FUNCTIONING PANCREATIC NEOPLASMS - Gregory Kaltsas MD FRCP EKPA-LAIKO ENETS Center of Excellence - OncologyPRO
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
FUNCTIONING PANCREATIC NEOPLASMS
Gregory Kaltsas MD FRCP
EKPA-LAIKO ENETS Center of Excellence
Endocrinology Unit
National University of Athens
Greece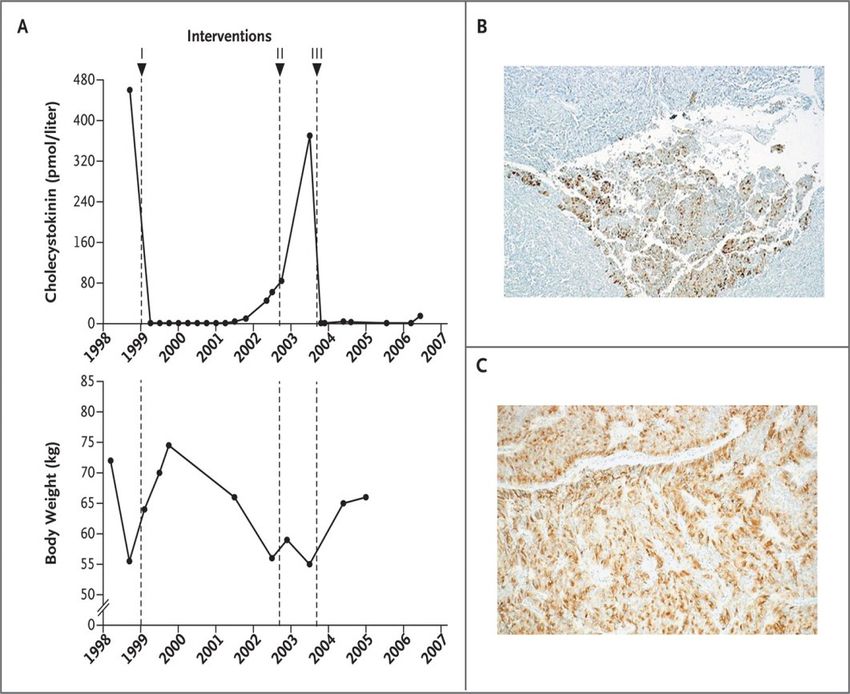
DISCLOSURE OF INTEREST Honorarium : IPSEN Departmental Research Grants: IPSEN, NOVARTIS, PFIZER, SHIRE, SANOFI

CLINICAL PRESENTATION OF COMMON FUNCTIONING PANNENS :
PRODUCING DISTINCT CLINICAL SYNDROME
SSAs first line treatment: Gastrinomas, VIPomas,
Glucagonomas, Insulinomas, ACTH secreting NETs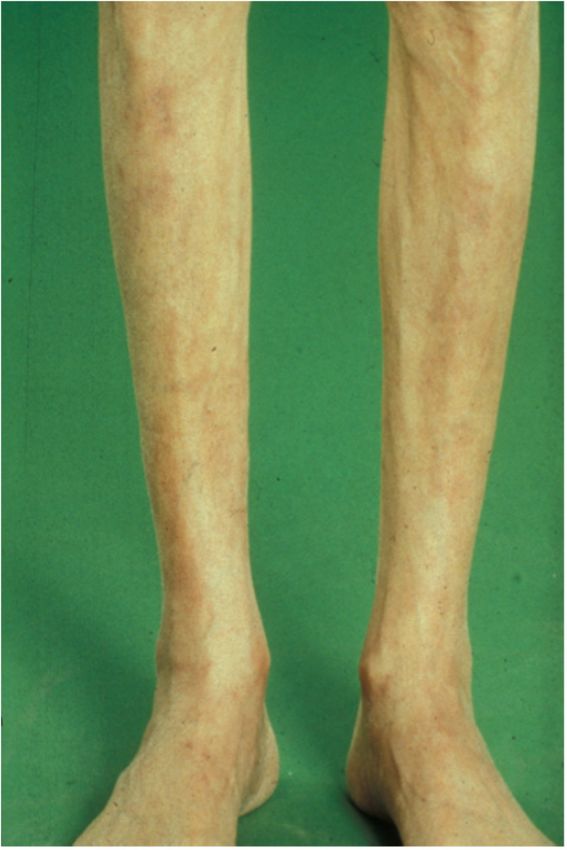
INSULINOMA : WHIPPLE’S TRIAD
SYMPTOMS and SIGNS TUMOR DISTRIBUTION
Neuroglycopenia
- Mild personality changes
- Confusion
- Seizures
Whipple’s Triad
- Coma Symptoms of low glucose
Low plasma glucose
Resolution with glucose
Catecholamine excess Other symptoms normalization
- Diaphoresis - Hunger
- Pallor - Fatigue
- Tachycardia - Nausea, Vomiting
- Peripheral neuropathy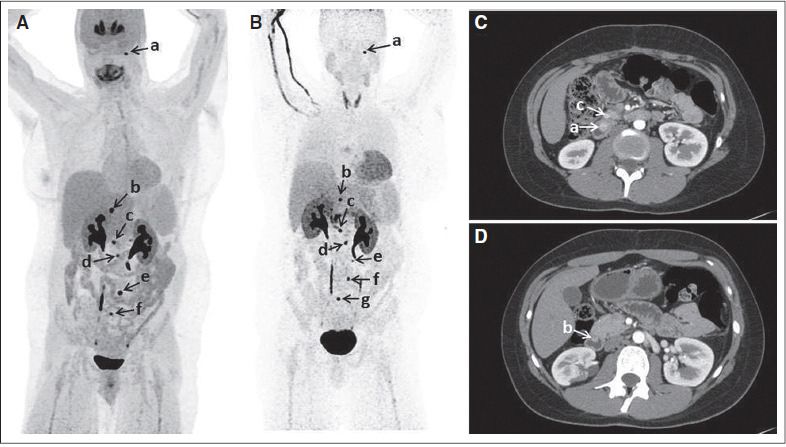
INSULINOMA
• Rare tumor (4 per million per year), mostly ‘benign’
• Whipple’s triad
• Biochemical Diagnosis
• Provocation testing
