Exogenous Ochronosis (EO): Skin lightening cream causing rare caviar-like lesion with banana-like pigments; review of literature and histological ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Clinical Case Report and Review
Exogenous Ochronosis (EO): Skin lightening cream causing rare
caviar-like lesion with banana-like pigments; review of literature and
histological comparison with endogenous counterpart
Amir Qorbani1 , Adnan Mubasher2 , George Peter Sarantopoulos3 ,
Scott Nelson3 , Maxwell Alexander Fung4
How to cite: Qorbani A, Mubasher A, Sarantopoulos GP, Nelson S, Fung MA. Exogenous Ochronosis (EO): Skin lightening
cream causing rare caviar-like lesion with banana-like pigments; review of literature and histological comparison with
endogenous counterpart. Autops Case Rep [Internet]. 2020 Oct-Dec;10(4):e2020197. https://doi.org/10.4322/acr.2020.197
ABSTRACT
Ochronosis is a cutaneous disorder caused by the accumulation of phenols, either endogenously as homogentisic acid
in patients with alkaptonuria (autosomal recessive disorder with deficiency of the enzyme homogentisic acid oxidase),
or exogenously in patients using phenol products such as topical creams containing hydroquinone or the intramuscular
application of antimalarial drugs. Exogenous ochronosis (EO) typically affects the face and was reported in patients with
dark skin such as Black South Africans or Hispanics who use skin-lightening products containing hydroquinone for extended
periods. Recently more cases have been reported worldwide even in patients with lighter skin tones, to include Eastern
Indians, Asians, and Europeans. However, just 39 cases of EO have been reported in the US literature from 1983 to 2020.
Here we present two cases; a 69 and a 45-year-old female who were seen for melasma, given hydroquinone 4% cream
daily and tretinoin 0.05%. Both patients noticed brown spots on their cheeks, which progressively enlarged and darkened
in color. The diagnosis of ochronosis was confirmed by characteristic histopathological features on the punch biopsy.
Unfortunately, neither patient responded to multiple treatments (to include, tazarotene 0.1% gel and pimecrolimus
ointment, topical corticosteroids, and avoidance of hydroquinone containing products). We also present a case of classic
(endogenous) ochronosis in a patient with alkaptonuria to picture the histological similarities of these two entities. EO is
an important clinical consideration because early diagnosis and treatment may offer the best outcome for this notoriously
refractory clinical diagnosis.
Keywords
Ochronosis, Ochronosis, Skin Care, Skin Cream, Skin Diseases, Skin Pigmentation
INTRODUCTION
Ochronosis an uncommon condition characterized containing phenols. It was initially described in
by the accumulation of phenols, either endogenously 1865 by Rudolf Virchow, based on the deposition of
as homogentisic acid in patients with alkaptonuria microscopic light brownish-yellow (ochre) pigments in
or exogenously in patients using topical products a patient with endogenous ochronosis.1,2 Endogenous
1
University of California, San Francisco (UCSF), Department of Pathology and Laboratory Medicine, San Francisco, CA, USA
2
Icahn School of Medicine at Mount Sinai Beth Israel, Department of Diagnostic Pathology & Laboratory Medicine, New York, NY, USA
3
University of California, Los Angeles (UCLA), Department of Pathology and Laboratory Medicine, Los Angeles, CA, USA
4
University of California, Davis (UC Davis), Department of Pathology and Laboratory Medicine, Sacramento, CA, USA
Copyright: © 2020 The Authors. This is an Open Access article distributed under the terms of the Creative
Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium,
provided the original work is properly cited.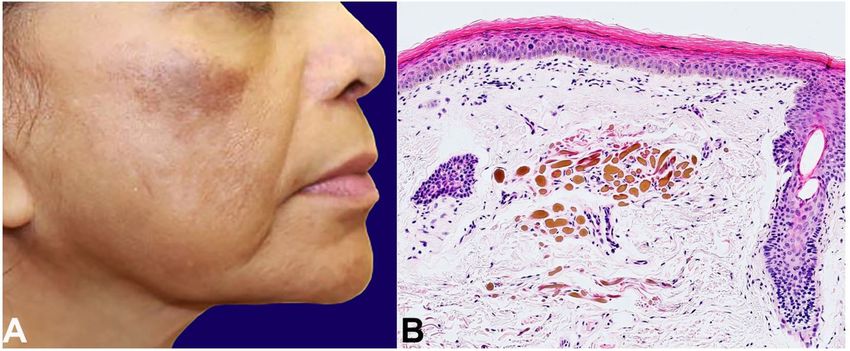
Exogenous Ochronosis (EO): Skin lightening cream causing rare caviar-like lesion with banana-like pigments; review of literature and histological
comparison with endogenous counterpart
ochronosis occurs as a manifestation of alkaptonuria, After a year, she noticed a red, scaly patch on her left
a rare autosomal recessive condition resulting in loss cheek that progressively grew and darkened in color.
