Guidance on Completing a Written Allergy and Anaphylaxis Emergency Plan
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
CLINICAL REPORT Guidance for the Clinician in Rendering Pediatric Care
Guidance on Completing a
Written Allergy and Anaphylaxis
Emergency Plan
Julie Wang, MD, FAAP,a Scott H. Sicherer, MD, FAAP,a,b SECTION ON ALLERGY AND IMMUNOLOGY
Anaphylaxis is a potentially life-threatening, severe allergic reaction. The abstract
immediate assessment of patients having an allergic reaction and prompt
administration of epinephrine, if criteria for anaphylaxis are met, promote
optimal outcomes. National and international guidelines for the management
aDivisionof Pediatric Allergy and Immunology, and bProfessor of
of anaphylaxis, including those for management of allergic reactions at
Pediatrics, Jaffe Food Allergy Institute, Icahn School of Medicine at
school, as well as several clinical reports from the American Academy of Mount Sinai, New York, New York
Pediatrics, recommend the provision of written emergency action plans to Dr. Wang drafted the initial report, revised the document for critically
those at risk of anaphylaxis, in addition to the prescription of epinephrine important intellectual content on the basis of comments from AAP
reviewers, and contributed to writing the final manuscript. Dr. Sicherer
autoinjectors. This clinical report provides information to help health contributed to the initial drafting and editing at all stages, including
the final manuscript. Drs. Wang and Sicherer approved the final
care providers understand the role of a written, personalized allergy and version to be published and agree to be accountable for all aspects
anaphylaxis emergency plan to enhance the care of children at risk of of the work.
allergic reactions, including anaphylaxis. This report offers a comprehensive This document is copyrighted and is property of the American
Academy of Pediatrics and its Board of Directors. All authors have
written plan, with advice on individualizing instructions to suit specific filed conflict of interest statements with the American Academy
patient circumstances. of Pediatrics. Any conflicts have been resolved through a process
approved by the Board of Directors. The American Academy of
Pediatrics has neither solicited nor accepted any commercial
involvement in the development of the content of this publication.
Clinical reports from the American Academy of Pediatrics benefit from
expertise and resources of liaisons and internal (AAP) and external
INTRODUCTION reviewers. However, clinical reports from the American Academy of
Pediatrics may not reflect the views of the liaisons or the organizations
Anaphylaxis is a potentially life-threatening, severe allergic reaction.1 As or government agencies that they represent.
such, it is a medical emergency that requires an immediate assessment of The guidance in this report does not indicate an exclusive course of
treatment or serve as a standard of medical care. Variations, taking
the patient and administration of epinephrine. Given the unpredictable into account individual circumstances, may be appropriate.
nature of anaphylaxis, preparedness promotes optimal outcomes. Thus,
All clinical reports from the American Academy of Pediatrics
national and international anaphylaxis guidelines, as well as several automatically expire 5 years after publication unless reaffirmed,
American Academy of Pediatrics (AAP) clinical reports (“Self-injectable revised, or retired at or before that time.
