Communications and Engagement Strategy 2019 to 2021
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Communications and Engagement Strategy
2019 to 2021
Andrea Harper
Head of Communication and Engagement
Sharon Smith
Author(s) (name Patient Engagement Lead
and post):
Version No.: Version 1.1
Approval Date: tbc
Review Date: March 2021
1
Document Control Sheet
Title: Communications and Engagement Strategy 2019 - 2021
Telford and Wrekin Communication and Engagement Strategy
Electronic File Name: C:2019-2020.doc
Placement in
Organisational Governance and Engagement: Communications and Engagement
Structure:
Consultation with
Governance Board, stakeholders, GP member practices
stakeholders:
Equality Impact Executive Lead Governance and Engagement
Assessment: December 2019
Approval Level: CCG Governance Board
Implementation
Dissemination Date: Date:
Method of
Via the CCG staff newsletter and placed on the CCG website.
Dissemination:
Document Amendment History
Version No. Shared with Date Brief Description of
amendments
V1.1 Board Members, GP Members 25/01/2016 Linking of Fig 2 to
(via email) CCG Deputy Team, Action Plan
Telford and Wrekin Re-emphasis of the importance of
Healthwatch, Health Round carers
Table and Public Health
V1.2 Internal further proofing and 03/03/2016 Inclusion of Gunning Principles
reformatting to reflect
available sources of Inclusion of reference documents
information for Consultation
Inclusion of involvement website
Update to reflect accessible
information standard
V1.3 Planning, Performance And 22/03/2016 Addition to resources section 7.1
Quality Committee (vi) to reflect prioritisation of CCG
priorities
V1.4 Planning, Performance And 28/01/2020 Strategy extended to April 2021 to
Quality Committee cover interim period prior to
creation of Single Strategic
Commissioning Organisation with
Shropshire CCG in April 2021
The formally approved version of this document is that held on Telford and Wrekin Clinical
Commissioning Group’s website at http://www.telfordccg.nhs.uk/strategies
Printed copies or those saved electronically must be checked to ensure they match the current online
version.
2
CONTENTS
1. Purpose of this Communication and Engagement Strategy ................................................... 4
Figure 1 SWOT analysis of Communication and Engagement..................................................... 7
2. CCG vision, values and objectives ............................................................................................... 8
3. What are the principles that underpin Communication and Engagement in NHS Telford and
Wrekin CCG? ....................................................................................................................................... 11
Figure 2 Engagement Principles ..................................................................................................... 12
4. NHS Telford and Wrekin CCG Communication and Engagement Objectives 2016-2019 13
5. Delivering the Objectives of CCG Communications and Engagement Activities ................ 14
6. Communication and Engagement: Legal Duties to Engage and Consult ................................. 18
7. Resources, Roles and Responsibilities ........................................................................................ 25
Figure 3 Overview Communication and Engagement Roles in Service Redesign ..................... 30
Figure 4 Recommended Consultation Activity Timelines ..........................................................31
8. CCG Stakeholders and Stakeholder Mapping ............................................................................. 32
Figure 5 Stakeholder Mapping Tool .................................................................................................. 33
9. Communication and Engagement throughout the Commissioning Cycle ............................... 34
10. Addressing the full scope of Communication and Engagement Requirements .................... 36
11. Evaluating the Strategy’s effectiveness ..................................................................................... 37
Appendix A Implementation plan to deliver improvements in Communication and
Engagement ....................................................................................................................................... 38
3
1 Purpose of this Communication and Engagement Strategy
1.1 NHS Telford and Wrekin CCG has made significant steps since it was formed on
st
1 April 2013, to develop a robust approach to communications and engagement.
We have worked hard to develop and maintain new and stronger stakeholder
relationships and undertaken communications and engagement activity that has
been well received by patients, carers, the public and other key stakeholders. Figure
1 on page 6, demonstrates our assessment of the current position based on
stakeholder 360 feedback/ staff survey results and best practice identified by the
team. We are now moving forward and drawing together in one place the values,
principles and statutory requirements, that will guide our organisation in taking
forward the CCGs’ communication and engagement functions during 2019-2021
1.2 In November 2018 NHS England set a running cost savings target of 20% for
CCGs to attain by the end of 2019/20, following this in January 2019 National Health
and Care leaders came together to produce the Long Term Plan to make the NHS fit
for the future. The Plan included the requirement to streamline commissioning
organisations with one commissioner for each STP/ICS. As a result, the two existing
statutory bodies NHS Shropshire and NHS Telford & Wrekin will be dissolved and a
new statutory body will be created that will serve the Shropshire county footprint.
This Communication and Engagement Strategy for Telford and Wrekin CCG will
continue on from the previous strategy and include the period up to and including
March 2021. It will not cover the process of the two statutory bodies becoming one
as that is covered separately by the development of a Communication and
Engagement Plan and subsequently becoming a Single Strategic Commissioning
Organisation, with a newly developed Communication and Engagement Strategy
that is being developed as part of our application process to NHS England.
1.3 The ever-changing landscape of the NHS means that communication and
engagement is now even more critical to ensure that all stakeholders (including
clinical, administrative, patient, carers and the public) are aware of, and understand
how the CCG commissions clinically led and patient centred services. Therefore
this strategy is a statement of the CCG core commitment that communication and
public engagement are fundamental to our performance and ability to deliver
excellent health services.
4
1
1.4 In delivering the Five Year Forward View, we recognise the importance and
value of patient and public engagement to develop and deliver whole scale system
change through new models of service provision .The success of these models will
be dependent on changes in the way we interact with and empower patients, and
the public to be involved in their own health care.
