Evaluation and Management
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Evaluation and Management

My Background
• My connection to coding and documentation
• My connection to clinical processes
• My connection to ICD-10
• My connection to YOU
Coding & Compliance Initiatives, Inc. 2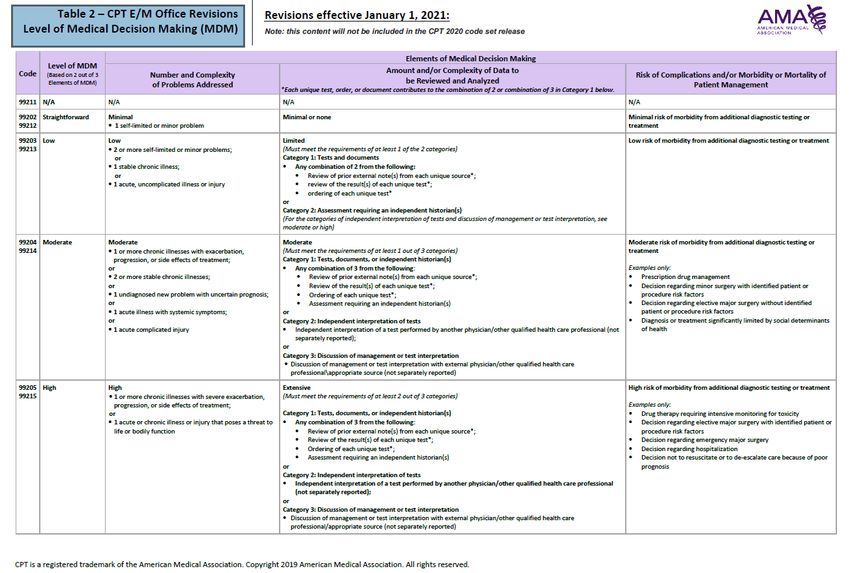
Disclaimer
The information provided within this presentation is for
educational purposes only and is not intended to be
considered legal advice. Opinions and commentary are
solely the opinion of the speaker. Many variables affect
coding decisions and any response to the limited
information provided in a question is intended to provide
general information only. All coding must be considered on
a case-by-case basis and must be supported by appropriate
documentation, medical necessity, hospital bylaws, state
regulations, etc. The CPT codes that are utilized in coding
are produced and copyrighted by the American Medical
Association (AMA).
Coding & Compliance Initiatives, Inc. 3
Agenda
• We will discuss some updates from 2019
• We will discuss the up coming E/M changes for
coding and documentation
• We will discuss Medicare preventive services
Coding & Compliance Initiatives, Inc. 4
Updates Coding & Compliance Initiatives, Inc. 5
2019 Updates
• HPI elements as well as the ROS elements can be
obtained by someone other than the billing provider.
• Train you Medical Assistants on how to obtain and
document an HPI, PERTINENT ROS and PFSH
• Check with your private contracted payers to see if they
will follow the same changes.
Coding & Compliance Initiatives, Inc. 62019 Updates
• Documentation guidelines for teaching physicians
• CMS eliminated its requirement that teaching physicians
personally document the extent of their participation in the
review and direction of services furnished to each patient.
The participation of teaching physicians in the provision of
E/M services and procedures may be demonstrated by
notes that residents, nurses, or other ancillary staff make in
the medical record. Teaching physicians still will be
responsible for verifying the accuracy of such notes, along
with further documenting their participation in the medical
record if the notes that other health care professionals
make inaccurately demonstrate the physician’s involvement
in the provision of the service.
Coding & Compliance Initiatives, Inc. 7Student Documentation
• Students may document services in the medical record.
The teaching physician must verify in the medical
record all student documentation or findings, including
history, physical exam and/or medical decision making.
• The teaching physician must personally perform (or re-
perform) the physical exam and medical decision-
making activities of the E/M service being billed, but
may verify any student documentation of them in the
medical record, rather than re-documenting this work.
Coding & Compliance Initiatives, Inc. 82019 Updates
• Effective January 1, 2019, FQHCs can receive payment for Virtual
Communication services when at least 5 minutes of communication
technology-based or remote evaluation services are furnished by an
FQHC practitioner to a patient who has had an FQHC billable visit within
the previous year, and both of the following requirements are met:
• The medical discussion or remote evaluation is for a condition not
related to an FQHC service provided within the previous 7 days, and
• The medical discussion or remote evaluation does not lead to an FQHC
visit within the next 24 hours or at the soonest available appointment.
