Granular parakeratosis secondary to benzalkonium chloride exposure from common household laundry rinse aids
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
CLINICAL CORRESPONDENCE
Granular parakeratosis
secondary to benzalkonium
chloride exposure from
common household
laundry rinse aids
Catherine JL Tian, Diana Purvis, Harriet S Cheng
ABSTRACT
AIM: Granular parakeratosis (GP) is a benign dermatosis characterised by a rash at intertriginous sites.
The pathogenesis is uncertain although it is proposed to be an irritant contact reaction with cases
related to benzalkonium chloride (BAC) reported. Our experience is that patients often have delayed
diagnosis. This study aims to review the clinical presentation and histopathological features of GP.
METHODS: This study is a retrospective case series of adult and paediatric patients seen at dermatology
clinics in Auckland, New Zealand. Information was collected on patient demographics, presentation,
investigations and management.
RESULTS: Thirteen cases (seven adults; six children) are included. The typical presentation of GP was
erythematous or brown, scaly papules and plaques with desquamation in a predominantly flexural
distribution. All patients reported recent exposure to BAC in laundry rinse solution. Nine biopsies were
taken from four patients. Psoriasiform and eczematous findings were common on histopathology. The
mainstay of treatment was cessation of BAC exposure.
CONCLUSION: GP has a distinct clinical pattern although histopathological findings are varied.
Clinicians should have a high index of suspicion for GP in patients presenting with erythematous
flexural eruptions and seek a history of BAC exposure, especially in the context of the COVID-19
pandemic and increased antiseptic use.
G
ranular parakeratosis (GP) is a benign understood. The process is possibly exacer-
skin condition first described by bated by mechanical and chemical irritation,
Northcutt et al in 1991 as pruritic, compounded by occlusive environments.2–4
red or brown, hyperkeratotic papules and In recent years, there has been a greater
plaques confined to one or both axillae of recognition of the association between GP
four patients.1 Since the initial description, and chemical irritants found in antiseptics,
extra-axillary sites of involvement have also especially laundry rinse aids and deter-
been reported. These include the inter- and gents containing benzalkonium chloride
infra-mammary areas, inguinal, groin, peri- (BAC).5,6 BAC is a quaternary ammonium
anal and genital skin, beneath the abdomi- cationic compound used as an antimicrobial
nal pannus and in non-intertriginous sites preservative for a range of applications. It
such as the lumbosacral area.2–4 is active against a wide range of bacteria,
GP is thought to be a consequence of yeasts and fungi, but it is increasingly being
abnormal epidermal differentiation and recognised as a skin irritant.7–9 We have
keratinocyte maturation from the stratum noticed a number of cases of GP in adults
granulosum to the stratum corneum1–3 and children who share a common history
through a pathogenesis that is not yet fully of recent exposure to BAC in laundry rinse
128
NZMJ 30 April 2021, Vol 134 No 1534
ISSN 1175-8716 © NZMA
www.nzma.org.nz/journal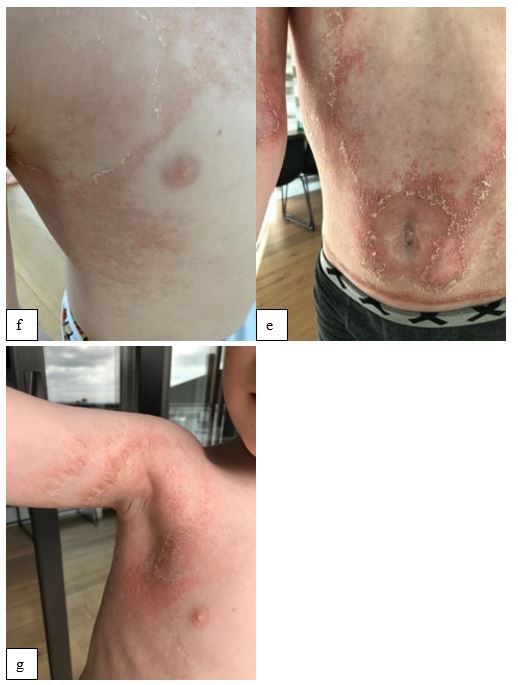
CLINICAL CORRESPONDENCE
solutions commonly found on the New recorded for patients where available. Insti-
Zealand market. tutional approval for the report was granted
Patients with GP often pose as a diag- by the Auckland District Health Board
nostic challenge for clinicians and can Research Office.
have a long period of symptomatology
with multiple presentations and investi- Results
gations prior to correct diagnosis. In the Thirteen cases of GP (seven adults; six
context of increasing use of antiseptics children) are included. Four patients (three
and disinfectants during and beyond the adults; one child) were seen at the Auckland
era of the novel coronavirus (SARS-CoV-2) District Health Board public dermatology
COVID-19 pandemic, we also anticipate the outpatient clinic, and nine patients (four
irritant effects of BAC to be heightened and adults; five children) were seen at a private
that cases of GP will continue to rise. The dermatology clinic in Auckland. The
aim of this study was to draw attention to duration from rash onset to GP diagnosis by
the presentations and course of illness of the dermatologist ranged from two weeks
patients with GP and examine the role of to 18 months. All patients reported recent
BAC as a possible aetiology. exposure to Dettol laundry additive (Reckett
Benckiser, United Kingdom) or Canesten
Methods rinse solution (Bayer, New Zealand), both of
We identified 13 cases of GP in adult and which are laundry rinse aids that contain
paediatric patients who presented to public BAC (content described in Table 1). One child
and private Auckland dermatological clinics (patient five) also had further exposure to
between 2015 to 2020. All diagnoses were BAC in QV Flare Up Cream (Douglas Phar-
made following specialist dermatologist maceuticals Ltd, New Zealand), which was
consultation. Epidemiological data, clinical applied topically after his rash had started,
presentation, investigation results and and this resulted in further exacerbation of
treatment outcomes were collected from his condition.
clinical records, and all patient information Clinical details of the 13 patients are
was de-identified. Skin biopsy findings were summarised in Appendix Table 1. Patient
Table 1: Benzalkonium chloride concentrations in selected products available in New Zealand.
