose is not necessary for PEP. A second dose should not be administered any sooner than 6
months after the first dose, regardless of HAV exposure risk.
o In addition to HepA vaccine, IG should be considered for postexposure prophylaxis for persons with
special risk factors for either HAV infection or increased risk of complications in the event of an
exposure to HAV.
AGE OF EXPOSED INDIVIDUALS
40 years
Documented as fully
None None None
vaccinated
IG (0.1 mL/kg)§ plus single-
IG (0.1 mL/kg)§ plus single-
Immune compromised IG (0.1 mL/kg)*
antigen HAV vaccine† antigen HAV vaccine†
IG (0.1 mL/kg)§ plus single-
Healthy IG (0.1 mL/kg) Single-antigen HAV vaccine†
antigen HAV vaccine†
Vaccine is
IG (0.1 mL/kg) IG (0.1 mL/kg) IG (0.1 mL/kg)
contraindicated**
* Measles, mumps, and rubella vaccine should not be administered for at least 3 months after receipt of IG.
† A second dose is not required for postexposure prophylaxis; however, for long-term immunity, the hepatitis A vaccination series should
be completed with a second dose at least 6 months after the first dose.
§ The provider’s risk assessment should determine the need for immune globulin administration. If the provider’s risk assessment
determines that both vaccine and immune globulin are warranted, HepA vaccine and immune globulin should be administered
simultaneously at different anatomic sites
¶ Vaccine and immune globulin should be administered simultaneously at different anatomic sites.
** Life-threatening allergic reaction to a previous dose of hepatitis A vaccine, or allergy to any vaccine component.
▪ Hepatitis A vaccine or IG should be administered to all previously unvaccinated household
and sexual contacts of persons with serologically confirmed hepatitis A4.
o In addition, persons who have shared illicit drugs with a person who has serologically confirmed
hepatitis A should receive hepatitis A vaccine, or IG and hepatitis A vaccine simultaneously4.
o Consideration also should be given to providing IG or hepatitis A vaccine to persons with other types
of ongoing, close personal contact (e.g., regular babysitting) with a person with Hep A4.
The Local Health Department may provide hepatitis A vaccine and IG for contacts.
o Sources for obtaining IG and HBIG can be found on the CDC website:
http://www.cdc.gov/hepatitis/ig-hbig_sources.htm
o Below is a sample protocol the health department may want to follow:
- After conferring with and verifying the need for post-exposure prophylaxis with the appropriate
staff (program manager, medical officer, etc.), epidemiology staff shall coordinate via telephone
with exposed contacts to receive hepatitis A vaccine with the lead Public Health Nurse
(PHN/CHN) or other designated staff person.
- Epidemiology staff shall immediately notify via email their immediate supervisor and the PHN
Division Manager of the need to refer exposed contacts to lead nurse of the day.
- Upon immediate identification of exposed contacts and their need for hepatitis A PEP,
epidemiology staff shall notify via telephone the lead nurse of the day and provide the following
information:
▫ Name of individual(s), age and/or date of birth, weight, contact information (i.e. phone
number, address), language spoken by the individual or family.
Hepatitis A Protocol
Last Revised: 3/28/2022▫ Significant medical conditions such as pregnancy, immunocompromised, chronic liver
disease, and/or blood clotting disorder.
▫ Last calendar day by which exposed may receive post-exposure prophylaxis.
- Following date of planned PEP, epidemiology staff shall contact via telephone lead nurse of the
day and ascertain completion date of hepatitis A PEP for all exposed contacts.
▪ Counsel contacts to watch for signs of hepatitis A occurring within 45 days of exposure.
Should symptoms develop, medical care should be sought promptly.
▪ Follow-up and monitoring of contacts may be needed to assure no disease transmission.
Per A.A.C. 9-6-343, food handlers should be monitored for 45 calendar days after exposure for symptoms of
hepatitis A11.
▪ Report the number of susceptible contacts who received the recommendation for post-
exposure prophylaxis (vaccination(s) or IG).