1.5 The CCG, in completing the analysis that informs figure 1 on page 6 recognises
that for improvements to be made, we need to be clear on the objectives we aim to
deliver to the people of Telford & Wrekin and these are set out in Section 2.
1.6 To support CCG staff in discharging their duties to involve patients and the
public, we have included sections in relation to legal duties, role of communication
and engagement in the commissioning cycle and resources to support CCG staff in
engagement and consultation activities.
1.7 Importantly, going forward we want to ensure that we are actively listening to
messages through our involvement and engagement with the residents of Telford
and Wrekin, in all commissioning activities. A priority within this will be, advancing
our Public Sector Equality Duties under Section 149 of the Equality Act 2010. This
means increasing our focus on engagement activities from the viewpoint of the nine
protected characteristics. We will also consider the importance of carers as a
distinct sub-group to engage with, in regard to changes to healthcare.
1.8 This strategy covers all external communications, stakeholder and public
engagement, including social marketing and health campaigns, as well as internal
communications, partnership and clinical engagement for the residents of Telford &
Wrekin. The implementation plan in Appendix A details how these areas will be
actioned. The implementation plan will be monitored quarterly and refreshed
annually. The actions in the implementation plan are cross referenced to the SWOT
diagram (Figure 1, page 6).
1
Five year Forward View available https://www.england.nhs.uk/wp-content/uploads/2014/10/5yfv-
web.pdf
5
1.9 This strategy document is designed to:
• inform the reader of the principles that will govern how the CCG
communicates internally and externally;
• identify the objectives that the CCG aims to deliver during 2019 - 2021; and
• act as the reference for commissioning managers with regard to
communication and engagement with our population and stakeholders,
importantly patients and carers.
6
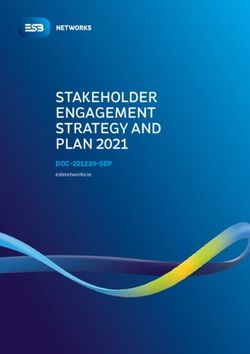
Figure 1 SWOT analysis of Communication and Engagement
Strengths Weaknesses
• Clinical leaders understand the • Low public awareness of the
local population needs CCG’s work
• GP community know each • Not seen as a system leader
other and Board GPs • Gaps in communication
• Some good examples of robust capability throughout the CCG
engagement and communications • Some relationships with
since becoming a CCG stakeholders need strengthening
• Good relationships with • Gaps in communication
community leaders and third with member practices
sector organisations • Gaps in communication with staff
• Work undertaken with people with • Strategic engagement
protected characteristics • Lack of adherence to
CCG branding guidelines
Opportunities Threats
• Build on best practice and • Lack of collaborative
successful engagement and working across teams
consultation • Clinical leaders managing
• Relationship building with a conflicting time commitments
broader spectrum of voluntary and and priorities
representative groups • Lack of understanding by
• Development of robust stakeholders of communications
internal communications and engagement
• Raise expectation and awareness • Limited joined up working
of local healthcare services. across commissioning and
• Strengthen self-care management provider organisations
and patient choice through • Lack of resource/finance
communications and engagement for campaigns
channels • Lack of planning of
• Build on existing good communications and
relationships with local media engagement requirements as
• More strategic approach to the part of the commissioning cycle
use of social media • Lack of communication and
• Move away from a reactive to a engagement activities in QIPP
proactive approach to and redesign projects.
communication and engagement
7
2. CCG vision, values and objectives
2.1 Our Overall CCG Vision
“Working with our patients, Telford & Wrekin
CCG aspires to have the healthiest
population in England.”
“Healthier, Happier, Longer”.
2.2 The values that lie at the heart of the CCG work are:
i. respect, dignity and compassion;
ii. put patients and the public at the heart of
commissioning;
iii. deliver effective planning for health services based
on a true understanding of the population and their
needs based upon the Joint Strategic Needs
Assessment (JSNA);
iv. maintain and improve the quality of health
outcomes and the safety of services for patients;
v. ensure clinical engagement and the achievement
of our Quality, Innovation, Productivity and
Prevention (QIPP) plans;
vi. ensure a partnership approach to health and social
care; and
vii. work with the resources available.
8
2.3 NHS Telford and Wrekin Strategic Objectives:
i. to improve commissioning of effective, safe and sustainable
services, which deliver the best possible outcomes, based upon
best available evidence;
ii. to increase life expectancy and reduce health inequalities;
iii. to encourage healthier lifestyles;
iv. to support vulnerable people; and
v. to exercise CCG functions effectively, efficiently and
economically, and in accordance with generally accepted
principles of good governance and as an employer of choice.
2.4 Key Programmes of work for Telford and Wrekin CCG
To help support delivery of these objectives, the CCG has set out four key
programmes of work, each with a series of projects discussed and agreed with our
practice members.:
i. Change the dynamic' To strengthen communities and individuals
ability to ‘self-care’;
ii. 'Patients at the centre' To sustain and improve primary care including
strengthening integrated multi-disciplinary working in line with current
BCF pilots;
iii. 'Streamlined care - robust pathways' to ensure we commission
sufficient capacity for planned care and improve the patient experience
of appointments and treatment.
iv. Support people in a crisis with the right care, right place' to make
sure people can 'navigate' a simplified 'Urgent Care System' to meet
both physical and mental health needs
.
These priority programmes are shown in the diagram below which emphasises the
centrality of the patient to the CCG’s priority programmes and the need for these
programmes to inter-link and be delivered simultaneously.
9
2.5 To deliver on these values, objectives and work priorities we are committed to
informing, engaging and listening to our communities in the broadest sense with;
patients, carers, CCG member practices, members of the public, Telford and Wrekin
Healthwatch, voluntary sector organisations, commissioned service providers,
partners in the local authority and our own staff.
