Factors Associated With Depression in Disease-Free Stomach Cancer Survivors
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Vol. 46 No. 4 October 2013 Journal of Pain and Symptom Management 511 Original Article Factors Associated With Depression in Disease-Free Stomach Cancer Survivors Kyung Hee Han, MD, PhD, In Cheol Hwang, MD, PhD, Sung Kim, MD, PhD, Jae-Moon Bae, MD, PhD, Young-Woo Kim, MD, PhD, Keun Won Ryu, MD, Jun Ho Lee, MD, Jae-Hyung Noh, MD, PhD, Tae-Sung Sohn, MD, PhD, Dong Wook Shin, MD, MBA, and Young Ho Yun, MD, PhD Division of Cancer Control and Hospital (K.H.H., Y.-W.K., K.W.R., J.H.L., D.W.S.), National Cancer Center, Goyang; Department of Family Medicine (I.C.H.), Gachon University Gil Medical Center, Incheon; Department of Surgery (S.K., J.-M.B., J-H.N., T.-S.S.), Samsung Medical Center, Sungkyunkwan University, Seoul; and Cancer Research Institute (Y.H.Y.), Seoul National University Hospital and College of Medicine, Seoul, Korea Abstract Context. Depression in cancer survivors affects the rest of their lives in many ways. Objectives. To estimate the prevalence of depression and identify associated factors in disease-free stomach cancer survivors. Methods. We enrolled 391 stomach cancer survivors who had been disease-free for at least one year after surgery from the cancer registries of two hospitals in Korea. Stomach cancer survivors were mailed a survey that included the Beck Depression Inventory, the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-Core 30, and the associated stomach module, the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-Stomach Cancer Module 22. Results. Forty-four percent of survivors suffered from depression, and more women (49%) than men (42%) had high depression scores (Beck Depression Inventory >13). In multiple logistic regression analysis, lower income (odds ratio [OR] 2.49; 95% CI 1.64e3.78), problems with care before treatment (OR 1.92; 95% CI 1.23e2.98), body image change (OR 2.23; 95% CI 1.41e3.53), and symptoms of fatigue (OR 3.11; 95% CI 1.49e6.52), dyspnea (OR 2.57; 95% CI 1.48e4.45), or insomnia (OR 4.51; 95% CI 1.88e10.83) were associated with depression. Conclusion. The prevalence of depression was high in stomach cancer survivors even after the completion of treatment, especially among those with problems amenable to treatment, and we identified the associated factors. We suggest that stomach cancer survivors should be screened for depression after the end of treatment. J Pain Symptom Manage 2013;46:511e522. Ó 2013 U.S. Cancer Pain Relief Committee. Published by Elsevier Inc. All rights reserved. Drs. Han and Hwang made similar contributions to 103 Daehak-ro, Jongno-gu, Seoul 110-799, Korea. this article. E-mail: lawyun@snu.ac.kr Address correspondence to: Young Ho Yun, MD, PhD, Accepted for publication: October 23, 2012. Seoul National University College of Medicine, Ó 2013 U.S. Cancer Pain Relief Committee. 0885-3924/$ - see front matter Published by Elsevier Inc. All rights reserved. http://dx.doi.org/10.1016/j.jpainsymman.2012.10.234
512 Han et al. Vol. 46 No. 4 October 2013
Key Words
Depression, stomach cancer, disease-free cancer survivors
Introduction in the post-treatment state. Continuous compli-
cations also can be a source of emotional distress
Stomach cancer is the fourth most common
for stomach cancer survivors, more so than in
cancer and the second leading cause of cancer
those who have recovered from other cancers.17
deaths worldwide. There are about 880,000
However, few data are available regarding
new cases of stomach cancer, and about
the prevalence of depression in patients with
650,000 people die of this disease each year.1,2
gastrointestinal malignancies, especially stom-
Although the overall death rate from stomach
ach cancer. Previous research has focused on
cancer has been decreasing worldwide over
the prevalence of, and predisposing factors
the past several decades owing to early detection
to, depression only at the time of diagnosis
and improvements in treatment, gastric cancer
or after particular types of surgery, such as total
remains an aggressive malignancy.3 The hazard
or subtotal gastrectomy.
