2020-21 PRE-BUDGET SUBMISSION QUEENSLAND - PSA
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

2020–21 PRE-BUDGET SUBMISSION QUEENSLAND

Submitted by: Contact:
Pharmaceutical Society of Australia Mark Lock
Level 2, 225 Montague Road State Manager – Qld
West End QLD 4101 Pharmaceutical Society of Australia
PO Box 6120 mark.lock@psa.org.au
Woolloongabba QLD 4102 0406 609 671
E: qld.branch@psa.org.au Level 2, 225 Montague Road
www.psa.org.au West End QLD 4101
FRONT COVER: Luke Vrankovich MPS Community pharmacist,
Townsville Qld
© Pharmaceutical Society of Australia Ltd., 2020
This submission contains material that has been provided by the
Pharmaceutical Society of Australia (PSA). Requests to use PSA
material should be addressed to: Pharmaceutical Society of Australia,
PO Box 42, Deakin West ACT 2600.
2 | 2020–21 Pre-budget submission – Queensland
CONTENTS
About PSA 4
Pharmacists in Queensland 4
Executive Summary 5
Recommendation one 6
Improve access to vaccinations to protect more Queenslanders
Recommendation two 11
Remove barriers to allow pharmacists to supply standard manufacturer pack size of medicines in
emergency and disaster situations
Recommendation three 13
Provide funding to employ pharmacists in state-operated residential aged care facilities
Recommendation four 16
Establish the role of Queensland Chief Pharmacist
Recommendation five 18
Facilitate and fund emergency presentations manageable by community pharmacists
Appendix I 21
Experience of a Queensland pharmacist following floods
Appendix II 22
Importance of effective emergency supply provisions for Prescription
Only Medicines in disasters
Appendix III 30
Role of a Residential Aged Care Facility Pharmacist33
2020–21 Pre-budget submission – Queensland | 3
About PSA
PSA is the only Australian Government-recognised PSA has a strong and engaged membership base
peak national professional pharmacy organisation that provides high-quality healthcare and are the
representing all of Australia’s 31,000 pharmacists custodians for safe and effective medicine use for
working in all sectors and across all locations. the Australian community.
PSA is committed to supporting pharmacists PSA leads and supports innovative and evidence-
in helping Australians to access quality, safe, based healthcare service delivery by pharmacists.
equitable, efficient and effective healthcare. PSA PSA provides high-quality practitioner
believes the expertise of pharmacists can be development and practice support to pharmacists
better utilised to address the healthcare needs of and is the custodian of the professional practice
all Australians. standards and guidelines to ensure quality and
integrity in the practice of pharmacy.
PSA works to identify, unlock and advance
opportunities for pharmacists to realise their full
potential, to be appropriately recognised and
fairly remunerated.
Pharmacists
in Queensland
6,370
Registered pharmacists working in
community pharmacies, hospital, general
practice, aged care, state and federal
government and within other private
sector organisations and as consultant
pharmacists.
Courtney McMahon MPS Community pharmacist, Biloela Qld
4 | 2020–21 Pre-budget submission – QueenslandExecutive Summary
Medicines are the most common intervention This pre-budget submission identifies five key
in health care1. Concerningly, problems with the areas for consideration as part of the 2020/2021
use of medicines is also alarmingly common. In Financial Year Queensland Government Budget.
Australia, 250,000 hospital admission a year are a The PSA seeks to work in partnership with the
result of medicine-related problems. The annual Queensland Government to achieve mutually
cost of these admissions is $1.4 billion, and 50% beneficial goals of improving safe access to
of this harm is preventable.2 This burden of harm medicines and health care for all Queenslanders in
is felt in Queensland just like it is throughout enabling better health outcomes.
Australia.
In light of this, the Pharmaceutical Society of
Australia recommends five areas of action:
1
Improve access to vaccinations to protect more Queenslanders against
preventable infectious diseases
PSA calls for regulatory change in Queensland to:
• lower the age of pharmacist-administered vaccines to persons 10 years and over
• increase the range of vaccines pharmacists can administer
• allow consumers to access pharmacist vaccination in more locations, and
• allow consumers access to NIP and state-funded program vaccines when receiving
pharmacist-administered vaccinations.
2
Remove barriers to improve access to medicines in emergency and disaster
situations
PSA calls for regulatory change in Queensland to enable pharmacists to supply a
standard manufacturer pack size of medicines for emergency and disaster situations as
opposed to the current 3-day supply provision.
3
Provide funding to employ pharmacists in state-operated residential aged care
facilities
PSA calls on the Queensland Government to provide funding to employ pharmacists in
state-operated residential aged care facilities to improve the Quality Use of Medicines
and to reduce the harm caused by overuse of psychotropic medicines, opioids and
antibiotics.
4
Establish the role of Queensland Chief Pharmacist
PSA calls on the Queensland Government to allocate ongoing funding annually to
improve coordination of health policy and regulatory controls by establishing the role of
Queensland Chief Pharmacist.
5
Facilitate and fund emergency presentations manageable by community pharmacists
PSA calls on the Queensland Government to allocate $26.45 million in funding over
4 years for the management of non-urgent or low-urgency medical conditions through
community pharmacy.
Chris Campbell
Pharmaceutical Society of Australia
Queensland President
2020–21 Pre-budget submission – Queensland | 5Recommendation One
Improve access to vaccinations to protect
more Queenslanders
The challenge The barriers
Immunisation is one of the most effective Organising to get to an immunisation provider for
disease prevention methods. Vaccines are safe, a vaccination, especially for parents with children
efficacious and easy for competently trained aged between 10 and 16 years, can often be a
health professionals to administer. They provide difficult exercise. For this reason other states have
protection against both health and economic looked at giving parents more opportunities to
impacts of epidemics of vaccine-preventable get their children vaccinated by pharmacists so
infectious diseases.3,4 more people are protected against potentially
fatal diseases.