of homogentisic acid oxidase. Homogentisic acid The patches became gray-black, itchy, and tender
oxidase is involved in the metabolism of tyrosine (Figure 1A). Due to the history of long-term use of
and phenylalanine, and its absence leads to the hydroquinone, and the asymmetrical presentation of
accumulation of homogentisic acid (HGA) in the the facial lesion, the clinical diagnosis of exogenous
body, which causes the dark blue discoloration of ochronosis was favored. Histological examination
cartilaginous tissue such as ear cartilage or articular showed yellow-brown sharply defined irregularly
surfaces. According to Laymon,2 exogenous ochronosis shaped pigment granules in the upper dermis,
(EO) was first coined in 1906 by L. Pick, which is diagnostic of exogenous ochronosis (Figure 1B).
characterized by a bluish-gray patches with a coarse She discontinued the hydroquinone and tretinoin,
texture and “caviar-like” papules. EO typically affects and started desonide 0.5% lotion with sun protection.
face and neck and mainly seen in patients with dark After a month, lesional inflammation was decreased,
skin. It was reported in Black South Africans 3 or but the hyperpigmentation and a mild thickening
Hispanics,4 who used certain skin-lightening products persisted. She continued hydrocortisone cream and
containing phenol substances for a long time.5 Many sun protection creams with minimal improvement in
drugs have been implicated in its etiology, including her symptoms.
benzene, quinone, antimalarials drugs, and mercury Case #2: A 68-year-old female presented with
derivatives. EO is more common in dark-skin individuals clinically diagnosed chronic melasma characterized by
due to the application of skin lightening/bleaching dark brown hyperpigmented macules coalescing into
products containing hydroquinone. To our knowledge, patches on both cheeks. She did not respond to tretinoin
there are 39 cases in English literature, reported in the 0.05% cream and hydroquinone 4% cream daily for
United States. We herein describe two cases of EO. one year. The cheek macules became erythematous
For comparison, we also present a case of endogenous and darker with hypopigmentation of the surrounding
ochronosis involving the knee articular surface. area (Figure 2A). Histological examination showed
yellow-brown dermal deposits with “banana bodies,”
Case Reports
diagnostic of ochronosis (Figure 2B). She started
Case#1: A 58-year-old female with a history of tazarotene 0.1% gel with pimecrolimus cream and
melasma was treated with hydroquinone 4% cream sun protection. Unfortunately, one year of follow up
daily and tretinoin cream with some improvement. showed minimal to no improvement.
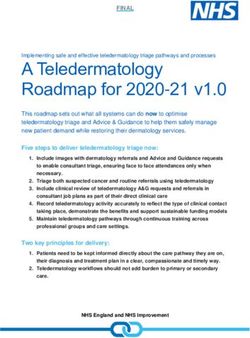
Figure 1. A – Exogenous ochronosis. Case#1; 58-year-old woman with melasma, treated with HQ 4% and
tretinoin, progressed to itchy, tender, and more darken macules; B – Photomicrography of the skin biopsy of skin
case #1, showing elongated yellow-brown deposits (“banana-like”) of acellular material in the superficial dermis
with associated solar elastosis (H&E, 200X magnification).
2-8 Autops Case Rep (São Paulo). 2020 Oct-Dec;10(4):e2020197
Qorbani A, Mubasher A, Sarantopoulos GP, Nelson S, Fung MA
Figure 2. A – Exogenous ochronosis. Case #2, 68-year-old female with hyperpigmented macules which did not
respond to HQ 4% and tretinoin 0.05%. The macules gradually got darker and erythematous with surrounding
hypopigmentation; B – Photomicrography of the skin biopsy of skin case #2, showing banana-like bodies (ochronotic
bodies) in the superficial dermis (H&E, 100X magnification).