Brand Product name and concentration (selected products containing
benzalkonium chloride)
Dettol • Dettol Anti-bacterial Laundry Sanitiser Eucalyptus: 1.25 litre, con-
(Reckett Benckiser, UK) tains benzalkonium chloride 70g per litre
• Dettol Washing Machine Cleaner Citrus Burst: 250ml, contains ben-
zalkonium chloride 2.25%
• Dettol Washing Machine Cleaner Original: 250ml, contains benzalko-
nium chloride 2.25%
Canesten • Canesten Rinse Solution: 1 litre, contains benzalkonium chloride
(Bayer, New Zealand) 70g per litre
QV series • QV Flare Up Cream: 100g tube, contains benzalkonium chloride 0.1%
(Douglas Pharmaceuticals) • QV Flare Up Bath Oil: 200 and 500ml bottles, each contains benzal-
konium 2.0%
Aveeno (Johnson • Aveeno Dermexa Daily Emollient Cream: 200ml, contains benzalko-
& Johnson Ltd, UK) nium chloride (unspecified percentage)
• Aveeno Baby Dermexa Emollient Cream: 200ml, contains benzalko-
nium chloride (unspecified percentage)
129
NZMJ 30 April 2021, Vol 134 No 1534
ISSN 1175-8716 © NZMA
www.nzma.org.nz/journalCLINICAL CORRESPONDENCE
ages ranged from eight months to 72 years growth. Nine 4mm skin biopsies of the
(median=31 years). Ten of the 13 patients affected areas were taken from four adults:
were of full or partial Asian ethnicity. Six seven of the nine specimens showed typical
patients had a personal (n=5) or family features of parakeratosis, acanthosis and
(n=1) history of atopic or irritant contact mixed dermal inflammatory infiltrates.
dermatitis. One patient also had active None of the nine biopsy specimens showed
psoriasis at the time of diagnosis, which evidence of bacterial or fungal infection
was confirmed histologically. The rashes on serial stains. The most frequent histo-
shared a common theme of erythem- logical diagnoses were dermatitis (eczema)
atous papules and plaques, accompanied or psoriasis. None of the paediatric patients
by varying degrees of desquamation and had skin biopsies performed. Patch testing
scaling (Figures 1 and 2). There was asso- was completed for two patients and both
ciated lichenification (indicating chronicity) were negative for a series of allergens
in eight patients. Four patients reported including BAC, thereby excluding allergic
pruritus. The distribution included the contact dermatitis.
axillae, groin, trunk, limbs, anterior neck Topical preparations (most commonly
and natal cleft. Interestingly, in one patient emollients and mild to moderate potency
the rash was noticed on the helices of the topical corticosteroids) had commonly been
ears. In two patients, the rash was predomi- trialled prior to presentation to the derma-
nantly in a pattern of distribution reflective tologist’s clinic, and systemic therapies,
of areas of close contact with clothing or such as broad-spectrum antibiotics or anti-
fabric (neckline, nappy and waistband). fungals, had also been prescribed in some
Blood tests were done on six patients and cases. These yielded variable responses.
did not reveal any systemic involvement. At the time of diagnosis, patients were
Skin scrapings were taken from six patients advised to avoid further contact with BAC
and all yielded skin flora of insignificant and rewash clothing without the BAC-con-
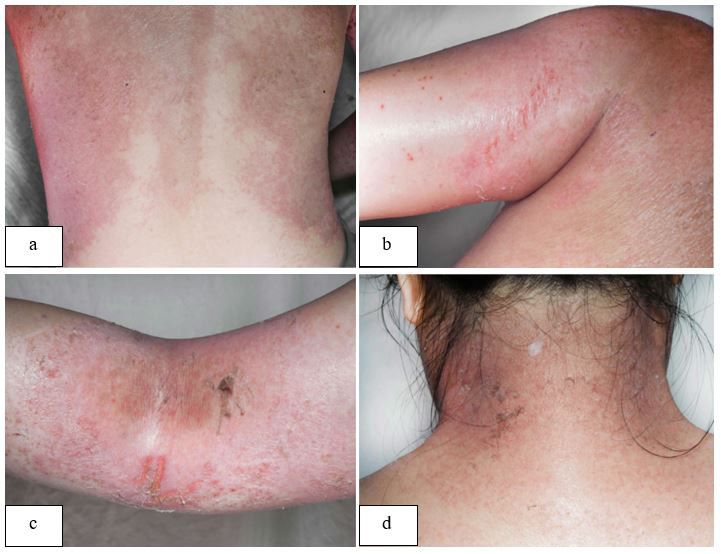
Figure 1: Granular parakeratosis in an adult. Close up of the back and left axilla, showing an erythem-
atous rash with areas of hyperkeratosis at the peripheries of the eruption (a, b). Hyperkeratosis and fis-
suring in the left elbow flexure (c). Hyperpigmentation, fissuring and desquamation at the neckline (d).