In 2019, Queensland had a record breaking
flu season with more than 68,000 influenza In 2019, both Western Australia and Tasmania
notifications and more than 3,000 hospitalisations, reduced the age of influenza vaccination that
an increase from the previous record of 56,000 in trained pharmacists are able to administer to 10
2017.5 There was also a large increase in measles years of age and over in order to ensure everyone
cases in 2019, with 74 cases recorded up from 14 had the maximum opportunity to get themselves
in 2018 and 8 in 2017.5 vaccinated.9 The Victorian Government have
announced this change will occur in Victoria in
Less than 40% of at-risk adults are considered
time for the 2020 influenza season. These changes
to be fully vaccinated.3 This includes healthcare
will allow more people to get vaccinated more
workers and those caring for our most vulnerable
easily in those states and reduce the burden of
people in Queensland, including children, the
disease.
ill, elderly and infirm. For example, less than
50% of childcare workers are fully vaccinated6 In addition to accessing vaccination providers for
and seasonal influenza vaccination uptake is immunisations, access to funded vaccines is the
inconsistent in aged care and health care workers.7 main barrier to uptake of vaccination by non-
To protect the Queensland community, it is crucial immunising parents which may relate to social
that those who have a higher risk of exposure to disadvantage and logistical barriers10. Amongst
contracting and spreading infectious diseases are health care workers in Australia, awareness, cost,
fully vaccinated including adolescents. and convenience have been identified as key
barriers to vaccination with data suggesting that
In addition, Queensland is a popular tourist
raising awareness of the benefits of influenza
destination attracting 2.8 million international and
vaccination, along with improving access to
7.8 million interstate travellers annually.8 With that
affordable, convenient vaccination are likely to
comes the risk of vaccine-preventable diseases
improve uptake.11
entering the state from unvaccinated travellers.
This amplifies the importance of ensuring that as While consumers are relatively aware of access to
many Queenslanders as possible are vaccinated influenza vaccination by pharmacists, this likely
against these diseases to ensure our health and does not extend to other vaccinations such as
wellbeing. pertussis and MMR, resulting in low awareness
being a barrier to consumer access.
Removing barriers to vaccination is essential
to achieving herd immunity and protecting
Queenslanders against vaccine-preventable
diseases.
6 | 2020–21 Pre-budget submission – QueenslandThe state’s obligations as part of the National
Box 1: PSA’s proposed list of vaccines able
Partnership Agreement on Essential Vaccines
to be administered by trained Queensland
(NPEV) is to purchase and distribute vaccines to
pharmacists
immunisation providers, manage the efficient and
effective delivery of the immunisation program • Influenza (including enhanced vaccines
and monitor and minimise vaccine wastage.12 for over 65’s)*
• Measles, mumps, rubella*
Currently in Queensland, pharmacist vaccinators
are unable to administer National Immunisation • Diphtheria, tetanus and pertussis*
Program (NIP) or state-funded vaccines to eligible • Meningococcal ACWY
Queenslanders. This means that some consumers • Meningococcal B
may choose to pay out-of-pocket privately to get • Hepatitis A
vaccinated, or may choose not to get vaccinated
• Hepatitis B
when access to a GP or other vaccination provider
is not convenient. • Human papillomavirus
• Pneumococcal
The proposed approach • Poliomyelitis
PSA recommends expanding vaccination services • Varicella
provided by trained pharmacist vaccinators in the • Zoster
following four ways: • Rabies
• Recommendation 1A (vaccine range): • Typhoid
allow pharmacist vaccinators in Queensland • Cholera
to administer all vaccines to persons aged * Currently able to be administered by pharmacists, but
subject to restrictions .
10 years and older in accordance with the
Immunisation Schedule Queensland.
• Recommendation 1B (vaccine funding): These vaccines would be funded privately by
allow pharmacist vaccinators in Queensland to consumers or workplaces, or through the National
access National Immunisation Program (NIP) Immunisation Program (NIP) or state-funded
and state-funded vaccine stock to administer programs, depending on individual eligibility.
to eligible persons aged 10 years and older to PSA also considers Queenslanders would benefit
allow consumers equal access to government- from integration of information regarding access
funded vaccines regardless of which authorised to vaccination within existing and future state
vaccinator they choose. public health campaigns which highlight the
• Recommendation 1C (travel vaccines): benefits of vaccination to their health. These
allow pharmacist vaccinators in Queensland public health campaigns should promote all
to administer low-risk travel vaccinations as vaccination providers, including pharmacists, as
recommended by the Queensland Parliament health professionals where consumers can seek to
HCDSDFVP Committee’s Report No 12 of the get vaccinated in convenient and affordable ways.
56th Parliament.
• Recommendation 1D (vaccination
Why it will work
location): remove barriers on where Pharmacists have been vaccinating in the state of
pharmacists can administer vaccines in Queensland since April 2014 when Queensland
Queensland in line with other immunisation led the way for pharmacist-administered
providers in the state. vaccinations with the Queensland Pharmacist
Immunisation Pilot (QPIP) Phase I trial. This led
The above proposals would allow any eligible
to pharmacists across Australia administering
Queenslander aged 10 years and above access
vaccinations in all other States and Territories by
to vaccines listed in Box 1 from a pharmacist
2016.
vaccinator in Queensland regardless of location
and reduce the burden of vaccine-preventable
diseases in Queensland:
2020–21 Pre-budget submission – Queensland | 7The accessibility of community pharmacists Evaluation of the Victorian pharmacist
(through a well-established network of administered vaccination program indicated
community pharmacies and extended operating that between June 2016 to September 2017,
hours) and consumer trust has provided an 47,525 Victorians were administered influenza
accessible and convenient location for the delivery and pertussis-containing vaccines and 10,420
of vaccination services. The pharmacist workforce Victorians received the vaccine for the first time.16
has been acknowledged as contributing to a
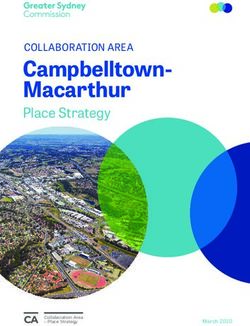
Ninety-six per cent of consumers reported they
meaningful reduction in the severity of seasonal
were ‘very satisfied’ or ‘extremely satisfied’ with the
influenza13 in particular.