2.6 There is a clear expectation that in the Long Term Plan that there will be one
Single Strategic Commissioning Organisation at a STP Level and for this Telford
and Wrekin CCG and Shropshire CCG are looking to create a Single Strategic
Commissioning Organisation for the Shropshire STP footprint from April 2021.
However, in the interim Telford and Wrekin through strong clinical engagement will
seek to continue to deliver change by proactively shaping health opinions and
aspirations of the public and patients.
2.7 To achieve this, we must continue to build strong relationships with stakeholders
and effective methods of communicating and we must make sure we involve people
in the decision-making processes. Patient and public confidence develops from
trust, and trust builds on integrity and competence. Therefore, we must
communicate the successes of the NHS and openly handle any crises effectively if
the population, employees and stakeholders are to support us in developing and
improving the local healthcare system
103. What are the principles that underpin Communication
and Engagement in NHS Telford and Wrekin CCG?
3.1 This strategy sets out our approach to communicating with stakeholders and the
public and involving local people in changes to NHS services in Telford and Wrekin.
Its effective delivery will ensure that patient views are at the heart of the services we
commission. We will develop a wide ranging programme of engagement, which
enables measurable involvement to ensure that the CCG listens and responds, and
influences the commissioning decisions of the CCG.
3.2 Our strategy is informed by the NHS Long Term Plan, the organisational
development plan and by the local engagement and consultation work already
undertaken, for example NHS Future Fit. The strategy will be supported by a set of
robust policies which will include a media policy, social media policy and corporate
brand guidelines.
3.3 However, whilst we will ensure we adhere to policies for good governance, this
strategy will not be prescriptive in the methods to be used for particular audiences,
we want to encourage innovative and genuine engagement according to the
subject area we are discussing.
3.4 What we do advocate is the following set of principles and objectives (which are
covered in section 3 + 4) to act as a guide for commissioners thinking about and
designing their communication and engagement plans.
3.5 At its conception the CCG had agreed the guiding principles it would follow in
communication and engagement. These were ratified and further developed in a joint
event with patients and carers and enshrined in the Patient Magna Charter, a copy of
which is prominently displayed in CCG headquarters.
3.6 To deliver the changes necessary for the future, fully harnessing the energy of
patients, local people and diverse communities will require a new model of
partnership. In order to support this new relationship, the Five Year Forward View
People and Communities Board, working with patients, the voluntary sector and
vanguards, has set out six principles for new care models. Figure 2 page 11 details
all these key principles.
11Figure 2 Engagement Principles
Core CCG Engagement Principles Patient Magna Charter Pledges NHS England FYFV Principles
Be open, honest, timely and transparent Work with partners and clinicians as Voluntary, community and social enterprise
when we communicate and engage with equal partners in commissioning and sectors are key enablers
all our stakeholders evaluating care services
Ensure communication and engagement Recognising that patients have different Services are created in partnership with
is meaningful, targeted and integral to levels of activation and need differing patients and diverse communities
our business planning and levels and types of support at all times
commissioning decision making
processes.
Embrace the ethos of: “No decision Include shared decision-making as a vital Care and support is person-centred:
about me, without me” part of all patients care personalised, coordinating and empowering
Be accountable, act on feedback Commission services which include Carers are supported
received and communicate the support for patients self –management,
outcomes of engagement work
Ensure communication and engagement Require providers to participate with There is a focus on reducing health
is everyone’s responsibility within the patients in their personal care plans inequalities
CCG
Our communications will be open and Listen to patients and hear their stories Volunteering and social action are key
accountable, ensuring that feedback and so we can work with them to co- enablers
two-way communication processes commission care that they want and
underpin the work we do. need in order to live well
124. NHS Telford and Wrekin CCG Communication and
Engagement Objectives 2019 - 2021
Objective 1 Objective 2
To continue to build continuous and meaningful Increase recognition by patients, public, providers, member
engagement with our public, patients and carers to practices and partner organisations in Telford & Wrekin
influence the shaping of services which improves the that the CCG is an effective and responsive commissioning
health and wellbeing of people in Telford & Wrekin. organisation.
Objective 3
Objective 4
Develop and maintain effective communication channels
to ensure that the people of Telford & Wrekin have the Develop a culture within Telford & Wrekin CCG that
information they need to enable them to access the right promotes open engagement and communication within and
care at the right time, helping them to both look after outside the organisation.
themselves and manage their health and wellbeing.
135. Delivering the Objectives of CCG Communications and
Engagement Activities
Objective 1
To continue to build continuous and meaningful engagement with our
public, patients and carers to influence the shaping of services which
improves the health and wellbeing of people in Telford & Wrekin.
This will be achieved by:
• Ensuring the public voice is directly involved in and influences the
decisions made by NHS Telford & Wrekin CCG
• Actively seeking out patient and carer experience data from a range of
sources.
• Ensuring that patient and carer experience data is systematically
collected and embedded into work programmes.
• Using the most appropriate means of communication for
the requirements of the audience.
• Using a wide variety of methods and innovative approaches
to engagement.
• Working closely with hard to reach groups to ensure they have a voice.
• Using patient / carer experience data and information to inform our work
and to work with provider organisations to listen to patients/carers more
and act on their feedback.
• ‘Closing the loop.’ by reporting on the impact of public feedback on
Telford and Wrekin CCG decisions.
• Learning from good practice and tried and tested examples of
engagement.
Expected Outcomes of Objective 1:
People in Telford & Wrekin feel they have a voice in the decisions
made by the CCG and will be able to identify how they have
influenced local NHS services.
14Objective 2
Increase recognition by patients, public, providers, member
practices and partner organisations in Telford and Wrekin that the CCG is
an effective and responsive commissioning organisation.