Concurrent measurement: Glucose, Insulin, C-peptide
Plasma/urine sulphonylurea screen
• Localization (almost always in the pancreas)
• Non-invasive vs. invasive
• Structural vs. functional
• Cross-sectional imaging techniques (CT/MRI)
• Endoscopic ultrasound
• Calcium stimulation study
• GLP1-radionuclide imaging (vs. SRS)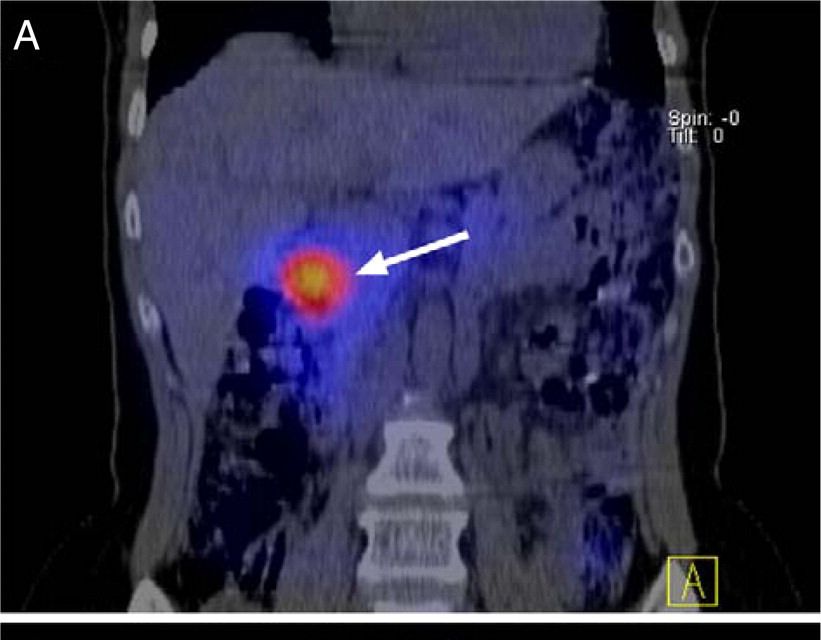
FUNCTIONING PANCREATIC NENS
HYPOGLYCEMIA : DIAGNOSIS AND DIFFERENTIAL DIAGNOSIS
Review history, examination and lab data for specific disorders
Exclude critical illness, surgery, hormone deficiencies (GH, Cortisol), non-islet cell tumors
(Big IGFII), factitious
Consider use of provocation testing
Prolonged supervised fast
Mixed meal test, OGTT (subset of patients post-prandial hypoglycaemia)
Controversy regarding hypoglycaemia threshold
Glucose 5.0 pmol/L
Consider post-glucagon glucose > 25mg/dl & β hydroxybutyrate < 2.7 mmol/L
JCEM 2009, 94:709-728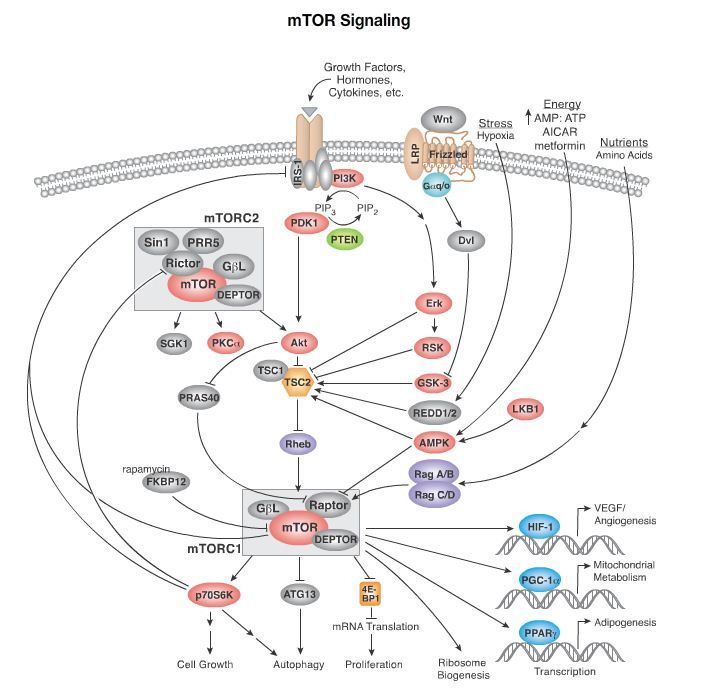
Endo Society, 2012
GLP-1 RADIONUCLEAR IMAGING
AVCS: USE OF CALCIUM OR SECRETIN TO LOCALISE
INSULINOMAS AND GASTRINOMAS
World J Surg 2006 30 1-111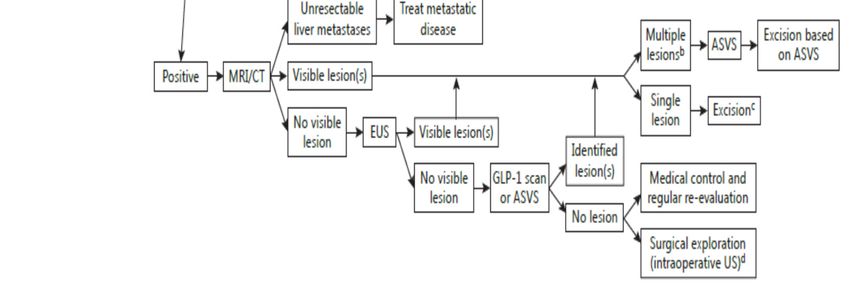
DIAGNOSTIC WORK-UP FOR HYPOGLYCEMIA SECONDARY TO AN INSULINOMA ENETS Neuroendocrinology, 2016; 103:153-171