Epinephrine for First-aid Management of Anaphylaxis,” “Management of DOI: 10.1542/peds.2016-4005
Food Allergy in the School Setting,” and “Medical Emergencies Occurring
Julie Wang, MD. E-mail: julie.wang@mssm.edu
at School”), recommend the provision of emergency action plans to
pediatric patients who are at risk of anaphylaxis, in addition to the
prescription of epinephrine autoinjectors.2–7 Guidance from the Centers To cite: Wang J, Sicherer SH, AAP SECTION ON ALLERGY AND
for Disease Control and Prevention for managing food allergy in schools IMMUNOLOGY. Guidance on Completing a Written Allergy
and Anaphylaxis Emergency Plan. Pediatrics. 2017;139(3):
and early education programs also supports the inclusion of written
e20164005
emergency plans for the management of children with food allergy.8
Downloaded from www.aappublications.org/news by guest on November 2, 2021
PEDIATRICS Volume 139, number 3, March 2017:e20164005 FROM THE AMERICAN ACADEMY OF PEDIATRICSWritten action plans have been WHEN TO PROVIDE A WRITTEN Having a history of asthma and/or
shown to improve outcomes for EMERGENCY PLAN of anaphylaxis is associated with a
asthma,9 and similarly, action plans higher risk of severe reactions and, as
An allergy and anaphylaxis
have the potential to improve such, these should be noted.12,13 The
emergency plan, developed by the
outcomes of anaphylaxis by reducing presence of asthma is associated with
health care provider, is a document
the frequency and severity of an increased likelihood of having
written in simple lay terms that
reactions, improving knowledge respiratory symptoms during an
can guide the patient, family and
of anaphylaxis, improving use of allergic reaction and can cause the
nonfamily caregivers, and school
epinephrine autoinjectors, and reaction to be more difficult to treat.
personnel in the event that the child
reducing anxiety of patients and In a recent study of anaphylaxis-
experiences an allergic reaction.
caregivers.10 Action plans serve as related hospitalizations over 2
Allergic reactions can occur
decades in the United Kingdom, 75%
an important tool for anaphylaxis anywhere and at any time, and health
of patients with fatal food-induced
education and treatment. care providers may not be present
anaphylaxis were noted to have
at the time a child has an allergic
concurrent asthma.14
Currently, several different reaction. Therefore, the emergency
anaphylaxis action plans are action plan serves as a guide for the
patient, caregiver, and/or school A child’s ability to self-carry
available, but variations exist emergency medications and/or
in content and treatment personnel to determine how to treat
allergic reactions. self-administer medications can be
recommendations, which can lead indicated. This ability will depend on
to confusion. A survey of AAP It is beneficial to provide an allergy the age and maturity of the child. All
Section on Allergy and Immunology and anaphylaxis emergency plan states have laws to allow self-carry
members found that there is wide when there is a diagnosis of an by students in schools; however,
variation in terms of which plans allergic disorder that places the some states require a student’s
are used by pediatric allergy child at risk of anaphylaxis (eg, food physician and parents to sign a
specialists.11 Therefore, a universal allergy, insect sting allergy). A new form stating the student has the
plan for pediatric patients could be written plan can be provided, for maturity to self-administer relevant
beneficial to patients, families, health example, annually at the beginning medications. Although no specific
care professionals, and schools to of the school year, to address any guidelines exist to determine when
facilitate care for children at risk need for adjustment of medication it would be appropriate for a child
of anaphylaxis. The AAP Allergy doses or whenever there is any to self-carry and/or self-administer
and Anaphylaxis Emergency Plan change in allergic triggers, comorbid epinephrine autoinjectors, a survey
associated with this clinical report conditions, or any new medical of members of the AAP Section on
was developed with the support information that would warrant a Allergy and Immunology found that
change in the plan. most pediatric allergy specialists
and advice of various committees,
councils, and sections within the begin to expect children 9 through
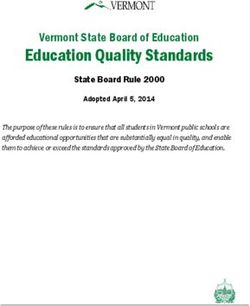
AAP. It is available online (www.aap. 11 years of age to be able to recognize
COMPLETING THE ALLERGY AND signs and symptoms of anaphylaxis
org/aaep) and shown in Fig 1. This ANAPHYLAXIS EMERGENCY PLAN and expect children 12 through 14
plan takes into consideration several
years of age to self-carry epinephrine
aspects of anaphylaxis emergency Demographic Information and
autoinjectors and self-administer
care, including the recognition of Allergy History
the device.11 In a study of family and
signs and symptoms and treatment.