130
NZMJ 30 April 2021, Vol 134 No 1534
ISSN 1175-8716 © NZMA
www.nzma.org.nz/journalCLINICAL CORRESPONDENCE
Figure 2: Granular parakeratosis in a child. Clinical photography showing the morphology and distribu-
tion of the erythematous and brownish hyperkeratotic papules and plaques, around the umbilicus (e),
in the front of the torso and axilla (f, g).
131
NZMJ 30 April 2021, Vol 134 No 1534
ISSN 1175-8716 © NZMA
www.nzma.org.nz/journalCLINICAL CORRESPONDENCE
taining laundry rinses. Follow-up data were may be abnormal processing of profil-
available for five cases, all of which reported aggrin to filaggrin (structures that maintain
improvement or resolution of skin rash the keratohyalin granules in the stratum
following cessation of BAC exposure. corneum during cornification).1–3 Physical
factors such as hyperhidrosis, obesity and
Discussion friction are also thought to contribute to
the evolvement of GP via chemical and
The clinical features in our 13 patients fit
or mechanical irritation, resulting in
well with the characteristic appearance of
compromised epidermal maturation and
GP described in published literature.1,3,9–12
barrier function.2,5,10 A humid and occlusive
Hyperkeratotic papules on an erythem-
environment, commonly found in cuta-
atous or brown base, often coalescing
neous folds, may exacerbate penetration
into plaques in a predominantly flexural
of irritants into the skin, which possibly
distribution, are characteristic. Non-inter-
explains the predominantly intertriginous
triginous involvement of the lumbosacral
distribution.2,4,13,14 Five of our patients also
area, abdomen, limbs, face and neck was also
had atopic dermatitis, which is a spec-
noted in our cases. Involvement of the helices
ulated risk factor for GP, as epidermal
of the ears has not previously been reported
barrier dysfunction in atopic dermatitis
and we postulate that this may be related to
may also facilitate increased penetration
site of contact with traces of BAC on bedding.
of irritants.13,15 The skin microbiome
GP has been described in all ages and is also important in mediating various
both sexes, although it is more commonly processes involving immune responses
reported in females.9–11 In our series, the age and epidermal development and differen-
of our patients at time of rash onset ranged tiation.16 Previous studies have commented
widely from eight months to 72 years and on how, in response to internal or external
just over half of cases were in females (7/13, factors, altered skin microbial communities
54%). Interestingly, 10/13 (77%) of our cohort contribute to the disease pathology of a
were of full or partial Asian ethnicity. To the number of cutaneous conditions including
best of our knowledge, the occurrence of GP acne, atopic dermatitis and psoriasis.17
has not previously been described to have a Perhaps akin to the hypothesis of atopic
particular geographical or racial predilection. dermatitis being associated with a loss of
Our finding may reflect local cultural prac- microbiome diversity secondary to over-
tices related to laundry and hygiene. abundance of cutaneous Staphylococcus
There are many histopathologic variants aureus,18 Kumarasinghe et al postulate that
of GP,11 with the most common findings flexural hyperkeratotic lesions such as GP
being hyperkeratosis, parakeratosis, could be triggered by an overgrowth of flora
epidermal acanthosis and hypergranu- with a predominance of anaerobes.19 In
losis.2,3 Mild to moderate capillary dilatation, recent years GP has also been reported in
proliferation of the upper papillary dermis association with chemotherapy for ovarian
and scattered perivascular inflammatory and breast carcinoma, as well as several
lymphohistiocytic infiltrate are also keratinocytic neoplasms.9,20,21
described.3,10,11 Some histological features Of the contact irritants that may
may overlap with psoriasis, and many of our contribute to development of GP, BAC is most
cases also had spongiosis in the epidermis, widely reported.5,7–9,22,23 BAC, an ammonium
which is classically seen in dermatitis compound commercialised for more than 50
(eczema). Of note, eczema and psoriasis years, is used as an antiseptic and preser-
were common histological misdiagnoses in vative7,23 across a wide range of applications
our series. We propose that GP is unlikely commonly found on the New Zealand
to be diagnosed on histopathology alone; in market, including but not limited to eye
most cases, GP should be a clinical diagnosis. drops, bath oils, skin cleansers, sanitisers
The precise aetiology and triggers of GP and laundry rinse aids. These are alternative
remain uncertain at present. Microscopic names for BAC:
studies showing decreased cytoplasmic • N-Alkyl-N-benzyl-N
expression of filaggrin during cornification
• N-dimethylammonium chloride
suggests that the primary underlying cause
132
NZMJ 30 April 2021, Vol 134 No 1534
ISSN 1175-8716 © NZMA
www.nzma.org.nz/journalCLINICAL CORRESPONDENCE
• Alkyldimethylbenzylammonium Australian Baseline Series (ABS). Prolonged
chloride exposure to BAC can potentially predispose
• ADBAC individuals to sensitisation and induce
allergic contact dermatitis.5,7,10,24
• BC50
The Environmental Protection Authority
• BC80
(EPA), a Crown Agent established in 2011,
• Alklbenzyldimethyl regulates BAC in New Zealand. The EPA
• Alkyl benzyldimethyl ammonium categorises BAC of different concentrations
chloride (>33%; >5–25%; >1–5%) into classification
• Ammonyx codes as per the Hazardous Substances and
New Organisms Act 1996. All businesses
• Barquat MB-50
selling goods containing chemicals must
• Barquat MB080 apply for hazardous-substances approval
• Benirol from the EPA, provide an accessible chem-
• Bradophen ical-safety data sheet and comply with
• BTC labelling in accordance with the hazards
of the particular chemical concentration.