INSULINOMA MEDICAL TREATMENT : INSULIN SECRETING
PATHWAYS
Closes ATP-sensitive K
channels
Opens ATP-sensitive K
channels
SSA’sMEDICAL TREATMENT OF INSULINOMAS
Frequent meals high in carbohydrate
Somatostatin analogs (test dose octreotide
or SRS as low sstr expression)
Diazoxide (50-300mg, max up to 600 mg)
Edema, hirsutism, RF
GH & glucocorticoids
◦ Multiple side effects
Glucagon
Verapamil, phenytoin, β blockers
◦ Not proven efficacy
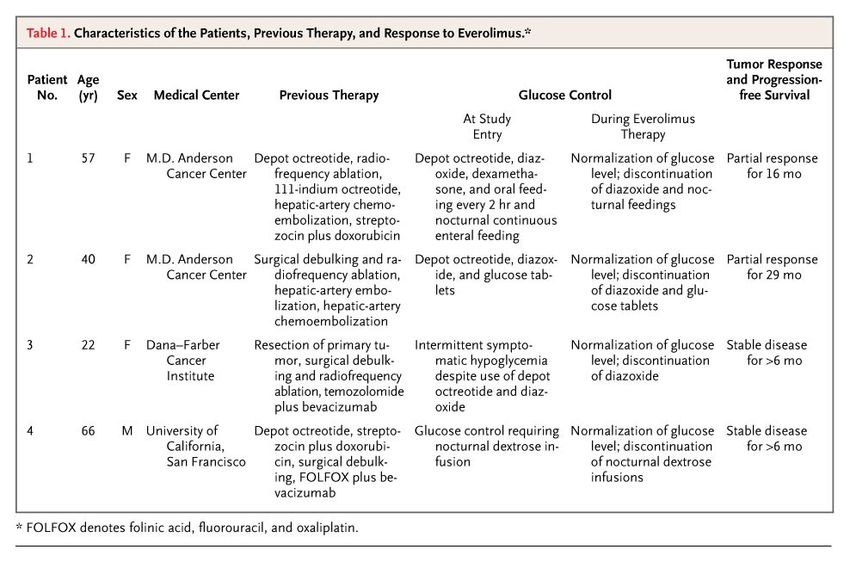
Everolimus (malignant insulinomas)
PasireotideEFFICACY OF 90YDOTATOC IN MALIGNANT INSULINOMA
315 mCi/4cycles Baseline 1 year
480 Gy to tumour
CT-scan
Volume: 22 cc Volume: 3 cc
OctreoScan111™
Uptake: 1.23 ID% Uptake: 0.23 ID%
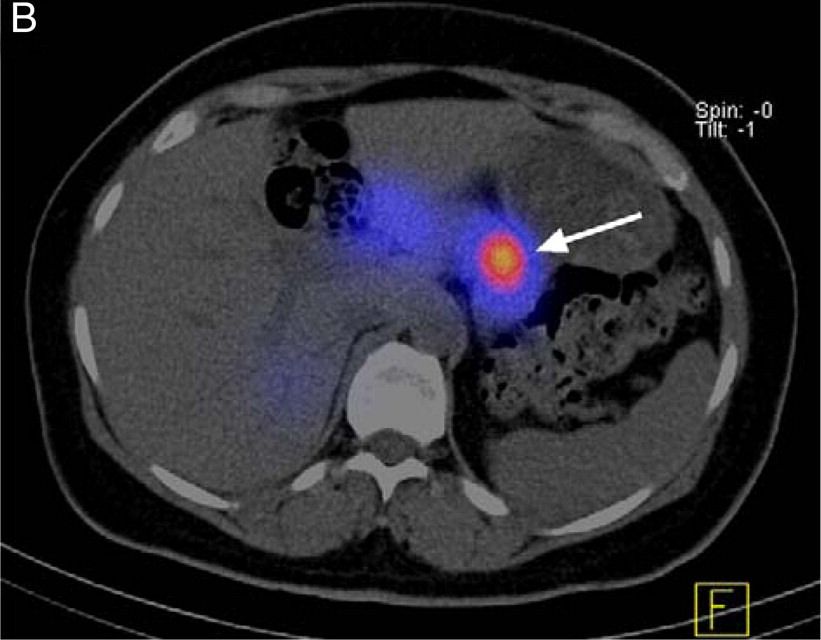
Bushnell et al. JCO 2010INSULIN RESPONSE TO 177LU-DOTATATE IN
MALIGNANT INSULINOMA
Ong et al. EJE 2010GASTRINOMAS : SPORADIC OR MEN 1 RELATED
Gastrinomas: Regulation of gastric acid
secretion
FUNDUS
PGE2 & I2 Nervous system
Gastric gland
H+ H+
H+
ANTRUM BODY
Histamine ECL cells
Parietal cells
G cell
D cell
Gastrin
Somatostatin
Majority of gastrinomas are found in the duodenumGASTRINOMA DIAGNOSTIC ISSUES
FSG > 10 X & PH < 2 facilitate diagnosis
60% gastrinomas do not fulfil these criteria and need
