Health System Review PORTUGAL - APRIL 2018 - SNS
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

APRIL 2018
Health System
Review
PORTUGAL
Phase 1 Final Report
European
on Health Systems and Policies
a partnership hosted by WHO
Health System Review © World Health Organization 2018 (acting as the host organization for, and secretariat of, the European Observatory on Health Systems and Policies). All rights reserved. The European Observatory on Health Systems and Policies welcomes requests for permission to reproduce or translate its publications, in part or in full. The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the European Observatory on Health Systems and Policies concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the European Observatory on Health Systems and Policies in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters. All reasonable precautions have been taken by the European Observatory on Health Systems and Policies to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either express or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the European Observatory on Health Systems and Policies be liable for damages arising from its use. The views expressed by authors, editors, or expert groups do not necessarily represent the decisions or the stated policy of the European Observatory on Health Systems and Policies or any of its partners.

APRIL 2018
Health System
Review
PORTUGAL
Phase 1 Final Report
1
Health System Review
2
Phase 1 Final Report
Contents page
Introduction 7
Background 8
DOMAIN 1: HEALTH AND
ITS DETERMINANTS 9
DOMAIN 2: NHS SECTORIAL REFORMS
AND HUMAN RESOURCES 15
DOMAIN 3: PERSON-CENTRED, BETTER
INTEGRATED NHS 21
DOMAIN 4: NHS FINANCING 27
Conclusions and Recommendations 35
References 39
3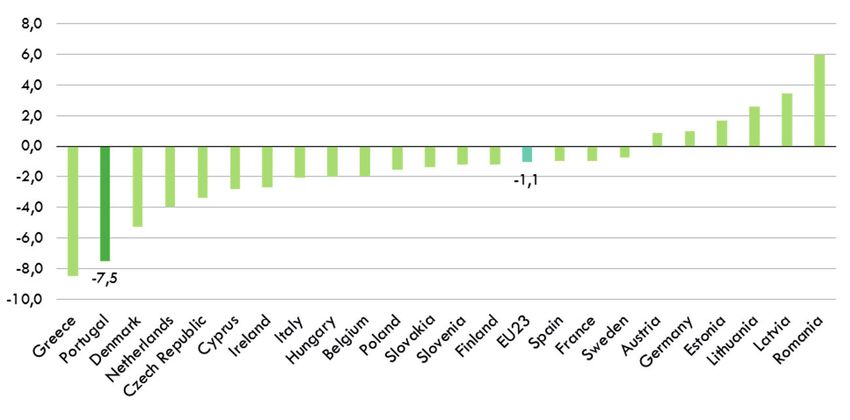
Health System Review
Abbreviations
EU European Union
GBD Global Burden of Disease
GP General Practitioner
IHME Institute for Health Metrics and Evaluation
IT Information technology
MoH Ministry of Health
NHP National Health Plan
NHS National Healthcare System
NPAPP National Physical Activity Promotion Program
OECD Organization for Economic Cooperation and Development
PPP Public Private Partnerships
WHO World Health Organization
4
Phase 1 Final Report
List of figures, tables and boxes
Figures page
Figure 1. Fertility rates in Portugal 1960 – 2014 10
Figure 2. Evolution of Monetary Poverty in Children and the Elderly, 2006 – 2014 10
Figure 3. Population at risk of poverty by working condition in Portugal 2003 – 2015 10
Figure 4. Unemployment rates in Portugal, seasonally adjusted, December 2016 11
Figure 5. Burden of Chronic Disease in Portugal, 2016 11
Figure 6. Multimorbidity in Portuguese population, by age group and gender 12
Figure 7. Depression among PHC (NHS) users in Portugal by health region. DGS, 2016 12
Figure 8. Healthy life expectancy at age 65, in European countries 12
Figure 9. Therapeutic cost of controlled diabetic patients in family health care units, by type of unit,
and health region 15
Figure 10. Long-term care services, by typology and health regions, 2017 16
Figure 11. Number of beds in Portuguese hospitals 16
Figure 12. Number of visits to the Emergency Departments (ED) per 100 population in Portugal 2002 – 2014 17
Figure 13. Doctors/nurses ratio in Portugal 18
Figure 14. Comparing health literacy across selected European countries 22
Figure 15. Health literacy levels by age and educational levels 22
Figure 16. Health expenditure as a percentage of GDP 27
Figure 17. Public Health expenditure 2010 – 2015 27
Figure 18. NHS expenditures in medicines in million Euros, 2003 – 2016 29
Figure 19. Out-of-pocket expenditure in the NHS market 30
Figure 20. Number of packages dispensed in the NHS market 30
Figure 21. Policy interventions related to medicines: Survey of measures taken in European countries
during 2010 – 2015 30
Figure 22. Average growth of the pharmaceutical market 30
Figure 23. Expenditure on pharmaceuticals per capita, 2014 (or nearest year) 31
Figure 24. Average medicines prices, 2003 – 2017 31
Figure 25. Generics Share, 2010 – 2016 31
Figure 26. Number of MEAs celebrated in the inpatient and outpatient settings 32
Table
Table 1. Current and capital expenditure in health 29
Box
Box 1. Persons centred NHS upgrade – main dimensions 24
5
Health System Review
6
Phase 1 Final Report
Introduction First, the initial findings of the assessment were
discussed with a panel of national and selected
international experts and decision makers. The aim of
In November 2016, the Ministry of Health of Portugal, this discussion was to identify key priorities and actions
the European Observatory on Health Systems and for strengthening the Portuguese health system which
Policies, and the Regional Office for Europe of the World could serve as a basis for policy development and
Health Organization (WHO) initiated an assessment policy implementation.
of the Portuguese health system in relation to its
For each of the four issues described above, a review
performance on key challenges and opportunities in
was made with the aim of framing the issue and
the post-financial crisis recovery period. The programme
describing the Portuguese context. Then, a review of the
of work included a review of the National Healthcare
ongoing responses was made, followed by a discussion
System (NHS) strengths and challenges. To provide
of further actions in order to face the challenges
focus, four key domains were used:
identified when the issue was made. Whenever possible,
• Domain 1: Health and its determinants examples of good practices and international guidelines
were integrated in this report.