• Cequartyl
As per the EPA’s most recent reassessment
• Drapolene of BAC in June 2020, BAC at all concentra-
• Dropolex tions is not classified as a skin sensitiser.
• Enuclene This means that in New Zealand there
is no mandatory requirement for goods
• Germitol
containing BAC to display any labelling
• Gesminol to warn consumers of potential irritant
• Osuan or sensitisation effects. There is currently
• Paralkan no limit on BAC concentration in cleaning
products, although for products directly
• Parasterol
in contact with skin, the EPA limits BAC
• Quaternary ammonium compounds content to 3% in hair products and 0.1% in
rodalon other cosmetics, such as hand-sanitisers. In
• Zephiran light of an increasing awareness of BAC’s
• Zephiran chloride irritant properties and association with GP,
we hence propose closer surveillance and
• Zilkonium chloride
an updated review of BAC at its various
Robinson et al described GP in a suscep- commercially available concentrations, with
tible subset of patients following exposure to a particular focus on cleaning products and
laundry wash containing BAC; 5 and a paedi- other common household solutions and
atric case study in Brazil reported six cases their potential role in dermal irritation or
of GP following exposure to commonly used sensitisation.
infant skincare products containing BAC.14
There is currently no optimal or stan-
In our series, all patients reported use of a
dardised approach to treatment for GP.
laundry rinse containing BAC prior to devel-
There is also a paucity of high-quality
opment of the rash. BAC is thought to irritate
evidence and controlled trials. According to
the skin by disrupting cellular epidermal
our experience and other reports, treatment
lipid bilayers and promoting inflammatory
in the form of topical and systemic corti-
cell infiltration, leading to activation of
costeroids, retinoids, vitamin D analogues
leucocytes, granulocytes, inflammatory
(eg, calcipotriene), keratolytics (such as
proteins and cytokines (tumour necrosis
salicyclic acid and ammonium lactate), anti-
factor-alpha, prostaglandin E2, interleuk-
fungals and antimycotics are all of variable
ins-1a, -1b, -6, and -8).7,8,22 As an antiseptic,
efficacy.15,25–27 Recently, the use of broad-
BAC may also contribute to disease
spectrum oral antibiotic therapy has been
pathology by means of inducing changes
reported, with the proposed mechanism
to resident microbiome populations and
being modification and correction of the
disrupting skin homeostasis. Although less
skin microbiome.19 However, this therapy
frequently reported as a sensitiser, BAC
was trialled in two of our cases without
is also listed as a contact allergen on the
133
NZMJ 30 April 2021, Vol 134 No 1534
ISSN 1175-8716 © NZMA
www.nzma.org.nz/journalCLINICAL CORRESPONDENCE
noticeable improvement. The use of neuro- or Letterer–Siwe disease.12,13 Clinical and
toxin Clostridium botulinum type A has been investigative findings, histopathological
described in patients who also suffer from subtleties, as well as limited or no response
hyperhidrosis;29 and destructive procedural to targeted treatment(s) will help differen-
treatments such as cryotherapy, YAG and tiate these from GP.
carbon dioxide lasers are also reported.30 This report is a retrospective case series,
Many patients demonstrate spontaneous which makes it difficult to prove causality.
improvement, although the course of the Only two of our patients received formal
eruption varies from several weeks to skin patch testing to exclude an allergic
years.3,4 In general, we consider general contact dermatitis; however, we consider
skin cares, withdrawal of BAC-containing patch testing to be unnecessary in most
laundry rinses, and avoidance of irritants to cases where the clinical presentation is clas-
be the mainstay of treatment. sical as GP arises from irritant rather than
The variability in time from rash onset allergic mechanisms. Patch testing should be
to diagnosis of GP in our cases (two weeks reserved for patients who do not respond to
to 18 months) may be reflective of the lack avoidance of BAC and other irritants.
of familiarity with this condition among
clinicians locally and perhaps even inter- Conclusion
nationally. Of the 363,343 skin biopsies
Our case series describes the development
from flexural dermatoses submitted by
of GP in a cohort of patients exposed to BAC
dermatologists at a large institute of derma-
via laundry rinses and provides further
topathology in New York, the frequency of
evidence for the hypothesis that GP is an
GP on histology was 0.005% (18 of 363,343),
irritant contact reaction pattern with BAC
with only one correct clinical diagnosis
as a likely culprit. Our experience is that
in the 18 histologically confirmed cases of
patients often have delayed diagnosis. We
GP.11 Similarly, Braun Falco and colleagues
advocate that healthcare professionals
found histopathological features of GP in
maintain clinical suspicion for GP when
ten of 250,000 skin biopsies (0.004%), but
encountering patients presenting with
GP had not been considered as a clinical
flexural dermatoses, and a history of recent
diagnosis in any of the ten cases.10 Our cases
exposure to BAC should be specifically
demonstrated that histopathology is rarely
sought. We anticipate this to be particularly
definitive in GP, which may lead to alter-
relevant in the context of the COVID-19
native diagnoses being sought, contributing
pandemic and an anticipatory increased
to further diagnostic delay.
use of antiseptics. Heightened awareness
The differential diagnoses of inter- of GP results in a more-timely diagnosis
triginous rashes are broad and include with reduced medical visits, investigations
seborrhoeic dermatitis, irritant or allergic and unnecessary therapies. Clinical diag-
contact dermatitis, acanthosis nigricans, nosis is usually possible, and biopsy should
Hailey–Hailey disease, Darier’s disease, only be considered to exclude differential
pemphigus vegetans, candidiasis, derma- diagnoses in selected cases. We propose
tophytosis, flexural drug eruptions and that the mainstay of treatment remains as
Dowling–Degos disease.3,9–11 In the paediatric identification and removal of skin irri-
population, differentials also include napkin tants including BAC, in combination with
dermatitis, acrodermatitis enteropathica, emollients.