The initial section is completed with nonfamily caregivers of children with
This clinical report focuses on
the child’s demographic information, food allergy, most expected the child
providing guidance to the clinician to including name, date of birth, and to be able to recognize anaphylaxis
complete the plan. The guidance in age, as a personalized plan for the at approximately 6 through 8 years
this clinical report has not undergone child. The plan should be dated so of age and believed that epinephrine
a systematic review nor a strict that it is easy to determine when autoinjector use was appropriate
weighing of the evidence and, as such, the health care provider created the for children 6 through 11 years of
should not be considered a practice emergency plan. Allergic triggers can age.15 Thus, these decisions may
guideline. Clinical guidance regarding be listed in the space provided. It is benefit from personalization with
treatment with epinephrine in the advisable to include the weight of the the input of the family. Of note, if it
first-aid management of anaphylaxis child at the time the plan was created is determined that self-carrying/
is covered in a separate clinical to allow confirmation of correct self-administration is appropriate,
report.5 medication dosages. it is important to designate adults
Downloaded from www.aappublications.org/news by guest on November 2, 2021
e2 FROM THE AMERICAN ACADEMY OF PEDIATRICSto be additionally and primarily it may be difficult to determine In some situations, licensed
responsible for treatment, because by the observer. Therefore, the health care providers will not
the child may not be depended on to plan provides options that can be be available in a school setting
self-treat if he or she is panicked or selected at the physician’s discretion and there is a desire to simplify
severely symptomatic. to address these possibilities. For the instructions for delegates or
example, if the child has a history designated individuals. In these
Treatment Pathways of very severe anaphylaxis, such cases, the health care provider can
Epinephrine is the first-line as with respiratory distress, indicate that definitive allergen
treatment of anaphylaxis; therefore, hypoxia, hypotension, or neurologic exposures would require immediate
the form indicates that if there is compromise after exposure to treatment with epinephrine. If the
any uncertainty about whether specific allergen(s), then the administration of antihistamine by
anaphylaxis is occurring, epinephrine health care provider may consider delegates or designated individuals
should be administered immediately. recommending epinephrine to be is not permitted by school or local
The early use of epinephrine has administered immediately after a regulations, this scenario would be
been shown to be associated with likely ingestion or sting at the onset another in which the health care
better outcomes. In studies of of the first symptom (even mild ones, provider should consider instructing
fatal and near-fatal anaphylaxis, such as itchiness of the face/mouth, epinephrine to be used in the event
delayed or lack of administration a few hives, or mild symptoms of of a definite allergen exposure even
of epinephrine was noted in stomach discomfort or nausea), if mild symptoms occur (see below
the majority of cases.13 Studies because severe reactions can for more details on the completion
have shown that the early use of of the form for no permission to use
progress rapidly.6,18 Other scenarios
epinephrine in the treatment of food- antihistamine).
in which to consider immediate
induced anaphylaxis was associated epinephrine use after definitive If there is a mild symptom alone,
with a decreased likelihood the child ingestion or sting when only mild an oral antihistamine may be
would require hospital admission.16,17 symptoms are present (assuming administered first. If additional
Therefore, the plan instructs on additional doses are available, symptoms are observed after oral
prompt treatment with epinephrine should symptoms emerge and antihistamine has been administered
for symptoms of anaphylaxis. progress) may include a child who or if more than 1 organ system
When allergic reactions are has a history of repeated anaphylaxis is involved, then epinephrine
suspected, the caregiver or school with exposure to the specific is indicated. Education about
personnel should observe for signs allergen(s), a child who has a history anaphylaxis and epinephrine is
and symptoms of an allergic reaction of significant reactions with trace helpful, and additional advice about
and determine the appropriate exposures, or a child with comorbid the administration of epinephrine
treatment pathway as outlined on asthma that is poorly controlled. is provided in another AAP clinical
the allergy and anaphylaxis The allergen(s) can be listed as a report.5
emergency plan (Fig 1). If any severe “special situation” (box within the The use of antihistamine is
symptom develops, anaphylaxis “For Severe Allergy and Anaphylaxis” included as an option because
is highly likely, and epinephrine box on the left-hand side of the this plan provides instructions
should be injected immediately.1,5 form). Although controversial,19 for managing allergic reactions
Epinephrine administration there may be situations in which the with a range of severities. Several
should be followed by activation health care provider may consider studies have examined allergic
of emergency medical services recommending epinephrine to be reactions attributable to accidental
(calling 911), monitoring of the child, administered immediately after a or intentional exposures in food-
and consideration of adjunctive definite ingestion or sting and before allergic children and noted that
treatment with oral antihistamines symptoms develop (manually write 30% to 70% of reactions are
and/or bronchodilators for known in “no” in place of “mild”), because characterized as mild in severity.