• To receive payment for Virtual Communication services, FQHCs must
submit an FQHC claim with HCPCS code G0071 (Virtual Communication
Services) either alone or with other payable services.
• RHC face-to-face requirements are waived when these services are
furnished to an FQHC patient, and coinsurance applies.
Coding & Compliance Initiatives, Inc. 92021 Changes
• Providers will have the flexibility on documentation
for the visits – current framework, medical
decision-making or time.
• For levels 2 through 5, when using the MDM or
current framework CMS will apply a minimum
supporting documentation standard associated
with level 2 visits.
• What about private payors or secondary insurance?
Coding & Compliance Initiatives, Inc. 102021 Changes Summary - AMA
• Removing history and exam as key components
• Must have a medically appropriate history and/or exam
• Making the basis for code selection either the level
of medical decision-making performed OR the total
time spent performing the service on the day of the
encounter
• Changing the definition of the time element
associated with codes 99202-99215 from typical
face-to-face time to total time spent on the day of
the encounter, and changing the amount of time
associated with each code
Coding & Compliance Initiatives, Inc. 11AMA Summary of History and/or
Exam
• Office or other outpatient services include a
medically appropriate history and/or physical
examination, when performed.
• The nature and extent of the history and/or
physical examination is determined by the treating
physician or other qualified health care professional
reporting the service.
Coding & Compliance Initiatives, Inc. 12AMA Summary of History and/or
Exam
• The care team may collect information and the
patient or caregiver may supply information
directly (eg, by portal or questionnaire) that is
reviewed by the reporting physician or other
qualified health care professional.
• The extent of history and physical examination is
not an element in selection of office or other
outpatient services.
Coding & Compliance Initiatives, Inc. 13AMA Summary of Assessment and Plan
• One element in the level of code selection for an
office or other outpatient service is the number
and complexity of the problems that are addressed
at an encounter.
• Multiple new or established conditions may be
addressed at the same time and may affect medical
decision making.
• Symptoms may cluster around a specific diagnosis
and each symptom is not necessarily a unique
condition.
Coding & Compliance Initiatives, Inc. 14AMA Summary of Assessment and
Plan
• Comorbidities/underlying diseases, in and of
themselves, are not considered in selecting a level
of E/M services unless they are addressed, and
their presence increases the amount and/or
complexity of data to be reviewed and analyzed or
the risk of complications and/or morbidity or
mortality of patient management.
Coding & Compliance Initiatives, Inc. 15AMA Summary of Assessment and
Plan
• The final diagnosis for a condition does not in itself
determine the complexity or risk, as extensive
evaluation may be required to reach the conclusion
that the signs or symptoms do not represent a
highly morbid condition.
• So, in other words – you get paid for the work (this
statement is not from the AMA)
• Multiple problems of a lower severity may, in the
aggregate, create higher risk due to interaction.
Coding & Compliance Initiatives, Inc. 16AMA
• Problem addressed: A problem is addressed or managed
when it is evaluated or treated at the encounter by the
physician or other qualified health care professional reporting
the service.
• This includes consideration of further testing or treatment
that may not be elected by virtue of risk/benefit analysis
or patient/parent/guardian/surrogate choice.
• Notation in the patient’s medical record that another
professional is managing the problem without additional
assessment or care coordination documented does not
qualify as being ‘addressed’ or managed by the physician
or other qualified health care professional reporting the
service.
• Referral without evaluation (by history, exam, or diagnostic
study[ies]) or consideration of treatment does not qualify
as being addressed or managed by the physician or other
qualified health care professional reporting the service.