rates for death from gastric cancer are relatively
We focus here on Beck Depression Inventory
high in the first few years after diagnosis but
(BDI)-diagnosed depression in stomach cancer
then decline markedly. The prognosis of pa-
survivors who had been disease-free for at least
tients who survive beyond the first several years
one year after surgery. We investigated the
can be substantially improved, and initial esti-
depression-associated factors, including de-
mates of survival time made at diagnosis no lon-
mographic and clinical variables, treatment
ger apply.3
experience, and functional problems and symp-
However, as survival time has increased, seri-
toms.18 The variables of functional and symp-
ous concerns with problems, especially depres-
tomatic problems were derived from the 22
sion, have been reported among cancer
items of the European Organization for Re-
patients.4e6 Depressive disorders affect up to
search and Treatment of Cancer Quality of
38% of patients with cancer, worsen over the
Life Questionnaire-Stomach Cancer Module
course of treatment, persist long after cancer
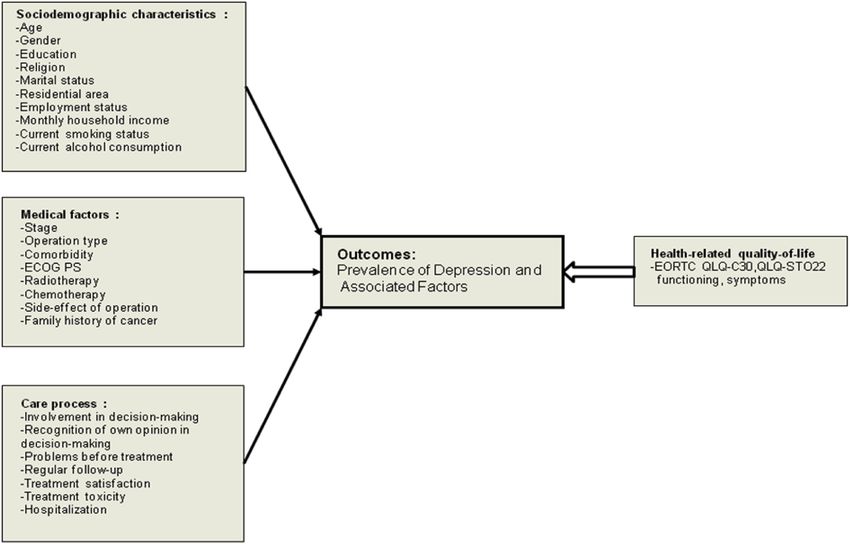
22 (EORTC QLQ-STO22) (Fig. 1). The purpose
therapy has concluded, and often reappear on
of the study was to evaluate the prevalence
cancer recurrence.7e10 In Korea, 32% of hospi-
of BDI-diagnosed depression and identify
talized cancer patients had major depressive
depression-associated factors in disease-free
disorders, and a further 16% had less significant
stomach cancer survivors.
depressive conditions.11 The reported preva-
lence of depression in cancer patients varies sig-
nificantly with differences in the criteria used to Methods
define depression, study methodology, time of Participants and Data Collection
assessment, and the population studied.12e14 We identified the patients through the stom-
Recently, depression is the psychiatric syn- ach surgery databases at the National Cancer
drome that has received most attention in pa- Center and the Seoul Samsung Medical Center
tients with cancer. Depression may be a part in Korea for this cross-sectional study, which
of the reaction to diagnosis,15 but depression was approved by the institutional review boards
persists in many patients, adding to patient of both centers. We, thus, chose patients
burden during treatment and creating difficul- treated at two representative hospitals, and
ties associated with general management and study participants resided in 15 different geo-
symptom control,16 prolonged hospital stays, graphic districts spread across the country.