• Domain 2: NHS sectorial reforms and
human resources The review was conducted by a team of international
and Portuguese health policy experts, and included
• Domain 3: Person-centred, better integrated NHS
extensive consultation with stakeholders from
• Domain 4: NHS financing government, healthcare employees and academia.
The preliminary findings from this review formed the
In addition, the current Portuguese priorities were basis for a policy dialogue in May 2017. This report
considered in the development of this report. There presents the findings of this review, taking on board
is ongoing public health reform, aiming at revitalizing the comments and contributions of Portuguese and
public health services and public health delivery in international experts in the Policy Dialogue.
Portugal. A new strategy for the National Health Plan
(NHP) is also a priority. Efforts have been made to
provide more and better quality person-centred care
in the NHS as a part of the strategies of the New
Public Health. This could be achieved using a two-fold
strategy: focusing on the local implementation of the
NHP on the one hand and on the promotion of health
literacy on the other hand. However, achieving a more
person-centred NHS is strongly dependent on the
progress of key sectorial NHS reforms. Another priority
is the digital transformation of the NHS, allowing for
both professionals and users to access information
and also tools which contribute to integrative care and
people centredness. The digital transformation would
also contribute to increase the transparency of the NHS,
which is a good practice for governance.
7
Health System Review
Background
Similarly to other European countries, the health system
in Portugal faces substantial challenges. These include
demographic changes, patterns of deprivation and
childhood poverty, unhealthy ageing, multimorbidity
and physical inactivity and consequences of the financial
crisis in the Portuguese NHS.
This report is divided in to four domains:
• Domain 1: Health and its determinants
• Domain 2: NHS sectorial reforms and human
resources
• Domain 3: Person-centred, better integrated NHS
• Domain 4: NHS financing
Each of these domains is further described below and
framed in the Portuguese context, together with a
summary of the key challenges encountered in each one
of them, followed by a summary of the main actions
already taken in Portugal and suggestions for further
actions to overcome the remaining challenges.
8Domain 1: Health and its determinants
DOMAIN 1: HEALTH AND ITS DETERMINANTS
1.1 Demography In Portugal the number of babies born alive have been
decreasing in the last decades for several reasons,
Portugal, in line with other European countries, has
including the lack of policies that support parenthood
had profound demographic changes, reflected in
and, formerly, the economic crisis. Portugal had the
the increase in longevity and the elderly population
lowest fertility rate in the European Union in 2014,
and in the reduction of the birth rate and the young
1.23 babies per woman, and was also the Member State
population. The number of elderly people tripled in
that registered the biggest births fall from 2001 to 2014.
the last 20 years, and this trend is expected to increase
in the coming years. The population of Portugal
1.2 Childhood and overall poverty, and
rose to 10.57 million in 2010, but has since fallen to
employment patterns
10.34 million (Simões et al. 2017). The Portuguese
population is expected to decrease to 7.5 million Studies conducted in several countries demonstrate
by 2080, with a sharp increase in the proportion of the impact of child poverty in areas as diverse as
the older population. The number of births has also physical and psychological health, education and
been decreasing in the last decades. Portugal was the qualifications, aspirations and expectations, wages in
European Union (EU) country with the lowest fertility adulthood, unemployment or dependence on social
rate in 2014 (1.23 children per woman) and was also security (Eurochild & EAPN, 2013; UNICEF, 2007).
the Member State that registered the highest reduction Children growing up in poverty are more likely to fall ill
in births between 2001 and 2014. The lack of policies throughout their lives and to die younger than children
to support parenthood coupled with the economic crisis growing up in better financial conditions; they are also
may have contributed to this reduction. more likely to suffer from a chronic illness or a disability.
The World Bank Group (UNICEF, 2016) notes the impact
Migration is also a key element in demographic changes.
of poverty on well-being, employment prospects and
The study “Migration and macroeconomic performance:
expectations of poor children. They can develop low
an exploratory analysis of the Portuguese case” found
motivation, have low aspirations, hopes and dreams.
that the current crisis may ultimately cause lasting
inflections in migration flows. In recent years there has In Portugal, the phenomenon of child poverty was
been a gradual decline in immigration coupled with studied by Bastos and Nunes between 1995 and 2001
a sudden increase in emigration. These changes can (Bastos e Nunes, 2009). They confirmed the vulnerability
be attributed to a need to escape from the economic of children and the increased risks of poverty, especially
crisis experienced by the Portuguese population. among children who belong to single parents and in
However, this increase in emigration will have important families where there is unemployment. Portugal has
consequences for the Portuguese macroeconomic historically had relatively high levels of deprivation and
performance in the long run, in particular through poverty, and continues to have overall poverty rates
the “brain drain” associated with the combination above the EU average. This is particularly the case for
of increased emigration, ageing of the Portuguese children, and rates of child poverty rose significantly
population and a reduced immigration. Portugal faces a during the financial crisis period. This contrasts with the
double challenge: preventing brain drain and attracting lower and generally declining risk of poverty in older
qualified immigration. people, as can be noted in Figure 1.
9Health System Review
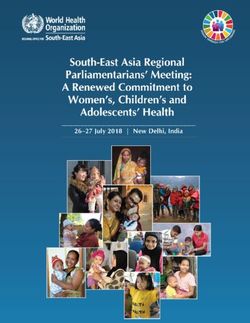
Figure 1. Fertility rates in Portugal 1960 – 2014 The poverty risk rate for the elderly population increased
again in 2015, with 18.3% (17.0% in the previous
year). On the other hand, a new reduction in the risk of
3.2
poverty for those under 18 years of age was recorded
3.0
in 2015: 22.4%, which is -2.4 percentage points (pp)
2.8 compared to 2014. The poverty rate for adults was
2.6 18.2%, down 0.6 percentage points from the previous
2.4 year (18.8% in 2014).
2.2
2.0 2014 (1.23) Figure 3. Population at risk of poverty by working
1.8
condition in Portugal 2003 – 2015
1.6
1.4
Portugal
1960 1965 1970 1975 1980 1985 1990 1995 2000 2005 2010
Source: Pordata, INE, Indicadores Demográficos, Anual.
The child poverty rate in 2015 was measured by the
proportion of inhabitants with income lower than
5 268 euros per year (439 euros per month). In 2015,
families composed of 2 adults and 3 or more dependent
children and families with one adult and at least one
dependent child have the highest risk of poverty (42.7%
and 31.6%, respectively). (Report “Inequality of Income
Source: EU-SILC.
and Poverty in Portugal, the social consequences of
the adjustment program” of the Francisco Manuel dos
The risk of poverty for the unemployed population was
Santos Foundation, in September 2016).
