FACT SHEET Interventions for Positional Foot Deformities in the Neonate
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

FACT SHEET
Interventions for Positional Foot Deformities in the Neonate
INTRODUCTION
Positional foot deformities are common pediatric orthopedic conditions noted at birth that may affect the bones,
tendons, and muscles of the foot. The incidence of neonatal positional foot deformities is difficult to define due
to underreporting of “mild” deformities and a limited delineation between true positional deformity and
congenital malformations in the literature. This underreporting emphasizes the need for therapy practitioners to
understand the deformities and provide appropriate interventions in a timely manner.
Positioning, splinting, therapeutic taping, and casting may be used to treat congenital and acquired
musculoskeletal deformities in preterm and critically ill infants.1-6 Limited evidence exists to support or oppose
the interventions of foot deformity in this population. Advanced training/mentoring for competency is strongly
recommended for managing the positional foot deformity in the neonatal intensive care unit (NICU) (see
resources at: https://pediatricapta.org/special-interest-groups/sigs).1,3 It is vitality important to understand the
immaturity of body systems and physiologic fragility of this population before intervening. It is also important to
note that bone morphology will not change with the applications discussed below.
This fact sheet discusses interventions for the management of flexible aspects of positional foot deformities
often seen in neonates. This fact sheet defines neonates as infants requiring a stay in a medical intensive care
unit. This fact sheet is intended for experienced licensed physical and occupational therapy providers working
with the neonate in the inpatient and outpatient settings. Specific provider roles will be dictated by state and/or
national practice acts.
CLINCIAL REASONING AND DECISION MAKING
Prior to initiating positional corrections, the provider should understand embryologic development, anatomy,
environmental/intrauterine factors, and delivery history to provide the best intervention and to effectively
collaborate with a multidisciplinary team.1-3;7,8,15-18 Table 1 describes the common positional foot deformities
seen with the neonatal population (this does not include deformities associated with genetic disorders).
ASSESSMENT
The physical exam should include an assessment of the following:
● integumentary integrity using visual inspection prior to or along with modalities listed below
● joint integrity - if bony end feel, obtain imaging before proceeding
● passive/active range of motion - assess all soft tissue restrictions while the joints above and below held
in the age appropriate position assess for symmetry in the range of motion
● tone - appropriate by age21,22
● strength - appropriate for age/diagnosis
● sensation - special care must be taken in diagnoses that include altered/absent sensation (i.e.,
myelomeningocele)
● circulation - consult the medical team if there are changes in temperature, color, or girth
● pain assessment/stress before, during and after intervention23-26
● presence of associated deformities (i.e., hip dysplasia)
TABLE 1: Types of Positional Foot Deformities7-14
Deformity Image Clinical Presentation* Flexible/ Grading Treatment
Rigid Scale Interventions
Preterm • Poor progression • Flexible • Positioning
postnatal towards a dorsiflexed • Stretching
positional foot forefoot with age- • Splinting
deformation* appropriate calcaneal • Taping
position
Metatarsus • Flexible hindfoot • Flexible: • Bleck Flexible:
Adductus** mild to Scale • Stretching
(MTA) • Metatarsals deviate moderate • Splinting
medially • Taping
• Rigid: Rigid:
Severe • Casting
• Surgical
intervention
Calcaneovalgus# • Excessive hindfoot • Flexible • Stretching
dorsiflexion • Splinting
• Taping
Talipes • Cavus • Extrinsic – • Dimeglio Extrinsic:
Equinovarus • Adduction of forefoot soft tissue Scale • Splining
(TEV) • Varus of hindfoot flexibility • Pirani • Taping
(clubfoot)## • Equinus • Intrinsic – Score • Casting
• Leg Internally rotated rigid bony Intrinsic:
frame • Surgical
intervention
Congenital • Talus valgus/equinus • Rigid • Casting
Vertical Talus • Talonavicular joint is • Surgical
(CVT) dislocated (rocker intervention
(rockerbottom bottom)
foot)^ • Forefoot dorsiflexed
For differential diagnoses, x-ray images, and comorbidities, please see the reference by Gore & Spencer, 2004.9
Images retrieved from:
* Photo courtesy of Audrey Wood
** https://www.orthobullets.com/pediatrics/4061/metatarsus-adductus
# https://www.orthobullets.com/pediatrics/4067/calcaneovalgus-foot
## https://orthokids.org/en-US/Condition/Clubfoot
^ https://orthokids.org/Condition/Vertical-Talus
May 2021 APTA Pediatrics Fact Sheets | 2
Table 2 below lists considerations to assess prior to developing a plan of care. Request appropriate referrals
as needed. For infants in the immediate newborn period, or those who are very premature, start with the most
conservative interventions to assess progression before intervening.