decreased compliance with treatment, and, Eligibility required a diagnosis of Stage IeIII
possibly, reduced survival.12e14 stomach cancer during 2001 or 2002. Patients
Stomach cancer is different from other can- were excluded if they had a history of another
cers in that the cancer occurs in the central diges- cancer, could not speak Korean, or were youn-
tive organ. Although a full recovery is possible if ger than 18 years. A total of 855 subjects who
early detection is followed by timely surgery, pa- had been diagnosed with Stage IeIII stomach
tients may still experience digestive problems cancer were eligible for the study.Vol. 46 No. 4 October 2013 Depression in Disease-Free Stomach Cancer Survivors 513 Fig. 1. Conceptual framework of the study. The model is based on the hypothesis that poor quality of life resulting from unsatisfactory functioning is associated with depression. EORTC QLQ-C30 ¼ European Organiza- tion for Research and Treatment of Cancer Quality of Life Questionnaire-Core 30; QLQ-STO22 ¼ Quality of Life Questionnaire-Stomach Cancer Module 22; ECOG PS ¼ Eastern Cooperative Oncology Group performance status. We telephoned the eligible subjects to invite agreed to participate was mailed the question- them to participate in the study, and each subject naires. However, 81 patients who agreed to par- who agreed was mailed the questionnaires, a con- ticipate changed mailing addresses. Of the 594 sent form, and a postage-paid return envelope. patients receiving postal material, 165 did not Any subject who did not return the questionnaire return the questionnaires. Among the remain- within one month received a reminder card and ing 429 subjects, six were excluded because a phone call from a staff member, who further re- they did not complete the questionnaires and, iterated the purpose of the study and requested finally, 32 were eliminated because they were that attention be given to the questionnaires. no longer disease-free. A total of 391 study sub- Subjects were asked to sign the informed consent jects thus remained, constituting 52.8% of the form and to return it with the completed ques- original 740 eligible subjects. The study design tionnaires. Any subject who did not wish to and recruitment procedures have been previ- participate was asked to provide a reason. ously described elsewhere.19 When efforts were made to contact eligible subjects by telephone to seek their participa- Demographic and Clinical Information tion in the study, it was discovered that 83 pa- Demographic information included gender, tients had died. Of the remaining 772 patients, age, marital status, education level, employ- 97 refused to participate because of time ment details, religion, monthly household constraints, inability to communicate either ver- income, alcohol use habits, and any family his- bally or in writing (i.e., because no one was avail- tory of cancer. Subjects also were asked about able to assist them), or because they were of the the care afforded to them during the treatment, view that the study was either an inconvenience for example, had a patient participated in the or an invasion of privacy. Each subject who treatment decision making, had any opinion
514 Han et al. Vol. 46 No. 4 October 2013
put forward by the patient been reflected in the We used a total BDI score of greater than 13
treatment, were there any problems before the as the cutoff point for depression as is usually
treatment, had regular follow-up been offered, used in Korean studies.18,22
had the treatment been satisfactory, had treat- The EORTC QLQ-C30 is a 30-item, cancer-
ment toxicity been experienced, and was hospi- specific, integrated questionnaire used to as-
talization necessary because of toxicity. This sess health-related quality of life (QOL) in
questionnaire was developed by a team of doc- cancer patients. The questionnaire incorpo-
tors, nurses, and social workers. After expert ad- rates five functional scales (physical, role, cog-
vice was obtained, the questionnaire was pilot nitive, emotional, and social), three symptom
tested by patients recruited from the National scales (fatigue, pain, as well as nausea and
Cancer Center in Korea. The domain of ‘‘prob- vomiting), a global health and QOL scale,
lems before treatment after diagnosis’’ included and several single items for assessment of ad-
difficulties within the family, poor communica- ditional symptoms commonly reported by
tion with a doctor during diagnosis, and eco- cancer patients (fatigue, nausea/vomiting,
nomic difficulty in meeting treatment costs. pain, dyspnea, appetite loss, insomnia, consti-
These questions had four response options pation, and diarrhea) and the perceived
(there was no problem; there was only a minor financial impact of disease and treatment.23
problem; there were many problems; and there The EORTC QLQ-STO22 is a 22-item ques-
were a great number of problems). Because we tionnaire that measures QOL specifically in
did not assess the number of problems, we just stomach cancer patients. The measure incorpo-
divided the responses into two categories: no rates five multi-item scales (dysphagia, pain, re-
problem and one or more problems. flux, eating, and anxiety) and four single items
Clinical data included information on can- (dry mouth, taste problems, body image, and
cer stage, tumor progress (early vs. advanced), hair loss) covering disease- and treatment-
type of treatment received (surgery, radiation related symptoms and specific emotional con-
therapy, or chemotherapy), comorbid condi- sequences of gastric cancer. Each EORTC
tions, type of surgery (total gastrectomy vs. sub- QLQ-STO22 item was scored according to the
total gastrectomy), time since operation, EORTC manual, with transformation to yield
and the extent of lymphadenectomy (limited scores from 0 to 100. A higher score repre-
lymphadenectomy of the perigastric nodes, sented either a better level of functioning or
extended lymphadenectomy, and others). a higher level of symptom. A score of 33 was
Eastern Cooperative Oncology Group perfor- used as the cutoff point for functional assess-
mance status (ECOG PS) is an observer-rated ment and 66 for symptom evaluation.24,25
scale of a patient’s physical ability using num- The reliability coefficients (as measured by
bers ranging from 0 (able to carry out all normal Cronbach’s alpha) and score distribution are
activities) to 4 (completely disabled). As the sub- presented in Table 1.