▪ Healthcare providers administering HAV vaccine should report any adverse event that
occurs after the administration of a vaccine to Vaccine Adverse Events Reporting System
at http://vaers.hhs.gov/index.
Case Management12
▪ Educate case on measures to avoid disease transmission.
▪ Follow-up to assure compliance with recommended restrictions, especially if a case is
involved in child care, is a health care worker, or is a food handler.
▪ Follow-up with case to assure compliance with work and/or child care facility restrictions.
Environmental Measures12
None, unless a commercial food service facility, child care facility, health care facility or a public
water supply is implicated. In each case, coordinate with proper agency on the following
activities:
▪ Inspection of facility.
o If food establishment, Food Safety and Environmental Services program should be notified.
o If child care center, Child Care Licensing should be notified.
▪ Collection of food, drink or water samples.
Notifications11
▪ Report all cases, including suspect cases, to ADHS within one working day.
▪ If case or suspect case is a food handler, works in a childcare establishment or healthcare
institution, report to ADHS one working day.
▪ Enter hepatitis A outbreaks/suspected outbreaks into the MEDSIS Outbreak Module
(OBM) within 24 hours of receipt of the report.
R. Outbreak Guidelines:
Refer to Outbreak Section of the Disease Investigation Manual14.
Hepatitis A Protocol
Last Revised: 3/28/2022Daycare Worker or Attendee12:
● For one case, proceed with the following activities:
○ Coordinate the following activities with the local daycare inspector.
○ Interview the operator and inspect attendance records to identify any suspect cases
among staff, attendees or household contacts of attendees.
○ Ensure restrictions and/or exclusions for cases are initiated as outlined above.
● If >1 case among attendees/workers or in >2 households of center attendees:
○ Illness among adult staff members or household contacts is often the first indication of
daycare outbreaks since often HAV in young children is asymptomatic. In the absence of
plausible alternative hypotheses, two or more reported cases from different households
linked to the same facility should be investigated as an outbreak associated with a
daycare facility.
○ Contact ADHS.
○ Unvaccinated staff member(s):
■ Centers that provide care to children in diapers should have PEP administered
to all staff members and attendees.
■ Centers that do not provide care to children who wear diapers may have PEP
administered to only classroom contacts of the index case.
● In outbreak settings with hepatitis A cases in >3 families, PEP should also be considered for
members of households that have attendees in diapers.
● Affected facilities should be discouraged from accepting new children for 45 days after onset of the
last case, unless IG is given prior to admission or the child has been vaccinated. Transferring children
to other facilities should also be discouraged during this period.
● Conduct ongoing surveillance for hepatitis-like illness among households connected to the facility
for 45 days after onset of the last case.
Case is a Food Handler or Restaurant is Implicated12:
● If one case or suspect case is identified among staff or if >1 case or suspected case is associated with
the facility, a thorough inspection of the establishment is indicated.
● Coordinate the following activities with Environmental Health.
o Interview the manager and identify possible case(s) among staff:
o All food handlers at the establishment should be evaluated to determine whether
any have, or recently have had, hepatitis A.
o Co-workers who are considered contacts and are susceptible to HAV should
receive appropriate prophylaxis or be restricted or excluded from work for 45
days.
o The disease investigator and food service manager should monitor other food
handlers at risk for hepatitis A for one incubation period (i.e., 45 days) after the
last exposure to the index case.
o If other food handlers are found to be infected, the risk to patrons should be
carefully evaluated. The risk to patrons is determined by the following:
▪ The food handler worked while infectious,
▪ Had the opportunity to have bare-hand contact with ready-to-eat food,
and
▪ Had poor personal hygiene or diarrhea (Past and current inspection
reports of the facility’s sanitation practices may be used to evaluate the
personal hygiene of workers).
● In setting in which more than one employee is infected or if repeated patron exposures to HAV
might have occurred, stronger consideration of PEP use might be warranted.
● The identified need for prophylaxis of patrons is determined based on risk of exposure and if
patrons can be treated within 2 weeks of exposure.