Coding & Compliance Initiatives, Inc. 17AMA
• Minimal Problem
• Self-limited or minor problem
• Stable Chronic Illness
• Chronic illness with exacerbation,
progression, or side effects of treatment
Coding & Compliance Initiatives, Inc. 18AMA
• Acute, uncomplicated illness or injury
• Acute, complicated injury
• Undiagnosed new problem with uncertain
prognosis:
• Acute or chronic illness or injury that poses a
threat to life or bodily function
Coding & Compliance Initiatives, Inc. 19Medical Decision-Making Table
2020 2021
Number and Complexity of
Number of Diagnoses or Problems Addressed at the
Management Options Encounter
Amount and/or Complexity of
Amount and/or Complexity of Data to be Reviewed and
Data to be Reviewed Analyzed
Risk of Complications and/or
Risk of Complications and/or Morbidity or Mortality of Patient
Morbidity or Mortality Management
Coding & Compliance Initiatives, Inc. 20Coding & Compliance Initiatives, Inc. 21
Examples
These are just examples to think about
Coding & Compliance Initiatives, Inc. 22Straightforward Medical Decision-
Making
• Patient presents after being on antibiotic for otitis –
doing well and infection is gone
• Patient presents with “feared” complaint
• Patient presents skin redness – you determine it is a
“sunburn”
• Patient presents with ankle pain – rest and elevate
Coding & Compliance Initiatives, Inc. 23Low Medical Decision-Making
• Patient presents with well controlled hypertension-
refilled meds
• Patient presents with sinusitis – treated with
antibiotic
• Patient presents with elbow pain – evaluated and
treated with NSAID
Coding & Compliance Initiatives, Inc. 24Moderate Medical Decision-
Making
• Patient presents to follow-up on HTN, DM and
Hyperlipidemia – refilled meds for all 3
• Patient presents with right lower quadrant pain
working up for appendicitis
• Patient presents with moderate to severe headaches
and your working up
• Diabetic patient presents with vision difficulties and
noncompliance
Coding & Compliance Initiatives, Inc. 25High Medical Decision-Making
• Patient presents with fatigue, weight loss,
intermittent fever, and presenting with diffuse
adenopathy and splenomegaly
• Patient presents with history of increasing
confusion, agitation and short-term memory loss
• Patient presents who is status post-transplant, with
new onset of peripheral edema, increased blood
pressure, and progressive fatigue
Coding & Compliance Initiatives, Inc. 262021 - Coding on Time
E/M Code Current “Typical” Time 2021 Time
99201 10 minutes Deleted Code
99202 20 minutes 15-29 minutes
99203 30 minutes 30-44 minutes
99204 45 minutes 45-59 minutes
99205 60 minutes 60-74 minutes
99211 5 minutes No time listed
99212 10 minutes 10-19 minutes
99213 15 minutes 20-29 minutes
99214 25 minutes 30-39 minutes
99215 40 minutes 40-54 minutes
Coding & Compliance Initiatives, Inc. 27Category Definition 2019 2021
CC/Reason for The reason for the Required Required
visit encounter
History of Present Symptoms describing the Staff may Document pertinent HPI as
Illness nature and severity of the document, medically indicated. This will no
patient’s presenting however, provider longer be counted for coding
problem(s) is responsible for purposes. The documentation
verifying and must support the necessity of
updating if the encounter.
needed.
Review of Systems Describes how pertinent Staff or patients Pertinent ROS should be
systems are impacted by may document documented to describe the
the presenting problem this information. complexity of the condition(s).
Provider must This will no longer be counted
review and verify. for coding purposes.
Past, Family, and Indicates areas of Staff or patients PFSH should be documented to
Social History concern within the may document describe any pertinent
patients PFSH that could this information. information that impacts care
impact the current Provider must and decision-making. This will
problem. review and verify. no longer be counted for coding
purposes.
Coding & Compliance Initiatives, Inc. 28Category Definition 2019 2021
Exam Quantifies the hands-on Providers are only Medically appropriate exam as
work performed by the required to determined by the provider.
provider. document interval This will no longer be counted
changes. Must for coding purposes. This could
meet the required still impact the level of service
elements for supposed based upon the
coding. necessity of the exam
documented.
Assessment (i.e. Credits the provider for Providers must Only diagnoses documented as
diagnosis and/or each diagnosis being document a final active treatment during the
sign(s)/symptom(s) treated during the diagnosis or encounter will be given credit.
current encounter. It also sign(s)/symptom(s) Additional work-up Is not listed
provides credit for in the table of risk. It will be
underlying conditions important to describe in detail
that impact the decision- the symptoms, differentials,
making. etc.
Data and The amount of work Providers receive Most of the elements are now
Complexity performed to obtain “points” based incorporated in the risk table.
and/or analyze data (i.e. upon the data “points” will no longer be
diagnostic results). ordered, reviewed, counted for coding purposes.
etc.
Coding & Compliance Initiatives, Inc. 29Category Definition 2019 2021
Table of Risk The highest level of risk The medical The table of risk has been
of mortality and/or decision-making revised. For the purposes of
morbidity posed by the component is medical decision making, level
presenting problem(s), based upon the of risk is based upon
ordered tests or diagnoses, data consequences of the
interventions. ordered/reviewed problem(s) addressed at the
and overall risk. encounter when appropriately
treated. Risk also includes
medical decision making
related to the need to initiate
or forego further testing,
treatment and/or
hospitalization.
