Evaluation and Management of Patients With Heart Disease and Cancer: Cardio-Oncology
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
REVIEW
Evaluation and Management of Patients With
Heart Disease and Cancer: Cardio-Oncology
Joerg Herrmann, MD; Amir Lerman, MD; Nicole P. Sandhu, MD, PhD;
Hector R. Villarraga, MD; Sharon L. Mulvagh, MD; and Manish Kohli, MD
Abstract
The care for patients with cancer has advanced greatly over the past decades. A combination of earlier
cancer diagnosis and greater use of traditional and new systemic treatments has decreased cancer-related
mortality. Effective cancer therapies, however, can result in short- and long-term comorbidities that can
decrease the net clinical gain by affecting quality of life and survival. In particular, cardiovascular com-
plications of cancer treatments can have a profound effect on the health of patients with cancer and are
more common among those with recognized or unrecognized underlying cardiovascular diseases. A new
discipline termed cardio-oncology has thus evolved to address the cardiovascular needs of patients with
cancer and optimize their care in a multidisciplinary approach. This review provides a brief introduction
and background on this emerging field and then focuses on its practical aspects including cardiovascular
risk assessment and prevention before cancer treatment, cardiovascular surveillance and therapy during
cancer treatment, and cardiovascular monitoring and management after cancer therapy. The content of
this review is based on a literature search of PubMed between January 1, 1960, and February 1, 2014,
using the search terms cancer, cardiomyopathy, cardiotoxicity, cardio-oncology, chemotherapy, heart failure,
and radiation.
ª 2014 Mayo Foundation for Medical Education and Research n Mayo Clin Proc. 2014;89(9):1287-1306
O
ver the past decades, there has been another level of complexity. Involvement of
a tremendous improvement in the cardiologists has thus become more and more
survival rates of a number of cancers advisable not only to most optimally manage From the Department of
Internal Medicine, Division
and a steady increase in the number of cancer cardiovascular complications of cancer therapy of Cardiovascular Diseases
survivors (see Supplemental Figure 1 and but also to assist in the overall care of patients (J.H., A.L., H.R.V., S.L.M.),
Supplemental Table 1 [available online at with cancer from the initial assessment to survi- Division of General Inter-
nal Medicine (N.P.S.), and
http://www.mayoclinicproceedings.org]). As a vorship. This integrative approach has been Department of Oncology
result, an increasing number of patients with termed cardio-oncology,6,7 and herein we will (M.K.), Mayo Clinic,
cancer are now being followed not only by on- reflect on this emerging field. An overview of Rochester, MN.
cologists or hematologists but also by general cancer therapyeinduced cardiotoxicity is pro-
practitioners. Cardiovascular complications vided in the first part and practical steps to its
are not uncommonly encountered in these pa- evaluation, management, and prevention in
tients with potentially profound impact on the following parts. The content is based on a
morbidity and mortality, and thus their recog- literature search of PubMed between January
nition and management has become an impor- 1, 1960, and February 1, 2014, using the
tant element in the overall care for patients with search terms cancer, cardiomyopathy, cardiotox-
cancer.1,2 Furthermore, there is an intriguing icity, cardio-oncology, chemotherapy, heart fail-
geographic overlap in the prevalence of cancer ure, and radiation.
and cardiovascular disease (see Supplemental
Figure 2 [available online at http://www. PART 1: CHEMOTHERAPY AND RADIATION
mayoclinicproceedings.org]) and expansion of THERAPYeINDUCED CARDIOTOXICITY
cancer therapies to more elderly individuals The armamentarium for the treatment of various
with a greater burden of comorbidities.3-5 cancers has increased substantially over the past
Hence, an increasing number of patients with decades, with a gradual change from a cell cycle
preexisting cardiovascular diseases are now be- kineticsebased approach to more specific tar-
ing considered for cancer therapy, which adds geting of crucial signaling pathway(s). In most
Mayo Clin Proc. n September 2014;89(9):1287-1306 n http://dx.doi.org/10.1016/j.mayocp.2014.05.013 1287
www.mayoclinicproceedings.org n ª 2014 Mayo Foundation for Medical Education and ResearchMAYO CLINIC PROCEEDINGS
both (eg, bevacizumab and sunitinib). Radiation
ARTICLE HIGHLIGHTS therapy leads to an all-encompassing form of
injury to the myocardium, the pericardium,
n Advances in cancer therapy have allowed for increasing
the valvular apparatus, and the coronary vascu-
numbers of long-term cancer survivors but have also generated lature from the epicardial to the microvascular
increasing potential and significance of cardiovascular level, though modern approaches appear to
complications. reduce cardiovascular damage compared with
n Involvement of cardiovascular disease specialists has therefore older techniques. The focus herein will be on
cardiotoxicity, and vascular toxicities will be dis-
become advisable from the initial assessment through survi-
cussed only as much as they relate to this topic.
vorship, and this integrative approach has been coined “cardio-
oncology.” Chemotherapy-Induced Cardiotoxicity
n Cardiotoxicity related to cancer therapy is currently defined by To organize the broad spectrum of cardiotoxic-
a decrease in cardiac function and categorized into 2 types: ity due to chemotherapy, an operational classi-
irreversible injury type (type 1) or reversible dysfunction type fication system was introduced by Ewer and
Lippman23 (see Supplemental Table 2 [available
(type 2).
online at http://www.mayoclinicproceedings.
n Monitoring and management algorithms for either type of org]). This system is based on the presence of
chemotherapy-induced cardiomyopathy are evolving around structural abnormalities and extent of func-
the central paradigm of early recognition and early treatment. tional reversibility. Accordingly, a distinction
n Radiation-induced cardiotoxicity encompasses a broad spec- can be made between an injury type (type 1
chemotherapy-induced cardiotoxicity) and a
trum of cardiac diseases that potentiates any chemotherapy-
dysfunction type (type 2 chemotherapy-
induced cardiotoxicity. induced cardiotoxicity). Given that cardiac
n Treatment of cardiovascular conditions of patients with cancer magnetic resonance imaging (MRI) has provided
generally follows the American Heart Association/American evidence for scar formation in patients with pre-
College of Cardiology guidelines with some particular nuances. sumed type 2 cardiotoxicity and appropriate
heart failure therapy led to an improvement in
n Preventive efforts should be considered for patients at an
presumed type 1 cardiotoxicity, the outlined
estimated high risk for cancer therapyeinduced cardiotoxicity, classification pattern may not be as much of an
with the preferred drugs being angiotensin-converting enzyme absolute as perceived.24,25 Also, one has to be
inhibitors and the specific b-blockers carvedilol or nebivolol. cognizant of the fact that there is no consensus
definition of cardiotoxicity at present.26,27 The
one used in recent times was developed by the
cases, these are cell proliferation pathways, Cardiac Review and Evaluation Committee of
which are regulated by receptor and nonrecep- trastuzumab-associated cardiotoxicity, and it de-
tor tyrosine kinases, leading to the development fines chemotherapy-induced cardiotoxicity as a
of a wide range of inhibitors. The extent to decrease in left ventricular ejection fraction
which this would interfere with normal cardio- (LVEF) by 5% or more to less than 55% in the
vascular function has often not been well antic- presence of symptoms of heart failure (diag-
ipated, but such “off-target” effects have become nosed by a cardiologist) or an asymptomatic
clinically relevant and revealing with regard to decrease in LVEF by 10% or more to less than
the functional role of signaling pathways in the 55%.28
cardiovascular system. A comprehensive list of
currently used cancer drugs with a propensity Chemotherapy-Induced Cardiotoxicity Type 1
for cardiovascular toxicities is provided in Induction of cardiomyocyte injury is a key distin-
Table 1, along with their Food and Drug Admin- guishing feature of this type of chemotherapy-
istrationeapproved cancer indications. 8-22 induced cardiotoxicity, with anthracyclines
Considering the spectrum of cardiovascular as the prototype class of drugs in this category.