Hepatitis A Protocol
Last Revised: 3/28/2022● If investigation indicates potential exposure to the general public and window for prophylaxis is still
open, consider public messaging and/or EpiX release to identify potentially exposed individuals that
would benefit from vaccine.
Public Gathering Implicated12:
● Sources may include food contaminated by a food handler.
● Conduct active case finding; ask about recent illness among food handlers.
● If a food establishment or distributor is implicated as the source of infection refer to food
handler/restaurant section above.
Long Term Care Facility, Residential Facility or Institutional Outbreaks12:
● Special measures may be required, including separate housing for cases and new admissions, and a
vigorous program of supervised hand washing.
● Coordinate efforts with institutional medical staff and appropriate regulatory agency.
Community Water Source Implicated:
Consult with ADHS Program Manager/supervisor when the investigation implicates a community
drinking water system.
Schools, Hospitals, Work Settings4:
● PEP is not routinely indicated when a single case occurs in an elementary or secondary school or an
office or other work setting, and the source of infection is outside the school or work setting.
● When a person who has hepatitis A is admitted to a hospital, staff members should not routinely be
administered PEP; instead, careful hygienic practices should be emphasized.
● Hepatitis A vaccine or IG should be administered to persons who have close contact with index
patients if an epidemiologic investigation indicates HAV transmission has occurred among students
in a school or among patients or between patients and staff members in a hospital.
Hepatitis A Protocol
Last Revised: 3/28/2022Additional Information & Resources
ADHS Disease Data, Statistics, & Reports:
http://azdhs.gov/preparedness/epidemiology-disease-control/index.php#data-stats-archive
Foodborne and Waterborne Disease Outbreak Investigation Resource Manual:
http://www.azdhs.gov/documents/preparedness/epidemiology-disease-control/disease-investigation-
resources/foodborne-waterborne-disease-outbreak-manual.pdf
Arizona Administrative Code Related to Infectious Disease:
http://apps.azsos.gov/public_services/Title_09/9-06.pdf
Outbreak Threshold Guide Healthcare Providers/Facilities:
http://www.azdhs.gov/documents/preparedness/epidemiology-disease-control/disease-investigation-
resources/outbreak-threshold-guide-providers.pdf
Arizona Food Safety Regulations:
https://www.azdhs.gov/preparedness/epidemiology-disease-control/food-safety-environmental-
services/index.php#az-food-safety-regulations
Manual for the Surveillance of Vaccine-Preventable Diseases:
http://www.cdc.gov/vaccines/pubs/surv-manual/chpt03-hepa.html
Additional CDC Resources:
- Webpage:
http://www.cdc.gov/hepatitis/hav/
- Vaccine Information Statement:
http://www.cdc.gov/vaccines/hcp/vis/vis-statements/hep-a.html
- Diagnosis and Management of Foodborne Illnesses:
http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5304a1.htm
- Prevention of Hepatitis A After Exposure to Hepatitis A Virus and in International Travelers. Updated
Recommendations (MMWR October 19, 2007: 56(41): 1080-1084):
http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5641a3.htm
- Hepatitis A Transmitted by Food (CID March 2004:38, 705-715):
http://www.cdc.gov/hepatitis/pdfs/fiore_ha_transmitted_by_food.pdf
Hepatitis A Protocol
Last Revised: 3/28/2022References
1. Spradling PR. Hepatitis A. In: Heymann. DL, ed., Control of Communicable Diseases Manual, 20th Edition.
Washington, DC, American Public Health Association, 2015: 253-257.
2. Hepatitis A [Internet]. In: Centers for Disease Control and Prevention. The Pink Book: Epidemiology and
Prevention of Vaccine-Preventable Diseases; 2015. Available from:
https://www.cdc.gov/vaccines/pubs/pinkbook/hepa.html
3. Kimberlin DW, Brady MT, Jackson MA, Long SS. Hepatitis A. In: American Academy of Pediatrics. 2021 Red
Book: Report of the Committee on Infectious Disease, 32nd Edition. Illinois, Academy of Pediatrics, 2021.