TABLE 2: Contraindications/Precautions3,16,19,20
Contraindications Precautions Other Considerations
Infants on minimal handling protocols Fragile/immature skin (may Application of distal weight on
due to physiologic instability shear or blister the skin) proximal joint
Acute fracture Osteopenia/metabolic bone Need for heel sticks (blood draw)
disease/fragile bones
Skin breakdown/open wounds Fluctuating Pain/stress when
Edema/lymphatic donning/doffing/creating device
dysfunction
Impaired perfusion Paralysis/Sedation Impact on infant’s movements
Fixed deformity Vascular Access (current or Coordination/support of
future) multidisciplinary providers and family
Impaired Sensation Need for imaging studies for bone
formation and alignment
Sensitivity to materials.
Infants < 34 weeks Post
Menstrual Age (PMA)
GOALS FOR INTERVENTIONS1,27-29
• Achieve functional position/alignment
• Prevent loss of range and/or manage contractures
• Address family/caregiver goals
• Family/caregiver education
• Minimize the need for surgical intervention
INTERVENTION PRINCIPLES
• Address the following clinical principles before providing an intervention:
o The physiologic stability of the neonate
o Family goals and infant's disposition19,27
● Parents should hold and support their baby, if possible,19
● Use non-pharmacologic comfort strategies such as23,30:
o Non-nutritive sucking with or without sucrose solution or breast milk,
o Hand or blanket swaddling containment in a flexed posture, and
o Skin to skin holding after the intervention.
● Minimize/prevent overcorrection as due to varying degrees of hypotonia, ligamentous, and connective
tissue laxity based on age,15,31 and neonates’ tissues respond quickly to deformational forces.1
● Understand that muscular fatigue is a result of decreased type I muscle fibers compared to type II
depending on the gestational age.21,22,31
● Use a low-load and prolonged stretch for soft tissue restrictions and reassess continuously to adapt the
intervention based on tolerance, results and family goals.
May 2021 APTA Pediatrics Fact Sheets | 3
INTERVENTIONS
The interventions listed below are suggestions for correction. Use of techniques and materials depend on
access, training, and the patient’s response to the treatment. Several methods may be used for one patient
during the course of the correction to achieve optimal alignment. Address postural deviations in the trunk, hip
and knee before or concurrently with interventions at the foot for a comprehensive outcome.
Passive Positioning
Prior to 34-35 weeks PMA, correct age appropriate positioning is imperative for encouraging proper alignment.
We encourage the reader to review the Positioning of the Medically Fragile Infant Fact Sheet (on the APTA
Academy of Pediatric Therapy webpage). Passive positioning (via blanket roll with or without positioning
devices) may also be used in conjunction with other interventions.
Range of Motion Exercises3,9
Range of motion should start with passive range to address soft tissue restriction within the limitations of bony
abnormalities, if present. This can be taught to the parents or may be accomplished by proper positioning in a
positioning device. Progress to active assist/active range of motion based on age and strength. Active
strengthening is crucial to facilitating a neuromuscular change.
Manual Therapies
Limited evidence exists for interventions such as myofascial release or massage for soft tissue restrictions in
this population. These techniques may enhance the outcomes of the more traditional/studied methods. Assess
the infant’s response 20-30 minutes after the intervention to ensure patient tolerance.32
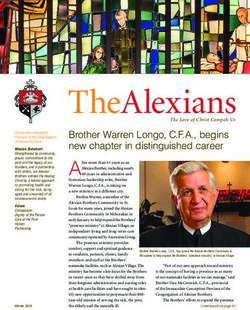
Splinting
Consider the precautions stated above and the implications of a splint on posture and active movement. While
thermoplastic materials can be contoured to the foot to address the deformity, care must be taken to protect
fragile skin from heat.
Splinting materials can include:
●
foam,
●
an IV board,
●
soft wrapping,
●
neoprene fabric,
●
soft strapping material, or
●
molded lightweight, low-temperature thermoplastic materials.3,4
Examples of neonatal foot splints:
Photo’s courtesy of Roberta Gaitlin and Audrey Wood
Consider the ease of donning and doffing the splint by nursing and families for the best outcomes and overall
compliance. Establish a wearing schedule based on the infant's tolerance to the splint. The wearing schedule
will progress from a short to a longer duration with the patient’s medical status, intervention needs/goals, and
May 2021 APTA Pediatrics Fact Sheets | 4age guiding the schedule. An example of a wearing schedule is 3-4 hours corresponding with cares.3 Assess
tolerance and need for splint modifications by careful examination of skin integrity, perfusion, changes in
alignment, and comfort while the splint is donned. Monitor splints carefully monitored to ensure that the desired
alignment is maintained throughout the wearing time. Movement within the splint, active movement or altered
muscle tone, can result in loss of optimal alignment and increase the risk for pressure injury to the skin.
