European Prospective Investigation into Cancer and Nutrition (EPIC): study populations and data collection
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Public Health Nutrition: 5(6B), 1113–1124 DOI: 10.1079/PHN2002394
European Prospective Investigation into Cancer and Nutrition
(EPIC): study populations and data collection
E Riboli1,*, KJ Hunt2, N Slimani1, P Ferrari1, T Norat1, M Fahey1, UR Charrondière1,
B Hémon1, C Casagrande1, J Vignat1, K Overvad3, A Tjønneland4, F Clavel-Chapelon5,
A Thiébaut5, J Wahrendorf6, H Boeing7, D Trichopoulos8,9, A Trichopoulou8, P Vineis10,
D Palli11, HB Bueno-de-Mesquita12, PHM Peeters13, E Lund14, D Engeset14,
CA González15, A Barricarte16, G Berglund17, G Hallmans18, NE Day19, TJ Key20,
R Kaaks21 and R Saracci1,22
1
Unit of Nutrition and Cancer, International Agency for Research on Cancer (IARC – WHO), 150 cours Albert-
Thomas, 69372 Lyon Cedex 08, France: 2Division of Clinical Epidemiology, University of Texas Health Science
Center, San Antonio, TX, USA: 3Department of Epidemiology and Social Medicine, University of Aarhus, Denmark:
4
Institute of Cancer Epidemiology, Danish Cancer Society, Copenhagen, Denmark: 5INSERM, U521, Institute
Gustave Roussy, Villejuif, France: 6German Cancer Research Centre, Heidelberg, Germany: 7Department of
Epidemiology, German Institute of Human Nutrition, Potsdam-Rehbrücke, Germany: 8Department of Hygiene and
Epidemiology, School of Medicine, University of Athens, Greece: 9Department of Epidemiology, Harvard School of
Public Health, Boston, MA, USA: 10Department of Biomedical Sciences and Human Oncology, University of Turin,
Italy: 11Molecular & Nutrition Epidemiology Unit, CSPO, Scientific Institute of Tuscany, Florence, Italy: 12Department
of Epidemiology, National Institute of Public Health and the Environment, Bilthoven, The Netherlands: 13Julius Center
for General Practice and Patient Oriented Research, University of Utrecht, The Netherlands: 14Institute of Community
Medicine, University of Tromsø, Norway: 15Department of Epidemiology, Catalan Institute of Oncology, Barcelona,
Spain: 16Service of Surveillance and Epidemiological Control, Institute of Public Health of Navarra, Pamplona,
Spain: 17Department of Medicine, Lund University, Malmö University Hospital, Sweden: 18Public Health and Clinical
Medicine, University Hospital of Northern Sweden, Umeå, Sweden: 19Department of Public Health and Primary
Care, School of Clinical Medicine, University of Cambridge, UK: 20Cancer Research UK, Epidemiology Unit,
University of Oxford, UK: 21Hormones and Cancer Group, IARC – WHO, Lyon, France: 22Division of Epidemiology,
IFC National Research Council, Pisa, Italy
Abstract
The European Prospective Investigation into Cancer and Nutrition (EPIC) is an
ongoing multi-centre prospective cohort study designed to investigate the
relationship between nutrition and cancer, with the potential for studying other
diseases as well. The study currently includes 519 978 participants (366 521 women
and 153 457 men, mostly aged 35–70 years) in 23 centres located in 10 European
countries, to be followed for cancer incidence and cause-specific mortality for several
decades. At enrolment, which took place between 1992 and 2000 at each of the
different centres, information was collected through a non-dietary questionnaire on
lifestyle variables and through a dietary questionnaire addressing usual diet.
Anthropometric measurements were performed and blood samples taken, from
which plasma, serum, red cells and buffy coat fractions were separated and aliquoted
for long-term storage, mostly in liquid nitrogen. To calibrate dietary measurements, a
standardised, computer-assisted 24-hour dietary recall was implemented at each
centre on stratified random samples of the participants, for a total of 36 900 subjects.
EPIC represents the largest single resource available today world-wide for Keywords
prospective investigations on the aetiology of cancers (and other diseases) that can Nutrition
Cancer
integrate questionnaire data on lifestyle and diet, biomarkers of diet and of
Chronic diseases
endogenous metabolism (e.g. hormones and growth factors) and genetic Cohort study
polymorphisms. First results of case–control studies nested within the cohort are Anthropometry
expected early in 2003. The present paper provides a description of the EPIC study, Biological samples
with the aim of simplifying reference to it in future papers reporting substantive or EPIC study
methodological studies carried out in the EPIC cohort. Europe
*Corresponding author: Email ntr@iarc.fr q The Authors 2002
Downloaded from https://www.cambridge.org/core. 03 Sep 2021 at 20:04:47, subject to the Cambridge Core terms of use.1114 E Riboli et al.