134
NZMJ 30 April 2021, Vol 134 No 1534
ISSN 1175-8716 © NZMA
www.nzma.org.nz/journalCLINICAL CORRESPONDENCE
Appendix
Appendix Table 1: Characteristics of patients presenting with granular parakeratosis.
Case Age Gender / Medical Presentation Investigations Histology Treatment Progress
Ethnicity history (4mm skin biopsy)
1* ++ 8 Male, Asian Infantile 6-month history worsening • No investigations. Clinical No skin biopsy Emollient and No follow-up data
months eczema, eczema on face and limbs since diagnosis potent topical available.
seborrheic 2 months of age. More recently corticosteroid.
dermatitis developing rash: red brown Advised to avoid
plaques on upper thighs sparing BAC and rewash
the folds. clothes.
2++ 10 Female, Irritant and Several months history of • PCR: Herpes simplex and No skin biopsy Topical pimecro- No response to
months New periorificial erythematous, peeling rash Varicella zoster negative limus. Vaseline topical steroids. No
Zealand dermatitis of in the groin mirroring contact • Skin swab right thigh: as barrier cream. complete follow-up
European face, infantile with nappies, sparing inguinal normal flora Advised to avoid data available.
haemangi- creases. Facial eruption with BAC and rewash
oma papules around eyes, nose and nappies.
mouth (concurrent diagnosis of
periorificial dermatitis).
3++ 4 years Female, None Several months history of red/ • Skin scraping groin: no No skin biopsy Emollient and No response to
Asian reported brown exfoliative symmetrical fungus moderate potency topical steroid or
groin rash. topical steroid antifungals. De-
and antifungal. spite advice contin-
Advised to avoid ued to use laundry
BAC and rewash rinse with BAC and
clothes. rash persisted.
Advice re-enforced
on follow-up and
rash resolved.
135
NZMJ 30 April 2021, Vol 134 No 1534
ISSN 1175-8716 © NZMA
www.nzma.org.nz/journalCLINICAL CORRESPONDENCE
Appendix Table 1: Characteristics of patients presenting with granular parakeratosis (continued).
Case Age Gender / Medical Presentation Investigations Histology Treatment Progress
Ethnicity history (4mm skin biopsy)
4+ 6 years Male, New Molluscum 16-month history bran-like scal- • Skin autoantibodies No skin biopsy Emollient, 10% Limited improve-
Zealand contagiosum. ing on an erythematous base. negative. urea as kerato- ment with topical
European Atopic ecze- Rash is pruritic and scattered • Plasma zinc; glucagon; lytic and mild to creams. Rash
ma (mother) pustules noted. Originated from amino acids; ANA, iron moderate potency resolved at time
and asthma neck, spreading to face, chest, studies; liver function, topical corticoste- of clinic follow up.
(father) groin and legs. Rash later re- coeliac markers, thyroid roid. Diagnosis of GP
curred as erythematous plaques function, immunoglobu- made retrospec-
in the groin, with a well-defined lin, B12/folate normal, tively.
peeling edge. Sister (9years) also • Urine: amino acid and
had a milder scaly rash around organic acid screen neg-
the neck and forearms. ative.
• Skin scraping neck: no
fungus
• Skin prick and patch test:
No reaction (house dust
mite, cat, dog, Alternaria,
aspergillus, mixed grass,
perennial rye, plantain,
birch mix, soyabean, cow’s
milk, egg white, peanut,
wheat, shrimp, fish mix).
Open application to zinc
oxide sunscreen negative.
136
NZMJ 30 April 2021, Vol 134 No 1534
ISSN 1175-8716 © NZMA
www.nzma.org.nz/journalCLINICAL CORRESPONDENCE
Appendix Table 1: Characteristics of patients presenting with granular parakeratosis (continued).
Case Age Gender / Medical Presentation Investigations Histology Treatment Progress
Ethnicity history (4mm skin biopsy)
5++ 9 years Male, New Infantile 3-month history dry, irritated • Skin scraping axilla: no No skin biopsy Emollient and Improved at 4
Zealand eczema eruption. Started in axillae, fungus advised to avoid weeks
European spread down sides of torso, onto • Skin swab: normal flora BAC and rewash
back and behind knees. No re- clothes.
sponse to topical antifungals or
topical corticosteroids. Exposed
to Canestan laundry rinse for
several years, QV flare up cream
used after eruption started,
making rash worse.
6++ 11 years Male, Childhood 12-month history worsening • No investigations. Clinical No skin biopsy Emollient and No follow-up data
Chinese eczema eczema. Superficial brown, diagnosis potent topical available.
European desquamating rash around corticosteroid.
waistband of underwear and Advised to avoid
trousers. BAC and rewash
clothes.
7++ 31 years Female, None report- 4-week history reticulate erythe- • No investigations. Clinical No skin biopsy Emollient, potent Did not attend for
Asian ed ma and scaling over lower ab- diagnosis topical cortico- planned follow up.
dominal wall, confluent in groin steroid and oral
and on buttocks. Later spreading loratadine for
to face and helix of ears, then pruritus. Advised
arms and hands. to avoid BAC and
rewash clothes.