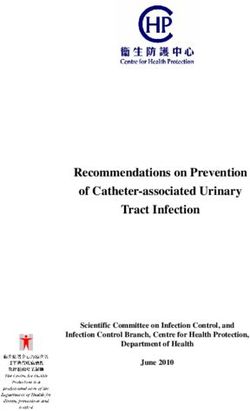
Taping
There are two major classifications of tape available: rigid/nonelastic or elastic. Rigid tape refers to a medical
grade tape that does not have extensibility. Elastic taping refers to a light weight non-medicated tape that has
stretch properties.33 Tape is indicated only if minimal assistance is needed manually for a positional correction.
Currently, there is limited research available on the use of either tape in the neonatal population. Taping should
only be used on a patient with intact skin integrity and no known skin sensitivities. A skin preparation solution
can be used per hospital guidelines/policies. For rigid tape, use care in the application to prevent shear
stresses on the skin. In some instances, it may be prudent to use a type of underwrap to protect the skin.
Elastic tape should not be used in a heated environment, if the adhesive is heat activated. Advantages of
elastic tape include:
● does not require periodic donning/doffing by non-therapy clinicians,
● minimal time and handling to apply,
● may be used in the presence of fluctuating edema,
● may be used with other positioning aids or techniques,
● may be used to address other factors affecting positioning such as scar tissue tightness or tight
opposing muscles.
Examples of elastic tape application for muscle or fascial relaxation:
Photo’s courtesy of Anjali Gupta
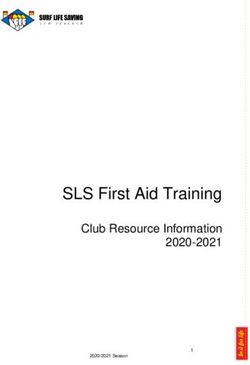
Casting
Casting, typically applied by an orthopedic surgeon, may be reserved for the more rigid deformity. Serial
casting generally is deferred in the NICU setting because of the numerous acute and chronic medical
conditions.14,35,36 Recently, studies show mixed results warranting further research and discussion regarding
the risks and benefits of early correction in medically fragile neonates.14,34
Ponsetti cast applied by Orthopedics
Photo courtesy of Audrey Wood
May 2021 APTA Pediatrics Fact Sheets | 5EDUCATION AND DISCHARGE PLANNING
Families and other caregivers need to understand the purpose, goals, and the plan of care for the chosen
intervention. Goals should align with family goals and priorities.27-29,37 Teamwork is essential for safe
management and compliance. Information regarding the intervention should be readily available at the bedside
and in the patient's medical record. Education should meet the learning preferences of the family.29,37
TABLE 3: Education Recommendations
General education
● Purpose and goals of the intervention
● Skin checks (irritation/rash, signs of pressure)
● Vascular checks (color, temperature, capillary refill)
● Edema assessment
● Behavioral assessment by infant (irritability, crying)
● What to do to address intolerance by infant
● Contact information for PT to address concerns
Splinting specific education
● Safe donning and doffing of splints
● Wearing time
● Signs that splint wearing should be put on hold
Taping specific education
● Safe application of tape after instruction & mentored practice
● Safe removal of tape
● Signs tape needs to be replaced
Casting specific education
● Safe removal of cast
● Signs cast needs to be removed or replaced
Exercises/HEP may include:
● Stretching
● Positioning to promote optimal alignment
● Facilitation of active movement
● Education for specific modalities as described above
● HEP should be family centered & incorporated into daily routines
Discharge Planning/Transition to home
● Ensure follow up with the appropriate medical team(s)
● Ensure parent/caregiver comfort and independence with HEP
● Referral to Early Intervention program/outpatient therapy
● The health care team must follow up with the family after discharge to confirm that referrals are
completed and the family remains comfortable with care for the infant.
SUMMARY OF KEY POINTS
While the incidence of positional foot deformities is unknown in the neonatal population, steps should be taken
to mitigate or correct these issues based on the physiologic maturity and stability of the neonate. Rule out any
bony malformations or other barriers to a safe and successful intervention before beginning interventions.