Time The use of face time When the majority There is not a requirement that
spent with the patient as of a face-to-face the majority of the visit must
the determining factor in visit (in the clinic) is be counseling and coordination
selecting an E/M level. spent in counseling of care. Also, the time spent
and coordination of will include the rendering
care provider can providers TOTAL time spent on
report the E/M the DAY of the encounter,
service on time in including NON face-to-fact time
lieu of the key spent on the specific encounter
components. for the patient.
Coding & Compliance Initiatives, Inc. 30AMA
• Medical decision-making table:
• https://www.ama-assn.org/system/files/2019-06/cpt-
revised-mdm-grid.pdf
• E/M Code and Guideline Changes
• https://www.ama-assn.org/system/files/2019-06/cpt-
office-prolonged-svs-code-changes.pdf
Coding & Compliance Initiatives, Inc. 31ICD-10
• How does ICD-10 affect Medical
Necessity and complexity or does it?
Coding & Compliance Initiatives, Inc. 32Implementing the Changes
• What steps do you need to take?
Coding & Compliance Initiatives, Inc. 33Summary
• Clinicians may use either time or medical decision making to
select a code.
• There will be no required level of history or exam for visits
99202—99215.
• Time will be defined as total time spent, including non-face-
to-face work done on that day, and will no longer require
time to be dominated by counseling. The time will be a
range of time.
Coding & Compliance Initiatives, Inc. 34Summary
• There will be new definitions within MDM.
• The MDM calculation will be similar, but not identical to, the
current MDM calculation.
• CPT® is providing numerous definitions to clarify terms in the
current guidelines, such as “chronic illness with
exacerbation, progression or side effects of treatment,” and
“drug therapy requiring intensive monitoring for toxicity.”
Coding & Compliance Initiatives, Inc. 35Medicare Preventive
Services
Medicare Benefits Policy Manual – Chapter 13
Coding & Compliance Initiatives, Inc. 36Qualifying Codes for G0468 (IPPE
or AWV)
• G0402 Initial preventive exam
• G0438 AWV, initial visit
• G0439 AWV, subsequent visit
Coding & Compliance Initiatives, Inc. 37New Patient - Payment Adjustment
• New Patient, Annual Wellness Visit (AWV) and
Initial Preventive Physical Exam (IPPE) Adjustments
• Payment rate will be increased by 1.3416 (i.e. 34%) for
new patients, IPPE, initial and subsequent AWVs
• New patient –someone who has not received any
Medicare covered services from any site or any
provider within the FQHC organization
Coding & Compliance Initiatives, Inc. 38Preventive Services
• FQHCs must provide preventive health services on
site or by arrangement with another provider.
• These services must be furnished by or under the
direct supervision of a physician, NP, PA, CNM, CP,
or CSW.
• Section 330(b)(1)(A)(i)(III) of the Public Health
Service (PHS) Act required preventive health
services can be found at
http://bphc.hrsa.gov/policiesregulations/legislation
/index.html
Coding & Compliance Initiatives, Inc. 39Preventive Services
• Examples:
• prenatal and perinatal services;
• appropriate cancer screening;
• well-child services;
• immunizations against vaccine-preventable diseases;
• screenings for elevated blood lead levels, communicable
diseases, and cholesterol;
• pediatric eye, ear, and dental screenings to determine
the need for vision and hearing correction and dental
care;
• voluntary family planning services; and
• preventive dental services
Coding & Compliance Initiatives, Inc. 40Preventive Services
• Examples:
• Cardiovascular screening blood test
• Diabetes screening test
• Screening mammography
• Screening pap smears
• Screening pelvic exam (can include clinical breast
exam)
• Prostate cancer screening
• Colorectal cancer screening tests
Coding & Compliance Initiatives, Inc. 41Coding & Compliance Initiatives, Inc. 42
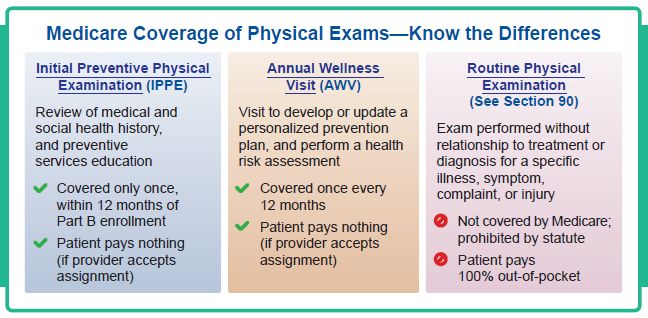
Preventive Services
Coding & Compliance Initiatives, Inc. 43Preventive Services
Coding & Compliance Initiatives, Inc. 44Coding & Compliance Initiatives, Inc. 45
Coding & Compliance Initiatives, Inc. 46
Preventive Services
Coding & Compliance Initiatives, Inc. 47IPPE/Welcome to Medicare
• Beneficiary has no more than 12 months from
effective Part B coverage for exam
• Co-insurance is waived