Case #3: A 63-year-old male with a history of
knee, hip, and shoulder osteoarthritis and lumbar
degenerative disc disease presented for management
of severe multifocal osteoarthritis. Pigmentation of
both ears was noted on physical examination, which
was reportedly congenital. Radiological findings
showed severe and extensive lumbar disc and facet
joint degeneration with disproportionately minor
osteophytes and calcification of numerous discs,
that favored ochronosis with ochronosis-associated
arthropathy (Figure 3).
Subsequent urine organic acid analysis revealed
elevated homogentisic acid, confirming the diagnosis
of alkaptonuria and endogenous ochronosis.
He underwent bilateral total knee arthroplasty. Gross
examination showed dark black articular surfaces
with eburnation (Figure 4A). Histological examination
showed extensive ochronotic pigment deposition in
fibrocollagenous and synovial tissue, diagnostic of
endogenous ochronosis (Figure 4B).
Figure 3. Radiographic findings in alkaptonuria. X-Ray
radiography of lumbar spine showing extensive lumbar
DISCUSSION disc degeneration with disproportionately minor
osteophytes and calcifications.
Ochrone means bright yellow in Latin. The term
ochronosis was first coined by Rudolf Virchow
(1821‑1902) in 1865, describing the strange dark Two types of ochronosis have been described,
lesions in an elderly man on autopsy, which on H&E exogenous and endogenous. Endogenous ochronosis is
were attributed to the presence of yellowish-brown caused by alkaptonuria, an autosomal recessive disorder
pigments on light microscopic examination. in which the absence of homogentisic acid oxidase
Autops Case Rep (São Paulo). 2020 Oct-Dec;10(4):e2020197 3-8Exogenous Ochronosis (EO): Skin lightening cream causing rare caviar-like lesion with banana-like pigments; review of literature and histological
comparison with endogenous counterpart
Figure 4. A – Alkaptonuria. Gross examination of total knee arthroplasty showing unusual dark articular surface
(head) with eburnation (arrow head); B – Photomicrograph of the synovium of the total arthroplasty in patient with
Alkaptonuria, showing ochronotic bodies in the synovium (arrow) and articular surface (arrow head). (H&E stain,
40X magnification).
leads to accumulation of homogentisic acid (HGA) in Hydroquinone,7 other phenolic compounds (especially
the body. HGA is soluble in water and circulates in the phenol carbolic acid),6,8 systemic antimalarial agents
blood. It is polymerized into a yellow‑green pigment in such as quinine injections,9 oral antimalarial drugs,
the susceptible connective tissue. It binds irreversibly benzene substances, and picric acid, to name a
with the developing collagen fibers and imparts a dark few chemicals that have been associated with
color to the affected tissue. Certain tissues are more causing exogenous ochronosis. Some authors believe
susceptible to the accumulation of HGA, including skin exogenous ochronosis could be a granulomatous
and especially articular cartilage of joints. The most disorder, as it was seen in patients with sarcoidosis and
common areas of skin involvement in alkaptonuria considering the fact that hydroquinone products can
are the nasal tip, sclera of the eyes, cheeks, and the exacerbate the granulomatous reactions in patients.10
pinnae of ears. These patients excrete HGA in urine, The exact pathogenesis of exogenous ochronosis
which is oxidized by ambient oxygen to benzoquinone is not clear. Multiple mechanisms have been proposed
acetate, turning the urine dark black. The diagnosis to explain EO, including i) high concentration of
of alkaptonuria is usually made in the third or fourth hydroquinone stimulates tyrosinase leading to
decade of life. increased pigmentation of the affected tissue; ii) local
Exogenous ochronosis was described later by Pick2 inhibition of activation of homogentisic acid oxidase
and then in further detail by Beddard and Plumtre6 leading to accumulation of homogentisic acid and
describing phenol (carbolic oil) as one of the causative sunlight activation of ochronotic pigments.11 Hull and
agents for EO. Exogenous or pseudo-ochronosis is an Procter12 suggested a causative role of melanocytes, as
infrequent dermatosis and is essentially the same entity they reported melanocyte-free areas of an ochronotic
as endogenous ochronosis but without the systemic patient with vitiligo were not hyperpigmented.13
complications. As the name implies, it is caused In humans, the phenols form complexes such
by the exogenous application of certain products as hydroquinone are excreted after conjugation with
leading up to the accumulation of polymerized HGA glucuronic acid or sulfur. These metabolic pathways
in collagen‑containing tissue, including the dermis, as can only handle a small amount to process and
a bright yellow pigment (ochre). Clinically it presents excrete. In the situation of excess absorption of these
as blue-black macules and/or minute papules in the substances, the excretory pathways are overwhelmed,