42.0% in 2015, maintaining the value registered in the
previous year. The risk of poverty for the employed
Figure 2. Evolution of Monetary Poverty in
population was 10.9% in 2015, unchanged from 2014.
Children and the Elderly, 2006 – 2014
In 2015, the risk of poverty increased in the retired
population, with a rate of 16.0% compared to 14.4%
30%
in 2014 (+1.6 pp). However, it has maintained the
28% decreasing trend observed in the series for this indicator:
25.5% 25.6% minus 10 percentage points since 2003.
25% 24.4%
22.8% 22.9% 22.4% 22.4%
24.8% If we consider the at-risk-of-poverty rate before social
21.8%
23%
20.9% transfers, the rate remains almost stable between 2013
20%
22.3% and 2014 in the EU-28 while it rises a bit more in some
22.0%
20.1% 20.0% EU Member States, with the largest increases registered
18% in Belgium, Finland, Portugal (each 1.2 percentage
15%
17.4% 17.0% points) and Sweden (1.4 percentage points).
15.1%
13%
14.7% Finally, the report “Inequality of Income and Poverty
in Portugal, the social consequences of the adjustment
10% program” of the Francisco Manuel dos Santos
2006 2007 2008 2009 2010 2011 2012 2013 2014 Foundation, in September 2016, concludes that one
Children Elderly
of the most affected vulnerable groups were “young
families with children” and that in “2014 it is possible
Source: National Institute of Statistics. to verify that 58.4% of the poor population belongs to
households with children.”
The “at-risk-of-poverty” rate in 2015 corresponded to
Unemployment in Portugal is high by EU standards,
the proportion of people with an annual net monetary
with only 5 of the EU 28 countries having higher
income, per adult, equivalent or less than 5 268 euros
unemployment. This feeds both directly and indirectly
(439 euros per month). This threshold, or poverty line
(through associated poverty) into health needs.
corresponds to 60% of the median (8 780 euros)
Young adults are at particular risk of unemployment
monetary income.
and precarious work. According to the Monthly
The risk of poverty is much lower among working Provisional Employment Survey, the seasonally adjusted
people, and unemployment is higher in Portugal unemployment rate (15 to 74 years) was 10.5% in
than the EU average. Additionally, rates of precarious December 2016, with a clear trend towards further
employment are high in Portugal particularly among decline, see Figure 4).
younger workers.
10Domain 1: Health and its determinants
Figure 4. Unemployment rates in Portugal, 1.4 Multimorbidity and mental health
seasonally adjusted, December 2016
Multimorbidity is closely related to age and socio-
economic conditions and most adults attending primary
health care have more than one chronic condition.
Studies on the epidemiology of multimorbidity show
that its prevalence increases with age, its onset is
10 to 15 years earlier in those living in deprived areas
compared with the more affluent ones and is strongly
associated with mental health disorders (Barnett et al.,
2012.
Ageing means that more people are living with multiple
chronic conditions (Rechel B, 2013). This has important
implications for care delivery, since in most cases the
treatment of one disease will be in the context of other
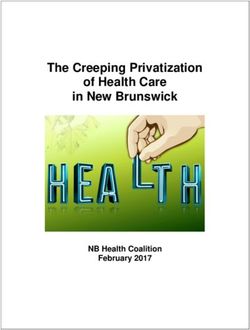
chronic conditions. Figure 5 shows the distribution of
the burden of chronic diseases in Portugal, with 41% of
Source: Eurostat the NHS users having multimorbidity (more than one
chronic disease).
The percentage of the population in a precarious work
situation in European countries is 12.3%. However, Figure 5. Burden of Chronic Disease in Portugal,
countries like Portugal, Spain, Poland, Slovenia and the 2016
Netherlands have a far higher rate, more than 20%,
young people are most affected because they cannot
find a permanent job.
Between 2000 and 2015, more than 75% of 22%
employment contracts were considered precarious by
the International Labour Organization – the same rate
as in Spain, Slovenia and Greece. Precarious work has
41%
several consequences, both for companies, workers and 41%
multimorbidity
the social economy itself, leading to less innovation, 8%
lower productivity, a risk to the sustainability of social
security systems, difficulties in accessing credit and
postponement in the decision to start a family. 11%
1.3 Obesity and physical inactivity
18%
Levels of obesity are rising, related to both unhealthy
diets and low levels of physical activity. Of the ■ No Chronic diseases ■ 1 Chronic disease ■ 2 Chronic diseases
population aged between 25 and 74 years old, 28.7% ■ 3 Chronic diseases ■ 4 or more Chronic diseases
are obese, and 38.9% pre-obese. There is a strong Note: Percentage of NHS users with chronic diseases.
socio-economic gradient with 43.1% of adults with
only basic education being obese, but only 14.7% of 22% of the population has 3 chronic conditions and
those with a university education. Portugal already 4% has 5 or more. Diabetes is an example of a chronic
has a system for identifying, managing and combating disease which is associated with multimorbidity, posing
pre-obesity in primary health care to prevent it from major challenges to health systems across Europe. The
developing into more severe clinical conditions (PAI – rate of diabetes provides a useful indicator of the
Pre-Obesity / DGS). However, the system is still in the success of population level interventions. In Portugal, the
very early stages of implementation and only 5.2% prevalence of diabetes in the adult population increased
pre-obese are registered in primary health care. The from 11.7% in 2009 to 13% in 2013. It will probably
prevalence of childhood obesity at 8 years old in rise with population ageing and may increase as a result
Portugal, measured by the same method (COSI / WHO of higher prevalence of obesity. The mortality rate from
study) seems to be stable over the last 3 measurements diabetes has been decreasing in the last years.
over 6 years.
Physical activity levels in Portugal are among the lowest
in Europe, in adults and particularly in teenagers. Up
until 2016, physical activity promotion did not have a
dedicated program at the Portuguese Health Ministry.
This was changed with the creation of the National
Physical Activity Promotion Program (NPAPP) which was
introduced in June 2016.