jects of this study were disease-free stomach can-
cer survivors, respondents were divided into two Statistical Analysis
groups, those with scores of 0 and those with We calculated the descriptive statistics for
scores of one or above.20 demographic, clinical, and therapeutic vari-
ables using a t-test and a Chi-squared test,
Instruments and the differences in observed characteristics
We used the BDI to measure the level of between respondents and nonrespondents can
depression.21 The BDI evaluates 21 symptoms lead to biased estimates. To minimize the bias
of depression, exploring both cognitive- between a respondent and nonrespondent, we
affective and somatic aspects of the condition. used a response propensity-weighted analysis,
Each symptom is rated on a four-point scale with weights equal to the inverse of the proba-
(0 through 3), and the scores are added to bility that a patient completed the survey in
give a total score between 0 and 63. Higher Table 2. For all individuals, a propensity score
scores represent more severe depression. The is the probability of being treated based on
Korean version of the BDI has been standard- observed characteristics (age, gender, cancer
ized,22 but the cutoff scores for the BDI have stage, tumor progress, operation type, time
not been validated in Korean cancer patients. since operation, and need for dissection).Vol. 46 No. 4 October 2013 Depression in Disease-Free Stomach Cancer Survivors 515
Table 1
Internal Consistency and Score Distribution
Range
n Cronbach’s Alpha Possible Actual Mean SD
BDI 344 0.921 0e63 0e38 13.2 8.5
EORTC QLQ-C30
Global quality of life 389 0.873 0e100 0e100 69.8 20.7
Functional scales
Physical functioning 380 0.691 33.3e100 81.2 14.3
Role functioning 390 0.777 0e100 78.5 22.5
Emotional functioning 382 0.859 8.3e100 79.4 20.2
Cognitive functioning 386 0.496 16.7e100 79.2 17.8
Social functioning 383 0.865 0e100 79.3 24.6
Symptom scales 371 0.840 0e79.5 20.8 13.8
EORTC QLQ-STO22
STODYS (dysphagia) 385 0.543 0e100 0e77.8 14.2 15.2
STOPAIN (pain) 382 0.724 0e83.3 19.2 16.9
STORFX (reflux) 382 0.705 0e88.9 14.5 18.5
STOEAT (eating) 387 0.750 0e91.7 18.8 17.9
STOANX (anxiety) 382 0.703 0e100 36.7 24.2
STODM (dry mouth) 385 0e100 25.9 28.8
STOTA (taste problems) 387 0e100 9.6 17.9
STOBI (body image) 386 0e100 36.2 33.6
STOHAIR (hair loss) 163 0e100 29.0 30.6
BDI ¼ Beck Depression Inventory; EORTC QLQ-C30 ¼ European Organization for Research and Treatment of Cancer Quality of Life
Questionnaire-Core 30; EORTC QLQ-STO22 ¼ European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-
Stomach Cancer Module 22.
We used response propensity-weighted analy- Answers were treated as binary outcomes,
sis, with weights equal to the inverse of the and we used univariate logistic regression anal-
probabilities (weighted number ¼ 726).26 ysis to estimate the odds ratio (OR) for each
Table 2
Characteristics of Those Who Did and Did Not Respond to the Questionnaires
Responders Nonresponders
(n ¼ 391) (n ¼ 349)
Adjusted
n (%) n (%) P Pa
Age, yrs; mean SD 54.5 10.6 57.0 11.6516 Han et al. Vol. 46 No. 4 October 2013
independent variable (demographic and clini- care process subquestionnaires, comorbidity,
cal variables, care process parameters, prob- a poor ECOG PS, treatment with chemother-
lems with functioning, and symptoms). We apy, recognition of the importance of patient
applied a forward (and backward) stepwise input into decision making, and problems be-
procedure to fit a logistic regression model fore treatment were all associated with depres-
with the entry (and removal) level of 0.15. In sion (P < 0.05 for all comparisons).