malar area, cheeks, forehead, and neck as most of leading to the accumulation of these substances in the
the cosmetic products are applied in these areas. tissues. It has been observed that the tissues where
4-8 Autops Case Rep (São Paulo). 2020 Oct-Dec;10(4):e2020197Qorbani A, Mubasher A, Sarantopoulos GP, Nelson S, Fung MA
oxidation pathways are active in the extracellular matrix, Histologically, endogenous, and exogenous
hydroquinone, and phenols are oxidatively polymerized ochronosis have identical features. Curvilinear yellow-
and stored as a dark amorphous solid pigment. This green elastic fibers and banana-shaped amorphous
pigment is then taken up by the developing fibers and material are seen in the lesional dermis. The overlying
remains in the extracellular matrix of these tissues. epidermis is usually normal, but pseudoepitheliomatous
This pigment accumulation has not been shown to hyperplasia can occur.5,10
affect the functionality of the tissue. The prolonged In long-standing disease, ochronotic fibers
accumulation of polymerized homogentisic acid may degenerate to form colloid milium. Prominent
stimulates melanin production, thus, leading to a inflammatory changes may include multinucleated
blue-black hue/ting to the tissue.5 The dark-blue or giant cells, epithelioid histiocytes, and plasma cells.18
grayish-blue pigment is visible in the skin when this Dermoscopy, reflectance confocal microscopy,
microscopy with UV surface excitation, or other
process takes place in the dermis, especially the dermis
techniques could also be a helpful tool in the diagnosis
of the face because of excessive and prolonged use
of ochronosis.19,20
of hydroquinone containing products and depends
on the depth of pigment accumulation. Clinically, The clinical manifestations have been described
in different stages by Hardwick et al. 21 in their
it can manifest as macules and papules obliterating
epidemiological study:
the follicular orifices with accentuation of the normal
pseudo network of the skin. Grade I – Faint macular sooty pigmentation
A recent study at Boston University on 11 patients 14
showed that topically applied hydroquinone (HQ) Grade II – Distinct macular stippling/small caviar-like
affects both elastic fibers and melanin production; HQ papules11
inhibits homogentisate 1,2dioxygenase (HGD) leading
to accumulation HGA, which will be engulfed by Grade III – Dark deposits and papules
fibroblasts that causes aberrant elastic fiber production.
HQ also inhibits tyrosinase, which leads to increase Grade IV – Colloid milia (1 mm and greater)
immaturity and apoptosis of melanosomes, result in
decrease photoprotection and deeper penetration of Grade V – Keloid-like nodules and cysts
UV radiation and increase solar elastosis. These two
effects lead to HGA and solar elastotic fibers, which A review of the English-speaking literature was
eventually develop ochronotic bodies in elastosis. performed using the PubMed database by searching
the terms “ochronosis” and “Exogenous Ochronosis”.
By far, the most notorious offender is hydroquinone
Incidence of exogenous ochronosis (EO) has been
products. It is widely used as a bleaching agent to
extremely low in the United States (US), and only
decrease the pigmentation of the skin. Hydroquinone is 39 cases have been described in the English literature
a mild local anesthetic and acts by reducing the number since 1983 to 2020 (Table 1).
of melanocytes, decreasing the production of melanin
One possible explanation can be attributed
by the remaining melanocytes, and bleaching the
to EO being under reported or underdiagnosed.
melanin pigment in the skin.15 It has been in use for the Hyperpigmentation and melasma commonly affect the
treatment of multiple hyper-pigmented conditions and female population of the African, Hispanic and Asian
is considered an excellent agent for conditions such as descends. In certain Asian communities, the incidence of
melasma.16 It was estimated that more than 10 million hyperpigmentation is estimated to be around 40%.16 As a
tubes containing hydroquinone containing compounds result of demographic and cultural shifts, it is reasonable
or related known ochronotic products are sold over the to believe that the use of bleaching and whitening
counter each year in the United States.17 On August compounds, including hydroquinone products, may
29, 2006, the U.S. Food and Drug Administration (FDA) increase, leading to the comparatively more frequent
proposed a ban on over-the-counter sales of cosmetic encounter of exogenous ochronosis in the US.
products containing hydroquinone as skin-bleaching Treatment of OE has been unsatisfactory with
(lightening) ingredient. the achievement of sub-optimal results. Cryotherapy,
Autops Case Rep (São Paulo). 2020 Oct-Dec;10(4):e2020197 5-8Exogenous Ochronosis (EO): Skin lightening cream causing rare caviar-like lesion with banana-like pigments; review of literature and histological
comparison with endogenous counterpart
Table 1. Exogenous Ochronosis Reported in the US from 1983 to 2020.