asthmatics or in the presence of severe reactions can occur suddenly In a cohort of 512 young children
respiratory symptoms, including without significant warning signs.18 (3–15 months at enrollment) with
wheezing or shortness of breath. An example is if a child has had a allergies to milk, egg, and/or peanut
In some circumstances, it may be history of severe cardiovascular followed over 3 years, 70% of the
beneficial to treat with epinephrine collapse to a specific allergen. These 1171 reactions occurring during the
even if anaphylaxis is not occurring, suggestions are based on expert study time frame were considered
such as when anaphylaxis is likely to opinion, not from data acquired to be mild (defined as skin and/or
develop after an exposure or when through controlled trials. oral symptoms and/or upper
Downloaded from www.aappublications.org/news by guest on November 2, 2021
PEDIATRICS Volume 139, number 3, March 2017 e3respiratory symptoms, but not all 3 After initiating treatment, additional or intramuscular injection in the
organ systems).20 In a study in 88 instructions for contacting deltoid.25
children with milk allergy (median emergency medical services (calling
Providing epinephrine ampules,
age: 32.5 months) followed for 1 911) and monitoring for progression
needles, and syringes to patients and
year, 53% of reported reactions of symptoms are provided on the
families for weight-based dosing is
were mild (defined as cutaneous plan. For those who are initially
often not practical and subject to
symptoms [angioedema excluded], treated with epinephrine, a second
human error; therefore, epinephrine
rhinitis, or conjunctivitis).21 A dose of epinephrine can be given
autoinjectors are prescribed for use
recent Canadian study of accidental if symptoms persist or recur. For
in the community setting. Currently,
exposures to peanut in 1941 children those who are observed only or for
only 2 epinephrine autoinjector
(mean age: 7 years) with confirmed those who receive antihistamines as
dosing options exist, 0.15 mg or
peanut allergy reported that 30% the first treatment, any progression
0.3 mg. Package inserts state that
of exposures resulted only in mild of symptoms would warrant
the 0.15-mg dose is appropriate for
symptoms (defined as involving epinephrine use, and the use of an
children weighing 15 to 30 kg, and
only pruritus, urticaria, flushing, or antihistamine should not delay the
the 0.3-mg dose should be prescribed
rhinoconjunctivitis).22 Therefore, in administration of epinephrine.
for those who weigh greater than or
the event of a mild allergic reaction
In some severe cases of anaphylaxis, equal to 30 kg. On the basis of the
involving isolated skin symptoms,
rapid vasodilation and extravasation lack of readily available alternatives
mild facial or oral symptoms, or mild
of fluid have been reported, resulting and the favorable benefit-versus-risk
gastrointestinal tract discomfort,
in a decrease of up to a 35% in ratio, prescription of the 0.15-mg
none of which meet the criteria
circulating blood volume within autoinjector can be considered for
for anaphylaxis, the use of oral
minutes.23 Upright posture in cases of those weighing 7.5 to 15 kg.5 Because
antihistamines may be an option.