the following order, we included variables Global QOL, role function, emotional func-
that showed statistical significance at the 0.10 tion, cognitive function, and social function
level in their univariate relationship with the problems also were associated with depression.
outcome variable: monthly household income, All symptomatic variables were significantly
comorbidity, ECOG PS, chemotherapy, recog- associated with a high risk of depression
nition of own opinion in decision making, (P < 0.05) (Table 4).
problems before treatment, and all problem-
atic group variables except physical function- Multivariate Logistic Regression Modeling of
ing. Finally, we used a hierarchical variable Factors Associated With Depression
selection method, which compared models Table 5 shows the results of a multivariate
that included the statistically and clinically sig- analysis of factors associated, by univariate anal-
nificant variables. Results were expressed as ysis, with a predisposition to depression. Survi-
ORs with 95% CIs. All data were analyzed using vors with lower monthly household incomes
SAS version 8.0 (SAS Institute, Cary, NC). had significantly more depression than
higher income survivors (OR 2.49; 95% CI
1.64e3.78). Those who had experienced prob-
Results lems before treatment were more depressed
than the subjects who had not experienced
Patient Characteristics
such difficulties (OR 1.92; 95% CI 1.23e2.98).
Respondents differed from nonrespondents
Subjects who had experienced a change in
in that the men-to-women ratio of respondents
body image were more depressed than those
was greater, respondents were of a younger
who did not suffer from such a change (OR
age, and a greater proportion had been ini-
2.23; 95% CI 1.41e3.53). Subjects with symp-
tially diagnosed with early-stage disease. We
toms including fatigue (OR 3.11; 95% CI
used response propensity-weighted analysis,
1.49e6.52), dyspnea (OR 2.57; 95% CI
with each weight being equal to the inverse
1.48e4.45), or insomnia (OR 4.51; 95% CI
of the probability that a subject completed
1.88e10.83) were more depressed than subjects
the survey (Table 2).
who did not experience these problems.
The mean ( SD) subject age was 54.5 10.6
years, and the mean time since surgery was
27.5 3.4 months. The mean depression score
for stomach cancer patients was 13.3 8.7 Discussion
when the full BDI was used. Treatment of cancer patients always has a cu-
rative intent, and, to date, most post-treatment
Univariate Logistic Regression Analysis for studies have focused on the incidence of can-
Factors Associated With Depression cer recurrence. However, as the number of
Overall, 43.9% of scores were equal to or long-term survivors of cancer increases, atten-
greater than the cutoff value of 13 and 19.7% tion has been increasingly directed toward
were at least 21.14 More women (49%) than treatment-related sequelae and their effects
men (42%) had high depression scores. on patient QOL, including depression.27
Table 3 lists the statistically significant fac- In the present study, the BDI scores of al-
tors associated with subject depression (BDI most 50% of patients indicated the presence
score >13 vs. #13) by univariate analysis. of depression. Overall, 43.9% of scores were
Stomach cancer subjects with low monthly greater than the cutoff value of 13. We found
household incomes were at a significantly that lower monthly household income, an ex-
higher risk of depression (P < 0.001). Among perience of many problems before treatment,
the variables evaluated in the clinical and any change in body image, and symptomsVol. 46 No. 4 October 2013 Depression in Disease-Free Stomach Cancer Survivors 517
Table 3
Association of Sociodemographic, Clinical, and Care Process Variables With Depression by Univariate Logistic
Analysis
BDI Score Analysis
#13% a
>13% a
OR (95% CI) Pb
Sociodemographic
Age (yrs)
$50 58.9 41.1
$2200 USD 66.7 33.3518 Han et al. Vol. 46 No. 4 October 2013
Table 3
Continued
BDI Score Analysis
#13%a >13%a OR (95% CI) Pb
Regular follow-up
Yes 56.5 43.5
No 45.9 54.1 1.52 (0.82e2.82) 0.177
Treatment satisfaction
Yes 58.2 41.8
No 42.9 57.1 1.51 (0.77e2.94) 0.221
Treatment toxicity
No 59.9 40.1
Yes 55.8 44.2 1.18 (0.39e3.55) 0.762
Hospitalization
No 56.2 43.8
Yes 41.3 58.7 1.82 (0.81e4.06) 0.143
BDI ¼ Beck Depression Inventory; OR ¼ odds ratio; ECOG PS ¼ Eastern Cooperative Oncology Group performance status.