effects, a distinction can be made between those Given the imposition of structural changes, it
agents that primarily affect cardiac function (eg, has become widely accepted that this type of
anthracyclines and trastuzumab), vascular func- cardiotoxicity is not reversible. Moreover,
tion (eg, 5-fluorouracil and capecitabine), or anthracycline-induced cardiomyopathy has
n n
1288 Mayo Clin Proc. September 2014;89(9):1287-1306 http://dx.doi.org/10.1016/j.mayocp.2014.05.013
www.mayoclinicproceedings.orgCARDIO-ONCOLOGY
TABLE 1. Most Commonly Used Chemotherapeutic Agents With Cardiotoxicity Potentiala
Chemotherapeutic Cardiomyopathy
class and agents incidence Other types of cardiovascular toxicity Clinical use in cancer therapy
Anthracyclines
Doxorubicin8 3%-26% Myopericarditis, cardiac arrhythmias, Acute myeloid leukemia, acute myelogenous leukemia,
ECG abnormalities chronic lymphocytic leukemia, Hodgkin and non-
Hodgkin lymphoma, Kaposi sarcoma, mycosis fungoides,
thyroid cancer, breast cancer, Ewing sarcoma, transitional
cell bladder cancer, multiple myeloma, gastric cancer,
prostate cancer, lung cancer, nephroblastoma
Epirubicin8 0.9%-3.3% Cardiac arrhythmias, ECG Breast, esophageal, and gastric cancer
abnormalities, arterial embolism
Idarubicin8 5%-18% ECG abnormalities Acute myeloid leukemia
Mitoxantrone9 0.2%-30% Cardiac arrhythmias, ECG abnormalities, Acute nonlymphocytic leukemias, prostate cancer (multiple
myocardial ischemia, hypertension sclerosis)
Alkylating agents
Cyclophosphamide 7%-28% Peri-/myocarditis, cardiac tamponade, Bone marrow transplant, bladder cancer, lung cancer,
(high dose)8 arrhythmias sarcomas, anal cancer, myeloproliferative disorders,
chronic myelogenous leukemias
Ifosfamide8 17% Arrhythmias, cardiac arrest, myocardial Testicular cancer, cervical cancer, Hodgkin and non-Hodgkin
hemorrhage, myocardial infarction lymphoma, Ewing sarcoma, osteosarcoma, soft tissue
sarcoma
Busulfan10 Rare Endomyocardial fibrosis, pericardial effusion Chronic myelogenous leukemia, hematopoietic stem cell
and tamponade, ECG changes, chest pain, conditioning regimen, polycythemia vera, essential
hyper-/hypotension, thrombosis, arrhythmias thrombocythemia
Mitomycin10 10% Stomach or pancreas adenocarcinoma, anal carcinoma,
bladder cancer
Antimetabolites
Clofarabine8 27% Arrhythmias, hypo-/hypertension, pericarditis/ Acute lymphocytic leukemia
pericardial effusion
5-Fluorouracil11 2%-20% Coronary vasospasm, myocardial ischemia Advanced colon cancer, anal cancer, gastrointestinal
and infarction, arrhythmias, ECG changes cancers, pancreatic cancer, hepatobiliary cancers, breast
including ventricular ectopy, hypotension cancer, bladder cancer, head and neck cancers, and as a
radiation sensitizer in several tumors
Capecitabine11 2%-7% Coronary vasospasm, myocardial ischemia Breast cancer, advanced colon cancer, anal cancer,
and infarction, arrhythmias, ECG changes, gastrointestinal cancers, pancreatic cancer, hepatobiliary
thrombosis cancers
Cytarabine10 Undefined Pericarditis, chest pain (including angina) Hodgkin and non-Hodgkin lymphoma, acute leukemia
(myeloid and lymphocytic)
Platinum agents
Cisplatin10 Rare Arterial vasospasm, cardiac/cerebral/ Lung cancer, bladder cancer, sarcomas, testicular cancer,
mesenteric/limb ischemia, ovarian cancer, head and neck cancer, metastatic breast
hypo-/hypertension, arrhythmias cancer, cancer of unknown origin, esophageal cancer
Antimicrotubule agents
Vincristine10 25% Hyper-/hypotension, myocardial ischemia Acute lymphocytic leukemia, central nervous system
and infarction, arrhythmias tumors, Hodgkin and non-Hodgkin lymphoma, multiple
myeloma, Ewing sarcoma, ovarian cancer, small cell lung
cancer, thymoma
Monoclonal antibody-based tyrosine kinase inhibitors
Bevacizumab8 1.7%-3% Hypertension, arterial and venous Renal cancer, colorectal cancer, lung cancer
thromboembolism
Trastuzumab8 2%-28% Hyper-/hypotension, arrhythmia, vascular HER2þ breast cancer, HER2þ gastric cancer
thrombosis
Pertuzumab12 3%-7% HER2þ breast cancer
Alemtuzumab13 Rare Hypo-/hypertension, arrhythmia Chronic lymphocytic leukemia, cutaneous T-cell
lymphoma, bone marrow transplant
Continued on next page
Mayo Clin Proc. n September 2014;89(9):1287-1306 n http://dx.doi.org/10.1016/j.mayocp.2014.05.013 1289
www.mayoclinicproceedings.orgMAYO CLINIC PROCEEDINGS
TABLE 1. Continued
Chemotherapeutic Cardiomyopathy
class and agents incidence Other types of cardiovascular toxicity Clinical use in cancer therapy
Small-molecule tyrosine kinase inhibitors
Dasatinib8 2%-4% Pericardial effusion, hypertension, Philadelphia chromosome-positive chronic myeloid
arrhythmia, QT interval prolongation leukemia and acute lymphoblastic leukemia
Imatinib mesylate8 0.5%-1.7% Pericardial effusion and tamponade, anasarca, Philadelphia chromosome-positive chronic myeloid
arrhythmias, hypertension, Raynaud leukemia and acute lymphoblastic leukemia,
disease gastrointestinal stromal tumors, dermatofibrosarcoma
protuberans, hypereosinophilic syndrome
Lapatinib14 1.5%-2.2% QTc interval prolongation, myocardial HER2þ breast cancer
ischemia (Prinzmetal angina)
Sunitinib15-17 3%-15% Hypertension, arterial and venous Renal cell cancer, pancreatic neuroendocrine tumors,
thrombosis, arrhythmias, aortic dissection, gastrointestinal stromal tumors
QTc prolongation
Sorafenib18 4%-28% Hypertension, thrombosis, coronary Renal cell cancer, hepatocellular carcinoma, differentiated
vasospasm, myocardial ischemia/infarction thyroid carcinoma
Pazopanib18,19 7%-13% Hypertension, thrombosis, myocardial Renal cell cancer, soft tissue sarcoma
ischemia/infarction, bradycardia, QTc
interval prolongation
Proteasome inhibitor
Bortezomib8 2%-5% Ischemia, bradycardia Multiple myeloma, mantle cell lymphoma
Miscellaneous
All-trans-retnoic 6% Hypotension, pericardial effusion Acute myeloid leukemia (promyelocytic leukemia)
acid10
Pentostatin10 3%-10% Myocardial ischemia and infarction, acute Hairy cell lymphoma, chronic lymphocytic leukemia,
arrhythmias cutaneous T-cell lymphoma
Interferon 25% Hypotension, myocardial ischemia and Metastatic melanoma, renal cell carcinoma
alpha-2b20 infarction, ECG changes, sudden cardiac
death
Aflibercept21,22 1%-6.8% Hypertension, myocardial ischemia/infarction, Metastatic colorectal cancer
stroke
a
ECG ¼ electrocardiographic; QTc ¼ corrected QT.