11Health System Review
Figure 6. Multimorbidity in Portuguese population, In 2014 the life expectancy at 65 years was 19.2 years
by age group and gender (17, 3 years for men and 20, 7 years for women). The
overall life expectancy at 65 years in 2015 was 19.3
90
years (PORDATA, 2017).
80
70 Figure 8 Healthy life expectancy at age 65, in
European countries
% with multimorbidity
60
50
40
30 20
18
20
16
10
14
Healthy years
0 12
[0;10] [10;20] [20;30] [30;40] [40;50] [50;60] [60;70] [70;80] [80;90] [90;150]
10
■ Men ■ Women Age groups 8
6
4
16.3
15.3
15.3
11.9
11.7
11.5
11.1
10.3
10.3
10.1
10.0
9.7
9.4
9.2
9.2
8.3
8.0
7.9
7.8
7.7
7.7
6.2
5.9
5.3
4.1
4.0
2
0
Mental illness has been identified as a problem that
en
No nd
er y
Ire y
De and
ite Bel k
ng m
F m
itz ce
th nd
m s
O urg
25
ec Fin n
Re d
Po ic
Sl nd
Au ia
G ia
e
Po aly
Hu gal
Es ry
a
Sl via
ia
G wa
an
xe nd
ar
ec
ni
ai
lan
bl
en
r
ak
a
d giu
do
st
Sw ran
ed
ela
Ne erla
D
la
It
t
Sp
to
rtu
ng
nm
bo
pu
La
m
re
Lu erla
l
r
ov
ov
EC
Sw
Ic
Ki
needs better services. There has been a shift away
h
Cz
Un
■ Total ■ Male ■ Female
from hospital treatment of mental illness and there
is evidence, in some diseases, of an increased use of Note: Countries are ranked in descending order of healthy life expectancy for the whole population.
Source: Eurostat Database 2017
medication. As is common in EU countries, there are Source: Eurostat Database, 2017.
identifiable gaps in mental health care. Note: Countries are ranked in descending order of healthy life expectancy for
the whole population.
Portugal has the highest per capita prescription of
anti-depressants in the EU, with 60% of the DDD of
Selected recent and ongoing developments
psychiatric drugs prescribed in the NHS, at a national
level, of 341 604 888. The increase was 5% compared In the budget for 2017 the government introduced a
to 2014 (the lowest in relative terms since 2011), new tax for sweetened beverages, the tax is based on
and this value does not pose similar concerns to the sugar content (Law 42/2016, de 28 de November,
those of the previous group. The antipsychotics, also articles 212.º, 213.º e 215.º). Whether this marginal
maintained a growth trend (since 2013) but only 2%, increase in tax will impact on the consumer price and
reaching 45 770 580 DDD, corresponding to 7% of the effect on consumption, is still to be seen. Moreover,
the group of psychotropic drugs. Depressive disorders the Government introduced a law to ban sugary
increased substantially in Portugal during the recent drinks and high density caloric food from the vending
economic crises. machines in NHS facilities.
A National Physical Activity Promotion Program (NPAPP)
Figure 7. Depression among PHC (NHS) users in
was introduced in June 2016, aimed at implementing
Portugal by health region
the recommendations laid down by the WHO European
Region’s “Physical Activity Strategy 2016 – 2025” and the
12 DGS’s “National Strategy for the Promotion of Physical
Activity, Health and Well-being 2016 – 2025”. The main
10
priority of the NPAPP is to establish an efficient and
8 well-resourced multi-sectorial platform that can engage,
Percentage
coordinate, and monitor national initiatives to promote
6
physical activity across all relevant sectors. NPAPP’s
4 specific contributions to a national Action Plan will focus
2 on the health sector, with the aim of physical activity
promotion becoming an integral part of the national
0 health system, especially among primary care units.
2011 2012 2013 2014
— North — Centre — Lisbon and the Tagus Valley
Public health campaigns to reduce salt and sugar usage,
— Alentejo — Algarve as well as tobacco smoking have been planned.
Source: DGS, 2016.
A number of public health programs, within the National
Plan Health framework are been implemented. For
example, one of these national programs has been
1.5 Unhealthy ageing dealing with diabetes risk evaluation using FinDRisk
While life expectancy has increased, data suggest that score. Its implementation in primary care units resulted
relative to other comparable European countries, healthy in 1.2 million risk evaluations being performed in
life expectancy has performed less well. While some of 2014 and 2015 in asymptomatic people. The screened
this may reflect measurement issues, and may reflect people with medium or high risk were then referred to
past deprivation levels affecting this age group, the poor a General Practitioner (GP) appointment. The national
outcome compared to other countries is a concern. program to prevent diabetes developed an integrated
care model based on a multidisciplinary approach.
12Domain 1: Health and its determinants
Key challenges – the way forward The National Health Plan provides a very useful basis
for actions tackling these challenges, but much more is
• The health system in Portugal will require long term
needed in terms of:
strategies to tackle the health consequences of family
deprivation, unemployment and child poverty which • Linking planning at national, regional and local levels;
were exacerbated during the financial crisis.
• Closer working with NGOs and civil society to
• Population ageing and unemployment coupled with implement public health plans, creating broader
high migration of younger people of working age opportunities for public participation;
contribute to an ongoing decline of the Portuguese
• Further modernisation of the public health workforce
population. This affects the demand and the supply
and providing stronger support for the development
of health services.
of the local public health units;
• The majority of users of the NHS have one or more
• Wider use of health impact assessment to guide and
chronic diseases which has important implications
monitor public health actions.
for the delivery of services: services are no longer
provided adequately in single disciplinary approaches.
The increasing prevalence of multi-morbidity also
calls for more attention to be paid to improving
quality of life in elderly people and community and
home care settings. Closer collaboration between
health care and social care organization is of
fundamental importance.
• There is a need for a particular focus on actions to
improve healthy life expectancy, especially among
older women.
• Diet and physical activity are among the most
pressing population health challenges in Portugal,
calling for continuing the current investment on
effective and more equitable health promotion and
disease prevention policy and implementation.
• Portugal has a strong record in development of
health plans and strategies, and weaknesses in local
approaches to implementation.