pharmacist-administered vaccinations received16
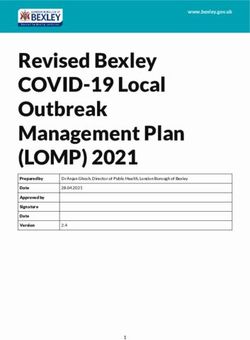
Pharmacists in other countries have also been (see Figure 2).
shown to safely administer various vaccinations,14
The evaluation results suggest the program had an
as summarised in Figure 1.
impact on reducing and avoiding disease burden
Research indicates the introduction of funded associated with influenza and pertussis. With
programs increases vaccination coverage.15 further expansion in the number of participating
Consumers already have access to NIP and pharmacies and number of trained pharmacists, it
government-funded vaccines in other Australian is anticipated this impact will continue to increase.
jurisdictions: In addition, consumers benefited from an increase
in access to these vaccination services, a reduction
Victoria
in wait time and for some patients, a smaller fee.16
Pharmacist vaccinators can administer
Western Australia
government-funded vaccines under the NIP,
Victorian Government’s Partner Whooping Cough WA Health provides NIP-funded influenza
Vaccine Program and Measles-Mumps-Rubella vaccines to community pharmacies, including
Adult Vaccine Program to eligible individuals 16 the enhanced vaccine for those aged 65 and over.
years of age and over.
Australia (other)
South Africa
Queensland
Switzerland
Argentina
Portugal
Canada*
USA*
UK
Influenza ü ü ü ü ü ü ü ü ü
Pertussis, ü& ü& ü ü ü ü û ü ü
diphtheria,
tetanus
MMR ü ü% ü ? û ü ü ü ü
Meningococcal û ü(WA ? ? ü ü û ü ü
only)
Hepatitis A û û ü ü ü ü ü ü ü
Hepatitis B û û ü ü ü ü ü ü ü
Varicella û û ? ü ü ü û ü ü
* denotes jurisdictional variation
% All except ACT
& only for purpose of pertussis immunity (most states)
? no data
Figure 1: Vaccines able to be administered by pharmacists – international comparison14
8 | 2020–21 Pre-budget submission – QueenslandThe program has improved access for thousands Australian Capital Territory
of West Australians, particularly those who live
ACT Health provide NIP-funded influenza vaccines
without GP services or in rural remote areas in
to participating ACT pharmacies as part of a pilot
single pharmacy towns.
program.
Figure 2: HealthConsult evaluation of the Victorian pharmacist-administered vaccination program consumer
survey 201716
BENEFITS TO QUEENSLANDERS
• Increased access to vaccinations by more Queenslanders to reduce and avoid disease burden
associated with vaccine-preventable diseases
• Improve efficient use of vaccines for the NIP and state-funded vaccination programs
• Increases uptake of vaccinations by a younger susceptible group, providing greater protection
to the community
• Slows the spread of outbreaks of vaccine-preventable diseases in schools
• Increases uptake of recommended vaccinations by health and carer workforce, providing
greater protection to the vulnerable Queenslanders they care for
• Increases access for immunisation services especially in rural and remote areas
• Reduced wait time for patients to access vaccinations
• Reduced out-of-pocket cost to access vaccination for some patients
2020–21 Pre-budget submission – Queensland | 9Timeline PSA calls on the Queensland
• Recommendation 1A, 1C Government to expand pharmacist-
and 1D: Implementing these administered vaccination services by:
recommendations is a matter of
regulatory change without any • Allowing Queenslanders aged
additional funding requirements 10 years and older to access all
to train the workforce or build vaccinations from a pharmacist
infrastructure.
vaccinator
• Recommendation 1B: Achieving
this recommendation is a matter
• Allowing people who are
of redistribution of a portion vaccinated by a pharmacist
of current NIP and state- access to National Immunisation
funded vaccines to community Program (NIP) and state-funded
pharmacies.
vaccine stock
As trained pharmacist immunisers
already have the skills and • Allow Queenslanders to access
infrastructure to provide these low-risk travel vaccinations from
services, this could be implemented pharmacist vaccinators
immediately following changes to the
Queensland regulations. • Remove barriers on where
pharmacists can administer
Cost
vaccines in Queensland in
• Recommendation 1A, 1C and 1D:
Nil direct cost. Cost savings may
line with other immunisation
be achieved through reduced providers in the state.
hospital admissions caused by
vaccine-preventable disease-
related complications.
• Recommendation 1B: Based
on the level of redistribution, a
small investment (estimated to
be $300,000) will be incurred
in planning and deployment
of vaccine stock to community
pharmacies in Queensland.
Incorporation of messaging regarding
access to vaccination services by
a pharmacist would not require
additional funding to public health
campaigns.
Rachel Dal Zilio MPS Community pharmacist, Pomona Qld
10 | 2020–21 Pre-budget submission – QueenslandRecommendation Two
Remove barriers to allow pharmacists to
supply standard manufacturer pack size
of medicines in emergency and disaster
situations
The challenge In addition to the challenges that exist in rural
and remote locations, Queensland’s extensive
Queensland is the most decentralised state in
history of natural disasters such as cyclones,
Australia, which means a large proportion of the
floods and bushfires has demonstrated the barrier
population is living in regional, rural and remote
this provision represents to providing access
locations of the state. Many barriers exist which
to essential ongoing medicines to consumers
may prevent patients from accessing the same
following a crisis event, such as being displaced by
level of health care as their urban counterparts.
an emergency (See flood example: Appendix I).
