Experience better with Moda Health and Delta Dental - Oregon 2022 | Affinity Individual & family
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Experience better
with Moda Health
and Delta Dental
Oregon 2022 | Affinity
Individual & family
We’re committed to making
healthcare work better for everyone. Welcome to Moda Health Table of contents
We realize that truly standing by this commitment means and Delta Dental Plan of
understanding that this goal isn’t one of equality – it’s one of equity. Oregon, the place you � Medical plans
It means truly seeing our members, hearing their unique needs, and go when you want to Overview . . . . . . . . . . . . . . . . . . . . . . . . . . 4
acknowledging that those unique needs are often directly tied to experience better — better How your health plan works . . . . . . . . . . . 6
systemic disparities that exist in not only the communities we serve, people, better plans, better Medical networks . . . . . . . . . . . . . . . . . . . . . 8
Picking a medical plan . . . . . . . . . . . . . . . . .10
but also throughout our entire country. And paramount to being services and better health.
Benefit tables . . . . . . . . . . . . . . . . . . . . . . . 12
empowered with this knowledge, it means doing everything we can
Gold plans . . . . . . . . . . . . . . . . . . . . . . . 12
to understand how to participate in building a more just society. Silver plans . . . . . . . . . . . . . . . . . . . . . . .14
As a company, we have been working for many years to forge Bronze plans . . . . . . . . . . . . . . . . . . . . . .18
ways that weave the pillars of DEI into everything we do. High-Deductible health plans . . . . . . . . . . . 20
Overview . . . . . . . . . . . . . . . . . . . . . . . . 20
Benefit table . . . . . . . . . . . . . . . . . . . . . . 21
Diversity: Equity: Inclusion: Limitations and exclusions . . . . . . . . . . . 22
We value, respect and We strive to understand the We are committed to creating
celebrate people of all underlying causes of outcome environments wherein every � Dental plans
backgrounds, identities, and disparities and actively work individual has an equal Overview . . . . . . . . . . . . . . . . . . . . . . . . . 24
abilities and actively seek toward increasing justice and opportunity to belong and
to identify how uniqueness fairness in our processes, can be recognized for their Dental network . . . . . . . . . . . . . . . . . . . . . 25
makes us better. procedures and systems – inherent worth and dignity. Benefit tables . . . . . . . . . . . . . . . . . . . . . . 26
both within our company and
within our communities. Limitations and exclusions . . . . . . . . . . . . . 28
Plan premiums . . . . . . . . . . . . . . . . . . . . . 29
Social injustices have served as a reminder of how crucial it is for these elements to be a � Member care resources
measure in doing right by our employees and communities. Crises that disproportionately
Member website . . . . . . . . . . . . . . . . . . . . 30
affect communities of color and other marginalized groups continue to leave us
feeling helpless at times. But at our core, we believe that with a new day comes the Online health tools . . . . . . . . . . . . . . . . . . . 31
opportunity to be better – to work harder and faster to create measurable change.
Through this lens, continuing to establish equity within our own walls is crucial. By not just building � Tips and terms
a more diverse workforce, but also by supporting that workforce through inclusion, education, and Answers to questions . . . . . . . . . . . . . . . . . 35
opportunity. And by creating spaces that allow for crucial conversations and transparency at all levels.
Glossary . . . . . . . . . . . . . . . . . . . . . . . . . . 37
We fully embrace these efforts that will better equip us to support our communities. We know
these goals will not be achieved overnight, but they are achievable and we are committed.
We will be better. We will do better. It is the right
thing to do and we expect it of ourselves.
3
Medical plans
Better plans
for the real you.
You have a lot to think about when choosing the right medical benefits for you and Affinity EPO Network • Salem Health
your family. Our exclusive provider organization (EPO) plans connect you with your The Affinity EPO Network is designed to offer • Sky Lakes Medical Center
primary care provider (PCP), who works closely with the rest of your care team a personalized care experience that helps • St. Alphonsus Regional Medical Center
(other providers, specialists, etc.) to help you achieve better health and wellness. members, like you, find their way to better • St. Charles Health Center
care, value and health. The Affinity EPO
Network offers access to a community of
• St. Luke’s Regional Medical Center
quality providers that you can choose from: • Wallowa Memorial Hospital
To help you manage your health, you Choose an • Blue Mountain Hospital For conditions that require treatment
will be required to select an in-network
PCP. By establishing a relationship with in-network provider • CHI - St. Anthony Hospital at OHSU or if a referral is made to
OHSU, the Affinity EPO network
a PCP, we can work together to achieve
your health and wellness goals based
All plans are connected to the Affinity EPO • Good Shepherd does offer access to OHSU.
Network. There are no out-of-network
on your history and preferences. benefits with an EPO plan except as • Grande Ronde Hospital The Affinity EPO Network is available
Our plans support your personal healthcare stated in the member handbook. Your • Harney District Hospital for residents of Baker, Crook, Douglas,
needs through partnerships between healthcare provider and specialists must • Lake Health District Gilliam, Grant, Harney, Jefferson,
you, Moda Health, and your in-network be in the Affinity EPO Network or you will be
responsible for the full cost of out-of-network
• Mercy Medical Center Klamath, Lake, Lane, Malheur, Marion,
Morrow, Polk, Sherman, Umatilla, Union,
providers. Once you’ve selected a PCP,
services except when prohibited by law. • Morrow County Health District Wallowa and Wheeler counties.
our plans use the Affinity EPO Network to
provide cost-effective, coordinated care If you have children you want to cover who
• Peace Health
on your journey to better overall health. live outside of Oregon but in the US, they
may be eligible for out-of-area benefits
if they are full-time students age 18 to 26
or if you have a qualified medical child
support order (QMCSO). In Oregon, all of
your enrolled family members must use
the Affinity network to be covered.
As a member, you choose from a list of quality
in-network providers to access care that’s
right for you. Moda Health does not require
a referral for in-network specialist care.
How to select an in-network PCP
As part of your enrollment, an in-network
PCP must be selected for each applicant.
Female members can pick a women's
healthcare provider, and enrolled
children may choose a pediatrician.
All plans are connected to the Moda Health may assign a PCP to
Affinity EPO Network. There members who do not select one.
are no out-of-network benefits
with an EPO plan except
as stated in the member
handbook. Your healthcare
provider and specialists
must be in the Affinity EPO
Network or you may be
responsible for the full cost
of out-of-network services.