This will be achieved by:
• Protecting the reputation of and promoting the Telford and Wrekin CCG
and NHS brand.
• Developing good media relations and addressing any inaccuracies
to prevent misunderstanding and confusion.
• Ensuring internal and external audiences are aware of the CCG and
locality developments, as well as issues facing the CCG.
• Providing consistent and timely messages, internally and externally,
to various audiences including staff, GP member practices, the public,
patients and key stakeholders.
• Working collaboratively with partners and other NHS organisations
in and around the Telford and Wrekin area.
Expected Outcomes of Objective 2
Stakeholders are confident that Telford and Wrekin CCG is taking the
lead across the local health economy to successfully commission
healthcare services and is operating in the best interests of the people of
Telford and Wrekin.
15Objective 3
Develop and maintain effective communication channels to ensure that
the people of Telford and Wrekin have the information they need to enable
them to access the right care at the right time, helping them to both look
after themselves and manage their health and wellbeing.
This will be achieved by:
• Working with GP member practices, providers and partners to
ensure that public information is accurate and up to date.
• Working collaboratively with providers and partners to ensure
that messages are consistent and timely.
• Working closely with our community groups, particularly those
groups the NHS traditionally struggles to fully engage on a consistent
basis, sometimes described as “hard to reach” groups to ensure that
messages and information are being received and are understood.
• Continuously scoping new and innovative ways of communicating,
making the best use of new technologies and digital communication.
• Regularly testing out the effectiveness of the communication methods
used.
• Making language meaningful for staff, public, patients and carers in all
communications.
Expected Outcomes of Objective 3:
The people of Telford and Wrekin will be well informed and will have a
good understanding of services and what is available to them. People
will have the information they need to help them improve their own
health and wellbeing, with the aim of helping to reduce inappropriate
use of services, reduction in ‘Did Not Attends’ and an increased use of
self-care.
16Objective 4
Develop a culture within Telford and Wrekin CCG that promotes open
engagement and communication within and outside the organisation.
This will be achieved by:
• Developing and maintaining good media relations.
• Developing internal two-way communication channels with
staff, practice and GP members.
• Ensuring internal and external audiences are aware of service
developments and successes by using a range of communication
techniques.
• Ensuring internal and external audiences are able to feedback
information on successes and achievements through accessible routes.
• Making language meaningful for staff, public, patients and carers in all
communications.
Expected Outcomes of Objective 4
The CCG will have the support it needs to ensure effective relations with
the media. CCG Clinicians will have support they need to understand
their role and what is expected of them in terms of promoting
engagement and communication externally to the CCG. CCG member
practices and staff feel they can express their opinions and judgement
and feel their contribution is valued. The public will feel valued and
informed and will be aware of how they can feedback to the CCG.
176. Communication and Engagement: Legal Duties to Engage and
Consult
6.1 Our Legal Duties
i. Data Protection Act 1998
The Data Protection Act controls how everyone’s personal information is used by
organisations, businesses or the government.
Everyone responsible for using data has to follow strict rules called
‘data protection principles’. They must make sure the information is:
• used fairly and lawfully
• used for limited, specifically stated purposes
• used in a way that is adequate, relevant and not excessive
• accurate
• kept for no longer than is absolutely necessary
• handled according to people’s data protection rights
• kept safe and secure
• not transferred outside the European Economic Area without adequate
protection
There is stronger legal protection for more sensitive information, such as:
• ethnic background
• political opinions
• religious beliefs
• health
• sexual health
• criminal records
The General Data Protection Regulation (EU) 2016/679 (GDPR) is a
regulation in EU law on data protection and privacy for all individual
citizens of the European Union (EU) and the European Economic Area
(EEA). It also addresses the transfer of personal data outside the EU and
EEA areas. The GDPR aims primarily to give control to individuals over
their personal data and to simplify the regulatory environment for
international business by unifying the regulation within the EU.
Superseding the Data Protection Directive 95/46/EC, the regulation
contains provisions and requirements related to the processing of personal
data of individuals (formally called data subjects in the GDPR) inside the
EEA, and applies to any enterprise established in the EEA or—regardless
of its location and the data subjects' citizenship—that is processing the
personal information of data subjects inside the EEA
The CCG has separate policies to govern how it manages and protects the
information it holds.
18ii. Freedom of Information Act 2000
The Freedom of Information Act 2000 provides public access to information
held by public authorities.
It does this in two ways:
• public authorities are obliged to publish certain information about
their activities; and
• Members of the public are entitled to request information from
public authorities.
The Act covers any recorded information that is held by a public authority in
England, Wales and Northern Ireland, and by UK-wide public authorities based in
Scotland. Information held by Scottish public authorities is covered by Scotland’s
own Freedom of Information (Scotland) Act 2002.
The CCG has separate function to manage FOIs via Midlands and Lancashire
CSU.
iii. National Health Service Act 2006 (as amended by the Local
Government and Public Involvement in Health Act 2007)
The Act requires NHS bodies, both commissioner and provider, to consult
with users of services:
• In the planning of provision,
• Development and consideration of changes in the way services are provided
and
• Decisions to be made that would affect the operation of services.
Section 234 of the same Act requires the CCG to report on the consultation
carried out before making its commissioning decisions and on the influence
that the results of consultation have had on its commissioning decisions.
Section 244 National Health Service Act 2006 requires the CCG where it has
under consideration a proposal for a “substantial development of health service”
in the area or for a “substantial variation in the provision” of a service; it must
consult with the overview and scrutiny committee of the local authority.