• Revenue code 0521
• HCPCS code G0402
Coding & Compliance Initiatives, Inc. 48IPPE/Welcome to Medicare
• Services include:
• Patient history (height, weight, and blood pressure at a
minimum)
• Visual acuity screen – this is one we see missed
• Measurement of body mass index
• Other factors deemed appropriate based on the
individual’s medical and social history and current
clinical standards
• Depression risk assessment –
• To obtain current or past experiences with depression or
other mood disorders, use any appropriate screening
instrument for beneficiaries without a current diagnosis
of depression from various available standardized
screening tests recognized by national professional
medical organizations..
Coding & Compliance Initiatives, Inc. 49IPPE/Welcome to Medicare
• Review the beneficiary’s functional ability and
level of safety
• Use appropriate screening questions or standardized
questionnaires recognized by national professional
medical organizations to review, at a minimum, the
following areas:
• Activities of daily living
• Fall risk
• Hearing impairment
• Home safety
Coding & Compliance Initiatives, Inc. 50IPPE/Welcome to Medicare
• End-of-life planning (verbal or written
information provided to the beneficiary about):
• The beneficiary’s ability to prepare an advance directive in
case an injury or illness causes the beneficiary to be unable to
make health care decisions
• Whether or not you are willing to follow the beneficiary’s
wishes as expressed in an advance directive
• Based on the results of the review and
evaluation services in the previous components,
provide education, counseling, and referral as
appropriate.
Coding & Compliance Initiatives, Inc. 51IPPE/Welcome to Medicare
• Educate, counsel, and refer for other
preventive services
• Includes a brief written plan, such as a
checklist, for the beneficiary to obtain:
• A once-in-a-lifetime screening electrocardiogram
(EKG/ECG), as appropriate
• The appropriate screenings and other preventive
services that Medicare covers
• Performed by doctor of medicine, or osteopathy,
PA, NP, or CNS
Coding & Compliance Initiatives, Inc. 52IPPE/Welcome to Medicare
• Revenue code 521
• HCPCS code G0402 (Welcome to Medicare)
• EKG Services
• HCPCS code G0404 (tracing only)
• HCPCS code G0405 (interpretation and report only) –
this is included in G0402 and should NOT be separately
reported. This does not have a waived co-insurance.
• Technical Billed to carrier
• CMS-1500 claim form or 837P
• Use Practitioners National Provider Identifier (NPI)
Coding & Compliance Initiatives, Inc. 53IPPE Summary of Requirements
• Review of the individual’s medical and social history
with attention to modifiable risk factors for disease
detection
• Review of the individual’s potential (risk factors) for
depression or other mood disorders
• Review of the individual’s functional ability and level of
safety
• An examination to include measurement of the
individual’s height, weight, BMI, blood pressure, a
visual acuity screen, and other factors as deemed
appropriate, based on the beneficiary’s medical and
social history
• End-of-life planning, upon agreement of the individual
Coding & Compliance Initiatives, Inc. 54IPPE Summary of Requirements
• Education, counseling, and referral, as deemed appropriate, based
on the results of the review and evaluation services described in the
previous elements
• Education, counseling, and referral including a brief written plan
(e.g., a checklist or alternative) provided to the individual for
obtaining the appropriate screening and other preventive services,
which are separately covered under Medicare Part B (that is,
pneumococcal, influenza and hepatitis B vaccines and their
administration, screening mammography, screening pap smear and
screening pelvic examinations, prostate cancer screening tests,
colorectal cancer screening tests, diabetes outpatient self-
management training services, bone mass measurements, glaucoma
screening, medical nutrition therapy for individuals with diabetes or
renal disease, cardiovascular screening blood tests, diabetes
screening tests, screening ultrasound for abdominal aortic
aneurysms, an electrocardiogram, and additional preventive services
covered under Medicare Part B through the Medicare national
coverage determinations process).