13Health System Review
14Domain 2: NHS sectorial reforms and human resources
DOMAIN 2: NHS SECTORIAL REFORMS AND
HUMAN RESOURCES
The Portuguese NHS is organized into five health regions Figure 9. Therapeutic cost of controlled diabetic
and aims to provide access to all effective medical patients in family health care units, by type of unit,
services on the basis of need. Though regulation, and health region
monitoring, control and financing of the public
health system are within the central administration EURO
competences, the principle of decentralization and 500
autonomy in the operational management of health 400
organizations has been granted since the establishment
of the NHS in 1979. However during the period of the 300
Cost
financial crisis, there was a set of actions and policy 200
355 313 334 436 333 318 388 346 311 352 307 267 366 314 285
measures that significantly diminished the extent
of decentralization and autonomy of healthcare 100
organizations within the NHS. 0
Alentejo Algarve Centre Lisbon and North
the Tagus Valley
Types of primary health care unit:
2.1 Primary health care ■ non-reformed family health units
■ reformed family health unit, without performance related pay
■ reformed family health unit with performance related pay
Primary health care reform has been strongly focused Source: BD NSCP (ACSS)
on transforming traditional health centres into network Source: BD NSCP (ACSS).
functional units, such as family health units, community
health care units, others health specialties support units 2.2 Long term care
and public health units. Changes in family health care
units towards contracted self-managed units, with The National Network of Continuing Integrated Care
performance related pay, have been made progressively (RNCCI) is defined as a response focused on providing
over the last decade. The main purpose is to create care to people who, regardless of age, are in a situation
more autonomous and multidisciplinary teams in of functional dependency. The purpose of the Network
primary care, and incentives for better performance is the rehabilitation and social reintegration and the
(e.g. better follow up of patients, notably chronic provision and maintenance of comfort and quality of life,
patients, better pre and post-natal care, more cost- even in cases where no recovery is possible.
effective use of medicines). By the end of 2017 there In January 2018 RNCCI is characterized by offering
were approximately 390 non-reformed family health 8 224 inpatient responses and 5775 home care
units versus 505 reformed one. Of the reformed health responses for adults. It also offers 10 inpatients and
care units, approximately 235 benefit from performance 10 ambulatory responses for children with complex
related pay, while 270 do not enjoy that benefit yet. chronic illness. Finally, it offers a diversity of inpatients
home and care responses, totaling 197 beds / places, for
young people and adults with severe mental illness and
psycho-social dependence.
Care for children with complex chronic illness and for
young people and adults with severe mental illness was
offered for the first time during 2017 and is therefore in
the experimental year.
15Health System Review
Figure 10. Long-term care services, by typology and
health regions, 2017
Health Region
ARS Lisboa
and Vale
Typology of Units ARS Alentejo ARS Algarve ARS Centro do Tejo ARS Norte Total
Convalescence Unit 135 74 251 199 157 816
Palliative Care Unit 14 – – 129 26 169
Medium Duration and Rehabilitation Unit 203 138 735 720 742 2 538
Long Term and Maintenance Unit 431 317 1 297 1 119 1 537 4 701
Pediatric Support Unit – – – 10 10 –
Assisted Living – – 13 14 27 –
Home Support Team – – 8 8 8 24
Integrated Continuing Care Team 566 750 846 2 072 1 641 5 875
Maximum Support Residence – – 24 – 24 –
Moderate Support Residence – – 8 16 – 24
Residence of Autonomy Training – – 19 – 19 –
Residence of Autonomy Training – Type A – – – 12 6 18
Integrated Pediatric Care Unit – Type 1 – – – 10 10 –
Socio-Occupational Unit – – 30 25 55 –
Socio-Occupational Unit – Childhood
– – 20 10 30 –
and Adolescence
Total 1 349 1 279 3 175 4 351 4 186 14 340
2.3 Hospital care
In Portugal, there are 113 public and 96 private hospitals. In 2002, private hospitals provided 16.5% of the total
In 2013 there were 25,000 beds in public hospitals and number of visits to Portuguese hospitals (around
10,500 in private hospitals. There has been a reduction 1.6 million visits), while in 2013 they accounted for 29%
of 1,659 beds in total since 2002, but a rise in the (around 5.1 million consultations).
proportion that are private. Portugal has rates of visits to emergency departments
(ED) considerably higher than other OECD countries
Figure 11. Number of beds in Portuguese hospitals (OECD average 30.8 visits / 100 inhabitants). That
pattern has remained fairly constant over the years;
however the ED visits in private facilities have risen,
35 503 contrasting with a small decline in NHS ED visits. The
0
00
40
37 162
Number of hospital beds in Portugal
literature points out that part of the demand for ED
0
00
35
25 029
visits could be treated elsewhere more efficiently,
0
28 733
00
30
namely in primary care by telephone-based services
0
00
25
0
(McHale et al. 2013), these visits were designated as
00
20
0
non-urgent or inappropriate. In Portugal a study found
00
15
10 474
0
8 429
00
that up to 30% of these visits could be inappropriate
10
0
00
0 (Pereira S, 2001). The ACSS access report states that
5
2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013
Total Public hospitals Private hospitals 8.6% of the user and considered frequent users (4 or
more visits in a year), those 8.6% represent 27.9% of
the ED visits.
16Domain 2: NHS sectorial reforms and human resources
Figure 12. Number of visits to the Emergency 2.4 Public-Private Partnerships (PPP)
Departments (ED) per 100 population in Portugal
The creation of Public-Private Partnerships (PPP) granted
2002 – 2014
more autonomy to organizations by conceding the
management of service units of care to private entities,
80 72 73 71 73 73 75 74 75 75 74 71 72 74 or by the joint investment between them and the State
(Barros, Machado & Simões, 2011). According to the
Number of visits to ED / 100 population
70
60 current Portuguese PPP legal framework (Decree-Law
50 n.º 111/2012, of May 23rd), a PPP is defined as “(…) a
40
contract or union of contracts through which private
30
entities, designated as private partners, oblige, in a
20
durable way, before a public partner, to assure, upon
10
0
payment, the development of an activity tending
2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 to the satisfaction of a collective need, in which the
Year in analysis responsibility for the investment, financing, operation,
Total ED visits NHS ED visits Private ED visits
and associated risks, falls, in whole or in part, to the
private partner”.