Australians living in rural and remote areas have
a higher prevalence of chronic health conditions The proposed approach
and are less likely than those living in cities to have
PSA proposes an expansion of existing provisions
a regular GP.17 Australians living in these rural and
which allow for Continued Dispensing and
remote areas frequently report there were times
emergency supply in Queensland to allow
they needed to see a GP, but could not because
ongoing supply of life-saving and illness-
there was no GP available nearby.17
preventing medicines. This expansion would
Evidence provided at the Queensland Parliament provide flexibility to supply greater quantities
public hearings on the recent Inquiry into the and a larger range of medicines through revision
establishment of a pharmacy council and transfer to existing emergency supply and continued
of pharmacy ownership in Queensland18, indicated dispensing arrangements.
that in rural areas patients are unable to access
PSA proposes that the Queensland Government
prescribers in short time frames due to distance
amend regulations to allow pharmacists to supply
and waiting times for consultation.
a standard manufacturer’s pack size of medicines
These challenges can make access to prescriptions in emergency and disaster situations in order to
and medicines difficult and can have negative ensure continuity of patient care.
impacts on the health of Queenslanders. This
is particularly important for patients who have Why it will work
chronic conditions, those who are at risk of low
Currently in Queensland, pharmacists can supply
adherence, patients who are already stabilised on
a PBS quantity (in most cases a manufacturer’s
their medicines, and medicines that require dose
pack size) of PBS listed oral contraceptive pill and
titration.
specific cholesterol lowering medicines (HMG CoA
reductase inhibitors) in an emergency situation
The barriers
as outlined in the National Health (Continued
Current regulation in Queensland allows Dispensing) Determination 2012 (Cwlth). This
pharmacists to supply up to 3 days’ supply of provision is governed by professional practice
most Prescription Only Medicines (Schedule 4) in standards and has been uncontroversial since
emergency circumstances which in most cases is its implementation. For most other medicines,
inadequate for continuity of patient care in many current regulations in Queensland only allow a
situations. This supply is not eligible for PBS subsidy. pharmacist to dispense a maximum of 3 days’
2020–21 Pre-budget submission – Queensland | 11supply of medication which is inadequate in most,
PSA calls on the Queensland
if not all situations to ensure continuity of care.
Government to amend emergency
PSA’s proposal represents a logical extension of
supply provisions of Queensland
these provisions which will help ensure patients
have proper access to their regular essential
regulations to allow pharmacists to
medicines in a timely manner. supply a standard manufacturer pack
In response to the bushfire crisis this summer, size of medicines.
the NSW, Victorian, South Australian and the
ACT governments successfully implemented the
expansion of continued dispensing provisions BENEFITS TO
during the bushfire period (See example – QUEENSLANDERS
Appendix II).
• Improved access to life-saving and illness-
preventing medicines during emergency
Timeline situations
1 July 2020.
• Reduced burden on patients trying to
This proposal is a matter of regulatory
access medicines in emergency situations
change and can be implemented
immediately following the revision to • Reduced burden on patients trying to
the relevant Queensland regulations. access medicines in rural and remote
areas when a GP is not accessible
Budget • Improved health outcomes of patients
through continuity of medicine supply
Nil direct investment required.
12 | 2020–21 Pre-budget submission – QueenslandRecommendation Three
Provide funding to employ pharmacists
in state-operated residential aged care
facilities
The challenge The Australian and New Zealand Society for
Geriatric Medicine (ANZSGM) ‘Prescribing in Older
Australia’s population is aging, and currently
People’ position statement recognises the role of
3.8 million people or 15% of the total population
‘clinical pharmacy services’ including medication
are aged 65 or over.19 With this growth in the aging
reviews as part of a targeted approach to identify
population, more and more older Australians are
and manage polypharmacy.22
entering residential care services.20 The health of
older people can be complicated by the presence The knowledge and expertise of pharmacists is
of many chronic conditions, and the subsequent essential in the unique situations presented in
need to take multiple medications. The care and residential aged care facilities. Many older people
medication management of aged care residents have multiple chronic health conditions and this
are becoming more and more complex, as people has a number of potential consequences.
are older and more frail when they enter aged care • Older people may be prescribed multiple
facilities.20 medicines (polypharmacy), resulting in a
While the need to treat multiple conditions significant increase in the potential for adverse
is recognised, the risk of adverse drug events effects and drug interactions.
increases with the number of medications • Many age-associated health conditions
prescribed. When this risk is combined with the can modify the pharmacokinetic and
age-related changes in how medications act, and pharmacodynamics properties of a medicine,
are cleared from the body, it leads to medication- increasing the variability in response to
related problems being commonly reported in medicines.
older people. Therefore, medication management
• More than one medicine is often needed
services play a paramount role in supporting the
to manage each health condition. As more
safe and effective use of medicines for those living
medicines are added to the medication
in residential care facilities.21
regimen, the increased ‘pill burden’ increases
PSA’s Medicine Safety: Take Care report released the risk of poor adherence, confusion and
in 2019 revealed that 98% of residents in aged- adverse effects.23
care facilities have at least one medication-related
Queensland Health operates sixteen residential
problem and that as many as 80% are prescribed
aged care facilities which would likely experience
potentially inappropriate medicines.2 The use of
the above challenges which exist throughout the
potentially inappropriate medicines in residents
aged care sector.
of aged-care facilities has been shown to increase
the risk of hospitalisation with the report revealing
that 17% of unplanned hospital admissions of
residents living in aged-care facilities taking
potentially inappropriate medicines are due to the
inappropriate medicine.
2020–21 Pre-budget submission – Queensland | 13The proposed approach The role complements the parallel roles of other
pharmacists involved in the care of residents in the
In order to achieve safe and best-possible use
community, hospital and general practice sector.
of medicines in residential aged care facilities,
pharmacists, with their unique knowledge and PSA recommends that in the 16 Queensland
medicines expertise, must have a greater role in Health operated aged care facilities, there should
the residential aged care sector. be 0.5 full-time equivalent (FTE) pharmacists
employed per 100 aged care residents in order to
PSA proposes incorporating a pharmacist on the
perform the recommended activities.
ground in Queensland Health operated residential
aged care facilities.
Why it will work
The non-dispensing role would include
In 2018, an ACT residential aged care facility was
undertaking comprehensive medication reviews,
the first in Australia to employ a pharmacist as part
identify and resolve multiple medicine related
of a 6 month trial. The study found that ‘including
problems and provide advice to prescribers,
a pharmacist in a residential aged care home can
nursing staff, carers and residents. It would also
improve medication administration practices by
enable greater communication and collaboration
reducing inappropriate dosage form modification
between members of the multidisciplinary team
and staff time spent on medication administration
involved in resident care.
rounds, and increasing the documentation of
PSA’s Pharmacists in 2023: For patients, for our resident allergies, adverse drug reactions and
profession, for Australia’s health system, the role medication incidents’26
of a pharmacist employed in an aged care facility
The role of the pharmacists employed within the
includes:24
aged care facility was well received by patients,
• Education and training of other health family members, care staff, doctors and other
professionals and facility staff in the quality use health care professionals involved in the care of
of medicines and medicines information; patients.