4 5
Know your medical plan
How your health
plan works
We're here to help you experience better, and part of experiencing better HDHP plans Deciding on a plan
health is understanding how your health plan works. When you get to Our high-deductible health plans (HDHP) are Plans vary by premiums, deductibles, copays
know your health plan, you can get the most out of your benefits. compatible with a health savings account and coinsurance. Understanding these
(HSA). Having an HDHP gives you the factors can help you pick the right plan.
flexibility and choice to use tax-free funds Generally, you’ll pay more for covered
for eligible healthcare expenses. You can use doctor visits and other services with a
Preventive care matters TruHearing HSA tax-free dollars to pay for deductibles, lower-premium plan. A higher-premium plan
Regular checkups are vital to staying Hearing aids are costly. Using TruHearing coinsurance and other qualified expenses shares more of those costs, so you’ll pay
well. And, when you feel good, it’s makes them more affordable. Eligible not covered by your health plan. Simply check less out-of-pocket for care. Metallic levels
easier to create healthy moments. members can get a routine hearing aid to see if your financial institution has an (listed below) can help you narrow down
Preventive care services include: exam and hearing aids through TruHearing. HSA option or use our partner, BenefitHelp what you’ll pay each month for coverage.
Solutions to set up an HSA account.
• Preventive health exams To learn more, log into your Member
Dashboard at modahealth.com
• Well-baby care
• Women’s annual exams CirrusMD
• Many immunizations Text a doctor
• Colorectal cancer and other screenings Enjoy fast and private access to a
dedicated doctor in under a minute — at
Medication tiers offer ways to save no cost to you*. With the CirrusMD app,
All of our medical plans include prescription all you need is Internet access to:
benefits. These benefits connect you with
our Preferred Drug Program, a way to save
• Connect with a doctor via text, 24/7,
without appointments or time limits
money on safe and effective prescription
medications. Through the program, plans • Ask urgent or general health questions
cover prescriptions by these medication • Message, share photos or video chat
tiers: value, select, preferred, non- • Get peace of mind, even at 2 a.m.
preferred, preferred specialty, and non-
preferred specialty. Each tier has a copay
• Come back to conversations or
follow up as often as you’d like
or coinsurance amount set by the plan.
Moda Health members can sign up for
To see medication tier coverage amounts, CirrusMD at modahealth.com/cirrusmd.
check the plan benefit tables in this Members can download the CirrusMD Metallic levels
brochure. You can visit modahealth.com/ app from the App Store or Google Play.
pdl and choose “Individual/Family” to � Gold plans typically have higher
search medications by plan and find out *For Individual members on Oregon Standard premiums, but they cover more,
your medication tiers and your costs. Plans, Moda Health Affinity Silver 3550 Off- too — about 80 percent of the
exchange only plan and HDHPs your cost is total average cost of care.
Pediatric vision and dental care the same as for a PCP office visit copay.
� Silver plans sit somewhere
Vision care is limited to members under age 19. in the middle, covering
Embedded pediatric vision coverage comes around 70 percent of the
with all Moda Health individual plans in Oregon. total average cost of care.
In plans that offer it, embedded pediatric � Bronze plans provide a little
dental care is limited to members under age 19. less coverage — about 60
percent of the total average
cost of care — but have
lower monthly premiums.
6 7
Medical networks
Life's better in
the network
Health happens, whether at home or on the road. We want to Our pharmacy network
make sure you stay covered, no matter where you go. So we’ve Members get the best benefit by using the
made it easy for you to find in-network coverage. Navitus pharmacy network. Pharmacies in this
network are contracted to offer prescriptions
at agreed-upon prices. Filling a prescription
at an out-of-network pharmacy is covered,
All plans include the If you have children you want to cover who but may cost you more. We also offer mail-
live outside of Oregon but in the US, they
Affinity EPO Network may be eligible for out-of-area benefits
order pharmacy services through Postal
Prescription Services (PPS) and Costco.
The medical plans in this brochure provide you if they are full-time students age 18 to 26
access to providers in the Affinity EPO network. or if you have a qualified medical child
This network includes a group of licensed support order (QMCSO). Children who
Travel with peace of mind
medical professionals, clinics, pharmacies, qualify for this coverage may use the First While traveling outside of Oregon, members
labs and hospitals. These providers offer Health network for better benefits. can receive emergency or urgent care
quality care and services to our individual through the First Health Network. Traveling
In Oregon, all of your enrolled family members
members who live within the Affinity Network for the purpose of seeking care does not
must use the Affinity network to be covered.
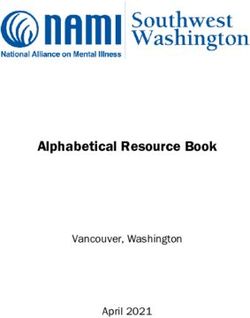
service area. When you shop for a plan, make qualify for the travel network benefit.
sure the Affinity EPO Network serves your area.
The map shows the network coverage area.
Affinity EPO Network Outside the United States, members may
access any provider for emergency care. This
The Affinity EPO network provides customized care is subject to balance billing. This means
There are no out-of-network benefits
care for members who want to manage that you may be responsible to pay in full any
with an EPO plan except as stated in the
their health in close partnership with a amount that your benefits do not cover. Other
member handbook. Your healthcare
PCP. The Affinity EPO network includes care received outside the U.S. is not covered.
provider and specialists must be in-
a community of primary care providers,
network for the plan you choose or you will The travel network is not available if
specialists and our partner health systems
be responsible for the full cost of out-of- you are temporarily residing outside
working together with Moda Health to
network services unless prohibited by law. of the primary service area unless you
provide quality care at affordable costs.
meet the eligibility and documentation
requirements for an out-of-area child.
Questions?
We’re here to help! Please see the
back cover for our individual sales
How to select an and services contact information.
Affinity PCP
As part of your enrollment,
an in-network PCP must be
selected for each applicant.
Be sure to check to see if your
current provider is included in
our Affinity EPO network.