Research has shown that PPP hospitals are generally
Concerning the reorganization of the hospital network,
efficient, in particular the hospitals of Braga and Cascais,
there is still a major gap of evidence regarding
which presented outstanding positive results. However,
the efficiency gains obtained by the merging and
it was not possible to identify statistically significant
concentration of services, hospitals and management
differences between the results of the PPP and the
boards. Likewise, the internal and intermediate
non PPP subgroups.
management of NHS hospitals also needs to be
improved, since their autonomy has been reduced by Results indicated that most PPP hospitals have on
the measures taken in the context of the economic and average a higher capacity for surgeries than the other
financial adjustment plan (Simões et al.,2017). comparable public hospitals, while they mostly present
a lower than average percentage of hip fractures
Hospitals are paid on global budgets based on
surgically repaired within 48 hours. Yet, all PPP
diagnosis-related groups, with the possibility to
hospitals presented a higher than average percentage
reallocate resources across cost-categories. In addition
of outpatient surgeries on planned surgical care for
to the transfers from the government, hospitals
ambulatory care-sensitive conditions, which means a
generate their own revenue, through flat rate user
better performance than comparable hospitals, with
charges for outpatient and diagnostic services, special
significant statistical difference between groups. As
services (e.g. individual private rooms) and from
far as the fulfilment of the maximum waiting times
privately insured patients. The contract covers several
imposed by law is concerned, PPP hospitals presented
areas, like consultation, inpatient care, and emergency
a better performance than comparable hospitals in the
care, among others. A new system of incentives for
case of surgeries, but a generally worse performance
hospital performance was created in 2017, which
regarding first outpatient appointments.
values comparisons and positive competition among
institutions, identifying the differences in care
2.5 Human resources
performance and efficiency that now occurs in hospitals
with similar characteristics, providing operational In 2014, the Ministry of Health employed 124 260
levers to encourage improved performance. This new people, of which 97% were related to institutions
mechanism considers a set of objectives that are used to providing primary and hospital care and 3% to central
make comparisons of performance among the hospitals and regional technical and administrative services.
of the NHS, organized in benchmarking groups, focusing Nurses are the professional group in healthcare with
on the areas of access, quality and efficiency. the largest number of workers, accounting for about
one-third of all Ministry of Health (MoH) workers
Hospitals are reimbursed for the comprehensive
(38 089), although numbers are low when compared
treatment provided to patients for several chronic
to international standards. The next largest group is
diseases: HIV infection, multiple sclerosis, pulmonary
medical staff (26 645, 22%), followed by operational
hypertension, different lysosomal storage diseases,
assistants (24 600, 20%). In the case of medical doctors,
familial amyloid polyneuropathy and selected
about 67% are specialists and 33% interns.
oncological diseases (i.e. breast cancer, cervical cancer,
colo-rectal cancer). The price for the comprehensive
treatment was based on the clinical guidelines for each
disease. It includes medicines, consultation, medical
tests, etc. The aim was to make providers familiar with
the guidelines and quality of care (Lourenço, 2016a).
The independent assessment for the HIV / AIDS showed
positive results.
17Health System Review
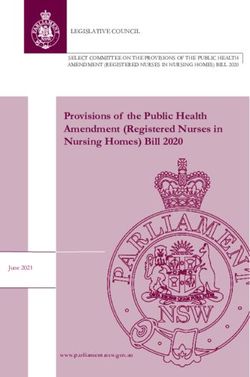
Figure 13. Doctors / nurses ratio in Portugal
EU average: 3.6
20
Practising nurses per 1 000 population, 2015 (or nearest year)
Doctors Low Doctors High
Nurses High Nurses High
DK
15
FI
DE
IE LU
NL SE
10 BE
SI FR EU average: 8.4
EU
UK MT AT
CZ LT
HU EE
RO IT Portugal
PL
HR
5
LV ES BG
SK
CY EL
Doctors Low Doctors High
Nurses Low Nurses Low
0
1 2 3 4 5 6 7
Practising doctors per 1 000 population, 2015 (or nearest year)
Note: In Portugal and Greece, data refer to all doctors licensed to practice, resulting in a large over-estimation of the number of
practising
Source: OECD doctors
/ European (e.g. ofon
Observatory around
Health30% in Portugal).
Systems In (2017).
and Policies Austria and Greece, the number of nurses is under-estimated as it only
includes those working in hospital.
Note: In Portugal and Greece, data refer to all doctors licensed to practice,
Source:
resulting in Eurostat Database.
a large over-estimation of the number of practising doctors (e.g. of
around 30% in Portugal). In Austria and Greece, the number of nurses is under-
estimated as it only includes those working in hospital.
The emigration of Portuguese health professionals is
In the period 2002 – 2013, the number of registered also stimulated by the difficulty for recently graduated
nurses increased continuously, with a total increase of nurses, dentists and diagnostic and therapeutic
about 24,000 professionals. This increase was equally technicians to find employment, the low salaries
strong for both women and men (an increase of offered in both the public and private sectors, heavy
58% for women and 56% for men compared to the workloads, remuneration not being performance-related
base year). The ratio of nurses per 1,000 population and limited career prospects. Further, the dynamics
increased from 4.0 in 2002 to 6.3 in 2013. The number of medical school graduates and the retirement of
of doctors per thousand inhabitants also increased Medical Doctors will generate a surplus that may
in the same period, from 3.2 to 4.3. In 2014 the role not be absorbed by the healthcare system by 2025
of family nurse was created (Decree-Law 118/2014). (Santana, 2014).
From 2009 until 2015, the nurses Council estimates that
12.500 nurses emigrated (Pereira, 2015). The occurrence of the burnout syndrome in Portuguese
health professionals is frequent, being associated with
Three quarters of nurses work in acute settings and a the perception of poor working conditions and reduced
quarter in the community. A further shift to community professional experience. The incidence of the burnout
settings will be needed if chronic diseases are to be syndrome shows regional differences which may be
effectively managed outside of hospitals. associated with different and suboptimal conditions
The distribution of health resources does not match for health care delivery. At the national level, between
population characteristics. There is no correlation 2011 and 2013, 21.6% of health professionals presented
between variables such as total number of physicians, moderate burnout and 47.8% burnout. The perception
nurses, hospital beds, primary care units, and the ageing of poor working conditions was the main predictor
index. Municipalities with a higher ageing index do not of the occurrence of burnout in Portuguese health
get more resources, resulting in more limited access professionals (Marôco, 2016). Promoting retention
to health care from those populations. Rural areas, strategies that increase satisfaction with opportunities
especially interior areas with low density of population for career advancement among Portuguese nurses
(and in many cases declining populations) are poorly has the potential to override individual characteristics
provided with skilled human resources (Simões, 2017). associated with increased turnover intentions
(Leone, 2015).