• Clinical governance activities around using
medicines appropriately including leading Timeline
programs and systems to reduce use of high From 1 July 2020
risk medicines such as antipsychotics and
benzodiazepines, and provide stewardship of
opioid and antimicrobial use; Budget
• Resident-level activities identifying, $900,000 annually to employ
preventing and managing medicine-related pharmacists in its sixteen Queensland
problems, reducing polypharmacy and Health operated residential aged care
optimising medicines use; and facilities.
• Supporting achievement of accreditation Cost savings may be achieved
standards related to medicine management. through reduced hospital admissions
due to medicine-related problems.
The role of aged care pharmacists is further
described in PSA’s Pharmacists in 2023: Roles and
Remuneration25, an excerpt of which is included in
Appendix III.
PSA calls on the Queensland
Government to invest $900,000
annually to employ pharmacists in
its 16 Queensland Health operated
residential aged care facilities
14 | 2020–21 Pre-budget submission – QueenslandBENEFITS TO QUEENSLANDERS
• Reduction in the use of psychotropic medicines/chemical restraints, improving the quality of life
for residents through reduced side effects (sedation, weight gain, impaired cognition etc)
• Reduction in hospitalisations from medicine-related adverse events
• More rational use of opioid medicines, resulting in improved pain management and alertness of
residents
• More rational and targeted use of antimicrobials in accordance with local resistance patterns
and treatment recommendations
• Increased staff access to pharmacist’s expertise in medicines and medication management
within the residential care facility
Dr Geraldine Moses AM FPS Drug Information Consultant Pharmacist, Brisbane Qld
2020–21 Pre-budget submission – Queensland | 15Recommendation Four
Establish the role of Queensland Chief
Pharmacist
The challenge The proposed approach
The Queensland health system provides support With the recent announcement by the
and advice to approximately 5.1 million people Commonwealth Health Minister the Hon Greg
but is challenged by a complex and fragmented Hunt to make Medicines Safety and the Quality
healthcare system. To deliver against key areas Use of Medicines Australia’s 10th National Health
of health policy requires engagement with Priority, PSA believes the Queensland Government
many state and federal stakeholders, often with should establish the role of Queensland Chief
conflicting and competing priorities. Added to Pharmacist.
this is the ever-changing landscape of medicines
This role would be employed within Queensland
and regulations in Australia, which require a
Health to support the Government’s coordination
collaborative and proactive approach to ensure
and implementation of policies relating to
health professionals and the public are kept aware
the prescribing, supply and administration of
of important updates.
medicines, as well as policy settings relevant to
This complexity is greater due to challenging the National Medicines Policy, Queensland Health
reform in areas such as primary health care, digital strategies and the pharmacy workforce.
health, preventive health, mental health and
This role, similar to roles of the Queensland’s Chief
chronic disease prevention. Pharmacists, being the
Health Officer, the Chief Nursing and Midwifery
most accessible health professional, are suitably
Officer and the Chief Allied Health Officer, would
equipped to support and progress these reforms
provide high-level advice on issues relating to the
consistent with governments’ objectives.
safe and quality use of medicines. The position
While the role of pharmacists in the logistical would serve as the Government’s principal
supply of medicines is well understood, the advisor on all matters related to the medicines,
risk mitigation and case management value of regulations and the National Medicines Policy. The
pharmacists in health care are often unrecognised. role would incorporate:
As the recognised peak body for pharmacists,
• Provision of high-level, high-calibre and
PSA plays a significant role in providing advice
independent advice on workforce and
on matters relating to pharmacists to the
workforce issues, pharmacist practice
Commonwealth and State Governments. However,
advice, actual and potential contribution of
there are no formal structures within Government
pharmacists to address existing and emerging
to provide independent ongoing expert advice
health priorities
on pharmacy and quality use of medicines
issues. Given the significance of the pharmacy • Clinical leadership across the Department
workforce and the need for improved quality use and sector to support the design, planning,
of medicines policy settings, the appointment of implementation and evaluation of health
a Chief Pharmacist means the Government would service delivery
maximise the opportunity to more efficiently and • Leadership on strategies of state significance
effectively respond to Australia’s health challenges to pharmacists, such as Medicines Safety and
and achieve desired reforms. Quality Use of Medicines, the Queensland
Antimicrobial Resistance Strategy, real-time
monitoring of medicines, Health and Wellbeing
Queensland, the National Medicines Policy,
and digital health strategies.
16 | 2020–21 Pre-budget submission – Queensland• Participation in the formulation and Timeline
implementation of policy, strategic direction From 1 July 2020.
and initiatives which support the delivery of
care and achieving state government health
Budget
objectives.
PSA estimates the budget allocation
The Chief Pharmacist would provide a link
to support this proposal would be
between regulation, programs, funding and
$300,000 annually, including salary
infrastructure, with a clear responsibility for
and on-costs.
coordinating all relevant segments of the
Department with the pharmacy sector and
fostering the collaboration of the pharmacy
workforce with other health professions within PSA calls on the Queensland
Queensland and other jurisdictions. The Chief Government to establish the role of
Pharmacist would liaise with all the contact Chief Pharmacist.
points within government and provide advice
to Ministers, Ministerial staff and agencies to
support policy development, planning and
BENEFITS TO
implementation of health service reform agendas.
QUEENSLANDERS
This position could also provide a consistent voice
and point of contact for peak professional bodies • Better coordination of government health
such as PSA to engage more efficiently with all policy and programs, particularly those
stakeholders. relating to the use of medicines and how
Creation of a Chief Pharmacist role would provide to utilise pharmacists to their full scope to
the strategic understanding and knowledge of improve Quality Use of Medicines
pharmacist capabilities to enable the Queensland • Provides a single point of contact
Government to most effectively utilise the between Queensland Government
pharmacist workforce to improve medicine agencies on pharmaceutical and
management and patient safety in hospitals, aged pharmacy sector issues
care, in the community and wherever medicines
• Provide advice to the Queensland
are used.