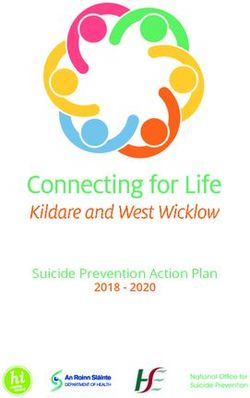
been considered to be associated with a prog- interstitial edema.31 It manifests primarily with
nosis that is worse than that for ischemic or electrocardiographic (ECG) changes (20%-30%)
dilated cardiomyopathies and possibly even for and arrhythmias (up to 3%), and occasionally
the primary cancer for which it was given.29,30 with reversible cardiac dysfunction, even acute
These views have been refined by the observa- heart failure and peri-/myocarditis. The afore-
tion of reversibility as a function of timely mentioned clinically much more recognized
institution of appropriate therapy.25 Although type is the chronic form of anthracycline-
anthracycline-induced cardiomyopathy was induced cardiotoxicity with early onset within 1
found to be rarely and never fully reversible year or late onset more than 1 year after comple-
when recognized and treated late, resolution tion of therapy.32 This type is marked by cardiac
can be noted with close surveillance and prompt dysfunction rather than ECG abnormalities. On
institution of therapy early on (Figure 1).25 histology, cytoplasmic vacuolization due to
Traditionally, a distinction has been made swelling of the sarcoplasmic reticulum and mito-
between an acute and a chronic form of chondria can be noted, as well as disruption of or-
anthracyline-induced cardiotoxicity. The acute ganelles, myocyte death, myofibrillar loss, and/or
form develops at the time (or within 1 week) of myofibrillar disarray.31,33 Studies on the exact
administration of anthracyclines and resembles mechanisms responsible for the cardiotoxicity of
an acute toxic myocarditis with myocyte damage anthracyclines have remained without a unifying
(pyknotic debris), inflammatory infiltrates, and explanation. The prevailing theory has been the
n n
1290 Mayo Clin Proc. September 2014;89(9):1287-1306 http://dx.doi.org/10.1016/j.mayocp.2014.05.013
www.mayoclinicproceedings.orgCARDIO-ONCOLOGY
“iron and free-radical hypothesis.”34 Accord-
100
ingly, reductases in cardiomyocytes catalyze the
addition of an electron to the quinone moiety
of anthracyclines, which leads to the formation 80
of a semiquinone that then regenerates the 64%
Responders (%)
quinone state by reducing molecular oxygen to 60
superoxide anion and its dismutation product
hydrogen peroxide (the so called “redox 40
cycling”).34 The propensity toward toxicity is 28%
significantly increased when these products 20
interact with low-molecular iron, generating a 7%
0% 0% 0% 0%
surge of oxidative stress (Fenton reaction). The 0
oxidative modification of proteins and lipids as 1-2 2-4 4-6 6-8 8-10 10-12 >12
well as genomic and mitochondrial DNA damage (n=75) (n=35) (n=20) (n=8) (n=7) (n=7) (n=44)
are the downstream consequences.34,35 Uncou- A Months
pling of the electron transport chain with im-
pairment of oxidative phosphorylation and 100
Death HF Arrhythmias
adenosine triphosphate synthesis contributes
further to mitochondrial dysfunction and dam- Responders 0% 0% 3%
Cardiac event-free rate (%)
80 (n=85)
age.36,37 Finally, the inhibition of topoisomerase
2-b in cardiomyocytes has recently been 60
proposed as an additional, if not key, mediator
of anthracycline-induced cardiomyopathy.38
40 Non-responders 4% 8% 16%
Anthracyclines thereby induce DNA damage
(n=90)
and impair its repair, which are the mechanisms Partial responders 0% 4% 23%
20
responsible for tumor cell death. In crucial (n=26)
distinction, however, it is the inhibition of topo-
0
isomerase 2-a in cancer cells.37
0 3 6 9 12 15 18 21 24
Other drugs that cause structural damage to
B Months
the heart include alkylating agents such as cyclo-
phosphamide at high doses (Table 1).39,40 It
FIGURE 1. Illustration of the percentage of patients with an improvement in
develops as an acute myopericarditis, which (usu- left ventricular ejection fraction to greater than 50%, depending on the
ally) does not take the course of chronic injury timing of the initiation of heart failure therapy after the diagnosis of
and hence does not meet all criteria for a type 1 anthracycline-induced cardiomyopathy (A) and survival free of cardiac
pattern. Similarly, the tyrosine kinase inhibitor events for patients with an improvement in left ventricular ejection fraction
sunitinib manifests cardiotoxicity that meets less than (partial responders) or greater than 50% (responders) (B).
some, but not all, of the above criteria and has, From Cardinale et al,25 with permission.
in fact, been considered to represent a type 2
pattern.41,42 Histology is not completely un-
remarkable and exhibits cardiomyocyte hy- pathway and the vascular endothelial growth
pertrophy with mild degenerative changes factor (VEGF) receptor pathway leads to hypoxia,
and myocyte vacuolization.15 However, edema, hypoxia-inducible genes, and a pattern of
inflammation, regional infarct or focal cell necro- myocardial hibernation rather than infarction.37
sis, and fibrosis are not seen.15 Transmission elec- This may explain the reversibility of sunitinib car-
tron microscopy exhibits a normal sarcomere diomyopathy in most, but not all, patients.17
structure but provides evidence of mitochondrial
injury.15 Mechanistically, sunitinib inhibits aden- Chemotherapy-Induced Cardiotoxicity Type 2
osine monophosphateeactivated protein kinase, This type of treatment-induced cardiotoxicity is
which interferes with the ability of the cardiomyo- marked by the absence of structural abnor-
cyte to adapt to energy demands with untoward malities and reversibility on cessation of therapy.