To choose an in-network PCP,
go to modahealth.com/shop to
search for an Affinity EPO network
provider or confirm that your PCP
is in the Affinity EPO network. Once
you’ve selected your provider(s),
enter the name in the subscriber
and dependent sections of
8 the member application. 9
Picking a medical plan
How open
enrollment works
Open Enrollment dates are subject to change due to government regulations. Follow these simple steps to enroll
Please visit ModaHealth.com/shop/dates to see what the current enrollment
periods are. You can enroll in a plan or switch to a different plan during that
time. If you miss the Open Enrollment period and experience a life change,
you might qualify for Special Enrollment. For example, having a baby, getting
married or divorced, losing health coverage or moving to a new state may make
you and those you want to cover eligible. Visit the Learning Center at
ModaHealth.com/shop/dates to find out more about open and Special Enrollment. Confirm Find the Enroll at
your eligibility plan you like ShopModaPlans.com
You must currently reside Browse and compare Open Enrollment dates
in the service area, and our 2022 plans in are subject to change
Eligibility After you enroll live in the service area for this brochure or at due to government
Subscribers must currently live and have a Once you’re enrolled, use the ID number at least six months out of ShopModaPlans.com. regulations. Please
fixed, permanent home address in the service you’ll receive in your welcome letter to the year, to be eligible to The website also visit ModaHealth.com/
area to be eligible to enroll. You must live in log in to your Member Dashboard at enroll. Eligible members explains how health shop/dates to see what
the service area for at least six months of the modahealth.com. There, you can find in- include you, your legal plans, healthcare reform the current enrollment
year. Eligible members include you, your legal network providers, select or change your spouse or registered and federal financial periods are. Even if
spouse or registered domestic partner and PCP, access health resources and review your domestic partner and any assistance work — so you qualify for federal
any children up to age 26. Coverage is not Member Handbook to get familiar with your children up to age 26. For take a look! For free print financial assistance, visit
available to a person who lives in the service plan. When your first bill is ready, you can dependent students age copies of plan summaries us at ShopModaPlans.com
area to get health coverage or for another also manage billing and payment options 18-26 attending school of benefits and coverage to view our plans before
temporary reason such as getting treatment. through eBill using your Member Dashboard. or dependents with a (SBCs), please call us. you go to HealthCare.gov.
If you have children you want to cover who QMCSO living inside the You may also view our All plans are available
live outside of Oregon but in the US, they US but outside of OR, Member Handbooks through Moda Health
may be eligible for out-of-area benefits out-of-area services at modahealth.com. and most through
if they are full-time students age 18 to 26 are covered subject HealthCare.gov.
or if you have a qualified medical child to certain restrictions.
Coverage is not available If you make changes
support order (QMCSO). In Oregon, all of to your medical plan,
your enrolled family members must use to a person who resides
in the service area for you must reselect your
the Affinity network to be covered. dental plan or you will lose
the primary purpose of
There are no out-of-network obtaining health coverage your dental coverage.
benefits with an EPO plan except as or receiving treatment.
stated in the member handbook.
Individuals who are enrolled in Medicare
(Part A or Part B) or Medicare Advantage
cannot enroll in a Moda Health individual
medical plan, regardless of age. Learn
more about Medicare at cms.gov, or visit
modahealth.com/medicare to see our
Medicare options available in Oregon.
10 11
2022 Medical plan benefit table
Moda Health Oregon Standard Gold (Affinity) Moda Health Affinity Gold 250 Moda Health Affinity Gold 1000
In-network you pay Out-of-network you pay In-network you pay Out-of-network you pay In-network you pay Out-of-network you pay
Calendar year costs
Deductible per person $1,500 Not covered $250 Not covered $1,000 Not covered
Deductible per family $3,000 Not covered $500 Not covered $2,000 Not covered
Out-of-pocket max per person $7,300 Not covered $8,700 Not covered $8,700 Not covered
Out-of-pocket max per family $14,600 Not covered $17,400 Not covered $17,400 Not covered
Care & services
Preventive care visit $0/visit Not covered $0/visit Not covered $0/visit Not covered
Primary care provider (PCP) office visit $20/visit Not covered $20/visit Not covered $15/visit Not covered
Specialist office visit $40/visit Not covered $40/visit Not covered $30/visit Not covered
Urgent care visit $60/visit Not covered $40/visit Not covered $30/visit Not covered
Virtual care visit $20/visit Not covered $10/visit Not covered $10/visit Not covered
Outpatient diagnostic X-ray & lab 20% after deductible Not covered 25% after deductible Not covered 15% after deductible Not covered
Emergency room visit 20% after deductible 20% after deductible 25% after deductible 25% after deductible 15% after deductible 15% after deductible
Ambulance 20% after deductible 20% after deductible 25% after deductible 25% after deductible 15% after deductible 15% after deductible
Inpatient/outpatient Care 20% after deductible Not covered 25% after deductible Not covered 15% after deductible Not covered
Outpatient mental health/substance use disorder visit $20/visit Not covered $20/visit Not covered $15/visit Not covered
Physical, speech or occupational therapy visit $20/visit Not covered $40/visit Not covered $30/visit Not covered
Acupuncture and spinal manipulation services $20/visit Not covered $20/visit Not covered $15/visit Not covered
Prescription medications1
Value $10 $10 $2 $2 $2 $2
Select $10 $10 $10 $10 $10 $10
Preferred $30 $30 40% 40% 40% 40%
Non-Preferred 50% 50% 50% 50% 50% 50%
Preferred Specialty 50% Not covered 40% Not covered 40% Not covered
Non-Preferred Specialty 50% Not covered 50% Not covered 50% Not covered
Features
Metallic level � Gold � Gold � Gold
Exchange In and Out In and Out In and Out
Provider network Affinity Network Affinity Network Affinity Network
Travel network First Health Network First Health Network First Health Network
Service area Baker, Crook, Douglas, Gilliam, Grant, Baker, Crook, Douglas, Gilliam, Grant, Baker, Crook, Douglas, Gilliam, Grant,
Harney, Jefferson, Klamath, Lake, Lane, Harney, Jefferson, Klamath, Lake, Lane, Harney, Jefferson, Klamath, Lake, Lane, These benefits and Moda Health
Malheur, Marion, Morrow, Polk, Sherman, Malheur, Marion, Morrow, Polk, Sherman, Malheur, Marion, Morrow, Polk, Sherman, policies are subject to change in
order to be compliant with state
Umatilla, Union, Wallowa, Wheeler Umatilla, Union, Wallowa, Wheeler Umatilla, Union, Wallowa, Wheeler and federal guidelines. This
brochure provides summaries
Additional benefits (not covered out-of-network) Pediatric vision: Exam $0/visit; Hardware 0% Accident benefit: No cost share for Accident benefit: No cost share for of various health plans and
the first $1,000 within 90 days the first $1,000 within 90 days. is not a contract. If there is
Specialty pharmacy: $500 cost sharing any discrepancy between the
maximum per 30-day prescription fill Pediatric vision: Exam $20/visit; Pediatric vision: Exam $15/visit; summaries and the contract, it
is the contract that will control.
Hardware 25% after deductible Hardware 15% after deductible
1 Copay amounts are per
Pediatric dental: Preventive 0%; Pediatric dental: Preventive 0%; 30-day supply. $75 maximum
Other dental 25% after deductible Other dental 15% after deductible cost share per 30-day supply
for insulin.