a
All estimates weighted to the total eligible stomach cancer survivors (weighted n ¼ 726).
b
Wald test, univariate logistic regression model.
such as fatigue, dyspnea, and insomnia were all 18% moderate) prevalence of depression
significantly associated with depression. Two among 62 adults hospitalized in oncology
reports using both the Diagnostic and Statistical units28 and a 33% prevalence in 80 hospital-
Manual of Mental Disorders (Third Edition) cri- ized adults with advanced cancer.29 Also, 57%
teria and the BDI found a 42% (24% severe, of all cancer patients included in a previous
Table 4
Association of Problematic Group Variables With Depression by Univariate Logistic Analysis
BDI Score Analysis
#13% a
>13% a
OR (95% CI) Pb
Functional problemsc
Global quality of life 32.6 67.4 2.84 (1.59e5.05)Vol. 46 No. 4 October 2013 Depression in Disease-Free Stomach Cancer Survivors 519
Table 5 to specific associated factors for depression.
Factors Associated With Depression by Stepwise Furthermore, psychological distress caused by
Multiple Logistic Regression Analysis
a cumulative number of difficulties would be
Analysis expected to affect QOL after treatment.
Associated Factors OR 95% CI Pa In previous reports, a depressive mood ap-
peared to be an important predictor of
Monthly household 2.49 1.64e3.78520 Han et al. Vol. 46 No. 4 October 2013
and fatigue, no evidence was found to facilitate overlap with somatic symptoms in cancer pop-
understanding of their causalities.43 ulations. However, the present literature sug-
Stomach cancer patients suffer from particu- gests that several methods currently used to
lar digestive problems that can have an intense evaluate psychological distress prevalence in
negative effect on psychological adjustment.17 cancer patients are valid, although the defini-
Such patients may have to cope with severe eat- tion and measurement of such distress have
ing problems, significant weight loss, nausea varied substantially among studies.37
and vomiting, abdominal discomfort, diarrhea, In conclusion, the prevalence of BDI-
or constipation and other disease-related prob- diagnosed depression was high in stomach
lems that are difficult to manage. Although sur- cancer survivors, even after the completion of
gery is potentially curative, serious side effects treatment. We found that depression in
such as postoperative weight loss, loss of appe- disease-free stomach cancer survivors was associ-
tite, fatigue, postprandial symptoms, and other ated with various factors. We believe that our re-
nutritional changes remain.37,44 Therefore, sults constitute the first step toward identifying
stomach cancer survivors should be screened factors associated with depression and provid-
for depression after the end of treatment. Our ing the support needed to reduce such depres-
results indicate that depression could be re- sion in disease-free stomach cancer survivors.
lieved by improved management of pervasive Further psychological interventional studies
troublesome symptoms. are necessary to reduce depression in these sub-
There were several limitations to our study. jects and to improve QOL. In addition, longitu-
First, we were not able to identify cause-and- dinal studies should be conducted to further
effect relationships between the aspects of de- validate the associations discovered in our work.
pression and predisposing factors owing to
the cross-sectional design of the study. Second,
the response rate (52.8%) was somewhat low.
However, this proportion was similar to those Disclosures and Acknowledgments
reported in other cancer survivor studies,45,46 This work was supported by a National
and we minimized the bias by the use of Cancer Center grant (04101502). The authors
response propensity-weighted analysis that declare no conflicts of interest.
should provide a representative picture of the
status of the entire group, including nonre-
spondents. Third, the results cannot be gener-
alized to all stomach cancer survivors because References
the study population was selected from those 1. Brenner H, Rothenbacher D, Arndt V. Epidemi-
treated at only two teaching hospitals in Korea. ology of stomach cancer. Methods Mol Biol 2009;
Additionally, the wide CIs in this study indi- 472:467e477.
cated an inadequate sample size. Further stud- 2. Crew KD, Neugut AI. Epidemiology of gastric
ies are needed to fully address the issue of cancer. World J Gastroenterol 2006;12:354e362.
depression and associated factors in stomach 3. Cancerbackup. Understanding stomach cancer,
cancer survivors. Fourth, in the participants 6th ed. London: Cancerbackup, 2006.