consequences for cardiac function.43,44 Further- Trastuzumab (Herceptin) is the prototype drug,
more, other studies suggest that the inhibition and the key pathophysiological mechanism is
of the platelet-derived growth factor receptor interference with the HER-2/ErbB2eregulated
Mayo Clin Proc. n September 2014;89(9):1287-1306 n http://dx.doi.org/10.1016/j.mayocp.2014.05.013 1291
www.mayoclinicproceedings.orgMAYO CLINIC PROCEEDINGS
signaling pathways in cardiomyocytes.45 These order of 45-50 Gy). Modifications of radiation
are key stress, adaption, and survival path- protocols, careful radiation field planning, and
ways, which explains why the incidence of techniques such as breath holding have been
cardiotoxicity is extremely high when trastu- implemented to reduce the radiation dose to
zumab is given in close temporal relationship the cardiovascular structures. As outlined in
with anthracyclines.42 Furthermore, mice recent studies and not without controversy,
with a cardiac-specific deletion of the ErbB2 however, there may not be a threshold level
receptor develop a dilated cardiomyopathy below which radiation therapy is safe to the
and are unable to tolerate high afterload (blood heart and the vascular system.51-53 From a cur-
pressure) challenges.45,46 As not all HER-2/ rent practice standpoint though, radiation-
ErbB2 pathway inhibitors, however, share the induced heart disease remains of significance,
same potential for cardiomyopathy, the ulti- as most patients seen today are those who
mate consequences are dictated by the net ef- had higher exposures 20 to 30 years ago.2,51,54
fect on multiple downstream targets.14 Radiation therapy induces a spectrum of
Another example of a drug that can cause cardiotoxicities that differ considerably from
type 2 treatment-induced cardiotoxicity is bev- chemotherapy-induced cardiotoxic effects and
acizumab. In contrast to the aforementioned affect all layers of the heart. Acute pericarditis
drugs, the cardiomyocyte does not appear to used to be the most frequent complication,
be the primary culprit. Rather, bevacizumab but advances reduced its incidence from 25%
binds to and prevents VEGF from interacting to 2%.2 Chronic pericarditis still develops
with its receptor(s), which reside primarily on with a clinical incidence of 3% at 20 years
endothelial cells. Still, cardiotoxicity including and 12% at 30 years in those who underwent
clinical heart failure has been reported with chest radiation at a dose of 35 Gy or greater.55
this drug.47 Reversibility of cardiac dysfunction Fibrinous exudates, fibrous adhesions, and
has been noted, suggesting that no structural collagenous thickening (predominantly of the
damage to the cardiomyocytes is induced, parietal pericardium) are characteristic fea-
though histological confirmation is lacking.48 tures.56 Similar fibrotic changes can be noted
The underlying mechanisms likely include in the endocardium and the valve apparatus,
interference with endothelial function, im- initially causing retraction and regurgitation
pairment of endothelial-myocardial coupling, and over time (>20 years) also stenosis, espe-
and capillary rarefaction.37 Indeed, mice with cially of the left-sided valves.57 Diffuse intersti-
cardiomyocyte-specific deletion of VEGF de- tial fibrosis as well as thickening and narrowing
velop hypovascular, nonnecrotic cardiac con- of arterioles and capillaries are characteristic
tractile dysfunction.49 changes in the myocardium.56 Capillary rare-
faction has also been noted, and injury to the
Radiation Therapy-Related Cardiotoxicity endothelium is considered an integral part of
Radiation therapy entails the use of high-energy radiation-induced heart disease. The theory
particles, x-rays, or g-rays that fragment cellular has been that microvascular insufficiency leads
DNA and thereby interfere with cell prolifera- to ischemia and cardiomyocyte death with
tion and viability. This affects cancer cells in replacement fibrosis; however, this has not
particular, given their high metabolic and pro- been substantiated by histological observa-
liferation index. The effect on normal cells tions.58,59 Instead, barrier breakdown of the
and tissues is related to their particular suscep- endothelium with microhemorrhage and aggra-
tibility and the extent of ionizing radiation vation of (radiation-induced) oxidative stress
exposure. For instance, radiation therapy to and inflammation seems to be an important
the chest can harm the cardiovascular system, pathomechanism.60 Furthermore, extravasation
and even more so if doses exceed 30 Gy.50 of albumin can lead to amyloid formation and
This had been the case with mantle field radia- predisposition to sudden cardiac death. These
tion and is still the case with involved field ra- recent observations add another dimension
diation therapy in patients with Hodgkin to the restrictive cardiomyopathy phenotype
lymphoma (up to a total dose of 20-35 Gy). observed after radiation therapy. They may
Doses for adjuvant radiation therapy in patients also have important implications for the early
with breast cancer can be even higher (in the detection of radiation-induced cardiotoxicity
n n
1292 Mayo Clin Proc. September 2014;89(9):1287-1306 http://dx.doi.org/10.1016/j.mayocp.2014.05.013
www.mayoclinicproceedings.orgCARDIO-ONCOLOGY
and the identification of patients at risk of malig- The following sections are devoted to discuss
nant cardiac arrhythmias.61 Conceivably, radia- the principles of practice of cardio-oncology
tion therapy may lead to more tissue fibrosis before, during, and after chemo- and/or radia-
and substrate for MRI.52,62 While diffuse fibrosis tion therapy (Figure 2).
might be present, focal (scar-like) fibrosis is rare
with anthracyclines.52,62,63 How the combina- Cardiovascular Evaluation of Patients Before
tion of anthracycline-based chemotherapy and and During Cancer Therapy
radiation therapy affects these aspects remains Before the initiation of cancer therapy, a thor-
to be defined. Alterations in cardiac function ough patient history and physical examination
and valve disease are most profound though should be performed to determine the baseline
with combined therapies.55,57 In contrast, the cardiovascular risk. Traditionally, there has
incidence of radiation-induced pericardial dis- been considerable variation in the use of adjunc-
ease is not increased by concomitant anthracy- tive tests such as ECG or echocardiography,
cline therapy and only limited, inconclusive directed mainly by the cardiotoxicity profile of
data are available for coronary artery disease the planned treatment regimen and individual
(CAD).57,58 practice styles. However, it is advisable to stan-
Given the sensitivity and vulnerability of dardize the assessment of patients with cancer
endothelial cells, it is not surprising that radiation and to stratify them in their cardiotoxicity risk
therapy induces and accelerates atheroscle- profile routinely. Such an approach allows for
rosis.64-66 A dose correlation has been noted a universal standard of care for all patients, facil-
and hence coronary artery segments with the itates communication across disciplines, and
highest degree of exposure are at greatest risk of aids in treatment decisions and follow-up plan-
disease. For mantle and even involved field radi- ning. Recent meta-analyses support operational
ation, this is the proximal left main and right cor- models that incorporate underlying patient-
onary artery.67,68 For left- and right-sided breast related risk factors.76 However, full assessment
cancer radiation, this is the mid left anterior should also include the cardiac toxicity potential
descending artery and proximal to mid right cor- of cancer therapies (as suggested in Figure 3) and
onary artery, respectively.69 Clinically, these the anticipated therapeutic benefit of the anti-
changes emerge after 15 years with an increase cancer regimen. Whether and which additional
in the incidence of myocardial infarction.55 An tests would further refine this risk assessment re-
intriguing aspect is that radiation therapy has a mains unanswered at present.