# Year Author PMID Age Sex Ethnicity Dosage Used Duration
1 1983 Cullison 6863651 58 F Black 2% HQ 2.5 years
2 1985 Hoshaw 3966811 75 F Black 2% HQ 2 years
3 1985 Hoshaw 3966811 49 F Black OTC skin lightening cream 2 months
4 1985 Penneys 4037813 NA NA NA NA NA
5 1987 Connor 3800410 72 F Black Skin-lightening cream Many years
6 1988 Lang 3192777 74 F White HQ and Mercury cream Many years
7 1988 Lawrence 3372785 62 F Black 1% HQ 2-3 years
8 1988 Lawrence 3372785 46 F Black 1% HQ NA
9 1988 Fisher 3203531 47 F Black 4% HQ 18 months
10 1990 Howard 2311433 36 F Hispanic 2% HQ 4 months
11 1990 Diven 2246407 53 F Black 2% HQ 2-3 months
12 1991 Jordaan 1928626 56 M Black 6.5-7.5% HQ Many years
13 1991 Jordaan 1928626 39 F Black Skin-lightening cream 5 years
14 1992 Martin 1603931 44 F Black 2% HQ 3-4 years
15 1992 Martin 1603931 56 F Black OTC skin-lightening creams 30 years
16 1993 Snider 8463477 59 F Black 2-4% HQ Many years
17 1995 Jacyk 7695007 49 F Black NA NA
18 1995 Jacyk 7695007 50 F Black NA NA
19 1995 Jacyk 7695007 70 F Black NA NA
20 1995 Jacyk 7695007 40 F Black NA NA
21 1995 Jacyk 7695007 49 F Black NA NA
22 1995 Jacyk 7695007 43 F Black NA NA
23 2000 Kramer 10767690 50 F Hispanic 2% HQ 30 years
24 2001 Bowman 11534909 75 F Black 2% HQ up to 1 year
25 2004 Bellew 15056151 47 F Black NA Many months
26 2004 Bellew 15056151 46 M Native American NA 1 year
27 2006 Huerta 16468299 70 F NA 2% HQ 6 years
28 2008 Merola 19061605 55 F NA NA Many years
29-39 2019 Ho 31725487 5 -7 F
th th
Black NA NA
NA: Data is not available, F: Female, M: Male, OTC: Over the counter, HQ: hydroquinone.
tretinoin, and topical acetic acid have been used impairs quality of life. It is of utmost significance to
without dramatic success. However, promising results distinguish EO from melasma, Ota nevus, drug-induced
have been reported using Q-switched alexandrite hyperpigmentation, post-inflammatory pigmentation,
laser, 22 Q-switched ruby laser, 23 CO2 laser and and dermatosis papulosa nigra, in part because of the
dermabrasion.24 Nevertheless, EO remains a difficult risk of being prescribed the very causative agent of the
condition to treat, emphasizing the importance of disease, leading to further worsening of the condition.
early detection.
A review of the literature for EO in the US revealed
that most of the cases were the result of 1-2% HQ ACKNOWLEDGEMENTS
creams with only a handful reporting use of the 3-4%
hydroquinone. Thus, low concentrations of these This study includes data from an abstract that
products applied for a longer period, or increased was accepted for a presentation at the American
frequency can also result in EO. 25-27 Furthermore, Society of Dermatopathologist (ASDP) 2019 in
EO is a psychologically debilitating condition that San Diego, USA.
6-8 Autops Case Rep (São Paulo). 2020 Oct-Dec;10(4):e2020197Qorbani A, Mubasher A, Sarantopoulos GP, Nelson S, Fung MA
REFERENCES http://dx.doi.org/10.1016/S0190-9622(98)70001-5.
PMid:9777759.