Specific training/mentorship is strongly recommended prior to beginning. Collaboration should occur with the
care team including the parents/primary care providers of the child. Clear and concise instructions and
indications to discontinue use should be clearly posted for all bedside providers to see. Plan for continuation of
care with the appropriate providers as the child moves from one care setting to another.
May 2021 APTA Pediatrics Fact Sheets | 6REFERENCES
1. Sweeney JK, Heriza HB, Blanchard Y. Neonatal physical therapy: clinical competencies and NICU
clinical training models. Part I. Pediatr Phys Ther. 2009;21:296-307.
2. Sweeney JK, Heriza CB, Blanchard Y, et al. Neonatal physical therapy. Part II: practice frameworks
and evidence-based practice guidelines. Pediatr Phys Ther. 2010;22:2-16.
3. Sweeney JK, Gutierrez T, Beachy JC. Medical and developmental challenges of infants in neonatal
intensive care: management and follow-up considerations. In Lazaro RT, Reina-Guerra SG, Quiben
MU, eds. Umphred’s Neurological Rehabilitation. 7th edition. St Louis MO. 2020.
4. Byrne E, Garber J. Physical therapy intervention in the neonatal intensive care unit. Phys Occupat Ther
Pediatr. 2013;33(1):75-110.
5. Ross K, Heiny E, Conner S. Occupational therapy, physical therapy, and speech-language pathology in
the neonatal intensive care unit: patterns of therapy usage in the level IV NICU. Res Dev Disabil.
2017;64:108-117.
6. Borges P, Snider L, Camelo JS, Boychuck Z, et al. The role of rehabilitation specialists in Canadian
NICUs: A 21st century perspective. Phys Occupat Therapy Pediatr. 2019;39(1):33-47.
7. Furdon SA, Reu Donlon C. Examination of the Newborn Foot: Positional and Structural
Abnormalities. Adv Neonatal Care. 2002;2(9):248-258.
8. Fuller DA, Raphael JS. Extensor tendon lacerations in preterm neonate. J Hand Surgery. 1999;
24A:628-632.
9. Gore AI, Spencer JP. The newborn foot. Am Fam Physician. 2004;69(4):865-72. PMID: 14989573.
10. Gray K, Pacey V, Gibbons P, Little D, Burns J. Interventions for congenital talipes equinovarus
(clubfoot). Cochrane Database Syst Rev. 2014;(8). doi:10.1002/14651858.cd008602.pub3.
11. Bettuzzi C, Abati CN, Salvatori G, Zanardi A, Lampasi M. Interobserver reliability of Diméglio and Pirani
score and their subcomponents in the evaluation of idiopathic clubfoot in a clinical setting: a need for
improved scoring systems. J Child Orthop. 2019;13(5):478-485. doi:10.1302/1863-2548.13.190010.
12. Dobbs MB, Purcell DB, Nunley R, Morcuende JA. Early Results of a New Method of Treatment for
Idiopathic Congenital Vertical Talus. J Bone Joint Surg. 2006;88(6):1192-1200.
doi:10.2106/jbjs.e.00402.
13. Aslani H, Sadigi A, Tabrizi A, Bazavar M, Mousavi M. Primary outcomes of the congenital vertical talus
correction using the Dobbs method of serial casting and limited surgery. J Child Orthop. 2012;6(4):307-
11.
14. Tanta KJ, Gunsolus K, Harley N, et al. Complications in the neonatal intensive care unit: brachial
plexus injuries and clubfoot. J Occup Ther Sch Early Interv. 2012;5: 275-292.
15. Sweeney JK, Gutierrez T. Musculoskeletal implications of preterm infant positioning in the NICU. J
Perinatal Neonatal Nurs. 2002;16(1):58-70.
16. Visscher MO, Adam R, Brink S, Odio M. Newborn infant skin: physiology, development, and care. Clin
Dermatol. 2015;33:271-280.
17. Solopova IA, Zhvansky DS, Dolinskaya IY, et al. Muscle Responses to Passive Joint Movements in
Infants During the First Year of Life. Front Physiol. 2019;10:1158. Published 2019 Sep 13.
doi:10.3389/fphys.2019.01158.
18. Furze J, Kenyon LK, Jensen GM. Connecting Classroom, Clinic, and Context. Pediatr Phys Ther.
2015;27(4):368-375. doi:10.1097/pep.0000000000000185.
19. Coughlin ME. Trauma-informed care in the NICU: evidence-based practice guidelines for neonatal
clinicians. New York. Springer Publishing Co. 2017.