4. Novak R, Williams I, Bell B. Update: Prevention of Hepatitis After Exposure to Hepatitis A Virus and in
International Travelers. Updated Recommendations of the Advisory Committee on Immunization Practices
(ACIP) [Internet]. Centers for Disease Control and Prevention. CDC; 2007 [cited 2022January20]. Available from:
https://www.cdc.gov/mmwr/preview/mmwrhtml/mm5641a3.htm
5. Viral Hepatitis [Internet]. Centers for Disease Control and Prevention. Centers for Disease Control and
Prevention; 2020 [cited 2022January20]. Available from:
https://www.cdc.gov/hepatitis/hav/havfaq.htm#general
6. Klevens RM, Sharapov U. Hepatitis A. In: Manual for the Surveillance of Vaccine-Preventable Diseases
[Internet]. Roush SW, Baldy LM, editors. Centers for Disease Control and Prevention. Centers for Disease
Control and Prevention; 2014 [cited 2022January20]. Available from: https://www.cdc.gov/vaccines/pubs/surv-
manual/index.html
7. Erhart LM, Ernst KC. The changing epidemiology of hepatitis A in Arizona following intensive immunization
programs (1988–2007). Vaccine. 2012;30(42):6103–10.
8. Disease Data, Statistics, & Reports [Internet]. Arizona Department of Health Services. ADHS; [cited
2022January20]. Available from: http://azdhs.gov/preparedness/epidemiology-disease-
control/index.php#data-stats-archive
9. Arizona Department of Health Services. In: Case Definitions for Reportable Communicable Morbidities: 2022.
2022 [cited 2022Feb24]; Available from: https://www.azdhs.gov/documents/preparedness/epidemiology-
disease-control/disease-investigation-resources/casedefinitions/case-definitions.pdf
10. Arizona Department of Health Services. Hepatitis A. In: Outbreak Threshold Guide Healthcare
Provider/Facilities. 2011 [cited 2022January20]; Available from:
http://www.azdhs.gov/documents/preparedness/epidemiology-disease-control/disease-investigation-
resources/outbreak-threshold-guide-providers.pdf
11. Arizona Administrative Code. 2021Sep30 [cited 2022January20]; Available from:
http://apps.azsos.gov/public_services/Title_09/9-06.pdf
12. Hepatitis A Investigation Guideline [Internet]. Kansas Department of Health & Environment. KDHE; 2012 [cited
2021December14]; Available from:
http://www.kdheks.gov/epi/Investigation_Guidelines/Hepatitis_A_Investigation_Guideline.pdf
13. Fiore AE. Hepatitis A Transmitted by Food. Clinical Infectious Diseases. 2004Mar1;38(5):705–15.
14. Arizona Department of Health Services. Foodborne and Waterborne Disease Outbreak Investigation Resource
Manual [Internet]. Foodborne and Waterborne Disease Outbreak Investigation Resource Manual. Arizona
Department of Health Services; 2010 [cited 2022January20]. Available from:
http://azdhs.gov/documents/preparedness/epidemiology-disease-control/disease-investigation-
resources/outbreak-investigation-resource-manual.pdf
15. Nelson NP. Updated Dosing Instructions for Immune Globulin (Human) GamaSTAN S/D for Hepatitis A Virus
Prophylaxis. MMWR 2017:66(36); 959-960 (https://www.cdc.gov/mmwr/volumes/66/wr/pdfs/mm6636a5.pdf)
16. Hepatitis A Outbreak [Internet]. Arizona Department of Health Services. ADHS; [cited 2021December9].
Available from: https://azdhs.gov/preparedness/epidemiology-disease-control/hepatitis/hepatitis-a/index.php
17. https://www.fda.gov/food/fda -food -code/food -code-2017
Hepatitis A Protocol
Last Revised: 3/28/2022You can also read

















