1. Findlay GH. Ochronosis. Clin Dermatol. 1989;7(2):28- 14. Ho JD, Vashi N, Goldberg LJ. Exogenous ochronosis
35. http://dx.doi.org/10.1016/0738-081X(89)90054-0. as an elastotic disease: a light-microscopic approach.
PMid:2667739. Am J Dermatopathol. 2019;Publish Ahead of Print.
2. Laymon CW. Ochronosis. AMA Arch Derm Syphilol. http://dx.doi.org/10.1097/DAD.0000000000001571.
1953;67(6):553-60. http://dx.doi.org/10.1001/ PMid:31725487.
archderm.1953.01540060015003. PMid:13050178. 15. Andersen FA, Bergfeld WF, Belsito DV, et al. Final amended
3. Phillips JI, Isaacson C, Carman H. Ochronosis in black South safety assessment of hydroquinone as used in cosmetics.
Africans who used skin lighteners. Am J Dermatopathol. Int J Toxicol. 2010;29(6, Suppl):274S-87. http://dx.doi.
1986;8(1):14-21. http://dx.doi.org/10.1097/00000372- org/10.1177/1091581810385957. PMid:21164074.
198602000-00003. PMid:3706666. 16. Simmons BJ, Griffith RD, Bray FN, Falto-Aizpurua LA,
4. Kramer KE, Lopez A, Stefanato CM, Phillips TJ. Exogenous Nouri K. Exogenous ochronosis: a comprehensive review
ochronosis. J Am Acad Dermatol. 2000;42(5 Pt 2):869- of the diagnosis, epidemiology, causes, and treatments.
71. http://dx.doi.org/10.1016/S0190-9622(00)90257-3. Am J Clin Dermatol. 2015;16(3):205-12. http://dx.doi.
PMid:10767690. org/10.1007/s40257-015-0126-8. PMid:25837718.
5. Findlay GH, Morrison JG, Simson IW. Exogenous ochronosis 17. Levitt J. The safety of hydroquinone: a dermatologist’s
and pigmented colloid milium from hydroquinone response to the 2006 Federal Register. J Am
bleaching creams. Br J Dermatol. 1975;93(6):613-22. Acad Dermatol. 2007;57(5):854-72. http://dx.doi.
http://dx.doi.org/10.1111/j.1365-2133.1975.tb05110.x. org/10.1016/j.jaad.2007.02.020. PMid:17467115.
PMid:1220808. 18. Dogliotti M, Leibowitz M. Granulomatous ochronosis
6. Beddard AP, Plumtre CM. A further note on ochronosis -- a cosmetic-induced skin disorder in Blacks. S Afr Med
associated with carboluria. Q J Med. 1912(4);5:505-8. J. 1979;56(19):757-60. PMid:505210.
7. Jordaan HF, Van Niekerk DJ. Transepidermal elimination 19. Gil I, Segura S, Martínez-Escala E, et al. Dermoscopic and
in exogenous ochronosis. Am J Dermatopathol. reflectance confocal microscopic features of exogenous
1991;13(4):418-24. http://dx.doi.org/10.1097/00000372- ochronosis. Arch Dermatol. 2010;146(9):1021-5.
199108000-00015. PMid:1928626. http://dx.doi.org/10.1001/archdermatol.2010.205.
PMid:20855704.
8. Penneys NS. Ochronosislike pigmentation from
hydroquinone bleaching creams. Arch Dermatol. 20. Qorbani A, Fereidouni F, Levenson R, et al. Microscopy with
1985;121(10):1239-40. http://dx.doi.org/10.1001/ ultraviolet surface excitation (MUSE): A novel approach
archderm.1985.01660100019003. PMid:4037813. to real-time inexpensive slide-free dermatopathology.
J Cutan Pathol. 2018;45(7):498-503. http://dx.doi.
9. Bruce S, Tschen JA, Chow D. Exogenous ochronosis org/10.1111/cup.13255. PMid:29660167.
resulting from quinine injections. J Am Acad Dermatol.
1986;15(2 Pt 2):357-61. http://dx.doi.org/10.1016/ 21. Hardwick N, Van Gelder LW, Van der Merwe CA, Van der
S0190-9622(86)70178-3. PMid:3734183. Merwe MP. Exogenous ochronosis: an epidemiological
study. Br J Dermatol. 1989;120(2):229-38. http://
10. Jacyk W. Annular granulomatous lesions in exogenous dx.doi.org/10.1111/j.1365-2133.1989.tb07787.x.
ochronosis are manifestation of sarcoidosis. Am J PMid:2923796.