18Domain 2: NHS sectorial reforms and human resources
An improved strategy for staff retention and motivation • reduction in the medium term in the number of
is needed. (Ribeiro, 2014). Promoting retention strategies people with functional dependency – adoption of
that increase satisfaction with opportunities for career the strategy for active and healthy aging (already
advancement among Portuguese nurses has the submitted).
potential to override individual characteristics associated
with increased turnover intentions (Leone, 2015). Several initiatives of decentralization and autonomy
in the health system have occurred recently. Examples
The discussion about skill mix in the NHS only
include the change in the status of several NHS
emerged recently. Despite, the exceptional training and
hospitals to public enterprises, and the creation of
qualifications of several health professions, the health
Responsibility Centres, which increased the degree
system continues to be focused on physicians. As
of autonomy in the day-to-day decision-making
an example, the recent created role of Family Nurses
of organizations and services, especially in terms of
requires more government measures (Simões et al.
acquisitions and recruitment. The XXI constitutional
2017).
Government introduced the principle of free access
and circulation (FAC) for users in the SNS (Order No.
2.6 Digital transformation
5911-B/2016). With the implementation of FAC, the
The development of eHealth in Portugal over the years patient who needs a specialty hospital consultation,
was an important tool to improve governance, and the may, together with the family physician responsible
availability of data is now much better than a decade for the referral, opt for any of the NHS hospital units
ago. Nevertheless, the available data are not always where the specialty in question exists. Before, there
used to improve process and results. The eHealth was a network of pre-defined hospitals for referral
market started in the late 80s and it has been evolving from primary care, based on the place of residence.
since then. Sometimes this is more market driven In principle this measure might increase efficiency and
and other times more centralized in public providers. equity in the NHS. Simultaneously, the NHS started to
However, it is clear that Portugal is now in the forefront release more information about waiting times. The
of eHealth in Europe. All the primary health care most recent estimates show that approximately 12%
providers have electronic health records, most hospitals of referred patients chose another hospital than the
have electronic health records, there is already some one previously assigned.
interoperability between different software.
Key challenges – the way forward
Selected past and ongoing efforts
1. F uture initiatives should take into consideration the
Current priorities for the primary health care reform may balance between the central functions of policy
be summarized as follows: guidance and monitoring; and the autonomy of
delivery health care organizations. The decrease in
• Enhancing primary health care response, by gradually
autonomy and the centralization of decision-making
strengthening their professional capacity in areas
diminishes the capacity to find solutions adapted to
such as oral health, psychology and nutrition and
the different organizations, and their unique contexts.
improving acute care management;
Therefore, the decentralization of functions in the NHS,
• Implementing a new contacting model for the from central services to hierarchically inferior levels,
primary health care functional units, more adapted namely for regional health administrations, hospitals
to respond to the current need to improve primary and health centre groups should be discussed in
health care performance; order to optimize (Gulbenkian, 2015). Recognising
that some of the recent centralisation was a response
• Improving the culture and tools for better health and
to external pressures, it is necessary to define more
clinical governance in primary health care, taking
clearly what roles are useful at the regional level and
advantage of further developments of the Business
to develop the structures and systems to allow these
Intelligence system now taking place.
roles to be developed.
The following developments are taking place in the 2. There is a need to improve the current pace of the
Portuguese long-term care network: primary health care reform, in order to provide similar
quality of care to the entire Portuguese population as
• increase of responses in extension and diversity –
soon as possible. Also, the integration of primary care
a strategy of increasing the number of responses,
network with other levels of care remains a challenge,
with priority for home care, is underway. The diversity
requiring measures to improve the continuum of
of responses to areas that lack some specificity
care and the efficiency of the health system (see also
(strategy for the care of people with dementia –
Domain 3).
already delivered) is being prepared;
3. An approach is needed to implement policy –
• greater integration of the Network with social
currently there remains a large gap between some
responses – although the current response is already
clear policy directions and the mechanisms for
integrated, this needs to be deepened, namely with
implementing policy and managing change.
multiple social responses such as home support
services and residential structures for the elderly;
19Health System Review
4. T here is a need to clarify the policy goals in the
interface of public and private provision, and to
integrate the different sectors more effectively.
5. S ystematic evaluation and review of service
delivery models will be useful and timely. Gaining
full advantage of these new models may require
more autonomy of providers and will have some
implications for local and national governance
arrangements and their balance. It is likely that the
best options will involve further moves to integrate
care provision and to simplify the ways in which
people access care.
6. Despite significant changes in skill mix, service
provision in Portugal remains very doctor centred,
and there is a need for a wider set of skills and a
better configuration of professionals to meet the
growing needs of people with multiple and complex
chronic diseases.
7. In line with most European Union countries, human
resource policy making and planning for service
provision and management needs to be placed clearly
ahead of the needs curve.
8. T here is also a need to reduce outward migration of
health care professionals and to examine in particular
the incentives for retention and motivation of staff.
While it can be difficult to compete on salaries with
some other employers, the wider working conditions
are important for motivation.
9. P ortugal can be proud of progress in terms of the use
of information and communications technologies in
the health sector. This provides a good basis both for
more efficient operation of the system and also to
further develop the role of patients and families. It is
important to retain the focus on these developments
as drivers and facilitators of better service delivery
and to make the best use of the potential for wider
use of the data in research, monitoring, quality
assurance and service development.