8++ 32 years Female, None report- 18-month history peeling skin • No investigations. Clinical No skin biopsy Emollients, Noticed im-
Chinese ed with subtle hyperpigmentation diagnosis salicylic acid ker- provement after
in the axillae, hips and forearms. atolytic and mild stopping laundry
potency topical rinse. Recurrence
corticosteroid. after wearing yoga
Avoid soap and clothes which
BAC and rewash had not been
clothes. rewashed.
137
NZMJ 30 April 2021, Vol 134 No 1534
ISSN 1175-8716 © NZMA
www.nzma.org.nz/journalCLINICAL CORRESPONDENCE
Appendix Table 1: Characteristics of patients presenting with granular parakeratosis (continued).
Case Age Gender / Medical Presentation Investigations Histology Treatment Progress
Ethnicity history (4mm skin biopsy)
9++ 34 years Male, Asian None report- 2-month history progressive • Skin autoantibodies Skin biopsy left cubital Emollient and Rash resolved at
ed eruption abdomen, groin, negative fossa and groin: Features advised to avoid follow up.
antecubital and popliteal fossae, • Renal and liver function of dermatitis with ortho- BAC and rewash
genitalia and axillae. Progressed normal keratosis, parakeratosis clothes.
to involve trunk. Mild erythema • QuantiFERON TB Gold, and mild spongiosis.
with brown bran-like scale. HIV and hepatitis screen Perivascular and inter-
Widespread xerosis. No pruritus. negative / stitial chronic inflamma-
• Skin scraping left thigh: no tory infiltrate in dermis,
fungus including occasional
• Skin swab left axilla: nor- eosinophils.
mal flora
• Patch testing: BAC neg-
ative
10+ 36 years Female, 25/40 preg- 6-week history rapidly evolving • QuantiFERON TB Gold, HIV Skin biopsy back, forearm Admitted as Improved after
Chinese nant, pustu- peeling rash torso and groins antibody and trepone- and thigh: Psoriasiform inpatient given cessation of BAC.
lar psoriasis associated with flare of pustular mal antibodies negative, features with parakerato- concurrent Discharged once
psoriasis. Concurrent diagnosis skin autoantibodies not sis and neutrophils within diagnosis of stable and pustules
of GP and pustular psoriasis of detected parakeratotic scale. pustular psoriasis. cleared.
pregnancy. • Skin scraping right arm: Underlying superficial Treatment with
no fungus perivascular lymphocytic moderate potency
inflammatory infiltrate topical corticoste-
with occasional eosino- roid, emollients
phils. and ciclosporin.
Advised to avoid
soap and BAC
and to rewash
clothing.
138
NZMJ 30 April 2021, Vol 134 No 1534
ISSN 1175-8716 © NZMA
www.nzma.org.nz/journalCLINICAL CORRESPONDENCE
Appendix Table 1: Characteristics of patients presenting with granular parakeratosis (continued).
Case Age Gender / Medical Presentation Investigations Histology Treatment Progress
Ethnicity history (4mm skin biopsy)
11+ 42 years Female, None report- 2-week history itchy and painful • Iron, FBC, liver, renal and Skin biopsy left axil- Emollient and No follow-up data
Chinese ed rash originating in groins. Ery- thyroid function normal. la, abdomen, breast: soap substitute. available.
thematous, fissured and scaly QuantiFERON TB Gold, Features of impetiginised Advised to avoid
papules coalescing into plaques. HIV antibody, hepatitis B dermatitis and/or subcor- BAC and rewash
Rash later spread to become and C antibodies negative. neal pustulosis with mild clothes.
symmetrical, well-demarcated ANA; ANCA; plasma zinc; acanthosis, parakeratosis
areas of desquamation and and skin autoantibodies and spongiosis. Mounds
hyperpigmentation on anterior negative / of parakeratosis contain
and posterior trunk, including • Skin scraping groin: no numerous neutrophils.
breasts. fungus Perivascular mixed
• Skin swab left knee infiltrate in dermis.
pustule: Staphylococcus Differentials include
aureus impetiginized eczema-
• Skin swab groin: normal tous reaction, a form of
flora, no yeast isolated psoriasis or subcorneal
neutrophilic dermatosis.
12++ 67 years Female, Childhood 6-month history painful dry rash ANA and RF negative. Skin biopsy left chest: Moderate potency Incomplete re-
Indian eczema, originating from right axilla. B12, folate and FBC normal Features of dermatitis topical corticoste- sponse to topical
allergic rhini- Asteototic plaques with erythe- with mild spongiosis and roid; oral erythro- steroid and anti-
tis, salicylate ma and lichenification affecting compact parakeratosis in mycin 2 weeks (al- biotics. Follow-up
sensitivity bilateral axillae, sub-mammary epidermis with super- lergy to penicillin). pending.
and multiple fold and groin. Not pruritic. ficial perivascular lym- Advised to avoid
drug allergies phohistiocytic infiltrate. BAC and rewash
Scattered lymphocytes clothing.
at dermoepidermal junc-
tion without basement
membrane destruction
or keratinocyte vacuo-
lation. Common pattern
occurring as a cutaneous
reaction to drugs
139
NZMJ 30 April 2021, Vol 134 No 1534
ISSN 1175-8716 © NZMA
www.nzma.org.nz/journalCLINICAL CORRESPONDENCE
Appendix Table 1: Characteristics of patients presenting with granular parakeratosis (continued).