Coding & Compliance Initiatives, Inc. 55Annual Wellness Visit (AWV)
• G0438: Annual wellness visit, includes PPPS, first
visit (annual wellness first)
• G0439: Annual wellness visit, includes PPPS,
subsequent visit (subsequent)
• Revenue code from 052X series
Coding & Compliance Initiatives, Inc. 56Annual Wellness Visit (AWV)
• Personalized prevention plan or “wellness visit”
• Includes but is not limited to
• Health risk assessment, and may contain:
• Establishment or updated individual medical and
family history
• List of current providers and suppliers that are
regularly involved in providing medical care (list
prescribed drugs)
• Measurement of height, weight, body mass index (or
waist circumference, if appropriate), blood pressure,
and other routine measurements
• Detection of cognitive impairment
Coding & Compliance Initiatives, Inc. 57Health Risk Assessment
• Demographic Data: • Behavioral Risk:
• Age • Tobacco use
• Physical activity
• Gender • Nutrition and oral health
• Race • Alcohol consumption
• Ethnicity • Sexual health
• Motor vehicle safety (seatbelt) and Home safety
• Self Assessment of:
•
• Health Status Activities of daily living
• Dressing
• Frailty • Feeding
• Physical Functioning • Toileting
•
• Psychosocial Risks: •
Bathing and Grooming
Physical ambulation (balance, fall risk, etc.)
• Depression/life satisfaction
• Instrumental activities of daily living
• Stress • Shopping
• Anger • Food preparation
• Loneliness/social isolation • Using the telephone
• Pain • Housekeeping and Laundry
•
• Fatigue •
Mode of transportation
Responsibility of medications
• Ability to handle finance
Coding & Compliance Initiatives, Inc. 58AWV – Medical and Family History
• At a minimum, document the following:
• Medical events of the beneficiary’s parents, siblings, and
children, including conditions that may be hereditary or place
the beneficiary at increased risk
• Past medical and surgical history, including experiences with
illnesses, hospital stays, operations, allergies, injuries, and
treatments
• Use of, or exposure to, medications and supplements,
including calcium and vitamins
• We encourage providers to pay close attention to opioid use
during this part of the AWV, which includes opioid use
disorders (OUD). If a patient is using opioids, assess the
benefit for other, non-opioid pain therapies instead, even if
the patient does not have OUD but is possibly at risk.
Coding & Compliance Initiatives, Inc. 59AWV - Summary
• Establish a list of current providers and suppliers
• Include current providers and suppliers that
regularly provide medical care to the beneficiary
• Obtain the following:
• Height, weight, body mass index (BMI; or waist
circumference, if appropriate), and blood pressure
• Other routine measurements deemed appropriate
based on medical and family history
Coding & Compliance Initiatives, Inc. 60AWV - Summary
• Detect any Cognitive Impairment:
• Assess the beneficiary’s cognitive function by direct
observation, while considering information from
beneficiary reports and concerns raised by family
members, friends, caregivers, and others. If
appropriate, use a brief validated structured
cognitive assessment tool. For more information,
refer to the National Institute on Aging’s
Alzheimer’s and Dementia Resources for
Professionals website.
Coding & Compliance Initiatives, Inc. 61AWV - Summary
• Potential risk factors for depression, including
current or past experiences with depression or
other mood disorders:
• Use any appropriate screening instrument. You may
select from various available standardized screening
tests designed for this purpose. For more
information, refer to the Depression section on the
Substance Abuse and Mental Health Services
Administration–Health Resources and Services
Administration’s Screening Tools website.