long-reaching effect despite a confined exposure Once patients have begun receiving treat-
period. This points to the induction of a smol- ment, it must be further decided which patients
dering process that continues after the initiating require cardiovascular follow-up. This depends
stimulus, and similar to the mechanisms dis- on the baseline cardiovascular risk profile, the
cussed for anthracycline-induced cardiomyopa- specific cancer treatment regimen, and the devel-
thy, this may be mitochondrial DNA damage opment of cardiac symptoms and/or events.
and perturbed mitochondrial function.70,71 Monitoring protocols were developed and
Another unique factor could be vasa vasorum validated for patients undergoing anthracycline-
compromise.33,72 DNA damage and activation based therapy in the 1970s and 1980s
of key proinflammatory pathways such as the nu- (Figure 4).77 These were based on radionucleo-
clear factor kB pathway has been pointed out for tide angiogram (ventriculogram) (RNA, also
traditional cardiovascular risk factors as well, known as multiple-gated acquisition or MUGA
which may explain why traditional cardiovascular scan), and the pivotal observation that a decrease
risk factors can affect the type and extent of in LVEF noted by this technique would precede
atherosclerosis after chest radiation.51,57,62,71,73-75 clinically overt heart failure.78,79 Importantly,
adhering to this protocol led to substantially bet-
PART 2: EVALUATION FOR CANCER ter clinical outcomes.80
THERAPYeINDUCED CARDIOTOXICITY Radionucleotide angiogram (ventriculo-
A multidisciplinary approach incorporating car- gram) is operator independent and highly
diology and oncology expertise is needed to reproducible but has been largely replaced
evaluate and manage short- and long-term ef- by echocardiography. Historically, change in
fects of cancer treatments enumerated above.7 LVEF by 2-dimenisonal (2D) transthoracic
Mayo Clin Proc. n September 2014;89(9):1287-1306 n http://dx.doi.org/10.1016/j.mayocp.2014.05.013 1293
www.mayoclinicproceedings.orgMAYO CLINIC PROCEEDINGS
Oncology/hematology patient
Before treatment During treatment After treatment
Cardiovascular review (incl. history, examination, CXR, ECG, and echocardiogram with strain)
Cardiovascular risk? Cardiovascular complications? Cardiovascular complications?
Cardiomyopathy (incl. abn strain) Decline in ejection fraction
Heart failure (incl. abn CXR) Myocardial strain abnormality
CAD or equivalent (incl. abn ECG) Any CV abnormality noted in f/u
Heart failure (incl. abn CXR)
HTN (esp. uncontrolled, end-organ signs) or
Pericardial effusion
Arrhythmias/syncope Doxorubicin ≥240 mg/m2
Cardiac biomarker elevation
QTc prolongation >500 ms
No No Radiation ≥30 Gy
Myocardial ischemia
Radiation + anthracycline or
For cardiotoxic drugs, esp. Arrhythmias
high-dose cyclophosphamide,
anthracyclines, QTc prolongation >500 ms
esp. if strenuous activity or
the following factors add to the risk: Syncope
pregnancy is planned
Age 65 years Hypotension
Female gender Uncontrolled hypertension
Yes Yes Yes
Cardio-oncology consultation Cardio-oncology consultation Cardio-oncology consultation
FIGURE 2. Outline of a general cardio-oncology algorithm. abn ¼ abnormal; CAD ¼ coronary artery
disease; CXR ¼ chest x-ray; CV ¼ cardiovascular; ECG ¼ electrocardiogram; f/u ¼ follow-up; HTN ¼
hypertension; QTc ¼ corrected QT.
echocardiography (TTE) has been reported as echocardiography has been used in multiple
high as 10%. However, LVEF assessment by independent studies, reporting changes in car-
contrast-enhanced 2D TTE or 3D TTE is su- diac (mechanical) function before a decrease in
perior in this regard and comparable to that LVEF and even before changes in diastolic
by RNA and cardiac MRI.81-84 As such, the al- function after chemotherapy.86-89 The degree
gorithms validated for RNA may be applied to of change in strain imaging is quite consistent
TTE imaging using these newer echocardio- across different laboratories and studies, and a
graphic techniques. Widespread availability, greater than 10% change in global longitudinal
feasibility, lack of radiation exposure, and strain after completion of anthracycline-based
acquisition of additional cardiac imaging in- chemotherapy relative to baseline is predictive
formation (valvular, pericardial, and hemody- of a future decrease in LVEF.86,90 Importantly,
namic data) make echocardiography an these (high-risk) changes can be noted in up to
attractive option for serial imaging, even 70% of the patients.86,90 Conceivably, but
though service fees might be higher. subject to further studies, abnormal strain
Of particular interest is strain imaging, values before cancer therapy may signal higher
which is a measure of regional deformation baseline risk for chemotherapy-induced
of the myocardium. It is currently mainly cardiotoxicity.
obtained by angle-independent 2D speckle Based on the above discussion, it seems
tracking echocardiography, which can appropriate to include strain imaging in moni-
evaluate all 3 domains of myocardial me- toring algorithms for cardiotoxicity. The dy-
chanics (longitudinal, circumferential, and namics after a cumulative dose of 200 mg/m2
radial) and derive data for deformation and of doxorubicin may be particularly instructive
rate of deformation for each myocardial and have been suggested to serve as a bench-
segment.85 Two-dimensional speckle tracking mark, with reassessment after each additional
n n
1294 Mayo Clin Proc. September 2014;89(9):1287-1306 http://dx.doi.org/10.1016/j.mayocp.2014.05.013
www.mayoclinicproceedings.orgCARDIO-ONCOLOGY
50 to 100 mg/m2 thereafter.42,91 After comple-
tion of therapy, reassessment is recommended 1. Risk assessment Tests: TTE with strain, EKG, cTn
at 6 and 12 months and as early as 3 months Medication-related risk Patient-related risk factors
for those at highest risk, for example, after
doxorubicin equivalent doses exceed 400 High (risk score 4): • Cardiomyopathy or heart failure
Anthracyclines, Cyclophosphamide,
mg/m2.42 The aforementioned observation of Ifosfamide, Clofarabine, Herceptin
• CAD or equivalent (incl. PAD)
• HTN
clinical outcome as a function of time to treat- Intermediate (risk score 2):
Docetaxel, Pertuzumab, • Diabetes mellitus
ment (Figure 1) would support expansion of Sunitinib, Sorafinib • Prior or concurrent anthracycline
these efforts to even earlier time points as Low (risk score 1):
• Prior or concurrent chest radiation
would the outlined data on strain imag- Bevacizumab, Dasatinib,
Imatinib, Lapatinib • Age 65 years
ing.42,86 Importantly, how well changes in Rare (risk score 0): • Female gender
these imaging parameters predict the develop- For example, Etoposide, Rituximab,
ment of clinical heart failure has not been Thalidomide
established. Also, how these algorithms Overall risk by Cardiotoxicity Risk Score (CRS)
should be modified for other drugs, for (risk categories by drug-related risk score plus number of patient-related risk factors:
CRS >6: very high, 5-6: high, 3-4: intermediate, 1-2: low, 0: very low)
instance, trastuzumab, remains to be defined.