Government on how to achieve the
objectives of the National Medicines
Why it will work
Policy
As the Australian Government’s principal
• Delivers cross-departmental strategic
medical advisor, the role of Chief Medical
advice and insights on how to best utilise
Officer27 is recognised as essential for leading
the pharmacist workforce to achieve key
sound public health policy through provision of
health initiatives and outcomes
advice to the Minister for Health and leadership
of strategic departmental committees. As the • Support Medicine Safety and Quality Use
medicines experts, the provision of a similar of Medicines as a National Health Priority
level of pharmacist advice would further inform
Government policy.
Other Australian jurisdictions, including New
South Wales and the Australian Capital Territory
have an appointed Chief Pharmacist who provides
coordinated advice and oversight to medicine-
related matters within their health systems. These
roles are recognised as providing high quality
advice within government and facilitating efficient
operation of pharmacist-related regulation.
2020–21 Pre-budget submission – Queensland | 17Recommendation Five
Facilitate and fund emergency
presentations manageable by community
pharmacists
The challenge The proposed approach
In 2018-2019, there were 8.4 million presentations As identified in Action 6 of PSA’s Pharmacists in
to Australian public hospital emergency 2023: For patients, for our profession, for Australia’s
departments—an average of about 23,000 health system, building upon the established
presentations per day and up 4.2% from accessibility of community pharmacies in the
2017–18.28 Of these, 1,561,825 emergency primary health care space will improve the
department presentations were in Queensland, community’s access to health services. This will
with 70,229 (5%) of these being considered as be achieved by lessening the burden on other
non-urgent.28 Seventy percent (70%) of non- healthcare providers such as hospitals. Improved
urgent presentations to emergency departments access to healthcare across the country will reduce
occur between the hours of 9am and 7pm, government costs associated with the delivery of
during the typical business hours of a community care.24
pharmacy.28
Building upon the accessibility of community
The Australian Institute of Health and Welfare pharmacies in primary health care, it could be
report Use of emergency departments for lower promoted to the public that instead of going to
urgency care: 2015-16 to 2017-18 highlighted that ED, patients can visit their community pharmacist.
presentations to hospital emergency departments In addition, remuneration of pharmacist services
that are for lower urgency care may be avoidable in the assessment, triage and management of
through provision of other appropriate health these patients will reduce state government
services in the community.29 expenditure and improve accessibility by
providing timely treatment for patients with
Measures of non-urgent care were based on the
non-urgent medical conditions through the
2018 National Health Agreement (NHA) indicator
community pharmacy in both metropolitan and
and were defined as presentations that:29
rural areas.
• did not involve arrival by ambulance
It is estimated that 2.9 to 11.5 percent of all ED
• were assessed upon arrival as needing semi or services in Australia could be safely transferred
non-urgent care to a community pharmacy as part of a national
• were discharged without needing further scheme.30
hospital care. When extrapolating this to the ED services
The report found that between 2017–2018, 37% transferrable to community pharmacy it is
(2.9 million) ED presentations were for non-urgent estimated that of the 1.56 million ED services
care. There was a higher rate of presentations from provided in Queensland annually, up to 179,610
regional Primary Health Network (PHN) areas than are potentially transferrable.30
urban PHN areas (152 versus 92 per 1000 people Based on the average cost of an ED attendance in
respectively), although within urban areas there Australia being AUD $535.61 and an average cost
were varied levels of presentations.29 per pharmacist consultation of $26.88 (including
out-of-pocket patient costs for medicines)
applied to account cost offsets, this results in a
18 | 2020–21 Pre-budget submission – Queenslandpotential cost reduction of $508.73 per patient A total of 94 international schemes are identified
in Queensland transferred from the ED setting to in the literature, including the UK (England,
community pharmacy.30 Scotland, Northern Ireland and Wales) and regions
of Canada (known as Minor Ailments Prescribing
Under this scenario, if pharmacists were paid
Services).32,33 These initiatives were implemented
through a consultation fee structure per
in Scotland in 1999, England since 2000, Northern
consultation and if the patient paid for their
Ireland since 2009, Wales in 2013 and in Canada
non-prescription medications, the Queensland
since 2007.32
Government would save up to $91.3 million per
annum. Internationally, pharmacies are paid a consultation
fee in Europe and Canada for the delivery of
The availability of late-night pharmacy services,
minor ailment services.34 In England, payment
such as through 24/7 or after hours pharmacies,
ranges from GBP2 to GBP10 (~$A4 to $A19) per
can also help to reduce the rising number of after-
consultation and in some localities pharmacies
hours ED presentations.
are reimbursed for the cost of medicines supplied
PSA recommends funding pharmacists for the under a given formulary for certain minor
management of non-urgent or low-urgency ailments.35 Pharmacies may also receive a small
medical conditions through community annual retainer to assist with set-up costs.35
pharmacy. This should be supported by a co-
ordinated health promotion that promotes visiting
Timeline
a community pharmacy instead of an emergency
department for non-urgent or low-urgency Program planning from 1 July 2020
medical conditions. Commence program from 1 January
The proposed funding model should be a fee-for- 2021
consultation model or a banded-capitation model
with medicines supplied during the consult from Budget
a defined formulary reimbursed or paid for by
the individuals as out-of-pocket expenses or the PSA estimates the following funding
health system for a specific patient class. commitment over the forward
estimates for the program:
PSA also seeks funding to implement the program
which includes development of process, support • 2020-21: $4.75 million
tools, pharmacy establishment costs as well as • 2021-22: $7.1 million
education development, training and delivery.
• 2022-23: $7.1 million
Why it will work • 2023-24: $7.5 million
Patients seeking care from ED for conditions such Cost savings of up to $342 million on
as headaches, coughs and colds, earaches and non-urgent hospital admissions over
other non-urgent conditions are an inefficient use 4 years could be achieved.
of resources.29
There is strong evidence the clinical advice
provided by pharmacists regarding symptoms
of minor illness will result in the same health
outcomes as if the patient went to see their GP or
attended the emergency department.31
There is consistent evidence pharmacy-based
minor ailment schemes that manage non-urgent
conditions or low-urgency conditions, provide the
right level of care, mitigate funding and system
inefficiencies as patients access professional
support for conditions that can be self-managed.32
2020–21 Pre-budget submission – Queensland | 19PSA calls on the Queensland Government to allocate $26.45 million in funding
over 4 years for the management of non-urgent or low-urgency medical
conditions through community pharmacy. This would include funding for
the development and implementation of the service in pharmacies across
Queensland along with a consumer awareness campaign to encourage people
to visit a pharmacy instead of ED for non-urgent and lower-urgency care.