with concomitant physical illness, the BDI’s re-
4. Tsunoda A, Nakao K, Hiratsuka K, et al. Anxiety,
liance on physical symptoms may artificially in- depression and quality of life in colorectal cancer
flate scores because of the illness itself rather patients. Int J Clin Oncol 2005;10:411e417.
than depression. Fifth, a problem checklist de-
5. Bodurka-Bevers D, Basen-Engquist K,
veloped for the study lacked reliability and val- Carmack CL, et al. Depression, anxiety, and quality
idity, and additional studies are needed to of life in patients with epithelial ovarian cancer.
obtain more empirical evidence. Finally, we Gynecol Oncol 2000;78:302e308.
did use the BDI to assess depression instead 6. Alacacioglu A, Yavuzsen T, Dirioz M, Yilmaz U.
of the recognized psychiatric criteria such as Quality of life, anxiety and depression in Turkish
Diagnostic and Statistical Manual of Mental Disor- breast cancer patients and in their husbands. Med
ders (Fourth Edition) criteria; this might lead Oncol 2009;26:415e419.
to a higher prevalence of depression in our 7. Miovic M, Block S. Psychiatric disorders in
study. The BDI has been criticized for its advanced cancer. Cancer 2007;110:1665e1676.Vol. 46 No. 4 October 2013 Depression in Disease-Free Stomach Cancer Survivors 521
8. Massie MJ. Prevalence of depression in patients 23. Yun YH, Park YS, Lee ES, et al. Validation of the
with cancer. J Natl Cancer Inst Monogr 2004; Korean version of the EORTC QLQ-C30. Qual Life
57e71. Res 2004;13:863e868.
9. Honda K, Goodwin RD. Cancer and mental 24. Blazeby JM, Conroy T, Bottomley A, et al. Clini-
disorders in a national community sample: findings cal and psychometric validation of a questionnaire
from the national comorbidity survey. Psychother module, the EORTC QLQ-STO 22, to assess quality
Psychosom 2004;73:235e242. of life in patients with gastric cancer. Eur J Cancer
2004;40:2260e2268.
10. Okano Y, Okamura H, Watanabe T, et al. Mental
adjustment to first recurrence and correlated 25. Fayers PM. Interpreting quality of life data:
factors in patients with breast cancer. Breast Cancer population-based reference data for the EORTC
Res Treat 2001;67:255e262. QLQ-C30. Eur J Cancer 2001;37:1331e1334.
11. Yang MJ, Jeon YW, Han SI, Han CW, Eom HS. 26. Jenkins P, Earle-Richardson G, Burdick P, May J.
Depression and pain in patients with cancer: a pre- Handling nonresponse in surveys: analytic correc-
liminary study. J Korean Neuropsychiatr Assoc 2000; tions compared with converting nonresponders.
39:1122e1131. Am J Epidemiol 2008;167:369e374.
12. Lloyd-Williams M, Shiels C, Taylor F, Dennis M. 27. Polsky D, Doshi JA, Marcus S, et al. Long-term
Depressiondan independent predictor of early risk for depressive symptoms after a medical diagno-
death in patients with advanced cancer. J Affect sis. Arch Intern Med 2005;165:1260e1266.
Disord 2009;113:127e132. 28. Bukberg J, Penman D, Holland JC. Depression
in hospitalized cancer patients. Psychosom Med
13. Breitbart W. Identifying patients at risk for,
1984;46:199e212.
and treatment of major psychiatric complications
of cancer. Support Care Cancer 1995;3:45e60. 29. Plumb MM, Holland J. Comparative studies of
psychological function in patients with advanced
14. Pelletier G, Verhoef MJ, Khatri N, Hagen N. cancerdI. Self-reported depressive symptoms.
Quality of life in brain tumor patients: the relative Psychosom Med 1977;39:264e276.
contributions of depression, fatigue, emotional
distress, and existential issues. J Neurooncol 2002; 30. Hopwood P, Stephens RJ. Depression in pa-
57:41e49. tients with lung cancer: prevalence and risk factors
derived from quality-of-life data. J Clin Oncol
15. Tavoli A, Mohagheghi MA, Montazeri A, et al. 2000;18:893e903.
Anxiety and depression in patients with gastrointes-
tinal cancer: does knowledge of cancer diagnosis 31. Burgess C, Cornelius V, Love S, et al. Depression
matter? BMC Gastroenterol 2007;7:28. and anxiety in women with early breast cancer: five
year observational cohort study. BMJ 2005;330:702.