food-induced anaphylactic shock has of the concern of underdosing in
been reported to be associated with children nearing 30 kg, expert
Another concern is that if
fatalities.24 This “empty ventricle consensus suggests that children
epinephrine is stipulated in all cases
syndrome” has not been reported be switched to the 0.3-mg dose
of allergic reaction regardless of
in children; however, it would be autoinjector when they reach 25 kg,
severity, a child may be hesitant
prudent to place the child in the with consideration of switching to
to voice any symptoms for fear
supine position to prevent pooling this higher dose at a lower weight
of epinephrine autoinjector use.
of blood in the lower extremities if the child has asthma or other
Thus, emphasizing the option to
after epinephrine is administered. risk factors for severe reaction.5
observe and also having the option
This position may not be tolerated Physicians can discuss the rationale
of using antihistamines for mild
in some circumstances, such as if a for selecting autoinjector doses
allergic reactions allows the plan to
child is vomiting or having difficulty with each individual family. Two
be individualized according to the
breathing. In these situations, the epinephrine autoinjectors should
child’s history. However, it is not
child can be placed in the lateral be available at all times, because
possible to know the eventuality
decubitus position (lying on his or a second administration may be
of any allergic reaction, and
her side). needed if there is not a quick or
consideration can be given to use
adequate response to the first dose of
epinephrine liberally. If an option
Medications epinephrine.
is needed where antihistamine
alone is not permitted (eg, if school Medications, specifying dosage, H1 antihistamines are effective for
or local policies do not permit should be clearly indicated at the the treatment of acute cutaneous
delegates or designated individuals bottom of the form. Standard dosing symptoms, such as pruritus
to administer antihistamines), then for epinephrine in the treatment of and urticaria, associated with
no antihistamine would be listed anaphylaxis in health care settings is allergy.26 Therefore, in cases of
under medications. In this situation, 0.01 mg/kg, intramuscularly, with the isolated mild symptoms, the use
mild symptoms would not be treated use of a 1:1000 dilution (maximum of oral antihistamines may be
and close observation and watching of 0.3 mg in a prepubertal child and appropriate. Diphenhydramine
for possible progression would 0.5 mg in a teenager). Intramuscular is the most commonly used H1
be indicated. However, there is an injection of epinephrine in the antihistamine. Standard dosing
option to list all of the allergens lateral thigh is the preferred route is 1 mg/kg, up to 50 mg. First-
under “special situation” to indicate of administration because it results generation H1 antihistamines,
that any symptoms would require the in higher and faster peak plasma such as diphenhydramine, cross
administration of epinephrine. concentrations than subcutaneous the blood-brain barrier, causing
Downloaded from www.aappublications.org/news by guest on November 2, 2021
e4 FROM THE AMERICAN ACADEMY OF PEDIATRICSsedation and impairment in to the family regarding the benefits nonfamily caregivers, and school
cognitive function. These side of permitting 2-way sharing of personnel in the management of
effects can potentially complicate information between the school allergic reactions.
the neurologic assessment of a child and the health care provider and 4. Epinephrine is the medication of
who is experiencing an allergic completing any forms that would be choice for the initial treatment
reaction. These adverse effects are required to allow this exchange of of anaphylaxis, and early
significantly less likely to occur for information. administration is associated
second-generation H1 antihistamines, with optimal outcomes. In the
In addition to providing this allergy
because these medications cross event of a definite exposure to
and anaphylaxis emergency plan,
the blood-brain barrier to a much an allergen that has previously
the patient should have updated
lesser extent.26 In a randomized caused a severe reaction, or if
prescriptions for emergency
double-blind study of 70 allergic anaphylaxis develops, immediate
medications. It is also helpful for
reactions during oral food challenge, use of epinephrine is warranted.
the health care provider to review
cetirizine (second-generation H1 If exposure to an allergen triggers
with the patient and/or family
antihistamine) was shown to have a only a mild symptom, observation
members instructions for, and show
similar efficacy and onset of action only or initiating treatment
the proper use of, epinephrine
compared with diphenhydramine in with an antihistamine may be
autoinjectors by using a training
treating cutaneous symptoms during appropriate.