40% secretin test
Secretin test under supervision with PPI
discontinuation
ENETS Neuroendocrinology, 2016; 103:153-171GASTRINOMAS : ZOLLINGER – ELLISON SYNDROME
MEDICAL THERAPY
PPIs (40-80 mg omeprazole)
± H2 blockers
SS analogs
CCK-B antagonists
25-30% MEN1
Hypercalcemia
Titration to reduce acid hyper-secretionGLUCAGONOMA Glucagonoma (3%) Characteristic clinical presentation Many NF panNEN stain glucagon Somatostatin analogs Correct hypoaminoacidemia & mineral deficiency Antibiotics LMWH: risk thrombosis
RESPONSE OF GLUCAGONOMA RASH TO OCTREOTIDE
VIPOMA VIPoma Vigorous rehydration Somatostatin analogs Diarrhea with low osmotic gap < 50mOsm/Kg (>700ml/D) Hyperglycemia, hypercalcemia Repletion of fluid electrolytes (>350mEq/d K) Ringer Lactate (↑ HCO3) SSA (doses of up 500mcg/h) Glucocorticoids (60 mg/d)
PANNETS: ALTERATION OF FUNCTIONAL STATUS
3-6% panNENs multiple hormones obscuring clinical phenotype
Alterations functional status
Non-functioning Functioning
Functioning Change secretory component
Meta-chronous hormonal secretion
15/435 panNENs (3.4%)
Insulin, VIP
Ki-67 LI
Reduced median survival
De Mesier et al 2015
Crona et al 2016FUNCTIONING PANNETS : PRODUCING CLINICAL
SYNDROME
Pancreatic NETs (F-panNENs)