12 132022 Medical plan benefit table
Moda Health Oregon Standard
Moda Health Affinity Silver 3500 Moda Health Affinity Silver 4500
Silver (Affinity)
In-network you pay Out-of-network you pay In-network you pay Out-of-network you pay In-network you pay Out-of-network you pay
Calendar year costs
Deductible per person $3,650 Not covered $3,500 Not covered $4,500 Not covered
Deductible per family $7,300 Not covered $7,000 Not covered $9,000 Not covered
Out-of-pocket max per person $8,550 Not covered $8,700 Not covered $8,700 Not covered
Out-of-pocket max per family $17,100 Not covered $17,400 Not covered $17,400 Not covered
Care & services
Preventive care visit $0/visit Not covered $0/visit Not covered $0/visit Not covered
Primary care provider (PCP) office visit $40/visit Not covered $35/visit Not covered $35/visit Not covered
Specialist office visit $80/visit Not covered $70/visit Not covered $70/visit Not covered
Urgent care visit $70/visit Not covered $70/visit Not covered $70/visit Not covered
Virtual care visit $40/ visit Not covered $10/visit Not covered $10/visit Not covered
Outpatient diagnostic X-ray & lab 30% after deductible Not covered 35% after deductible Not covered 35% after deductible Not covered
Emergency room visit 30% after deductible 30% after deductible 35% after deductible 35% after deductible 35% after deductible 35% after deductible
Ambulance 30% after deductible 30% after deductible 35% after deductible 35% after deductible 35% after deductible 35% after deductible
Inpatient/outpatient Care 30% after deductible Not covered 35% after deductible Not covered 35% after deductible Not covered
Outpatient mental health/
$40/visit Not covered $35/visit Not covered $35/visit Not covered
substance use disorder visit
Physical, speech or occupational therapy visit $40/visit Not covered $70/visit Not covered $70/visit Not covered
Acupuncture and spinal manipulation services $40/visit Not covered $35/visit Not covered $35/visit Not covered
Prescription medications1
Value $15 $15 $2 $2 $2 $2
Select $15 $15 $20 $20 $20 $20
Preferred $60 $60 40% 40% 40% 40%
Non-Preferred 50% 50% 50% after deductible 50% after deductible 50% after deductible 50% after deductible
Preferred Specialty 50% Not covered 40% Not covered 40% Not covered
Non-Preferred Specialty 50% Not covered 50% after deductible Not covered 50% after deductible Not covered
Features
Metallic level � Silver � Silver � Silver
Exchange In and Out In and Out In and Out
Provider network Affinity Network Affinity Network Affinity Network
Travel network First Health Network First Health Network First Health Network
Baker, Crook, Douglas, Gilliam, Grant, Harney, Jefferson, Baker, Crook, Douglas, Gilliam, Grant, Harney, Jefferson,
Baker, Crook, Douglas, Gilliam, Grant, Harney, Jefferson, Klamath, Lane, Lake,
Service area Klamath, Lane, Lake, Malheur, Marion, Morrow, Polk, Klamath, Lane, Lake, Malheur, Marion, Morrow, Polk,
Malheur, Marion, Morrow, Polk, Sherman, Umatilla, Union, Wallowa, Wheeler
Sherman, Umatilla, Union, Wallowa, Wheeler Sherman, Umatilla, Union, Wallowa, Wheeler
Additional benefits (not covered out-of-network) Pediatric vision: Exam $0/visit; Hardware 0% Pediatric vision: Exam $35/visit; Hardware 35% after deductible Pediatric vision: Exam $35/visit; Hardware 35% after deductible
These benefits and Moda Health policies are subject to change in order to be compliant
with state and federal guidelines. This brochure provides summaries of various health
plans and is not a contract. If there is any discrepancy between the summaries and the
contract, it is the contract that will control.
1 C
opay amounts are per 30-day supply. $75 maximum cost share per 30-day
supply for insulin.
14 152022 Medical plan benefit table
Moda Health Affinity Silver 3400 Off-exchange only Moda Health Affinity Silver 3550 Off-exchange only Moda Health Affinity Silver 4400 Off-exchange only
In-network you pay Out-of-network you pay In-network you pay Out-of-network you pay In-network you pay Out-of-network you pay
Calendar year costs
Deductible per person $3,400 Not covered $3,550 Not covered $4,400 Not covered
Deductible per family $6,800 Not covered $7,100 Not covered $8,800 Not covered
Out-of-pocket max per person $8,700 Not covered $8,550 Not covered $8,700 Not covered
Out-of-pocket max per family $17,400 Not covered $17,100 Not covered $17,400 Not covered
Care & services
Preventive care visit $0/visit Not covered $0/visit Not covered $0/visit Not covered
Primary care provider (PCP) office visit $35/visit Not covered $40/visit Not covered $35/visit Not covered
Specialist office visit $70/visit Not covered $80/visit Not covered $70/visit Not covered
Urgent care visit $70/visit Not covered $80/visit Not covered $70/visit Not covered
Virtual care visit $10/visit Not covered $40/visit Not covered $10/visit Not covered
Outpatient diagnostic X-ray & lab 35% after deductible Not covered 30% after deductible Not covered 35% after deductible Not covered
Emergency room visit 35% after deductible 35% after deductible 30% after deductible 30% after deductible 35% after deductible 35% after deductible
Ambulance 35% after deductible 35% after deductible 30% after deductible 30% after deductible 35% after deductible 35% after deductible
Inpatient/outpatient Care 35% after deductible Not covered 30% after deductible Not covered 35% after deductible Not covered
Outpatient mental health/
$35/visit Not covered $40/visit Not covered $35/visit Not covered
substance use disorder visit
Physical, speech or occupational therapy visit $70/visit Not covered $40/visit Not covered $70/visit Not covered
Acupuncture and spinal manipulation services $35/visit Not covered $40/visit Not covered $35/visit Not covered
Prescription medications1
Value $2 $2 $15 $15 $2 $2
Select $20 $20 $15 $15 $20 $20
Preferred 40% 40% $60 $60 40% 40%
Non-Preferred 50% after deductible 50% after deductible 50% 50% 50% after deductible 50% after deductible
Preferred Specialty 40% Not covered 50% Not covered 40% Not covered
Non-Preferred Specialty 50% after deductible Not covered 50% Not covered 50% after deductible Not covered
Features
Metallic level � Silver � Silver � Silver
Exchange Out Out Out
Provider network Affinity Network Affinity Network Affinity Network
Travel network First Health Network First Health Network First Health Network
Baker, Crook, Douglas, Gilliam, Grant, Harney, Jefferson, Baker, Crook, Douglas, Gilliam, Grant, Harney, Jefferson,
Baker, Crook, Douglas, Gilliam, Grant, Harney, Jefferson, Klamath, Lane, Lake,
Service area Klamath, Lane, Lake, Malheur, Marion, Morrow, Polk, Klamath, Lane, Lake, Malheur, Marion, Morrow, Polk,
Malheur, Marion, Morrow, Polk, Sherman, Umatilla, Union, Wallowa, Wheeler
Sherman, Umatilla, Union, Wallowa, Wheeler Sherman, Umatilla, Union, Wallowa, Wheeler
Additional benefits (not covered out-of-network) Pediatric vision: Exam $35/visit; Hardware 35% after deductible Pediatric vision: Exam $0/visit; Hardware 0% Pediatric vision: Exam $35/visit; Hardware 35% after deductible
These benefits and Moda Health policies are subject to change in order to be compliant
with state and federal guidelines. This brochure provides summaries of various health
plans and is not a contract. If there is any discrepancy between the summaries and the
contract, it is the contract that will control.