device that has the same mechanism
acute food-induced allergic reactions.
but does not contain medication 5. This allergy and anaphylaxis
Given these findings, in addition
or the needle. Patients and family emergency plan allows
to the longer duration of action
members should be reminded to health care providers the
compared with diphenhydramine,
check expiration dates on their opportunity to individualize the
cetirizine is a good option to consider
epinephrine autoinjectors and treatment plan according to the
for the treatment of isolated mild
be familiar with proper storage child’s history, family input, and
symptoms of an allergic reaction.27
conditions. Additional information local regulations. Options and
Additional Instructions Regarding about anaphylaxis management is considerations for completing the
Completion of the Emergency Plan reviewed in another AAP clinical plan are reviewed in this clinical
report.5 report.
Space is provided for parents’ and
health care providers’ signatures as
an additional measure to indicate AUTHORS
SUMMARY Julie Wang, MD, FAAP
parental understanding and
1. National and international Scott H. Sicherer, MD, FAAP
agreement with the allergy and
anaphylaxis emergency plan. Space is guidelines support the use of a SECTION ON ALLERGY AND IMMUNOLOGY
provided to indicate the dates of the written allergy and anaphylaxis EXECUTIVE COMMITTEE, 2015–2016
parents’ and health care providers’ emergency plan to enhance
Elizabeth Matsui, MD, FAAP, Chair
signatures. the care of children at risk of Stuart Abramson, MD, PhD, FAAP
The second page provides space anaphylaxis. Although several Chitra Dinakar, MD, FAAP
for additional instructions, such plans are currently available, they Anne-Marie Irani, MD, FAAP
differ in content and treatment Jennifer S. Kim, MD, FAAP
as statements of disability. Space Todd A. Mahr, MD, FAAP, Immediate Past Chair
is provided to include contact recommendations, potentially
Michael Pistiner, MD, FAAP
information for health care providers, leading to confusion. Thus, a Julie Wang, MD, FAAP
parents/guardians, and other universal plan may be beneficial
to patients, families, health care LIAISON
caregivers.
professionals, and schools. Paul V. Williams, MD, FAAP – American Academy of
There is blank space on the second Allergy, Asthma, and Immunology
page that can be used to provide 2. An allergy and anaphylaxis
information specific to the school emergency plan, developed by STAFF
or child or illustrations of using the the health care provider, would Debra Burrowes, MHA
autoinjector. be beneficial for patients who are
at risk of anaphylaxis and those
The plan is given to the patient and
who have been prescribed an
his or her family so they may review ABBREVIATION
epinephrine autoinjector.
it and share it with the school or
AAP: American Academy of
other child care facility or caregivers. 3. The written plan may serve as
Pediatrics
The health care provider may speak a guide for patients, family and
Downloaded from www.aappublications.org/news by guest on November 2, 2021
PEDIATRICS Volume 139, number 3, March 2017 e5FIGURE 1
AAP Allergy and Anaphylaxis plan.
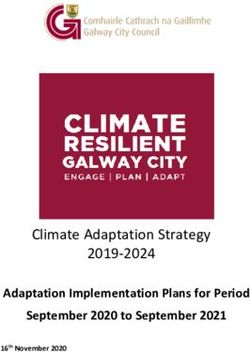
Downloaded from www.aappublications.org/news by guest on November 2, 2021FIGURE 1
Continued
Downloaded from www.aappublications.org/news by guest on November 2, 2021PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2017 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they do not have a financial relationship relevant to this article to disclose.
FUNDING: No external funding.