16. Tiernan E. Depression in terminally ill cancer
patients. Ir Med J 1998;91:47e48. 32. Akechi T, Okuyama T, Imoto S, Yamawaki S,
Uchitomi Y. Biomedical and psychosocial determi-
17. Matsushita T, Matsushima E, Maruyama M. nants of psychiatric morbidity among postoperative
Assessment of peri-operative quality of life in ambulatory breast cancer patients. Breast Cancer
patients undergoing surgery for gastrointestinal Res Treat 2001;65:195e202.
cancer. Support Care Cancer 2004;12:319e325.
33. Ell K, Xie B, Quon B, et al. Randomized con-
18. Rhee YS, Yun YH, Park S, et al. Depression in trolled trial of collaborative care management of
family caregivers of cancer patients: the feeling of depression among low-income patients with cancer.
burden as a predictor of depression. J Clin Oncol J Clin Oncol 2008;26:4488e4496.
2008;26:5890e5895. 34. Ell K, Sanchez K, Vourlekis B, et al. Depression,
19. Bae JM, Kim S, Kim YW, et al. Health-related correlates of depression, and receipt of depression
quality of life among disease-free stomach cancer care among low-income women with breast or gyne-
survivors in Korea. Qual Life Res 2006;15: cologic cancer. J Clin Oncol 2005;23:3052e3060.
1587e1596. 35. Ell K, Xie B, Wells A, et al. Economic stress
20. Oken MM, Creech RH, Tormey DC, et al. Toxic- among low-income women with cancer: effects on
ity and response criteria of the Eastern Cooperative quality of life. Cancer 2008;112:616e625.
Oncology Group. Am J Clin Oncol 1982;5:649e655. 36. Visser MR, Smets EM. Fatigue, depression and
21. Richter P, Werner J, Heerlein A, Kraus A, quality of life in cancer patients: how are they
Sauer H. On the validity of the Beck Depression In- related? Support Care Cancer 1998;6:101e108.
ventory. A review. Psychopathology 1998;31: 37. Vickery CW, Blazeby JM, Conroy T, et al. Devel-
160e168. opment of an EORTC disease-specific quality of life
22. Hahn HM, Yum TH, Shin YW, et al. module for use in patients with gastric cancer. Eur
A standardization study of Beck Depression Inven- J Cancer 2001;37:966e971.
tory in Korea. Korean J Neuropsychiatr 1986;25: 38. Maeda T, Onuoha FN, Munakata T. The effect
487e502. of postoperative symptom experience, and522 Han et al. Vol. 46 No. 4 October 2013 personality and psychosocial factors on depression pain, and fatigue in patients with cancer. J Clin among postgastrectomy patients in Japan. Gastroen- Sleep Med 2009;5:132e136. terol Nurs 2006;29:437e444. 43. Brown LF, Rand KL, Bigatti SM, et al. Longitu- 39. Bower JE, Ganz PA, Desmond KA, et al. Fatigue dinal relationships between fatigue and depression in breast cancer survivors: occurrence, correlates, in cancer patients with depression and/or pain. and impact on quality of life. J Clin Oncol 2000; Health Psychol 2012. [Epub ahead of print]. 18:743e753. 44. Roukos DH. Current advances and changes in 40. Servaes P, Verhagen S, Bleijenberg G. Determi- treatment strategy may improve survival and quality nants of chronic fatigue in disease-free breast can- of life in patients with potentially curable gastric cer patients: a cross-sectional study. Ann Oncol cancer. Ann Surg Oncol 1999;6:46e56. 2002;13:589e598. 45. Sarna L, Padilla G, Holmes C, et al. Quality of 41. Oh H, Seo Y, Jeong H, Seo W. The identification life of long-term survivors of non-small-cell lung of multiple symptom clusters and their effects on cancer. J Clin Oncol 2002;20:2920e2929. functional performance in cancer patients. J Clin 46. Rowland JH, Desmond KA, Meyerowitz BE, Nurs 2012;21:2832e2842. et al. Role of breast reconstructive surgery in physi- 42. Stepanski EJ, Walker MS, Schwartzberg LS, et al. cal and emotional outcomes among breast cancer The relation of trouble sleeping, depressed mood, survivors. J Natl Cancer Inst 2000;92:1422e1429.
You can also read