Dermatopathol. 1995;17(1):18-22. http://dx.doi.
org/10.1097/00000372-199502000-00004. 22. Bellew SG, Alster TS. Treatment of exogenous ochronosis
PMid:7695007. with a Q-switched alexandrite (755 nm) laser. Dermatol
Surg. 2004;30(4 Pt 1):555-8. PMid:15056151.
11. Levin CY, Maibach H. Exogenous ochronosis: an update
on clinical features, causative agents and treatment 23. Kramer K, Lopez A, Stefanato C, Phillips TJ. Exogenous
options. Am J Clin Dermatol. 2001;2(4):213-7. http:// ochronosis. J Am Acad Dermatol. 2000;42(5 Pt 2):869-
dx.doi.org/10.2165/00128071-200102040-00002. 71. http://dx.doi.org/10.1016/S0190-9622(00)90257-3.
PMid:11705248. PMid:10767690.
12. Hull P, Procter P. The melanocyte: an essential link in 24. Kanechorn-Na-Ayuthaya P, Niumphradit N, Aunhachoke
hydroquinone-induced ochronosis. J Am Acad Dermatol. K, Nakakes A, Sittiwangkul R, Srisuttiyakorn C. Effect
1990;22(3):529-31. http://dx.doi.org/10.1016/S0190- of combination of 1064 nm Q-switched Nd:YAG and
9622(08)80401-X. PMid:2312837. fractional carbon dioxide lasers for treating exogenous
ochronosis. J Cosmet Laser Ther. 2013;15(1):42-5.
13. Touart D, Sau P. Cutaneous deposition diseases. Part http://dx.doi.org/10.3109/14764172.2012.748198.
II. J Am Acad Dermatol. 1998;39(4 Pt 1):527-44. PMid:23368689.
Autops Case Rep (São Paulo). 2020 Oct-Dec;10(4):e2020197 7-8Exogenous Ochronosis (EO): Skin lightening cream causing rare caviar-like lesion with banana-like pigments; review of literature and histological
comparison with endogenous counterpart
25. Martins VM, Sousa AR, Portela NC, Tigre CA, Gonçalves 1988;18(5 Pt 2):1207-11. http://dx.doi.org/10.1016/
LM, Castro RJ Fo. Exogenous ochronosis: case report and S0190-9622(88)70126-7. PMid:3372785.
literature review. An Bras Dermatol. 2012;87(4):633-6.
http://dx.doi.org/10.1590/S0365-05962012000400021. 27. Gandhi V, Verma P, Naik G. Exogenous ochronosis after
PMid:22892783. prolonged use of topical hydroquinone (2%) in a 50-year-
old Indian female. Indian J Dermatol. 2012;57(5):394-
26. Lawrence N, Bligard CA, Reed R, Perret WJ. Exogenous 5. http://dx.doi.org/10.4103/0019-5154.100498.
ochronosis in the United States. J Am Acad Dermatol. PMid:23112363.
This study carried out at the University of California San Francisco (UCSF), UCSF Medical Center at Mission
Bay, Pathology Department, San Francisco, USA, in collaboration with the University of California Los Angeles
(UCLA), and the University of California Davis (UC Davis).
Authors’ contributions: Amir Qorbani, Adnan Mubasher, George Peter Sarantopoulos, Scott Nelson and Maxwell
Alexander Fung substantially contributed to the conception and design of the work, acquisition, analysis, and
interpretation of data, review of literature, and preparing the draft. All authors collectively proofread the final
version of the manuscript and approved it for publication.
Ethics statement: The institutional patient’s consent was retained, and the manuscript is by the Institutional
Ethics committee.
Conflict of interest: None
Financial support: None
Submitted on: February 21st, 2020
Accepted on: June 17th, 2020
Correspondence
Amir Qorbani
University of California, San Francisco (UCSF), UCSF Medical Center at Mission Bay, Pathology Department
1825 4th Street, M2369, 94158, San Francisco, CA, USA
Phone: +1 (949) 609-9916
amir.qorbani@ucsf.edu
8-8 Autops Case Rep (São Paulo). 2020 Oct-Dec;10(4):e2020197You can also read