20. Dabezies E, Warren P. Fractures in Very Low Birth Weight Infants with Rickets. Clin Orthop.
1997;335:233-239.
21. Amiel-Tison C. Neurological evolution of the maturity of newborn infants. Arch Dis Child. 1968;43:89-
93.
May 2021 APTA Pediatrics Fact Sheets | 722. Allen MC, Capute AJ. Tone and reflex development before term. Pediatr Suppl. 1990;85:393-399.
23. Field T. Preterm newborn research review. Infant Behavior Devel. 2017;49:141-150.
24. AAP Committee on Fetus and Newborn and Section on Anesthesiology and Pain Medicine. Prevention
and management of procedural pain in the neonate: an update. Pediatrics. 2016;137(2):e20154271.
25. Byrne E, Campbell SK. Physical therapy observation and assessment in the intensive care unit
neonatal care unit. Phys Occup Ther Pediatr. 2013;33(1):39-74.
26. Holsti L, Gruna RE, Oberlander TF, et al. Body movements: an important additional factor in
discriminating pain from stress in preterm infants. Clin J Pain. 2005;21:491-498.
27. Goldstein LA. Family support education. Phys Occup Ther Pediatr. 2013;33(1):139-161.
28. Hall SL, Hynan MT, Phillips R, et al. The neonatal intensive parenting unit: an introduction. J Perinatol.
2017;37:1259-1264.
29. Byrne E, Sweeney JK, Schwartz N, et al. Effects of instruction on parent competency during infant
handling in the neonatal intensive care unit. Pediatr Phys Ther. 2019;31:43-49.
30. Hatfield LA, Murphy N, Karp K, Polomano RC. A systematic review of behavioral and environmental
interventions for procedural pain management in preterm infants. J Pediatr Nurs. 2019;44:22-30.
31. Grant-Beuttler M, Palisano R, Miller D, et al. Gastrocnemius-Soleus Muscle Tendon Unit Changes
Over the First 12 Weeks of Adjusted Age in Infants Born Preterm. Physical therapy. 2009;89:36-48.
32. Parnell Prevost C, Gleberzon B, Carleo B, Anderson K, Cark M, Pohlman KA. Manual therapy for the
pediatric population: a systematic review. BMC Complement Altern Med. 2019 Mar 13;19(1):60. doi:
10.1186/s12906-019-2447-2. PMID: 30866915; PMCID: PMC6417069.
33. Boonkerd C, Limroongreungrat W. Elastic Therapeutic tape: do they have the same material
properties? J. Phys. Ther. Sci. 2016;28:303-1306.
34. Lebel E, Weinberg E, Berenstein-Weyel TM, Bromiker R. Early application of the Ponseti casting
technique for clubfoot correction in sick infants at the neonatal intensive care unit. J Pediatr Orthop B.
2017;26(2):108-111. doi:10.1097/bpb.0000000000000363
35. Cooper DM, Dietz FR. Treatment of idiopathic clubfoot. A thirty-year follow-up note. J Bone Joint Sug
Am. 1995;77-A(10):1447-89.
36. Sankar WN, Weiss J, Skaggs DL. Orthopaedic Conditions in the Newborn. J Am Acad Orthop Surg.
2009;17(2):112-122. doi:10.5435/00124635-200902000-00007.
37. Dusing SC, Murray T, Stern M. Parent preferences for motor development education in the neonatal
intensive care unit. Pediatr Phys Ther. 2008;20:363-368.
ADDITIONAL RESOURCES
• Academy of Pediatric Physical Therapy, Neonatal Physical Therapy Practice: Roles and Training Fact
Sheet. Available at: https://pediatricapta.org/fact-sheets/
• Neonatal Didactic Training Resource List. Available at: https://pediatricapta.org/special-interest-
groups/NN/pdfs/Neonatal%20Didactic%20Training%20Resource%20list.pdf?v=2
©2021 by the APTA Academy of Pediatric Physical Therapy, American Physical Therapy Association,
1020 N Fairfax St, Suite 400, Alexandria, VA 22314, www.pediatricapta.org
Supported by the Practice Committee of APTA Pediatrics. Developed by expert contributors: Audrey
Wood, PT, MS, DPT, Board-Certified Pediatric Clinical Specialist & Anjali Gupta, PT, MS, CLT.
The APTA Academy of Pediatric Physical Therapy provides access to these member-produced fact
sheets and resources for informational purposes only. They are not intended to represent the position
of APTA Pediatrics or of the American Physical Therapy Association.
May 2021 APTA Pediatrics Fact Sheets | 8You can also read