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
REFERENCES
1. Sampson HA, Muñoz-Furlong A, 9. Gibson PG, Powell H, Coughlan J, is associated with a lower risk of
Campbell RL, et al. Second Symposium et al. Self-management education and hospitalization. J Allergy Clin Immunol
on the Definition and Management regular practitioner review for adults Pract. 2015;3(1):57–62
of Anaphylaxis: summary report— with asthma. Cochrane Database Syst
17. Gold MS, Sainsbury R. First aid
Second National Institute of Allergy Rev. 2003;1:CD001117
anaphylaxis management in children
and Infectious Disease/Food
10. Nurmatov U, Worth A, Sheikh A. who were prescribed an epinephrine
Allergy and Anaphylaxis Network
Anaphylaxis management plans for the autoinjector device (EpiPen). J Allergy
Symposium. J Allergy Clin Immunol.
acute and long-term management of Clin Immunol. 2000;106(1 pt 1):
2006;117(2):391–397
anaphylaxis: a systematic review. 171–176
2. Simons FE, Ardusso LR, Bilò MB, J Allergy Clin Immunol.
18. American Academy of Allergy, Asthma,
et al; World Allergy Organization. World 2008;122(2):353–361, e1–e3
and Immunology Board of Directors.
Allergy Organization guidelines for
11. Simons E, Sicherer SH, Simons FE. Anaphylaxis in schools and other
the assessment and management of
Timing the transfer of responsibilities childcare settings. J Allergy Clin
anaphylaxis. World Allergy Organ J.
for anaphylaxis recognition and use Immunol. 1998;102(2):173–176
2011;4(2):13–37
of an epinephrine auto-injector from 19. Turner PJ, DunnGalvin A, Hourihane
3. Lieberman P, Nicklas RA, Oppenheimer adults to children and teenagers:
J, et al The diagnosis and management JO. The emperor has no symptoms:
pediatric allergists’ perspective. the risks of a blanket approach to
of anaphylaxis practice parameter: Ann Allergy Asthma Immunol.
2010 update. J Allergy Clin Immunol. using epinephrine autoinjectors for
2012;108(5):321–325 all allergic reactions. J Allergy Clin
2010;126(3):477–480, e1–e42
12. Bock SA, Muñoz-Furlong A, Sampson Immunol Pract. 2016;4(6):
4. Muraro A, Roberts G, Worm M, et al; 1143–1146
HA. Fatalities due to anaphylactic
EAACI Food Allergy and Anaphylaxis
reactions to foods. J Allergy Clin 20. Fleischer DM, Perry TT, Atkins D,
Guidelines Group. Anaphylaxis:
Immunol. 2001;107(1):191–193 et al. Allergic reactions to foods
guidelines from the European Academy
of Allergy and Clinical Immunology. 13. Bock SA, Muñoz-Furlong A, Sampson in preschool-aged children in a
Allergy. 2014;69(8):1026–1045 HA. Further fatalities caused by prospective observational food
anaphylactic reactions to food, allergy study. Pediatrics. 2012;130(1).
5. Sicherer SH, Simons FE; Section Available at: www.pediatrics.org/cgi/
2001-2006. J Allergy Clin Immunol.
on Allergy and Immunology. Self- content/full/130/1/e25
2007;119(4):1016–1018
injectable epinephrine for first-aid
management of anaphylaxis [published 14. Turner PJ, Gowland MH, Sharma V, 21. Boyano-Martínez T, García-Ara C,
correction appears in Pediatrics. et al. Increase in anaphylaxis-related Pedrosa M, Díaz-Pena JM, Quirce
2007;119(6):1271]. Pediatrics. hospitalizations but no increase S. Accidental allergic reactions
2007;119(3):638–646 in fatalities: an analysis of United in children allergic to cow’s milk
Kingdom national anaphylaxis data, proteins. J Allergy Clin Immunol.