Case Age Gender / Medical Presentation Investigations Histology Treatment Progress
Ethnicity history (4mm skin biopsy)
13+ 72 years Male. Asian Congestive 1-year history hyperpigmented, QuantiFERON TB Gold, HIV, No skin biopsy Topical and oral Incomplete re-
heart failure, dry rash in axillae with general- hepatitis B&C screen negative steroid therapy, sponse to topical
type 2 diabe- isation to involve the popliteal Skin autoantibodies negative antifungals, and or oral steroid ther-
tes mellitus, and antecubital fossae; anterior course of roxithro- apies; antifungals;
hypertension abdominal wall and natal cleaft/ mycin. Emollient or antibiotics. No
groin. Well-demarcated, xerotic, and soap substi- complete follow-up
hyperpigmented plaques with tute. Advised to data available.
fissures, peeling and scale. Initial avoid bleach and
diagnosis of seborrhoeic derma- BAC and rewash
titis, treated with itraconazole clothes.
which precipitated liver dysfunc-
tion and uncovered diagnosis of
hepatocellular carcinoma.
*Telehealth consultation during COVID-19 lockdown.
+ Seen in public.
++ Seen in private.
ANA (antinuclear antibodies); RF (rheumatoid factor); ANCA (antineutrophil cytoplasmic antibodies); HIV (human immunodeficiency virus); FBC (full blood count).
140
NZMJ 30 April 2021, Vol 134 No 1534
ISSN 1175-8716 © NZMA
www.nzma.org.nz/journalCLINICAL CORRESPONDENCE
Competing interests:
Nil.
Author information:
Dr Catherine JL Tian: House Officer (Doctor),
Auckland District Health Board, Auckland, New Zealand.
Dr Diana Purvis: Dermatologist, Department of Dermatology,
Auckland District Health Board and University of Auckland, Auckland, New Zealand.
Dr Harriet S Cheng: Dermatologist, Department of Dermatology,
Auckland District Health Board and University of Auckland, Auckland, New Zealand.
Corresponding author:
Dr Harriet S Cheng, Department of Dermatology, Auckland District Health Board,
Private bag 92189, Auckland Mail Centre, Auckland 1142, (09) 367 0000
harrietc@adhb.govt.nz
URL:
www.nzma.org.nz/journal-articles/granular-parakeratosis-secondary-to-benzalkonium-chlo-
ride-exposure-from-common-household-laundry-rinse-aids
REFERENCES
1. Northcutt AD, Nelson 6. Tartari F, Vincenzi C, correlation of 10 cases.
DM, Tschen JA. Axillary Di Altobrando A, et al. J Dtsch Dermatol Ges.
granular parakeratosis. Allergic contact dermatitis 2009 Apr;7(4):340-
J Am Acad Dermatol. to benzalkonium chloride 4. English, German.
1991 Apr;24(4):541-4. doi: with erythema multi- doi: 10.1111/j.1610-
10.1016/0190-9622(91)70078- forme-like reaction in a 0387.2008.06964.x.
g. child. Contact Dermatitis. Epub 2008 Dec 3.
2. Mehregan DA, Thomas 2020 Jun;82(6):397-399. PMID: 19054421.
JE, Mehregan DR. doi: 10.1111/cod.13481. 11. Scheinfeld NS, Mones J.
Intertriginous granular Epub 2020 Apr 3. Granular parakeratosis:
parakeratosis. J Am PMID: 32112429. pathologic and clinical
Acad Dermatol. 1998 7. Basketter DA, Marriott M, correlation of 18 cases of
Sep;39(3):495-6. doi: 10.1016/ Gilmour NJ, et al. Strong granular parakeratosis. J
s0190-9622(98)70333- irritants masquerading as Am Acad Dermatol. 2005
0. PMID: 9738790. skin allergens: the case of May;52(5):863-7. doi:
3. Metze D, Rütten A. Granu- benzalkonium chloride. 10.1016/j.jaad.2004.12.031.
lar parakeratosis - a unique Contact Dermatitis. 2004 PMID: 15858479.
acquired disorder of kera- Apr;50(4):213-7. doi: 12. Pimentel DR, Michalany N,
tinization. J Cutan Pathol. 10.1111/j.0105-1873.2004.00331.x. Morgado de Abreu MA, et
1999 Aug;26(7):339-52. doi: PMID: 15186375. al. Granular parakeratosis
10.1111/j.1600-0560.1999. 8. Wentworth AB, Yiannias in children: case report and
tb01855.x. PMID: 10487291. JA, Davis MD, et al. review of the literature.
4. Wohlrab J, Lüftl M, Wolter Benzalkonium Chloride: Pediatr Dermatol. 2003
M. Submammary granular A Known Irritant and May-Jun;20(3):215-20.
parakeratosis: an acquired Novel Allergen. Dermatitis. doi: 10.1046/j.1525-
punctate hyperkeratosis of 2016 Jan-Feb;27(1):14-20. 1470.2003.20306.x.
exogenic origin. J Am Acad doi: 10.1097/ PMID: 12787269.
Dermatol. 1999 May;40(5 Pt DER.0000000000000160. 13. Patrizi A, Neri I, Misciali
2):813-4. PMID: 10321622. PMID: 26756511. C, et al. Granular paraker-
5. Robinson AJ, Foster 9. Wallace CA, Pichardo atosis: four paediatric
RS, Halbert AR, et al. RO, Yosipovitch G, et al. cases. Br J Dermatol. 2002
Granular parakeratosis Granular parakeratosis: a Nov;147(5):1003-6. doi:
induced by benzalkonium case report and literature 10.1046/j.1365-2133.2002.04953.x.
chloride exposure from review. J Cutan Pathol. PMID: 12410715.
laundry rinse aids. Austral- 2003 May;30(5):332-5. doi: 14. Giraldi, S, Abagge, KT,
as J Dermatol. 2017 10.1034/j.1600-0560.2003.00066.x. Carvalho, VOd, et al. Para-
Aug;58(3):e138-e140. PMID: 12753175. queratose granular: relato
doi: 10.1111/ajd.12551. 10. Braun-Falco M, Laaff H. de seis casos em crianças.