The Equality Act 2010
The Equality Act 2010 replaces previous anti-discrimination legislation (such as the
Race Relations Act 1976 and the Disability Discrimination Act 1995). It simplifies and
19strengthens the law, removing inconsistencies and making it easier for people and
organisations to understand and comply with legislated equality requirements.
iv. The Equality Act 2010 extends protection to groups not previously
covered under legislation. The protected characteristics under the Act are:
Age, disability, gender, gender re-assignment, race,
religion or belief, marriage and civil partnership and
pregnancy and maternity.
The Public Sector Equality Duty (PSED) comprises a general equality duty
which is supported by specific duties. The general equality duty states that
public authorities must, in the exercise of their functions, have due regard to the
need to:
• Eliminate unlawful discrimination, harassment and victimisation.
• Advance equality of opportunity between different groups.
• Foster good relations between different groups.
To enable the CCG to monitor this duty, project document requires an
Equality Impact Assessment to have been completed before the project is
agreed to be implemented.
v. Health and Social Care Act 2012 –
The 2012 Health and Social Care Act sets out two duties for NHS Commissioners
with respect to patient and public participation. The first concerns individual
patient participation in their care decisions. The second duty places a
requirement on CCGs and NHS England to ensure public involvement and
consultation in commissioning processes and decisions.
It includes involvement of the public, patients and carers in:
• Planning of commissioning arrangements, which might include consideration of
allocation of resources, needs assessment and service specification.
• Proposed changes to services which may impact on patients.
The relevant clauses in the Act as they relate to CCGs are as follows:
20Section 14Z2 Public involvement and consultation by clinical
commissioning groups
1) This section applies to any health services which are, or are to be,
provided pursuant to arrangements made by a clinical commissioning group
in the exercise of its functions (‘commissioning arrangements’).
2) The clinical commissioning group must make arrangements to secure that
individuals to whom the services are being or may be provided are involved
(whether by being consulted or provided with information or in other ways)
a) In the planning of the commissioning arrangements by the group,
b) in the development and consideration or proposals by the group for
changes in the commissioning arrangements where the implementation of
the proposals would have an impact on the manner in which the services are
delivered to the individuals or the range of health services available to them,
and
c) In decisions of the group affecting the operation of the commissioning
arrangements where the implementation of the decisions would (if made)
have such an impact.
6.2 In order for the CCG to discharge its duties under the legislation listed
previously, it is important that the CCG seeks good evidence and engages with
those parts of its population that may suffer discrimination to ensure its decisions do
not knowingly discriminate. This duty lies internally with the Deputy Executive
leading the service redesign and collectively with the Board for approving
commissioning decisions.
6.3 In practical terms commissioners should actively engage with patients/public
whenever they propose a change to the services currently commissioned including
when they decide not to recommission a contract that has ceased, as this is a
decommissioning decision.
6.4 To assist CCGs in these engagement duties NHS England published a
guidance document Transforming participation in Health and Social Care
guidance (published September 2013) available at:
21https://www.england.nhs.uk/wp-content/uploads/2013/09/trans-part-hc-guid1.pdf
This guidance discusses formal consultation occurring when there is a major service
change.
6.5 In addition there is guidance within the HM Government Code of Practice on
Consultation 2012. Available at:
https://www.gov.uk/government/publications/consultation-principles-guidance
6.6 The following guide for CCGs engaging the public in difficult decisions about
health service change by NHS Clinical Commissioners is another useful resource
document to assist commissioners:
http://www.nhscc.org/wp-content/uploads/2015/05/NHSCC-Engaging-the-Public-
Final.pdf
6.7 The governing principle is proportionality of the type and scale of consultation to
the potential impacts of the proposal or decision being taken, and thought should be
given to achieving real engagement rather than merely following bureaucratic
process. Consultation forms part of wider engagement and decisions on whether and
how to consult, should in part, depend on this wider scheme of engagement.
6.8 There are no definitive prescriptive rules on whether engagement or
consultation should be in place, but it would need to demonstrate that it is
as proportionate to the change being proposed.
6.9 To support the CCG in their engagement / consultation duties there is a CSU
online platform for guidance, resources and tools and sharing of best practice:
http://nhsinvolvement.co.uk/connect-and-create/consultations/what-to-include-in-
a-consultation-document
6.10 Consultation and the Gunning Principles
Before 1985 there was little consideration given to consultations until a landmark
case in that year (R v London Borough of Brent ex parte Gunning). This case
sparked the need for change in the process of consultations when Stephen Sedley
QC proposed a set of principles that were then adopted by the presiding
judge. These principles, known as Gunning or Sedley, were later confirmed by the
Court of Appeal in 2001 (Coughlan case) and are now applicable to all public
consultations that take place in the UK.
22I. When proposals are still at a formative stage
Public bodies need to have an open mind during a consultation and not
already have made the decision, but have some ideas about the proposals.
II. Sufficient reasons for proposals to permit ‘intelligent consideration'
People involved in the consultation need to have enough information to
make an intelligent choice and input in the process. Equality impact
assessments should take place at the beginning of the consultation and
published alongside the document.
III. Adequate time for consideration and response
Timing is crucial – is it an appropriate time and environment, was enough
time given for people to make an informed decision and then provide that
feedback, and is there enough time to analyse those results and make the
final decision?
IV. Must be conscientiously taken into account
Think about how to prove decision-makers have taken consultation responses
into account.
The risk of not following these principles could result in a judicial review. A
number of public bodies across the UK have been taken to judicial review and
deemed to have acted unlawfully in their Public Sector Equality Duty – usually
linked to the four Gunning Principles.
6.11 SCCI1605 Accessible Information .NHS England 2015
The ‘Accessible Information Standard’ directs and defines a specific, consistent
approach to identifying, recording, flagging, sharing and meeting the information
and communication support needs of patients, service users, carers and parents,
where those needs relate to a disability, impairment or sensory loss. The Standard
applies to service providers across the NHS and adult social care system, and
effective implementation will require such organisations to make changes to policy,
procedure, human behaviour and, where applicable, electronic systems.