1 C
opay amounts are per 30-day supply. $75 maximum cost share per 30-day
supply for insulin.
16 17Moda Health Affinity Standard Bronze Moda Health Affinity Bronze 7000 Moda Health Affinity Bronze 8700
In-network you pay Out-of-network you pay In-network you pay Out-of-network you pay In-network you pay Out-of-network you pay
Calendar year costs
Deductible per person $8,700 Not covered $7,000 Not covered $8,700 Not covered
Deductible per family $17,400 Not covered $14,000 Not covered $17,400 Not covered
Out-of-pocket max per person $8,700 Not covered $8,700 Not covered $8,700 Not covered
Out-of-pocket max per family $17,400 Not covered $17,400 Not covered $17,400 Not covered
Care & services
Preventive care visit $0/visit Not covered $0/visit Not covered $0/visit Not covered
Primary care provider (PCP) office visit $50/visit Not covered $85/visit Not covered $85/visit Not covered
Specialist office visit $100/visit Not covered $120/visit Not covered $120/visit Not covered
Urgent care visit $100/visit Not covered $120/visit Not covered $120/visit Not covered
Virtual care visit $50/visit Not covered $10/visit Not covered $10/visit Not covered
Outpatient diagnostic X-ray & lab 0% after deductible Not covered 40% after deductible Not covered 0% after deductible Not covered
Emergency room visit 0% after deductible 0% after deductible 40% after deductible 40% after deductible 0% after deductible 0% after deductible
Ambulance 0% after deductible 0% after deductible 40% after deductible 40% after deductible 0% after deductible 0% after deductible
Inpatient/outpatient Care 0% after deductible Not covered 40% after deductible Not covered 0% after deductible Not covered
Outpatient mental health/
$50/visit Not covered $85/visit Not covered $85/visit Not covered
substance use disorder visit
Physical, speech or occupational therapy visit $50/visit Not covered $120/visit Not covered $120/visit Not covered
Acupuncture and spinal manipulation services $50/visit Not covered $85/visit Not covered $85/visit Not covered
Prescription medications1
Value $20 $20 $2 $2 $2 $2
Select $20 $20 40% 40% $25 $25
Preferred 0% after deductible 0% after deductible 40% after deductible 40% after deductible 0% after deductible 0% after deductible
Non-Preferred 0% after deductible 0% after deductible 50% after deductible 50% after deductible 0% after deductible 0% after deductible
Preferred Specialty 0% after deductible Not covered 40% after deductible Not covered 0% after deductible Not covered
Non-Preferred Specialty 0% after deductible Not covered 50% after deductible Not covered 0% after deductible Not covered
Features
Metallic level � Bronze � Bronze � Bronze
Exchange In and Out In and Out In and Out
Provider network Affinity Network Affinity Network Affinity Network
Travel network First Health Network First Health Network First Health Network
Baker, Crook, Douglas, Gilliam, Grant, Harney, Jefferson, Baker, Crook, Douglas, Gilliam, Grant, Harney, Jefferson,
Baker, Crook, Douglas, Gilliam, Grant, Harney, Jefferson, Klamath, Lane, Lake,
Service area Klamath, Lane, Lake, Malheur, Marion, Morrow, Polk, Klamath, Lane, Lake, Malheur, Marion, Morrow, Polk,
Malheur, Marion, Morrow, Polk, Sherman, Umatilla, Union, Wallowa, Wheeler
Sherman, Umatilla, Union, Wallowa, Wheeler Sherman, Umatilla, Union, Wallowa, Wheeler
Additional benefits (not covered out-of-network) Pediatric vision: Exam $0/visit; Hardware 0% Pediatric vision: Exam $85/visit; Hardware 40% after deductible Pediatric vision: Exam $85/visit; Hardware 0% after deductible
These benefits and Moda Health policies are subject to change in order to be compliant
with state and federal guidelines. This brochure provides summaries of various health
plans and is not a contract. If there is any discrepancy between the summaries and the
contract, it is the contract that will control.
1 C
opay amounts are per 30-day supply. $75 maximum cost share per 30-day
supply for insulin.
18 19High-deductible health plan (HDHP)
Moda Health Affinity Bronze HSA 6900
Tax advantages
In-network you pay Out-of-network you pay
Calendar year costs
Deductible per person $6,900 Not covered
with an HDHP Deductible per family
Out-of-pocket max per person
Out-of-pocket max per family
$13,800
$6,900
$13,800
Not covered
Not covered
Not covered
Care & services
Our health savings account (HSA)-compatible, high-deductible EPO health plans Preventive care visit $0/visit Not covered
(HDHP) give you flexibility and choice. You have the freedom to choose any financial Primary care provider (PCP) office visit 0% after deductible Not covered
institution for your HSA. You can use HSA tax-free dollars to pay for deductibles, Specialist office visit 0% after deductible Not covered
coinsurance and other qualified expenses not covered by your health plan. Urgent care visit 0% after deductible Not covered
Virtual care visit 0% after deductible Not covered
Outpatient diagnostic X-ray & lab 0% after deductible Not covered
Calendar year costs Eligibility
Emergency room visit 0% after deductible 0% after deductible
Deductible Anyone can enroll in a Moda Health
HDHP, even if you do not have an HSA. Ambulance 0% after deductible 0% after deductible
If you have subscriber-only coverage, you
must meet the per-person deductible. If To be eligible to participate Inpatient/outpatient Care 0% after deductible Not covered
your plan covers more than one person, in an HSA, you must: Outpatient mental health/
0% after deductible Not covered
you must meet the per person deductible • Use a financial institution that has an HSA substance use disorder visit
only until the total family deductible is option. You have the option to open an Physical, speech or occupational therapy visit 0% after deductible Not covered
satisfied before benefits are payable. HSA through our partner organization, Acupuncture and spinal manipulation services 0% after deductible Not covered
BenefitHelp Solutions. To learn more, call
Out-of-pocket maximum BenefitHelp Solutions at 503-412-4210. Prescription medications1
After you meet the per-person or per- • Be covered by a Moda Health HDHP Value $2 $2
family out-of-pocket maximum, the plan plan. Please see the Moda Health Affinity
pays 100 percent of covered care for the Bronze HSA 6900 plan on page 19. Select 0% after deductible 0% after deductible
remainder of the year. If your plan covers • Not be covered under another non- Preferred 0% after deductible 0% after deductible
more than one person, the per-person HSA-compatible medical plan
maximum applies only until the total family (including your spouse’s plan) Non-Preferred 0% after deductible 0% after deductible
out-of-pocket maximum is reached.