Epub 2016 Sep 19. Granular parakeratosis--a Anais Brasileiros de
PMID: 27641714. clinical-pathological Dermatologia, 81(1), 59-64.
141
NZMJ 30 April 2021, Vol 134 No 1534
ISSN 1175-8716 © NZMA
www.nzma.org.nz/journalCLINICAL CORRESPONDENCE
https://doi.org/10.1590/ treated with liposomal doi: 10.1001/arch-
S0365-05962006000100008 doxorubicin for ovarian dermatol.2011.214.
15. Borok J, Matiz C, Gold- carcinoma. J Am Acad PMID: 21844474.
enberg A, et al. Contact Dermatol. 2008 May;58(5 26. Contreras ME, Gottfried
Dermatitis in Atopic Suppl 1):S84-7. doi: LC, Bang RH, et al. Axillary
Dermatitis Children-Past, 10.1016/j.jaad.2007.05.031. intertriginous granular
Present, and Future. Clin PMID: 18489055. parakeratosis responsive
Rev Allergy Immunol. 21. Resnik KS, DiLeonardo to topical calcipotriene
2019 Feb;56(1):86-98. doi: M. Incidental granular and ammonium lactate.
10.1007/s12016-018-8711- parakeratotic cornifica- Int J Dermatol. 2003
2. PMID: 30225535. tion in carcinomas. Am May;42(5):382-3. doi:
16. Sanmiguel, Adam, Eliza- J Dermatopathol. 2007 10.1046/j.1365-4362.2003.01722.x.
beth A. Grice. Interactions Jun;29(3):264-9. doi: 10.1097/ PMID: 12755978.roebrock
between Host Factors DAD.0b013e3180465860. 27. Samrao A, Reis M, Niedt
and the Skin Microbiome. PMID: 17519624. G, Rudikoff D. Granular
Cellular and Molecular Life 22. Roebrock K, Wolf M, parakeratosis: response
Sciences 72, no. 8. 2014: Bovens S, et al. Inhibition of to calcipotriene and brief
1499-515. doi:10.1007/ benzalkonium chloride-in- review of current thera-
s00018-014-1812-z. duced skin inflammation peutic options. Skinmed.
17. Weyrich LS, Dixit S, in mice by an indol-1- 2010 Nov-Dec;8(6):357-9.
Farrer AG et al. The skin ylpropan-2-one inhibitor PMID: 21413654.
microbiome: associations of cytosolic phospholipase 28. Brown SK, Heilman
between altered microbial A2 α. Br J Dermatol. 2012 ER. Granular paraker-
communities and disease. Feb;166(2):306-16. doi: atosis: resolution with
Australas. J. Dermatol. 10.1111/j.1365-2133.2011.10637.x. topical tretinoin. J Am Acad
2015; 56: 268–74. Epub 2011 Dec 6. Dermatol. 2002 Nov;47(5
PMID: 21929537. Suppl):S279-80. doi:
18. Kong HH, Oh J, Deming C
et al. Temporal shifts in the 23. Sadakane K, Ichinose T. 10.1067/mjd.2002.109252.
skin microbiome associated Effect of the hand antisep- PMID: 12399751.
with disease flares and tic agents benzalkonium 29. Ravitskiy L, Heymann
treatment in children with chloride, povidone-iodine, WR. Botulinum toxin-in-
atopic dermatitis. Genome ethanol, and chlorhexidine duced resolution of
Res. 2012; 22: 850–9. gluconate on atopic derma- axillary granular para-
titis in NC/Nga mice. Int. J. keratosis. Skinmed. 2005
19. Kumarasinghe SPW,
Med. Sci. 2015; 12: 116–25. Mar-Apr;4(2):118-20.
Chandran V, Raby E, et al.
Hyperkeratotic flexural 24. Isaac J, Scheinman PL. doi: 10.1111/j.1540-
erythema responding to Benzalkonium Chlo- 9740.2005.03700.x.
amoxicillin-clavulanic acid ride: An Irritant and PMID: 15785142.
therapy: Report of four Sensitizer. Dermatitis. 30. Laimer M, Emberger
cases. Australas J Dermatol. 2017 Nov/Dec;28(6):346- M, Brunasso AM, et al.
2019 Nov;60(4):311-314. 352. doi: 10.1097/ Laser for the treatment of
doi: 10.1111/ajd.13069. DER.0000000000000316. granular parakeratosis.
Epub 2019 May 2. PMID: 28885313. Dermatol Surg. 2009
PMID: 31049927. 25. Patel U, Patel T, Skinner RB Feb;35(2):297-300. doi:
20. Jaconelli L, Doebelin B, Jr. Resolution of granular 10.1111/j.1524-4725.2008.01052.x.
Kanitakis J, et al. Granular parakeratosis with topical Erratum in: Dermatol
parakeratosis in a patient calcitriol. Arch Dermatol. Surg. 2009 Mar;35(3):557.
2011 Aug;147(8):997-8. PMID: 19215276.
142
NZMJ 30 April 2021, Vol 134 No 1534
ISSN 1175-8716 © NZMA
www.nzma.org.nz/journalYou can also read

















