23I. Commissioners of NHS and publicly-funded adult social care must also have
regard to this standard, in so much as they must ensure that contracts,
frameworks and performance-management arrangements with provider
bodies enable and promote the Standard’s requirements.
II. Commissioners MUST ensure that their commissioning and procurement
processes, including contracts, tariffs, frameworks and performance
management arrangements (including incentivisation and penalisation),
with providers of health and / or adult social care reflect, enable and support
implementation and compliance with this standard.
III. Commissioners MUST seek assurance from provider organisations of their
compliance with this standard, including evidence of identifying, recording,
flagging, sharing and meeting of needs.
IV. By 01.09.16 commissioners have sought and received assurance from provider
organisations of their compliance with this standard, including receipt of
evidence of identifying, recording, flagging, sharing and meeting of needs.
V. The CCG will be required to meet the criteria for accessible information for
services it directly provides e.g. TRAQS, Continuing health Care
and Complaints/Pals.
VI. Full document is accessible at:
https://www.england.nhs.uk/ourwork/patients/accessibleinfo-2/
247. Resources, Roles and Responsibilities
7.1 Resources
i. Board level Lead for the engagement and communication function is held
by the Director of Corporate Affairs.
ii. The engagement support function is delivered via a small CCG team of a
Patient Engagement Lead and Patient Experience Lead led by Head of
Communication and Engagement for Shropshire and Telford & Wrekin CCG’s
The team provides both, direct engagement with patients and support for
CCG colleagues to engage as part of commissioning projects and service
redesign, as well as the management of complaints and PALs, to ensure
engagement is embedded throughout the commissioning cycle process.
iii. In addition, a contract with NHS Midlands and Lancashire Commissioning
Support Unit (MLCSU) provides the services of a part time Communications and
Engagement lead, three days of which are embedded within the CCG.
iv. The Communications lead provides the CCG’s communications support and
this lead is further supported by a senior consultant and a team of at scale
specialists which can provide; engagement, design and digital, social media,
marketing, event management and website expertise, as and when required,
in accordance with the CSU service level agreement. This support also
provides staffing resilience and emergency cover.
v. These resources as a whole make up the communications and engagement
team for the CCG.
vi. The CCG has made some central funding provision for ongoing
communications and engagement support, however each commissioning
lead/manager will need to ensure that for every service redesign project
initiated, they are clear on the financial and staff communications and
engagement support required and how this will be provided i.e. from central
25funding or from a project bid. This will be determined by using the four key
priorities outlined in section 2.4 as the means of prioritising funding.
7.2 Roles and Responsibilities
i. The Director of Corporate Affairs has overall responsibility for the
communications and engagement function for the CCG, overseeing delivery
of the communications function via the MLCSU.
ii. All executives and deputy executives have the responsibility to ensure the
service redesign and commissioning functions of their teams have due regard
to both the principles of engagement and the legal requirements. This must be
articulated on Planning. Performance and Quality Reports, Project Planning
documents and Board Papers.
7.3 Corporate Communications
i. The Communication and Engagement team will take overall responsibility for
corporate communications and public engagement, including annual reports,
media work, public events, formal relationship management with
stakeholders, the annual Statement of Involvement, supporting and
developing the CCG’s Assuring Involvement Committee, and CCG
membership scheme, development and maintenance of a CCG brand identity
and image that promotes trust and integrity as well as the delivery of media
training.
26ii. We will continue to work closely with our colleagues across the local health
economy on areas of shared interest, and it will be the responsibility of the
Communications and Engagement team to collaborate and deliver shared
pieces of work i.e. campaign messages, like the winter resilience campaign.
7.4 GP Membership
i. The GP Lead for Primary Care and the Chair of the CCG will be responsible
for member relations and engagement, ensuring strong two-way involvement
in the commissioning decision making process.
ii. The Communications and Engagement team will be responsible for
supporting the Chair with associated communication plans, methods
and materials such as a monthly GP newsletter.
7.5 Quality and Provider Management
i. Formal quality assurance is led by the Executive Nurse Lead for Quality,
Nursing and Safety
ii. The Communications and Engagement Team will take responsibility for
gathering patient satisfaction data from various sources, i.e. complaints,
PALs, NHS to NHS concerns to help to inform the quality contracting process.
7.6 Service Redesign Role of the Deputy Executives/ Commissioning Managers
i. It is the role of the Deputy Executive Leads for Commissioning /
commissioning manager leading the project to consider information from all
available sources as part of the pre engagement process.
27ii. This includes requesting support from the patient engagement team to assist
in this process. This support may be for information on patient experience and
feedback or a request for operational assistance to organise and deliver pre
engagement activities to collect data to inform a decision whether a project
should be undertaken.
iii. It is the role of the Deputy Executive / Commissioning Manager to develop the
case for change and to provide the background information for engagement
/consultation documents as well as the responses to Frequently Asked
Questions.
iv. The Deputy Executive Leads for Commissioning will be responsible for
incorporating a communications plan and patient engagement timetable into
service redesign projects. This should allow adequate time for pre
engagement, planning, conducting the systematic engagement/consultation
and importantly time for conscious consideration of the outcome of the
engagement. This is in line with the Gunning Principles (Refer section 6.10)
v. Refer Figure 4 page 30 for suggested timescales for Consultation.