BENEFITS TO QUEENSLANDERS
• Relieving pressure on existing emergency departments and urgent care services
• Reducing the number of non-urgent presentations and/or low urgency presentations to
Queensland emergency departments, reducing state budget expenditure
• Improves accessibility by providing timely treatment for patients with non-urgent medical
conditions through the community pharmacy in both metropolitan and rural areas
• Empowering consumers to seek the appropriate level of care
• Increases primary care capacity and availability of general practice for medical provision
of chronic and complex patients through the transfer of common non-urgent medical
consultations from general practice to community pharmacy
James Buckley MPS Community pharmacist, Cooroy Qld
20 | 2020–21 Pre-budget submission – QueenslandAppendix I
Experience of a Queensland pharmacist
following floods
Burrey, J 2020. ‘Use every option when a natural disaster hits’. Australian Pharmacist. Pharmaceutical
Society of Australia. Vol 39. No 1.
MEMBER OPINION
DISASTER MANAGEMENT
MEMBER OPINION
DISASTER MANAGEMENT
Use every option when a
natural
Use everydisaster hits a
option when
natural disaster hits
Dispensing from a
I
t’s almost 10 years since a flood put side of town, and then a third pharmacist
the majority of Emerald, 270 from another pharmacy was over the bridge.
house, a library and
I
kilometres west of Rockhampton in There was lots of opening of boxes,
Dispensing
evacuation from a
centres: that’s t’s Queensland,
almost 10 years since a flood
underwater. put cut off
We were side ofcutting
town, and thenoff
things a third pharmacist
– ‘here’s a couple of
thefrom
majority
everyofdirection.
Emerald, 270 from another pharmacy
tablets to get youwas over the
through’ bridge.
– and
house,
whata library
happens andin a flood. kilometres It waswest
about offiRockhampton
ve days before in
the water There was lots lots
handwriting of opening
of labels.ofThere
boxes,was also
evacuation centres:
BY JESSICA BURREY MPSthat’s
Queensland,
subsided.underwater.
It didn’t quiteWeget
were cut point
to the off cutting things
a lot off – ‘here’s
of dealing a couple
with the of from the
doctors
from where
every direction.
we had to fly people out of town. tablets to get you
hospital. through’
For the – and it was trying
community
what happens in a flood. It But
wasitabout five close.
was very days before
At the the
timewater
I was handwriting lots of labels.
to help people There
establish wasmedicines
what also
subsided.
managingIt didn’t two quite
of thegetpharmacies
to the pointin town. a lot of
theydealing
couldwith and the doctors
couldn’t go from the
without.
BY JESSICA BURREY MPS
whereThe weluckier
had to of flythe
peopletwo out onlyofhad town. hospital. After
an inch of For the thecommunity
flood we weren’t it was trying
able to
But itwater
was very close.the
through At thestore.time TheI was
unlucky of to help people
occupy one establish what medicines
of the buildings for nearly
managingthe two twowas of the pharmacies
covered by about in 800
town. they could and couldn’t
five months. We hadgotowithout.
condense all our
The luckier
millimetresof thewater.
two only Andhad thatanwater
inch sat
of in After the flood
operations from wetwoweren’t able toto one
pharmacies
watertherethrough for fithe store.so
ve days, The unlucky
it was pretty of occupyveryone tinyofoutlet
the buildings
and encouragefor nearly staff to take
the two was covered
disgusting by the bytimeabout 800access again.five months.
I got leave. We Wewerehadreally
to condense
mindfulalltoour not put
millimetres When water.we Andknewthat thewaterfloodsat wasincomingoperations
peoplefrom two pharmacies
off because everybody to onewas doing
thereeverybody
for five days, was somadly
it was trying
pretty to get very tiny outlettough
it pretty and encourage
– you wantstaff to take
to look after
disgusting by the time
prescriptions filled.I got
Andaccesswe only again.
had a leave.yourWe were
people really mindful
as much as toyounot can.put
When
limited wenumber
knew the of flpeople
ood was to coming
process people offLooking because everybody
back, my advice was doing
is to also
everybody
those was madly trying
prescriptions and to get people it pretty
service toughwhat
consider – you want to
support lookgoing
you’re after to need
prescriptions
who lived filled.
on the Andother we only sidehad
of thea bridgeyour people
post-event as much
– thatas you can.
includes support for
limited number
before of people to process
it closed. Looking
yourself,back,yourmy advice
staff is to also
and your community.
those prescriptions and service
It was like nothing I’ve people
ever seen. Weconsider what support
Postscript: In lightyou’re going
of the to need
recent
who lived
were on onlytheableother side of the
to operate outbridge
of one of post-event – that includes
devastation that hassupport
swept the for country,
before theit closed.
pharmacies and literally couldn’t keep yourself, your
as an staff and
industry weyour
needcommunity.
to advocate for
‘It was like nothing It the
wasbasket
like nothing
on theI’ve bench, everthere We so Postscript:
seen.were the roleInof light of the recent
pharmacists in disaster
were many
only able to operate
scripts waiting out to be offione
lled.ofAt the devastation
management. that hasAs swept the country,
the most accessible
I’ve ever seen. We ... the pharmacies
same time our andstaffliterally
werecouldn’t
concerned keepaboutas an health
industry weprofessionals,
care need to advocate and withfor the
‘It was like nothing
literally couldn’t keep the basket
their own on the bench, there
properties and we werewere sopackingthe role
needof pharmacists
for patients to in have
disaster continuity in
manystuff scripts
up waiting
for the SES to be to flfiylled.
outAtto the management.
properties, medicinesAsaccess, the most accessibleneed to be
pharmacists
I’vethe
everbasket
seen. We ...
on the sameso time
it wasourallstaff werehectic.