6. Sicherer SH, Mahr T; Section on Allergy 2009;123(4):883–888
and Immunology. Management of 1992-2012. J Allergy Clin Immunol.
food allergy in the school setting. 2015;135(4):956–963, e1 22. Cherkaoui S, Ben-Shoshan M,
Pediatrics. 2010;126(6):1232–1239 15. Simons E, Sicherer SH, Weiss C, Alizadehfar R, et al. Accidental
Simons FE. Caregivers’ perspectives on exposures to peanut in a large cohort
7. Council on School Health. Medical
timing the transfer of responsibilities of Canadian children with peanut
emergencies occurring at school.
for anaphylaxis recognition and allergy. Clin Transl Allergy. 2015;5:16
Pediatrics. 2008;122(4):887–894
treatment from adults to children 23. Fisher MM. Clinical observations on
8. Centers for Disease Control and
and teenagers. J Allergy Clin I the pathophysiology and treatment
Prevention. Voluntary Guidelines for
mmunol Pract. 2013;1(3): of anaphylactic cardiovascular
Managing Food Allergies in Schools
309–311 collapse. Anaesth Intensive Care.
and Early Care and Education
1986;14(1):17–21
Programs. Washington, DC: US 16. Fleming JT, Clark S, Camargo CA Jr,
Department of Health and Human Rudders SA. Early treatment of food- 24. Pumphrey RS. Fatal posture in
Services; 2013 induced anaphylaxis with epinephrine anaphylactic shock. J Allergy Clin
Downloaded from www.aappublications.org/news by guest on November 2, 2021
e8 FROM THE AMERICAN ACADEMY OF PEDIATRICSImmunol. 2003;112(2): 2004;113(6):1039]. J Allergy Clin 27. Park JH, Godbold JH, Chung D,
451–452 Immunol. 2004;113(5):837–844 Sampson HA, Wang J. Comparison of
25. Simons FE. First-aid treatment 26. Simons FE, Simons KJ. Histamine cetirizine and diphenhydramine in
of anaphylaxis to food: focus on and H1-antihistamines: celebrating the treatment of acute food-induced
epinephrine [published correction a century of progress. J Allergy Clin allergic reactions. J Allergy Clin
appears in J Allergy Clin Immunol. Immunol. 2011;128(6):1139–1150, e4 Immunol. 2011;128(5):1127–1128
Downloaded from www.aappublications.org/news by guest on November 2, 2021
PEDIATRICS Volume 139, number 3, March 2017 e9Guidance on Completing a Written Allergy and Anaphylaxis Emergency Plan
Julie Wang, Scott H. Sicherer and SECTION ON ALLERGY AND IMMUNOLOGY
Pediatrics 2017;139;
DOI: 10.1542/peds.2016-4005 originally published online February 13, 2017;
Updated Information & including high resolution figures, can be found at:
Services http://pediatrics.aappublications.org/content/139/3/e20164005
References This article cites 26 articles, 4 of which you can access for free at:
http://pediatrics.aappublications.org/content/139/3/e20164005#BIBL
Subspecialty Collections This article, along with others on similar topics, appears in the
following collection(s):
Allergy/Immunology
http://www.aappublications.org/cgi/collection/allergy:immunology_s
ub
Permissions & Licensing Information about reproducing this article in parts (figures, tables) or
in its entirety can be found online at:
http://www.aappublications.org/site/misc/Permissions.xhtml
Reprints Information about ordering reprints can be found online:
http://www.aappublications.org/site/misc/reprints.xhtml
Downloaded from www.aappublications.org/news by guest on November 2, 2021Guidance on Completing a Written Allergy and Anaphylaxis Emergency Plan
Julie Wang, Scott H. Sicherer and SECTION ON ALLERGY AND IMMUNOLOGY
Pediatrics 2017;139;
DOI: 10.1542/peds.2016-4005 originally published online February 13, 2017;
The online version of this article, along with updated information and services, is
located on the World Wide Web at:
http://pediatrics.aappublications.org/content/139/3/e20164005
Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
has been published continuously since 1948. Pediatrics is owned, published, and trademarked by
the American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 2017
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.
Downloaded from www.aappublications.org/news by guest on November 2, 2021You can also read