Engagement timescales may be shorter dependent upon the nature of the
change or information sought.
vi. The responsibility for sourcing the budget that will be required to deliver the
engagement or consultation will need to be secured by the Commissioner lead
for the project. The engagement team will assist with estimated costs as part
of the development of a Communication and Engagement Plan. Costs of
promotional materials, postal costs, room hire, advertisements in local press,
travel costs for focus groups and larger survey analysis resources will all incur
costs however this will need to be scoped on a case by case basis for each
project.
28vii. Consideration may need to be given to outsourcing engagement/ consultation
for harder to reach groups or engagement at scale.
viii. The Communications and Engagement team will be responsible for supporting
deputy executives/ managers to develop communication and engagement
plans, identification of stakeholders, design of surveys, briefing and FAQS.
These activities will need joint input because it will be the commissioning leads
who fully understand the service under redesign and the proposals for change.
ix. The case for change developed by the Deputy/commissioning managers is a
fundamental document that will need to be formulated ahead of any discussion
with HOSC and formulation of the communication and engagement plan.
x. There is no set format for the case for change however, it should contain the
background and rationale for the decision to change current services.
xi. The Communication and Engagement team will support the development of a
case for change through planned pre engagement activities.
xii. The Head of Communications and Engagement will lead on the compilation of
reports and analysis of information and recommendations as a result of
engagement activities.
xiii. The Deputy Executive for the relevant commissioning portfolio will be
responsible for producing a briefing to be shared on the website that
informs patients/public how the results of the feedback have been used to
influence commissioning decisions.
xiv. If Deputy Executives chose to outsource their communication and engagement
activities they are required to ensure the Communication and Engagement
team via the Deputy Executive for Quality and Engagement are fully informed
of all activities.
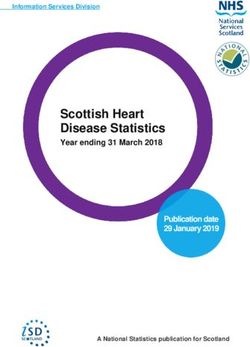
29Figure 3 Overview Communication and Engagement Roles in Service
Redesign
Potential Service Change Proposer to research
Current service usage /
outcome by 9 protected
characteristics
Notify the Communication
Proposer to develop case Liaise with colleagues in Public
& Engagement Team of
for change including Health for JSNA data
potential change planned
via Head of completing initial equality
communications & impact assessment
Engagement
Proposer to review the
feedback known about
Executive Level/PPQ service from patient
Communication &
engagement team and
Engagement Team review Discuss and agree need
consider initial patient
feedback from existing to inform / engage /
discussion
Patients / Stakeholders formal consultation
sources
Executive Lead for
Refer to Figure 4 Timelines
Governance / Head of
Communications & For more detailed Proposer advises HOSC / NHSE
Engagement provides information re formal (in major changes) of case for
advice consultation process change & proposed format for
communication & engagement
supported by Deputy Executive
Quality and Engagement
• Proposer secure funding /
Communication & additional resources
Engagement Team to dependent upon scale of
organise and implement change Agreement to
engagement plan as agreed • Commissioners to support proposals
internally or with HOSC communication and
engagement activities as
Prepare Report and analysis
subject experts
for Proposer
Report Back If formal consultation is
Proposer to consider being undertaken, a
feedback and provide specific project group with
evidence of using this or appropriate external
rationale for non-inclusion support will be required
Results of feedback and
30Figure 4 Recommended Consultation Activity Timelines
318. CCG Stakeholders and Stakeholder Mapping
The key to success of the Communications and Engagement Strategy is
recognising and understanding who our stakeholders are and the most effective way
to communicate with them.
Our stakeholders include, but are not limited to, the following groups:
• patients;
• carers;
• the public;
• GP practice members;
• CCG staff;
• partner organisations: (NHS England, NHS Shropshire Clinical
Commissioning Group, Telford and Wrekin Council, Telford and Wrekin
Healthwatch and the STP/ICS;
• provider organisations: Shrewsbury and Telford Hospital NHS Trust,
Shropshire Community Health NHS Trust, West Midlands Ambulance Trust,
South Staffordshire and Shropshire Mental Health Foundation Trust, Robert
Jones and Agnes Hunt Health Foundation Trust Shropdoc (NB there are other
multiple smaller providers according to the area of commissioning);
• influencers (councillors, MPs, Health Overview and Scrutiny
Committee, Media, Health and Wellbeing Board Leads);
• voluntary sector (e.g. Age UK, CVS); and
• professional Bodies (e.g. Local Medical Council, Local Pharmaceutical
Committee).
Understanding our stakeholder’s needs is vital in everything we do to understand the
impact of the CCG’s plans and decisions may have on them and vice versa.
Stakeholders have a significant contribution to make to the CCG’s decision making
and the following table underlines the importance and influence stakeholders have in
the process.
Commissioners are advised to complete a stakeholder mapping exercise, using the
table following as a basis for identifying particular stakeholders when they are
considering change or wishing to communicate messages. Stakeholders position
on the table will alter according to the nature of the topic/ proposal being
engaged/consulted upon.
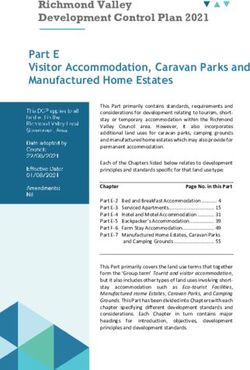
32Figure 5 Stakeholder Mapping Tool
Level of interest
Low
High
Occasional contact Close contact
Local businesses Local voluntary groups
Local schools Carers
Low
Other local contractor groups Local media
NHS healthcare provider staff MPs
Housing Trust and other local public bodies Local authority leaders
Telford and Wrekin Healthwatch
Health Overview and Scrutiny
ofLevel power
STP / ICS / ICPs
STAKEHOLDERS
Relevant contact Continuous contact
National media Patient and patient groups
GP member practices and
Health media PCNs
Specialist media GP patient participation groups
Professional bodies CCG and CSU embedded staff
Local Councillors NHS England
Hig
Other NHS commissioners Local healthcare providers
h
Health and Wellbeing Board
Telford and Wrekin Council
CCG public Membership
scheme
Red – High Power/High Interest – fully engage and satisfy
Orange – High Power/Moderate Interest – inform, seek approval and satisfy
Purple – Moderate Power/High Interest – inform and engage
Green – Low Power/Low Interest – monitor and inform
339. Communication and Engagement throughout the Commissioning
Cycle
Against the background of changes driven by the CCG priorities, it is also necessary
to continue to commission a wide range of services designed to meet the healthcare
needs of the population of Telford and Wrekin.