Coding & Compliance Initiatives, Inc. 62AWV - Summary
• Functional ability and level of safety:
• Use direct observation of the beneficiary or
select appropriate questions from various
available screening questionnaires, or use
standardized questionnaires recognized by
national professional medical organizations to
assess, at a minimum, the following topics:
• Ability to successfully perform ADLs
• Fall risk
• Hearing impairment
• Home safety
Coding & Compliance Initiatives, Inc. 63AWV - Summary
• Establish an appropriate written screening
schedule for the beneficiary, such as a checklist
for the next 5 to 10 years
• Base written screening schedule on:
• Recommendations from the United States
Preventive Services Task Force (USPSTF) and the
Advisory Committee on Immunization Practices
(ACIP)
• The beneficiary’s HRA, health status and screening
history, and age-appropriate preventive services
Medicare covers
Coding & Compliance Initiatives, Inc. 64AWV - Summary
• Establish a list of beneficiary risk factors and
conditions for which primary, secondary, or
tertiary interventions are recommended or
underway
• Include the following:
• Mental health conditions including depression,
substance use disorder, and cognitive impairment
• Risk factors or conditions identified through an IPPE
• Treatment options and their associated risks and
benefits
Coding & Compliance Initiatives, Inc. 65AWV - Summary
• Furnishing of personalized health advice to
the individual and a referral, as appropriate,
to health education or preventive counseling
services or programs aimed at reducing
identified risk factors and improving self-
management, or community-based lifestyle
interventions to reduce health risks and
promote self-management and wellness,
including weight loss, physical activity,
smoking cessation, fall prevention, and
nutrition.
Coding & Compliance Initiatives, Inc. 66AWV - Summary
• Furnish, at the beneficiary’s discretion, advance
care planning services. Include discussion
about:
• Future care decisions that may need to be made
• How the beneficiary can let others know about care
preferences
• Caregiver identification
• Explanation of advance directives, which may
involve the completion of standard forms
Coding & Compliance Initiatives, Inc. 67AWV Initial versus Subsequent
G0438 - Annual wellness visit; includes a personalized
prevention plan of service (PPS), initial visit
G0439 - Annual wellness visit; includes a personalized
prevention plan of service (PPS),subsequent visit
Coding & Compliance Initiatives, Inc. 68INITIAL AWV SUBSEQUENT AWV
Administer Health Risk Assessment (HRA) Update Health Risk Assessment
Establish medical/family history Update to medical/family history
Establish list of current providers & suppliers involved in Update list of providers & suppliers
medical care
Measurement of height, weight, BMI, BP and other Measurement of height, weight, BMI, BP and other routine
routine measurements deemed appropriate based on measurements deemed appropriate based on history
history
Detection of any cognitive impairments Detection of any cognitive impairments
Review potential (risk factors) and conditions for which Update to list of risk factors and conditions
interventions are recommended or already underway
Establish a written screening schedule Update to written screening schedule
Review of functional ability and level of safety based on
direction observation or use of appropriate screening
questions or questionnaire recognized by national
professional medical organizations
Furnish personalized health advise and refer as Furnish personalized health advise and refer as appropriate
appropriate to health education, preventive counseling to health education, preventive counseling services or
services or programs aimed at reducing identified risk programs aimed at reducing identified risk factors
factors
Any other element determined by HHS Any other element determine by HHS
Coding & Compliance Initiatives, Inc. 69IPPE/Welcome to Medicare and
AWV
• When IPPE or AWV is rendered on same day as
another billable visit, only the preventive is
reimbursed, however, we should report all
services rendered that are appropriate and
medically necessary.
• Co-insurance waived
Coding & Compliance Initiatives, Inc. 70AWV and IPPE Strategies
• Combine templates
• Train staff – double book providers schedule
• Run reports to see who is due for their wellness
visit
Coding & Compliance Initiatives, Inc. 71EKG
• FQHCs are instructed to bill the technical
component of the EKG to the carrier when
applicable
• CMS-1500 claim form or 837P
• Use practitioner’s NPI
• As noted in the CMS IOM Publication 100-04,
Chapter 9, the professional component is
included in the all-inclusive rate for FQHCs
Coding & Compliance Initiatives, Inc. 72EKG Documentation
• As far back as 1992, the CPT® codebook has included
language stating, “a written report, signed by the
interpreting physician, should be considered an integral part
of a radiologic procedure or interpretation.”
• CMS does not require the provider to document an ECG
interpretation on a separate piece of paper, but instead
allows for a complete written interpretation to be recorded
within the medical record (check with your local carrier for
further guidance). CMS further requires a report to be
complete, documented similarly to that of a specialist in the
field (radiology), and consistent with the treatment
rendered. CPT® states there must be a “separate, signed,
written, and retrievable report.”
Coding & Compliance Initiatives, Inc. 73Screening Pelvic and Breast
Exam
• Screening Pelvic and Clinical Breast Examination
(G0101)
• Screening Pap Smear (Q0091)
• Billable if this is the only service rendered for date
of service or with other services on the same day
• Co-insurance waived
Coding & Compliance Initiatives, Inc. 74Screening Pelvic and Breast
Exam
• She has not had such a test during the preceding two years or is a
woman of childbearing age (§1861(nn) of the Social Security Act
(the Act).