pretty concerned about healthincluded care professionals,
and remunerated and with forthe
literally
bench couldn’t keep so
there were
their ownOnce
stuff up
properties
for the
we were andno welonger
were packing
allowed need involvement
for patients to inhave
bothcontinuity
disaster in
access theSES to fly outI had
pharmacy, to properties,
a staff member medicines access, pharmacists
management planning, and need to be
in the
themany
basketscripts
on thewaiting to so it was
whoalllivedpretty hectic.
in the dry area store a bunch of included and remunerated
provision for
of frontline services during
Once
stuffwe were
at her no longer
place. We also allowed
set up shop in involvement in both disaster
natural disasters. (See cover feature, p16.)
benchbe fithere
lled.‘ were so accessthe thelocal
pharmacy,
library. The I had a staff member
hospital was management Workplanning,
on permanent and inchanges
the to
many scripts waiting to who lived
operatingin theout dryofarea store asite
a remote bunch of itprovision
because of frontline
emergency servicesmust
dispensing during continue –
stuff atwas herunderwater,
place. We also so we sethad up shop
limitedin natural
notdisasters. (See cover
only to prepare feature,
us for futurep16.)
be filled.‘
JESSICA BURREY BPharm, Grad Cert Buis, MPS has the local library.
services in The
town. hospital
Towards wasthe end, I was at Work on permanent
challenges, changes
but to assist to
pharmacists and
been a pharmacist for 13 years, 10 of them in Emerald,
operating out of a remote
one evacuation site because
site, another it
pharmacist emergency dispensing must
their communities continue
in recovery –
efforts
central Queensland. She has been a director of Emerald
Pharmacy Services for the past 3 years. was underwater,
was at an evacuationso we hadsite limited
on the other not only to preparedisaster.
post-natural us for future
JESSICA BURREY BPharm, Grad Cert Buis, MPS has services in town. Towards the end, I was at challenges, but
2020–21 Pre-budget to assist pharmacists
submission and – Queensland | 21
been a pharmacist for 13 years, 10 of them in Emerald,
central Queensland. She has been a director of Emerald
one evacuation site, another pharmacist their communities in recovery efforts
Pharmacy Services for the past 3 years. was at an evacuation site on the other post-natural disaster.Appendix II
Importance of effective emergency supply
provisions for Prescrpition Only Medicines
in disasters
FEATURE Barbeler, D Cooke J. ‘Preparing for Disasters’. Australian
Pharmacist. Pharmaceutical Society of Australia. Vol 39. No 1.
COVER STORY
PREPARING FOR
DISASTERS
Pharmacies play a vital role in supporting communities
during natural disasters, but just how well prepared are
pharmacists and staff for a devastating event?
BY DAVID BARBELER AND JENNIFER COOKE
Burnt out buildings along the main street of historic Cobargo, NSW,
population 776, on 31 December, 2019.
(Photo by SEAN DAVEY/AFP via Getty Images)
22 | 2020–21 Pre-budget submission – Queensland
22
22Learn more at
australianpharmacist.
com.au
E
mmanuel Pasura MPS, the pharmacist- brought in by helicopter, police barge,
in-charge at remote Mallacoota navy vessel, cargo ship, ferry and even jet
Pharmacy, worked non-stop for weeks skis – were examples, according to PSA
after day turned to night on New Year’s Eve National President Associate Professor
morning and a raging fire roared towards the Chris Freeman, of ‘pharmacists going above
town, forcing thousands to the beach and and beyond for their communities’.
boats where they saw in 2020. But were pharmacists prepared for
‘Just a few weeks before the fire I started a disaster that has changed the federal
ordering increased quantities of medicines government rhetoric on climate change?
like Ventolin (salbutamol) and antibiotics – Were disaster plans adequate to meet
just in case,’ he said. a permanent shift in fire risk that now
With ash, thick smoke and poor air quality threatens the survival of many species
adding to asthma risks in the vulnerable, of birds and animals, urban catchments,
he had run out of puffers within an hour of water security and the permanence of
opening the pharmacy the previous day. infrastructure?
It was the start of a nightmare logistical Australia is no stranger to sudden
effort to get supplies of salbutamol, masks natural disasters. Bushfires, cyclones, floods
and other essential medicines into the tiny – 300 millimetres of rain fell in just hours
town on the eastern-most tip of Victoria. around the Gold Coast during a 1-in-100-
During the annual Christmas holiday season year thunderstorm while fires still burned
the population swells dramatically to about elsewhere last month – a community
5,000 people. (See Member Opinion, p15.) somewhere in Australia has been affected.
Thousands of evacuated tourists and Yet, according to Queensland
locals camped on the beach and in boats that University of Technology (QUT) researcher
night to outrun the flames that razed up to Dr Elizabeth McCourt, pharmacists are 1.7
300 homes and felled bushland that closed times more likely to have experienced a
the only road out for at least a month. natural disaster than they were to have
Raj Gupta, the only pharmacist in the tiny received previous education or training for
NSW South Coast town of Malua Bay, was a disaster. ‘That, to me, is quite shocking. It
forced into emergency accommodation in shows just how scarce training, information
Batemans Bay, the Shoalhaven area hard-hit and resources are for pharmacists in
by the relentless fires that destroyed swathes this area,’ says Dr McCourt, a hospital
in and around nearby towns. pharmacist whose research focuses on the
Mr Gupta continued dispensing in the preparedness of pharmacists for disasters
dimness of his power-less pharmacy to keep and emergencies.
local residents in necessary medicines while
the 3-day supply rule remained in effect in
Townsville
NSW up to 7 January.
‘There’s been no power, there’s been no
Rockhampton
communication [so] we can’t take payments, Emerald
but that’s not much of a concern. People will
come back and pay. They are very honourable
people,’ Mr Gupta told SBS at the time.
His and other heroic efforts by Gold Coast
pharmacists in the worst-hit areas of NSW,
Victoria and Kangaroo Island off South
Australia – where supplies eventually were
Kangaroo Island Culburra Beach
Canberra
Bateman’s & Malua Bay Bay
Narooma Malua Bay
Eden
Mallacoota
2020–21 Pre-budget submission – Queensland | 23
AUSTRALIAN PHARMACIST 23You can also read