Gastrinomas and insulinomas
Rare F-pNETs (>100 cases)
VIPoma, Glucacagonoma, GRFoma, ACTHomas, panNETs causing CS
PTHrPomas, Somatostatinomas
Very rare F-pNETs (1-5 cases)
Renin, LH, EPO, IGF-II, CCK (CCKoma)
p-NETs secreting Ct, Neurotensin, PP, Ghrelin
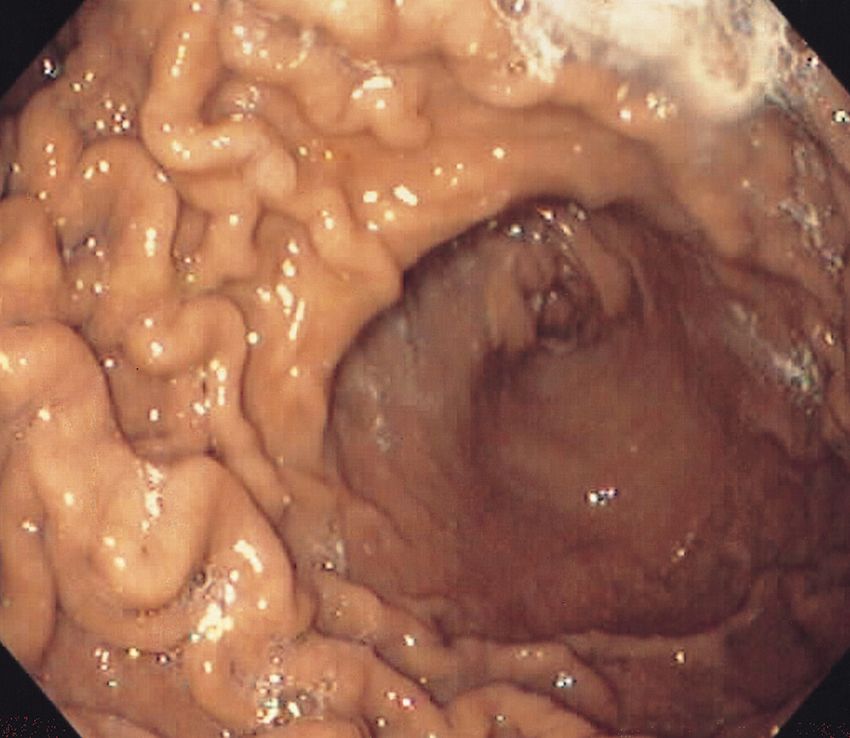
CCKoma: Watery diarrhea, weight loss, gallbladder disease, PGomas, SSomas, EPO
peptic ulcer and normal gastrin level, NEJM 2013, 368:1165 JCO 2013, 31:1690-1698DURATION OF FASTING
127 patients with proven insulinoma
NIH cohort 1970-2000
62% female, 37% male
84% benign, 16% malignant, 12% MEN1
NIH Protocol NIH
Fast until glucose 40 mg/dL (2.2 mmol/L) 48 hours sufficient to demonstrate all cases of
with neuroglycopaenia hypoglycaemia and to obtain concurrent samples
for insulin / proinsulin and related peptides
Mayo clinic
66.9% hypoglycaemic within 24 hours Concur but 72 hours necessary to demonstrate
94.5% concluded within 48 hours suppression of beta-cell peptides in the absence
7 patients continued fast beyond 48 hrs of hypoglycaemia (ie the demonstration of normal
Retrospective data review : biochemistry).
Biochemical criteria fulfilled in all inJCEM 2006, 91(12):4733-6
You can also read

















