Changes in strain values, however, have been 2. Monitoring recommendations
found to precede changes in LVEF by a mini-
mum of 3 months in this setting as well.88 Very high cardiotoxicity risk: TTE with strain before every (other) cycle, end, 3-6
months and 1 year, optional ECG, cTn with TTE during chemotherapy
One unique aspect of trastuzumab is the High cardiotoxicity risk: TTE with strain every 3 cycles, end, 3-6 months and 1 year
prolonged (1-year) treatment duration. Algo- after chemotherapy, optional ECG, cTn with TTE during chemotherapy
rithms are in place, with LVEF as a central Intermediate cardiotoxicity risk: TTE with strain, mid-term, end and 3-6 months after
chemotherapy, optional ECG, cTn mid-term of chemotherapy
evaluation parameter; there is no guidance yet Low cardiotoxicity risk: Optional TTE with strain and/or ECG, cTn at the end of chemotherapy
on how to interpret changes in strain imaging Very low cardiotoxicity risk: None
data over time (Figure 5). One may argue that
Applies as preventive measures before and
the recognition of abnormalities in these echo- 3. Management recommendations with abnormalities during/after chemotherapy
cardiographic parameters should prompt the
initiation of effective cardiac therapies with Very high cardiotoxicity risk: Initiate ACE-I/ARB, Carvedilol, and statins, starting at lowest dose
and start chemotherapy in 1 week from initiation to allow steady state, up-titrate as tolerated
continuation rather than suspension of cancer High cardiotoxicity risk: Initiate ACE-I/ARB, Carvedilol, and/or statins
therapy as long as LVEF is preserved and signs Intermediate cardiotoxicity risk: Discuss risk and benefit of medications
and symptoms of heart failure are absent. Low cardiotoxicity risk: None, monitoring only
Specific guidelines addressing the use of strain Very low cardiotoxicity risk: None, monitoring only
imaging in patients with cancer are to be
released by the American Society of Echocardi- FIGURE 3. Outline of a putative risk assessment, monitoring, and manage-
ography in the near future. The current (2012) ment model for patients undergoing chemotherapy. The central concept is
clinical practice guidelines by the European that patient- and medication-related risk factors can be used to generate an
Society for Medical Oncology are summarized overall risk score that can then be used to determine monitoring intervals and
in Supplemental Tables 3 and 4 (available on- thresholds for preventive strategies. Such models need to be accounted for
line at http://www.mayoclinicproceedings. the fact that not all chemotherapeutic agents and patient-related risk factors
weigh the same, and hence the ultimate prediction models will need to be
org).27
more stratified and will need to be verified. ACE-I ¼ angiotensin-converting
Regarding the use of circulatory bio-
enzyme inhibitor; ARB ¼ angiotensin receptor blocker; CAD ¼ coronary
markers, only cardiac troponin (cTn) has stood artery disease; cTn ¼ cardiac troponin; ECG ¼ electrocardiogram; HTN ¼
the test of time whereas brain natriuretic pep- hypertension; PAD ¼ peripheral arterial disease; TTE ¼ transthoracic
tides and C-reactive protein have not and echocardiography.
emerging data on myeloperoxidase are yet to
be confirmed.86,92,93 The replacement, additive,
or synergistic role of cTn in the outlined moni- with strain imaging.86,94 With trastuzumab,
toring algorithms also requires further investi- new cTn elevation is mainly seen with the first
gation. With anthracycline-based protocols, or second cycle and only early and persistent el-
cTn serum concentrations increase during and evations seem to carry the greatest prognostic
early after completion of chemotherapy but weight.95 These data are intriguing if trastuzu-
their predictive value for a future decrease in mab is to lead only to myocardial dysfunction
LV function is not superior to that obtained and not myocardial injury.
Mayo Clin Proc. n September 2014;89(9):1287-1306 n http://dx.doi.org/10.1016/j.mayocp.2014.05.013 1295
www.mayoclinicproceedings.orgMAYO CLINIC PROCEEDINGS
Cardiovascular Evaluation of Patients After is typically for a duration of 12 months). The
Cancer Therapy need for posttreatment cardiovascular follow-
After completion of cancer therapy, follow-up up is hence confined to only those patients
recommendations are to be individualized ac- who have ongoing cardiovascular disease pro-
cording to the overall survival prognosis of the cesses or are at risk of late cardiotoxicity.
underlying malignancy, the specific anticancer Patients with breast cancer and lymphoma
therapy administered, each patient’s unique who have undergone anthracycline-based ther-
cardiovascular risk and comorbidity profile, apy and patients who have had mediastinal radi-
and whether they suffered adverse cardiac ef- ation therapy are prime candidates for long-term
fects during therapy. Goals of management cardiac surveillance programs (ideally integrated
should be explained and managed together into cancer survivorship programs). A recently
with other subspecialists involved in the can- published expert consensus statement from
cer care of the patient. the European Association of Cardiovascular Im-
Serial, long-term postexposure cardiac sur- aging and the American Society of Echocardiog-
veillance does not pertain to drugs that are asso- raphy recommends evaluation based on signs
ciated with acute but not chronic injury patterns and symptoms and echocardiographic surveil-
in the absence of any persistence of complica- lance starting 5 years after treatment in high-
tions after completion of therapy. One example risk patients and 10 years in all other patients.
is cyclophosphamide, and even if acute cardio- High-risk patients should also receive a func-
toxicity were to occur, ongoing follow-up would tional noninvasive stress test within 5 to 10
not be necessary after recovery. Similarly, cardi- years of completion of chest radiation therapy
otoxicity has not been reported to develop late (Figure 6).96
after completion of trastuzumab therapy, and Intriguingly, even in the highest-risk group
hence there is no need to continue with cardiac of patients with Hodgkin lymphoma who
monitoring after completion of therapy (which received 35 Gy or more of radiation to the chest,
treadmill exercise ECGs do not reflect the
burden of CAD.97 Moreover, stress echocardiog-
Initial evaluation
raphy and nuclear stress test can be quite discor-
dant in their resultsdthe former being more
sensitive to abnormalities at rest and the latter
LVEF >50% LVEFCARDIO-ONCOLOGY
to those without significant coronary calcifica-
tions.100 Combination with perfusion imaging Initial evaluation
may help overcome these limitations and in-
creases the yield of coronary computed tomogra-
LVEF ≥50% LVEFMAYO CLINIC PROCEEDINGS
Baseline pre-radiation
comprehensive Chest radiation exposure
echocardiography
Yearly targeted clinical history and
physical examination
New murmur Echocardiography
Screen for modifiable Search for signs and symptoms suggestive of
risk factors CMR if suspicion
• Pericardial effusion/constriction Signs/symptoms
of pericardial
• Valvular heart disease of heart failure
constriction
• LV dysfunction/heart failure
• Coronary artery disease
• Carotid artery disease Angina
• Conduction system disease
Neurological
Carotid US
signs/symptoms
Correct risk factors Asymptomatic
Screening echocardiography 5 years Functional noninvasive stress test for
after exposure in high-risk patients CAD detection (5-10 years after
10 years after exposure in the others exposure in high-risk patients)
Reassess every 5 years
FIGURE 6. Monitoring algorithm of patients after radiation therapy. CAD ¼ coronary artery disease;
CMR ¼ cardiac magnetic resonance; LV ¼ left ventricular; US ¼ ultrasound. From Lancellotti et al, 96 with
permission.