• Not be enrolled in Medicare Preferred Specialty 0% after deductible Not covered
• Not be claimed as a dependent Non-Preferred Specialty 0% after deductible Not covered
on someone else’s tax return
Features
Metallic level � Bronze
Exchange In and Out
These benefits and
Provider network Affinity Network Moda Health policies
are subject to change
Travel network First Health Network in order to be compliant
with state and federal
Baker, Crook, Douglas, Gilliam, Grant, guidelines. This
brochure provides
Harney, Jefferson, Klamath, Lake, Lane, summaries of various
Service area health plans and is
Malheur, Marion, Morrow, Polk, Sherman,
not a contract. If there
Umatilla, Union, Wallowa, Wheeler is any discrepancy
between the summaries
Additional benefits Pediatric vision: 0% after deductible and the contract, it is
(not covered out-of-network) the contract that will
control.
1 Copay amounts are
per 30-day supply.
For all tiers - $75
maximum cost share
per 30-day supply
for insulin..
20 21Plan premiums
Limitations and exclusions for medical plans
These are some common limitations and exclusions for our Moda Health individual and
family medical plans. For a full list of limitations and exclusions per plan or for copies of
plan summaries of benefits and coverage (SBCs), please call us at 855-718-1767.
Understand what
Limitations
− Acupuncture is limited to 12 visits per year
− Transplants must be performed at the authorized
transplant facility to be eligible for coverage
you will pay each month
− Authorization by Moda Health is required for − Vision exam and glasses or contacts covered
all medical and surgical admissions and some once per year for members under age 19
outpatient services and medications
− Biofeedback limited to 10 visits per Exclusions As your healthcare partner and your guide to accessing quality care, we’re
lifetime, for tension or migraine − Care outside the United States, here to help you understand the amount you pay each month for coverage.
headaches or urinary incontinence other than emergency care
− Coordination of benefits — when a member − Charges above the maximum plan allowance
has more than one health plan, combined − Cosmetic services and supplies (exception
benefits for all plans is limited to the maximum for reconstructive surgery if medically What affects your premium? How your premium could change
plan allowance for all covered services necessary and not specifically excluded)
− Court-ordered sex offender treatment The plan, your age and the ages of your 2022 premiums are effective Jan. 1, 2022,
− Dental - Pediatric only. Subject to frequency
and age limits when covered − Custodial care dependents affect your premium amount. If through Dec. 31, 2022. Your premium could
− Hearing aids limited to once every 3 years. − Dental examinations and treatment you have more than three dependents under change during the plan year if you add a family
Hearing tests limited to twice per year under except for accidental injury, and age 21 on the plan, you will only be charged a member through a special enrollment. If that
age 4 and once per year age 4 and older. pediatric coverage on some plans premium for the first three. Child dependents happens, in most cases the new premium is
− Hospice respite care limited to 30 days − Experimental or investigational treatment ages 21 through 25 will each have a premium effective the first of the month following the
lifetime maximum, up to five days in a row − Infertility (services or supplies for treatment based on their age. For medical plans, your special enrollment event. Your premium may
− Infusion therapy — Some medications require of, including reversal of sterilization) rating area, or where you live, also matters. also change if you remove a family member.
use of an authorized provider and/or supplier − Injury resulting from practicing for or If you qualify for federal financial assistance, Having a birthday during a plan year won’t
to be eligible for coverage. Outpatient hospital participating in professional athletic events it may cover some of your premium. To find affect your current premium. When you
setting is not covered for some medications. − Instruction programs, except as provided under out what you’d pay with this assistance, renew your plan in January, your premium will
− Medicare — Any expense that is actually paid the outpatient diabetic instruction benefit visit the Marketplace at HealthCare.gov. reflect the current plan amount for your age.
under Medicare, or would have been paid − Massage or massage therapy
under Medicare Part B if you had enrolled in
− Naturopathic supplies, including herbal, If you learn that you are not eligible for Yearly premium updates
Medicare, will have benefits reduced by the
naturopathic or homeopathic medicines, subsidies on the exchange, you may want to
amount Medicare paid or would have paid. consider some of our new off-exchange only We adjust premiums for individual and
substances or devices and any other
− Prescriptions — If you use a brand medication when nonprescription supplements Silver plans, which are more affordable. family plans each year. You’ll receive
a generic equivalent is available, you will have to pay
− Obesity (all services and supplies except those a renewal notice 90 days prior to the
the nonpreferred cost sharing plus the difference
required under the Affordable Care Act) new plan effective date explaining any
in cost between the generic and brand medication. changes to your plan and premium.
Prescriptions are limited to a 30-day supply for retail − Optional services or supplies, including those for
and most specialty pharmacy and 90 days for mail comfort, convenience, environmental control or
order and participating retail pharmacies. Some education, and treatment not medically necessary
medications that are often used to treat complex − Orthognathic surgery except when
chronic health conditions must be dispensed medically necessary to repair an accidental
through an exclusive specialty pharmacy provider. injury or for treatment of cancer
− Preventive care - Cost sharing may apply to services − Out-of-network providers, except
not required under the Affordable Care Act for medical emergency care
− Rehabilitation and habilitation benefits limited to − Services or supplies available under any city,
30 inpatient days and 30 outpatient sessions per county, state or federal law, except Medicaid
calendar year. May be eligible for up to 60 days − Services you provide to yourself
rehabilitation after acute head or spinal cord − Services provided by a member of your immediate
injury (except for Standard Metal plans and Moda family other than services by a dental provider
Health Affinity Silver 3550 Off-exchange plan) or − Temporomandibular Joint Syndrome (TMJ)
60 outpatient rehabilitation sessions for treatment − Vision surgery to change the
of neurologic conditions. Limits apply separately refractive character of the eye
to rehabilitative and habilitative services.