• There is evidence (on the basis of her medical history or other
findings) that she is at high risk of developing cervical cancer and
her physician (or authorized practitioner) recommends that she
have the test performed more frequently than every two years.
• High risk factors for cervical and vaginal cancer are:
• Early onset of sexual activity (under 16 years of age)
• Multiple sexual partners (five or more in a lifetime)
• History of sexually transmitted disease (including HIV infection)
• Fewer than three negative or any pap smears within the previous
seven years; and
• DES (diethylstilbestrol) - exposed daughters of women who took
DES during pregnancy.
Coding & Compliance Initiatives, Inc. 75Screening Pelvic and Breast
Exam
• COUNTING: To determine the 11- and 23- month
periods, start counts beginning with the month
after the month in which a previous test/procedure
was performed.
• COUNTING EXAMPLE: A beneficiary identified as
being at high risk for developing cervical cancer
received a screening Pap smear in January 2000.
Start counts beginning with February 2000. The
beneficiary is eligible to receive another screening
Pap smear in January 2001 (the month after 11 full
months have passed).
Coding & Compliance Initiatives, Inc. 76Documentation Requirements for
Screening Pelvic and Breast Exam
1. Inspection and palpation of breasts for masses or
lumps, tenderness, symmetry, or nipple discharge
2. Digital rectal examination including sphincter tone,
presence of hemorrhoids, and rectal masses
3. External genitalia (for example, general appearance,
hair distribution, or lesions)
4. Urethral meatus (for example, size, location, lesions,
or prolapse)
5. Urethra (for example, masses, tenderness, or
scarring)
6. Bladder (for example, fullness, masses, or
tenderness)
Coding & Compliance Initiatives, Inc. 77Documentation Requirements for
Screening Pelvic and Breast Exam
7. Vagina (for example, general appearance,
estrogen effect, discharge, lesions, pelvic support,
cystocele, or rectocele)
8. Cervix (for example, general appearance,
lesions or discharge)
9. Uterus (for example, size, contour, position,
mobility, tenderness, consistency, descent, or
support)
10. Adnexa/parametria (for example, masses,
tenderness, organomegaly, or nodularity)
11. Anus and perineum
Coding & Compliance Initiatives, Inc. 78Coding & Compliance Initiatives,
79
Inc.Contact
• Shellie Sulzberger, LPN, CPC, ICDCT-CM
• 913-768-1212
• ssulzberger@ccipro.net
• www.ccipro.net
Coding & Compliance Initiatives, Inc. 80About CCI
• CCI assists our clients improve their documentation
quality, coding and billing accuracy, and compliance
with health care regulations www.ccipro.net
Coding & Compliance Initiatives,
81
Inc.Shellie Sulzberger, LPN, CPC, ICDCT-CM
Ms. Sulzberger is a Licensed Practical Nurse, Certified Professional
Coder and ICD-10 Trainer. She received her Bachelors of Science
degree in Business Administration from Mid America Nazarene
University. Ms. Sulzberger received her nursing license in 1994 and
was a practicing clinician at Saint Luke’s Health System for several
years before transferring to the internal compliance/audit area. She
became credentialed as a Certified Professional Coder in 1996 and
assisted the Saint Luke’s Health System with performing medical
record chart audits to verify the accuracy of the internal coding and
claims processing.
Ms. Sulzberger spent approximately six years as a coding/billing
consultant with National accounting and consulting firms (BKD, Grant
Contact Info: Thornton) before becoming the President of Coding & Compliance
Tel: 913-768-1212 Initiatives, Inc. (CCI) in April 2003. Ms. Sulzberger assists her clients
with improving their operational performance in a variety of critical
Or email outcome areas, including coding/billing, corporate compliance,
ssulzberger@ccipro.net charge capture processes, etc. Ms. Sulzberger works with a variety of
www.ccipro.com health care providers including hospitals, physician practices, and
rural health clinics in their daily compliance and operational activities.
Ms. Sulzberger presents locally and nationally on coding topics as well
as developing specialized training programs to meet the needs of her
clients. Shellie recently was credentialed through American Institute
of Healthcare Compliance as a Certified ICD-10 Trainer.
Coding & Compliance Initiatives, Inc. 82You can also read