20Domain 3: Person-centred, better integrated NHS
DOMAIN 3: PERSON-CENTRED, BETTER INTEGRATED NHS
3.1 Healthcare integration Although there are still challenges to be addressed
regarding the success of vertical integration, recent
The European Commission stresses that it is necessary
studies suggest that quality indicators such as
to offer alternative care models to improve quality of
readmissions decreased after a vertical integration,
life, health care and reduce avoidable hospitalizations
especially among patients with diabetes and
and costs. The integrated care model should be based
complications (Lopes et al. 2017). Even though
on better coordination among health and social care
improvements were not found for all institutions or
professionals, higher efficiency, improved healthcare
condition-specific groups, this study shows that merging
processes, supported by information technology (IT)
acute and primary care providers is associated with
and new organizational models and use of technologies
reduced readmissions (Lopes et al. 2017). Vertical
for remote care (e.g. at home or at work).
integration, in organizational terms, between primary
Care integration can be achieved with appropriate and hospital care, was introduced in 1996, as Local
structures and appropriate care integration and Health Units (ULS in Portuguese), covering only a
procurement tools. There has been some innovation geographical areas in the NHS. Since than a number of
in contracting and procurement in Portugal (Simões projects, within and outside ULS, aiming at improving
et al., 2017) that has provided experience in the use of health care integration, have been implemented in
financing mechanisms that might be used as incentives Portugal. These projects focus on different aspects of
for integration of care delivery, alongside the experience health care integration, including case-management of
of integration of primary and secondary care delivery. highly complex patients, tele-communication between
In Portugal, the integration experiences of health care, hospital and primary health care settings, more
particularly between primary health care (PHC) and sophisticated referral systems between different levels
secondary care already exist, but little is known about of care, home care follow-up of post hospitalization.
the effectiveness of these models in improving care Interventions that include experts focused on discharge
delivery. This issue thus becomes important, not only management, that include post-discharge rehabilitation
because it is relevant to assess if significant efforts to and follow-up and those based on multicomponent
integrate care have been made in Portugal but also strategies were most likely to be associated with
because there is a particular experience of integration significant reductions in hospital use for patients with
of PHC and secondary care which requires a deeper single conditions such as heart failure and chronic
knowledge, specifically the model of local health unit obstructive pulmonary disease (COPD).
(ULS in Portuguese). Still on the issue of evaluation, and
especially the evaluation of health care integration, there Remote monitoring of patients with COPD
is still a need for better methodologies and metrics
One of the main objectives in the treatment of COPD
for measuring the integration of care and there is also
is the prevention of hospital readmissions, as well as
a lack of consensus on the terminology and on the
the improvement of survival. This program was already
concepts related to the integration of care.
ongoing and this specific payment mechanism was
applied in 2017, following a pre-established home
protocol, according to the inclusion criteria and the
objectives defined. Portugal has the second lowest
asthma and COPD admissions in adults among EU21.
21Health System Review
Telemonitoring program for status after acute Figure 15. Health literacy levels by age and
myocardial infarction educational levels
The 30 day mortality after admission to hospital
for acute myocardial infarction (AMI) in Portugal is 0% 20% 40% 60% 80% 100%
slightly higher than the EU21 average. Appropriate 15-25 years 12.7% 53.6% 30.9% 2.7%
treatment and follow-up of AMI also reduces avoidable 26-35 years 11.8% 52.0% 32.4% 3.8%
readmissions and hospital stays, as well as improves
36-45 years 11.8% 47.0% 34.9% 6.3%
patient survival. In these terms, a 2014 Telemonitoring
46-55 years 45.2%
Program for status after acute myocardial infarction 7.0% 40.2% 7.6%
was developed. There are also implemented “vias 56-65 years 3.8% 41.9% 39.7% 14.7%
verdes coronárias” that is a pathway for faster access 66-75 years 6.4% 28.2% 42.9% 22.6%
to hospitals with primary angioplasty. 76+ years 2.3% 16.0% 46.6% 35.1%
0% 20% 40% 60% 80% 100%
3.2 Health literacy
Up to
Basic 2 2.0% 32.9% 44.7% 20.4%
When health literacy is compared across different
European countries, Portugal appears in a less Basic 3 8.3% 48.9% 37.1% 5.7%
favourable position (Figure 14).
Secondary
14.4% 49.6% 33.6% 2.4%
education
Figure 14. Comparing health literacy across Tertiary
selected European countries education 18.7% 48.5% 27.2% 5.6%
■ Excellent HL ■ Sufficient HL ■ Problematic HL ■ Inadequate HL
Portugal 8.4% 30.1% 44.4% 17.0% Source: ILS-PT, 2014, CIES-IUL/ Fundação Calouste Gulbenkian e HLS-EU Consortium (2012)
Source: ILS-PT, 2014, CIES-IUL / Fundação Calouste Gulbenkian e HLS-EU
Poland 19.5% 35.9% 34.4% 10.2%
Consortium (2012).
Netherlands 25.1% 46.3% 26.9% 1.8%
Ireland 21.3% 38.7% 29.7% 10.3%
Spain 9.1% 32.6% 50.8% 7.5%
Selected recent or ongoing developments
Greece 15.6% 39.6% 30.9% 13.9%
Since 2016 new developments are taking place in
Germany 19.6% 34.1% 35.3% 11.0%
Portugal concerning people centeredness and better
Bulgaria 11.3% 26.6% 35.2% 26.9%
health care integration. These can be summarized
Austria 9.9% 33.7% 38.2% 18.2%
as follows:
Total 15.5% 35.3% 36.2% 13.0%
0% 10% 20% 30% 40% 50% 60% 70%
Levels of health literacy by country and by total
80% 90% 100%
NHS Portal
■ Excellent ■ Sufficient ■ Problematic ■ Inadequate
In 2016, the new government launched the NHS portal,
with information mainly targeted for the user (3 million
Source: Pedro, Amarel & Escoval, 2016.
views in 1 year) aiming at better governance on the
basis of enhanced communication, transparency and
However two distinct groups can be identified in
accountability on health and health care. Users can
Portugal when it comes to health literacy: elderly
enrol into the “personal area” of the Portal in order to
people with lower education, and a highly educated
organize and manage their own health information and
young population. These two groups need different
receive relevant health information or take advantage
strategies as a health literacy target, (elderly people with
of more general information continuously updated, as
lower incomes and educational resources are the most
for instance waiting times in the emergency department
vulnerable group) in the use of health information in
and for surgeries. Mobile applications, linked to Portal’s
their daily routines. Figure 15 shows health literacy levels
information have developed.
by age and education levels.
Since early 2017 the Portal offers a health literacy
library and a new collection of thematic microsites
presented as attractive digital books, covering areas
such as “Preventing Falls”, “Healthy Eating Habits”,
“Winter Health”, “Positive Personal Relationships, Violent
Behaviours and Health”. Although details on the Portal’s
overall performance are not yet available, this is a step
towards more informed and active users.
22You can also read