− Skilled nursing facility limited to 60 days per year
− Spinal manipulation is limited to 20 visits per year
To view plans
and premiums, visit
modahealth.com/shop
22 23Dental plans
Quality coverage
for your smile
Healthy teeth are happy teeth. With our individual and family Delta Dental Dental coverage options Delta Dental network
Plan of Oregon plans, you’ll have access to quality in-network dentists. We offer three types of dental plans. goes where you go
Choose the one that is right for you. Each Delta Dental Plan of Oregon plan
comes with a Delta Dental network. It
Delta Dental PPO SM
plan
Dental benefit highlights Tools for better oral health includes thousands of dentists with
This plan offers a broad range of both statewide and national access.
Our Delta Dental Plan of Oregon plans connect To get started, visit DeltaDentalOR.com and services and providers. You receive in
you with great benefits. You can count on: log in to your Member Dashboard account. If In-network dentists agree to accept our
network benefits when seeing a Delta Dental
contracted fees as full payment. This means
• No waiting periods for Class 1 services you don't have a Member Dashboard, you can PPO Network dentist. For out-of-network
they don’t balance bill — the difference
create one. Look for Dental tools. Dental tools
• Savings with in-network dentists help you manage your dental health, such as:
benefits, you can save money by seeing
providers in the Delta Dental Premier ®
between the allowed amount and the dentist’s
• Cleanings every six months • Scheduling for virtual checkups Network. In both cases, providers accept
billed charge. This can help you save on out-
• Predetermination of benefits if • Scheduling for emergency virtual consults the Delta Dental contracted fee, so there will
of-pocket costs. If you see providers outside
the network, you may pay more for care.
requested in a pretreatment plan be no additional balance billing charge.
• Fast and accurate claims payment • Viewing your benefits dashboard Delta Dental PPO Network
• Superior customer service • Using a cost calculator Delta Dental EPO plan
This is one of the largest preferred provider
And much more. This plan gives you a higher level of benefits
Our dental plans also include useful organization (PPO) dental networks in
than the PPO plan, but you must see Delta
online tools, resources and special Oregon and across the country. It includes
Dental PPO-contracted providers to receive
programs if you need a little extra more than 1,300 participating providers in
a benefit. This exclusive provider option
attention for your pearly whites. Oregon and offers access to over 113,000
does not pay for services provided by a
Delta Dental PPO dentists nationwide.
Premier or non-contracted dentist. Care
from providers outside this network is not Is my dentist in the network?
covered, except for emergency services.
Visit DeltaDentalOR.com to see if your
Delta Dental PPO Bright Smiles plan dentist is in our network or search for a
dentist. Choose a dental network and look
This PPO plan is available for all individual
for participating dentists in your area.
members, but benefits only cover children
under age 19. You receive in-network
benefits when seeing a Delta Dental PPO
Network dentist. For out-of-network benefits,
you can save money by seeing providers
in the Delta Dental Premier Network. In
both cases, providers accept the Delta
Dental contracted fee, so there will be
no additional balance billing charge.
Enroll in a dental plan
To enroll in a dental plan, please
see “How open enrollment
works” on page 10.
24 252022 Dental plan benefit table
Delta Dental PPOSM Delta Dental EPO Delta Dental PPO Bright Smiles
Ages 0 – 18 Ages 19+ Ages 0 – 18 Ages 19+ Ages 0 – 18 Ages 19+
In-network Out-of-network Out-of-network In-network Out-of-network Out-of-network In-network Out-of-network Out-of-network Out-of
In-network, Out-of-network, In-network, Out-of-network, In-network,
PPO dentist, Premier dentist, nonparticipating PPO dentist, Premier dentist, nonparticipating PPO dentist, Premier dentist, nonparticipating network,
you pay you pay you pay you pay you pay
you pay you pay dentist, you pay you pay you pay dentist, you pay you pay you pay dentist, you pay you pay
Calendar year costs
Deductible per person $0 $0 $0
Out-of-pocket max per $375 for one member / $750 for two or more members $375 for one member / $750 for two or more members $375 for one member / $750 for two or more members
person (ages 0 – 18) (in-network only) (in-network only) (in-network only)
Annual benefit max (age 19+) $1,000 $1,500 N/A
Class 1
Exams and X-rays 0% 40% 40% 25% 50% 50% 0% Not covered 0% Not covered 0% 40% 40% Not covered
Cleanings 0% 40% 40% 25% 50% 50% 0% Not covered 0% Not covered 0% 40% 40% Not covered
Periodontal maintenance 0% 40% 40% 25% 50% 50% 0% Not covered 0% Not covered 0% 40% 40% Not covered
Sealants 0% 40% 40% 25% 50% 50% 0% Not covered 0% Not covered 0% 40% 40% Not covered
Topical fluoride 0% 40% 40% 25%1 50%1 50%1 0% Not covered 0%1 Not covered 0% 40% 40% Not covered
Class 2
Space maintainers 75% 75% 75% Not covered Not covered Not covered 30% Not covered Not covered Not covered 75% 75% 75% Not covered
Restorative fillings2 75% 75% 75% 40% 50% 50% 30% Not covered 30% Not covered 75% 75% 75% Not covered
Class 3
Oral surgery3 75% 75% 75% 50% 50% 50% 50% Not covered 50% Not covered 75% 75% 75% Not covered
Endodontics3 75% 75% 75% 50% 50% 50% 50% Not covered 50% Not covered 75% 75% 75% Not covered
Periodontics3 75% 75% 75% 50% 50% 50% 50% Not covered 50% Not covered 75% 75% 75% Not covered
Restorative crowns3 75% 75% 75% 50% 50% 50% 50% Not covered 50% Not covered 75% 75% 75% Not covered
Bridges3 Not covered Not covered Not covered 50% 50% 50% Not covered Not covered 50% Not covered Not covered Not covered Not covered Not covered
Partial and complete dentures3 75% 75% 75% 50% 50% 50% 50% Not covered 50% Not covered 75% 75% 75% Not covered
Anesthesia3 75% 75% 75% 50% 50% 50% 50% Not covered 50% Not covered 75% 75% 75% Not covered
Orthodontia4 75% 75% 75% Not covered Not covered Not covered 50% Not covered Not covered Not covered 75% 75% 75% Not covered
Features
Delta Dental Delta Dental All other Delta Dental Delta Dental All other Delta Dental All other Delta Dental All other Delta Dental Delta Dental All other
Provider network N/A
PPO Network Premier Network providers PPO Network Premier Network providers PPO Network providers PPO Network providers PPO Network Premier Network providers
Delta Dental Delta Dental Delta Dental Delta Dental Delta Dental Delta Dental
Delta Dental PPO Nonparticipating: Delta Dental PPO Nonparticipating: Nonparticipating:
Balance bill Premier Premier PPO Yes PPO Yes PPO Premier N/A
Network: No Yes Network: No Yes Yes
Network: No Network: No Network: No Network: No Network: No Network: No
1 Covered once in a 12-month period if there is recent history of periodontal 3 12-month exclusion period for ages 19 and over if member does not have 12 These benefits and Delta Dental Plan of Oregon policies are subject to change in order to be compliant with state and federal guidelines. This brochure provides
surgery or high-risk of decay because of medical disease or chemotherapy continuous months of prior dental coverage with no more than a 90-day summaries of various health plans and is not a contract. If there is any discrepancy between the summaries and the contract, it is the contract that will control.