Commissioning is the process of arranging continuous improvements to services.
This helps the CCG to deliver the best possible quality and outcomes for patients,
meet the needs of the local health population and reduce inequalities with the
resources available. Commissioning can be divided into three distinct parts of a
continuous cycle:
Strategic planning – planning the optimum services which meet national standards
and local ambitions, ensuring patients and the public are involved in the process
alongside other key stakeholders and the range of health professionals who
contribute to patient care;
Specifying outcomes and procuring - securing services, using the contracting
route that will deliver the best quality and outcomes and promote shared decision
making, patient choice and integration; we will involve patients and carers in
development of service outcomes and as appropriate throughout the procurement
process
Managing demand and performance – monitoring, assessing and where
necessary challenging the quality of services and using this intelligence to design
and plan continuously improving services for the future. We will actively seek and act
on patient feedback, both collected via the CCG engagement activities and through
Pals, Complaints and Provider or National Surveys.
In the diagram below we show what engagement and communications the CCG
expects to see at each stage of the commissioning cycle:
3435
10. Addressing the full scope of Communication and
Engagement Requirements
The Strategy to date has focused on our duties to communication and engage when
we are exercising our core commissioning duties for the people of Telford & Wrekin,
however as previously stated the purpose of the strategy is to assist us to deliver all
our communication and engagement functions. These other functions can be
categorised as:
• corporate communications;
• internal communications;
• public/stakeholder engagement;
• media & public relations;
• marketing; and
• design and digital.
Appendix A details the actions that will be undertaken in these areas which
collectively will deliver the outcomes of our 4 strategy objectives. The actions are
also cross referenced against the original SWOT analysis in Figure 2, page 5.
3611. Evaluating the Strategy’s effectiveness
The principles that inform the strategy will be reviewed annually throughout the life
of the document with subsequent updates to the action plan accordingly.
Progress against the action plan will be monitored monthly by the Executive Lead for
Governance and Performance in the first six months of the strategy to ensure that
the key actions are implemented which provide the foundation for the longer term
actions.
Progress against the action plan will be reported quarterly to the Planning
Performance and Quality (PPQ) committee and subsequently through the
PPQ Chair’s report to Board.
37Appendix A Implementation plan to deliver improvements in Communication and Engagement
Link to updated action plan
38EQUALITY IMPACT ASSESSMENT
Stage 1 Initial screening
Name of the proposed policy/service/function: Communications and Engagement Strategy 2019 - 21
Author(s) of the policy/service/function: Andrea Harper, Head of Communications and Engagement
and Michelle Beddow MLCSU
Directorate: Governance and Engagement Date created: December 2019 Date for review: March 2021
The main aims of the policy or proposed policy/service/function:
The strategy documents the CCG’s approach to communications and engagement functions for 2019 - 21.
The intended objectives and outcomes of the policy/service/function:
• Continue to build continuous and meaningful engagement.
• Increase recognition that the CCG is an effective commissioning organisation
• Develop and maintain effective communication channels
• Develop a culture that promotes open engagement
Does the policy/service/function affect any of the following groups of people? (Y or N)
Group Positive Negative Why? (Please explain your reasons. This
impact impact section must be completed)
Race X The strategy acknowledges the legal requirement
that the CCG is mindful of the 9 protected
characteristics when it communicates and engages
with its population, staff, GP member practices and
stakeholders and the need for the CCG to have
more consistent and open communication and
engagement approaches that promote
inclusiveness. Therefore it is expected that the
Strategy will have a positive impact on the
experience of the 9 protected characteristics.
Gender X See above.
Disability X See above.
Sexual orientation X See above.
Age X See above.
Religion or belief X See above.
Gender reassignment X See above.
Marriage and Civil X See above.
Partnership
Pregnancy and X See above.
Maternity
39Positive impact – there may be a positive impact on any of the groups above in relation to promoting equal
opportunities and equality. For example, a targeted programme for black and minority ethnic women would
have a positive effect on that group compared to white women and all men. It is not, however, necessarily an
adverse impact on white women and men.
Negative impact – there may be a negative impact on any of the groups (i.e. disadvantage them in any
way). An example of this would be that if an event were to be held in a building with no loop facilities a
negative and adverse impact would affect attendees with a hearing impairment
What evidence has been used to screen the policy? (e.g. monitoring data, consultation, focus
groups, local population data):
Evidence outlined in NHS England guidance demonstrates that nationally NHS communication and
engagement with all the 9 protected characteristics can be inconsistent and piecemeal. The Strategy seeks
to highlight the need to use different approaches to help engage on a wider consistent basis across the 9
protected characteristics.
What monitoring arrangements are in place for the future?
This EIA will be reviewed periodically and at least annually in conjunction with the action plan to ensure that
the expected positive impact from the Strategy can be demonstrated.
If no negative or adverse impact has been identified please sign off and the process ends here.
Signature: Date:
If a negative or adverse impact has been identified please proceed to Stage 2
40You can also read