response rate (Figure 1).25 These observations agents that cause type 2 cardiotoxicity. Initial
substantiate the paradigm shift to the early detec- studies on trastuzumab-associated cardiomyopa-
tion and early treatment of chemotherapy- thy reported improved cardiac function after
induced cardiotoxicity. withholding therapy alone.114 This has remained
Hemodynamic device support may become the primary approach common to all published
necessary if medical therapy fails. Acute hemo- management algorithms for trastuzumab-
dynamic support can be temporarily lifesaving associated cardiotoxicity. However, HER-2 inhi-
as in those with acute myopericarditis owing to bition is a vital element in the treatment of
cyclophosphamide.39,107 Alternatively, chronic patients with breast cancer overexpressing
left ventricular assist device support may this receptor, and thus “drug holiday” is of
become a bridge to transplant or destination concern.115-117 It is currently undefined whether
therapy as reported recently.108,109 One unique institution of cardioactive medication is neces-
aspect is the relatively high rate of biventricular sary and would allow continuation of therapy
failure in these patients compared with those without concerns for cardiac adverse effects. As
receiving left ventricular assist device therapy the Akt/PKB signaling pathway is one of the
for other indications.108 The most severe forms key pathways affected by HER-2/ErbB2 signaling
of heart failure are usually observed in patients and is involved in trastuzumab-associated cardi-
receiving both chemotherapy and radiation otoxicity, up-regulation of this pathway in the
therapy because of the profound injury and in heart may be of merit. Intriguingly, statins and
those of young age.110,111 Two key processes nebivolol induce potent up-regulation of this
have been noted in children developing cardio- pathway.118,119 Whether such strategies would
toxicity: reduction in contractility and/or in- be counterproductive to the anticancer effects
crease in afterload. These have not been of therapy, however, remains an unanswered
described in adults but may be of significance question.
for the choice of therapy.111-113 The treatment of patients with radiation-
At present, it is unknown whether the med- induced heart disease is challenged by the mul-
ical therapies outlined above are necessary for tiplicity of processes and the high propensity for
n n
1298 Mayo Clin Proc. September 2014;89(9):1287-1306 http://dx.doi.org/10.1016/j.mayocp.2014.05.013
www.mayoclinicproceedings.orgCARDIO-ONCOLOGY
surgical intervention over time. One aspect often much symptom relief. Thus, hemodynamic
not considered is the fact that radiation therapy catheterization is advised to differentiate be-
to the chest increases the level of complexity for tween a primarily constrictive or restrictive pro-
open heart operation and risk of complica- cess. Cardiac MRI might help to define the
tions.54 The internal mammary artery (IMA) is burden of cardiac fibrosis, especially in those
often not a prime bypass conduit in these pa- with equivocal hemodynamic findings. It can
tients owing to radiation damage. Furthermore, also outline the pericardium, but in most cases
radiation-induced left subclavian artery disease there is no inflammation and these patients do
may cause both a traditional steal phenomenon not benefit from anti-inflammatory therapy.
and flow limitation to the left IMA. Aortic calci- A high level of clinical suspicion for
fication may pose significant challenges to aorto- arrhythmia needs to be maintained in patients
coronary (saphenous and arterial) bypasses. after radiation therapy to the chest because
Assessment of the ascending aorta, aortic arch, interstitial fibrosis may lead to ventricular
and IMAs is recommended if these patients are tachycardias and degeneration of the conduc-
considered for coronary artery bypass grafting.50 tion system may cause bradyarrhythmias.2,57
Given the surgical challenges in these patients, Calcification of the aortomitral ridge is a char-
percutaneous coronary intervention might be acteristic clue for those at risk of heart block.121
preferred over coronary artery bypass grafting Treatment of these ultimate complications
whenever possible.2 A “heart team” approach should be in keeping with current guidelines.
should be pursued, and a comprehensive risk
and benefit assessment should be made. As PART 4: PREVENTION OF CANCER
with patients with CAD in general, medical ther- THERAPYeINDUCED CARDIOTOXICITY
apy remains the cornerstone of treatment. How- The poor prognosis of cancer therapyeinduced
ever, experimental data indicate that although heart disease and the lack of a universal response
radiation induces an inflammatory and throm- to the institution of therapy argue for a preven-
botic phenotype, conventionally used drugs tive approach. This has to be based on the
such as statins and clopidogrel are not effective, premise that the perceived benefit is greater
though clopidogrel seems more favorable.120 than the perceived risk in terms of both adverse
Similarly, neither aspirin nor the newer nitric effects and reduction of the anticancer effects.
oxideedonating aspirin reduces the amount of Ideally, these approaches should be supported
plaque development in radiation-induced by prospective randomized trials that also define
atherosclerosis despite efficacy for age-related target subsets of patients at varying levels of risk.
atherosclerosis.120 This has been the case for dexrazoxane, the
Another important consideration is that drug with the best level of evidence for the preven-
these patients may require more than 1 open tion of chemotherapy-induced cardiotoxicity. In a
heart surgery (eg, bypass surgery and valve meta-analysis of 8 trials with more than 1500 pa-
replacement). Postradiation mediastinal fibrosis tients, dexrazoxane reduced the incidence of clin-
poses a challenge at baseline and limits the num- ical heart failure by more than 80% (relative risk,
ber of redo surgeries. It is therefore advisable, if 0.18; 95% CI, 0.10-0.32; PMAYO CLINIC PROCEEDINGS
retrospective evidence for b-blockers and sta- the prevention of LVEF reduction at 6 months
tins but remain limited in therapy details.123,124 and even outlined a benefit in terms of the
This is important as experimental studies have combined secondary end point of death or
found that not all b-blockers provide cardio- heart failure.130 No interaction was observed
protection from chemotherapy-induced cardi- in terms of the primary end point and cTnI
otoxicity. Nonselective b-blockers such as or brain natriuretic peptide elevation; howev-
propranolol may, in fact, potentiate cardiotox- er, LVEF benefits remained largely confined
icity, likely related to inhibition of b-2 activ- to patients with acute leukemia.130 This obser-
ity.136,137 In contrast, b-blockers with proven vation thus supports the limitation of preven-
evidence for cardioprotection in this setting tive strategies to those patients at highest
include carvedilol and nebivolol whereas the presumed risk of cardiotoxicity on the basis
effect of metoprolol appears neutral.125-129 of treatment-related and patient-related factors
In contrast to experimental data, randomized as outlined in the beginning (Figure 3). This is
clinical trial data supporting the use of statins in keeping with the European Society for Med-
remain scarce with only one reported so far.135 ical Oncology guidelines (see Supplemental
In keeping with the reported benefit in the treat- Table 3), which recommend ACE inhibitors
ment of patients with chemotherapy-induced as first-line agents; however, as outlined above
heart failure, ACE inhibitors have been the first and summarized in Table 2, carvedilol, nebi-
ones tested and contended. The ACE inhibitor Af- volol, and statins should be considered as
ter Anthracycline study in survivors of pediatric well.27 Obviously, patients already receiving
cancer did not find any significant long-term these therapies should continue with them.