or similar type of treatment. break in coverage from the end of the old policy to the effective date of the
2 Six-month exclusion period for ages 19 and over if member does not have 2022 Delta Dental policy.
12 continuous months of prior dental coverage with no more than a 90-day 4 Only medically necessary orthodontia to treat cleft palate is covered.
break in coverage from the end of the old policy to the effective date of the
2022 Delta Dental policy.
26 27Limitations and exclusions for dental plans
These are some common limitations and exclusions for our Delta Dental Plan of Oregon individual
and family dental plans. For a full list of limitations and exclusions per plan or for copies of plan Dental plan premiums for Oregon
summaries, please see back cover for our sales and service team contact information.
These premiums apply to members who live anywhere in Oregon.
Limitations Exclusions
Class 1 − Anesthetics, analgesics, hypnosis and most Age 2022 Delta Dental PPO 2022 Delta Dental EPO 2022 Delta Dental
− Bitewing X-rays once in a 12-month period medications, including nitrous oxide for adults Bright Smiles
− Exam once in a six-month period − Charges above the maximum plan allowance 0-18 $37 $41 $37
− Fluoride once in a six-month period under age − Charting (including periodontal, gnathologic)
19 and once every 12 months if there is recent − Congenital or developmental malformations 19-24 $27 $29
history of periodontal surgery or high risk of − Cosmetic services
decay due to medical disease or chemotherapy − Duplication and interpretation of X-rays or records 25-29 $27 $29
or similar type of treatment for age 19+ − Experimental or investigational treatment 30-34 $29 $31
− Full-mouth or panoramic X-rays − Hospital costs or other fees for facility
once in a five-year period or home care except for emergency 35-39 $32 $34
− Interim caries arresting medicament application care for members under age 19
is covered twice per tooth per year. Many − Implants 40-44 $33 $35
restorations are not covered within 3 months of
interim caries arresting medicament application.
− Instructions or training (including plaque control 45-49 $34 $36
and oral hygiene or dietary instruction)
− Prophylaxis (cleaning) or periodontal maintenance − Orthodontia (exception for treatment 50-54 $37 $39
is covered once in any six-month period. Additional
of cleft palate under age 19)
periodontal maintenance is covered for members 55-59 $40 $43
with periodontal disease, up to a total of 2 − Over-the-counter night guards
additional periodontal maintenances per year. and athletic mouth guards
60-63 $44 $47
− Sealants limited to unrestored occlusal surface − Rebuilding or maintaining chewing surfaces
of permanent molars once per tooth in a five-year (misalignment or malocclusion) or stabilizing teeth 64+ $47 $50
period except for evidence of clinical failure − Self treatment
Class 2 and Class 3 − Services or supplies available under any city,
− Athletic mouth guard covered once in any 12-month county, state or federal law, except Medicaid
period for members age 15 and under and once − Translation or sign language services are
in any 24-month period age 16 and over not covered as separate charges
− Bridges once in a seven-year period age 19 and over − Temporomandibular joint syndrome (TMJ)
− Crowns and other cast restorations − Treatment not dentally necessary
once in a seven-year period − Treatment before coverage begins
− Crown over implant once per lifetime per tooth. or after coverage ends
− Dentures once in a seven-year period age 16 and over
− IV sedation or general anesthesia only with surgical
procedures. Oral anesthesia only for members
under age 19 used during an in-office procedure.
− Night guard (occlusal guard) covered at 100 percent
once in a five year period, up to $150 maximum.
Repair and reline of occlusal guard are covered
once every 12-month period. One occlusal guard
adjustment is covered every 12-month period.
− Periodontal surgical procedures by the same
dentist at the same site are covered once in
a 3 year period for members 19 and over.
− Porcelain crowns on back teeth are limited
to the amount for a full metal crown.
− Scaling and root planing is limited to once
per quadrant in any 2-year period
Premiums effective Jan. 1, 2022, through Dec. 31, 2022
28 29Member care resources
Tools and
programs for
your health
Momentum
Health coaching
Take charge of your health — and follow your
progress. It’s easy with Momentum, powered Need a hand with your health? Our
journey
by Moda Health. Log in to your Member health coaches use evidence-based
Dashboard and look for Momentum to: practices to help you set goals and feel
your best. Our care programs include:
• Take a health assessment and
see your “health age” • Cardiac Care
• Set goals and track progress • Depression Care
Moda Health and Delta Dental Plan of • Find health content and resources • Diabetes Care
Oregon are here to help you feel better • Access fun healthy recipes • Kidney Care
and live longer. We even have special • Lifestyle Coaching
programs and care teams to support • Women’s Health & Maternity Care
you in reaching your health goals. • Respiratory Care
• Spine & Joint Care
• Weight care
Get started with your
Member Dashboard
Your Member Dashboard is a personalized
Active&Fit Direct™
member website that gives you access
to health tools and resources to help Discounted gym membership
you manage your health and benefits. Stay active in the gym or at home.
As a member, just log in to your Member With the Active&Fit Direct™
Dashboard at modahealth.com to: program, you have access to:
• Find in-network providers • 16,000+ Standard and Premium fitness
• Select or change your PCP centers and exercise studios nationwide
• See your benefits and Member Handbook • The ability to purchase a membership Prescription price check
for your spouse (or domestic partner)
• Check claims and find claim forms See prescription medication costs and
• Review electronic explanations • The option to switch fitness centers how much you would pay by medication
to make sure you find the right fit tier at an in-network pharmacy.
of benefits (EOBs)
• Look up medication prices • 4,000+ digital workout videos so you This tool makes it easy to find medication
can work out at home or on-the-go
• Download your member ID card cost estimates and generic options.
• Access tools to get and stay healthy
and manage your dental care needs
Tools for better health
These handy resources come with every
individual and family plan. Use them to
create a healthier you! Simply log in to
your Member Dashboard to get started.
30 31You can also read