benefit.131 However, the qualifying enrollment The exception, however, as implied, is that ef-
criteria included a broad spectrum of cardiac ab- forts should be made to switch patients from
normalities and treatment was not commenced b-blockers other than carvedilol and nebivolol
until at least 2 years after discontinuing anthracy- to these specific agents, given their evidence-
cline therapy.131 Still, a prospective randomized based level of benefit for the prevention of
controlled study comparing monotherapy with chemotherapy-induced cardiomyopathy.
enalapril or metoprolol to placebo in patients un-
dergoing adriamycin, bleomycin, vinblastine, and
CONCLUSION
dacarbazine or rituximab-cyclophosphamide,
Advances in cancer therapy and the outcome
doxorubicin, vincristine, and prednisone therapy
limiting effect of cardiovascular adverse effects
for Hodgkin or non-Hodgkin lymphoma,
have generated a growing need for cardio-
respectively, did not find any benefit in the pre-
oncology. With this, the paradigm has shifted
vention of clinical or subclinical cardiotoxic-
toward early recognition and treatment of car-
ity.129 At the other end of the spectrum,
diotoxicity and even pre-cancer therapy car-
confined only to those with cTnI elevation
diovascular risk assessment and prevention.
within 3 days of initiation of high-dose chemo-
The key practical steps in the cardio-
therapy, initiation of enalapril therapy was of
oncology approach outlined in this review
remarkable benefit.132 The surveillance intensity
comprise the following:
of such a protocol, however, may pose a barrier
for general use, even though it underscores the Step 1: Ongoing interaction between cardiolo-
merit of defining a high riskehigh yield patient gists, oncologists or hematologists, and
population. general practitioners in a “cardio-
With regard to combination therapies, the oncology team” approach, ideally with
preventiOn of left Ventricular dysfunction the development of “cardio-oncology
with Enalapril and caRvedilol in patients sub- clinics” staffed by dedicated specialists.
mitted to intensive ChemOtherapy for the These efforts should be linked to and
treatment of Malignant hEmopathies (OVER- even start with evaluation efforts of po-
COME) trial was conducted with universal tential cardiotoxic adverse effects of
consideration of enalapril and carvedilol for chemotherapeutic agents.
all patients referred for intensive chemo- Step 2: Clinical screening of patients with
therapy or stem cell transplant.130 The study cancer for underlying or developing
remained positive in its primary end point of cardiovascular disease, followed by
n n
1300 Mayo Clin Proc. September 2014;89(9):1287-1306 http://dx.doi.org/10.1016/j.mayocp.2014.05.013
www.mayoclinicproceedings.orgTABLE 2. Adjunctive Pharmacological Strategies for the Prevention of Chemotherapy-Induced Cardiotoxicitya
Cardiotoxic Radiation Cardiotoxicity Outcome with vs without
Study Year Cohort F/u time chemotherapy therapy Preventive therapy definition previous therapy
Observational studies
Seicean et al,123 2012 Breast cancer 2.61.7 y Anthracyclines 66% Any statin therapy during CT Rate of new HF 6.0 vs 17.2b (HR, 0.3; 95%
2012 (n¼628) admission (%) CI, 0.1-0.9)
Seicean et al,124 2013 Breast cancer 32 y Anthracyclines and/or 59% Any BB therapy during CT Rate of new HF 4.7 vs 12.7b (HR, 0.2; 95%
CARDIO-ONCOLOGY
2013 (n¼318) Herceptin admission (%) CI, 0.1-0.7)
www.mayoclinicproceedings.org
Randomized controlled trials
Kalay et al,125 2006 Breast cancer (68%), 6 mo Anthracyclines: 0% Carvedilol 12.5 mg/d, LVEF (%) Carvedilol: no change;
2006 lymphoma (18%) doxorubicin 520 administered before CT and Control: significant
mg/m2 or epirubicin continued for 6 mo decrease (68.9-52.3b)
780 mg/m2
Mayo Clin Proc. n September 2014;89(9):1287-1306
El-Shitany 2012 Children with ALL 1 wk after Doxorubicin 0% Carvedilol 0.1-1 mg/d, FS (%) 39.56.3 vs 33.56.2b
n
et al,126 2012 (n¼50) CT 120 mg/m2 administered 5 d before CT GPSS (%) 19.32.0 vs 15.11.8b
cTnI (ng/mL) 0.020.02 vs 0.060.05b
Elitok et al,127 2013 Breast cancer 6 mo Anthracyclines 0% Carvedilol 12.5 mg/d, Peak systolic strain, septal (%) 205.3 vs 164.3b
2013 (n¼80) 520 mg/m2 administered before CT and Peak systolic strain, lateral (%) 185.6 vs 146.1b
continued for 6 mo LVEF (%) 645.1 vs 634.8
Kaya et al,128 2013 Breast cancer 6 mo Anthracyclines: 27% Nebivolol 5 mg/d, administered LVEF (%) 63.83.9 vs 57.55.6b
2012 (n¼45) doxorubicin 7 d before CT and NT-proBNP (pmol/L) 15269 vs 20473b
246 mg/m2 or continued for 6 mo
epirubicin
354 mg/m2
Georgakopoulos 2010 HL and NHL 12 mo ABVD 21% Metoprolol 25-50 mg BID or New HF rate (%) 2.4 or 4.7 vs 0 (P¼.56)
et al,129 2010 (n¼125) 30 mo R-CHOP enalapril
2.5-10 mg BID, administered
http://dx.doi.org/10.1016/j.mayocp.2014.05.013
with CT
Bosch et al 2013 Acute leukemia 6 mo Anthracyclines 18% Carvedilol (6.25-25 mg BID) and LVEF (%), absolute change by 0.17 vs 3.28b
(OVER- (n¼36) or HSCT (40% before, 40% enalapril (2.5-10 mg BID), TTE
COME (n¼54) during, cumulative administered 24 h before CT LVEF (%), absolute change by 0.36 vs 3.04 (P¼.09)
trial),130 2013 265 mg/m2) and continued in f/u CMR imaging
Silber et al 2004 Pediatric cancer 35 mo Anthracyclines 36% Enalapril 0.05-0.15 FS (%) Interaction term (change due
(AAA survivors with 300 mg/m2 mg/kg per d to treatment) P¼.84
study),131 1 cardiac LVESWS (g/cm2) Interaction term (change due
2004 abnormalities in to treatment) P¼.28
f/u (n¼135) MCI (L/min per m2) Interaction term (change due
to treatment) P¼.55
Cardinale 2006 HDC (n¼114, 60% 12 mo Various, cumulative 11% Enalapril 2-20 mg/d, administered LVEF decrease >10% to 0 vs 43b
et al,132 2006 NHL and breast doxorubicin after cTnI elevation and ULN within 3 d 335 mg/m2 Arrhythmia rate (%) 2 vs 17b
of any cycle
Continued on next page
1301You can also read