The existence of a relationship between nutrition and Cancer programme of the European Union. Initiated in
cancer was first shown clearly in the 1940s in a series of 1992, this study has grown progressively into a
experimental studies in which severe energy restriction collaborative endeavour between 23 centres in 10
markedly reduced the occurrence of cancers in mice1. In European countries. The principal aim of EPIC is to
the 1960s, following the development of cancer registries, investigate, in a prospective manner, the aetiology of
ecological studies drew attention to the large world-wide cancers at various sites (as well as other forms of chronic
variations in cancer incidence, and provided first disease) in relation to diet and lifestyle, taking advantage
suggestions that these variations might be related to both of the contrast in cancer rates and dietary habits
differences in lifestyle, particularly diet2 – 4. In the 1970s between centres and countries and of the large overall size
and 1980s, a large number of traditional case– control of the study, which makes it possible to explore
studies were conducted to identify dietary risk factors with interactions between nutritional, genetic, hormonal and
greater specificity, and since the late 1980s these studies lifestyle factors.
have been followed by a series of prospective cohort Enrolment of the EPIC cohort participants and collec-
studies5. tion of baseline questionnaire data, anthropometric
In spite of several decades of research, comparatively measurements and blood samples have now been
few nutrition-related factors have been established completed for all countries. By May 2002, the follow-up
unequivocally as playing a causal role in human cancer for cancer incidence had already led to the identification of
occurrence. These established factors include obesity and large numbers (1000 – 4500 cases) of subjects who
alcohol consumption5. In fact, epidemiological studies on developed cancer after cohort enrolment at one of the
nutrition and cancer have faced several methodological major sites (lung, colon–rectum, prostate and breast). This
problems. Dietary habits are difficult to assess accurately represents a total of about 16 000 incident cases. In
and dietary exposures relevant to the aetiology of today’s previous reports, the rationale for the EPIC study and its
cancer incidence or mortality may have occurred over future perspectives have been discussed6,9,10. In the
many years. Food patterns and specific food components, present paper, we describe in some detail the individual
macro- and micronutrients, may all play aetiological roles EPIC study cohorts and their source populations, as well as
and their effects may also be modified by other lifestyle the baseline information and biological samples collected
factors such as physical activity or childbearing patterns. from the participants of each cohort.
Case –control studies may be flawed by differential bias
between cases and controls in the recall of dietary habits,
and case –control studies that use biomarkers of diet or Methods
metabolism may also be flawed because the markers may
be altered by the presence or diagnosis of a tumour. In
principle, prospective cohort studies are not subject to Outline
these two major forms of bias. But, unless they are very EPIC is an ongoing multi-centre prospective cohort study.
large in size, they are inadequate to generate informative The prospective cohort approach includes the collection
data on the aetiology of less common forms of cancer, of baseline questionnaire and interview data on diet and
such as those of the oesophagus, gall bladder, thyroid non-dietary variables, as well as anthropometric measure-
gland, ovary or endometrium. Even for the common forms ments and blood samples for long-term storage from
of cancer, such as those of the lung, colon–rectum, breast, apparently healthy populations. The cohort participants
prostate and stomach, prospective cohort studies may are followed over time for the occurrence of cancer and
prove less than adequate as soon as the aetiological other diseases, as well as for overall mortality, to allow
investigation focuses on sub-types characterised by incidence and mortality comparisons by exposure vari-
localisation, histology or other biological traits. ables. At regular intervals, follow-up questionnaires are
Finally, a drawback of prospective studies has been the used to update information on selected aspects of lifestyle
fact that so far they have often been conducted within that are known or strongly suspected to be related to
populations with relatively homogeneous lifestyles and cancer risk and that may have changed over time. The
dietary patterns. This homogeneity, combined with EPIC study has recruited 519 978 participants, in 23 centres
relatively large errors in dietary intake assessments, may located in 10 European countries. The study started with
make it very difficult to demonstrate moderate associ- 17 research centres in seven core EPIC countries (France,
ations of specific aspects of diet with cancer risk. Germany, Greece, Italy, The Netherlands, Spain and the
In an attempt to overcome these various limitations, the UK). Subsequently, these were joined by centres in three
International Agency for Research on Cancer (IARC) Scandinavian countries (Sweden, Denmark and Norway)
initiated the European Prospective Investigation into and one centre in Italy (Naples) that were conducting
Cancer and Nutrition (EPIC) – a multi-centre prospective broadly similar prospective studies. The enrolment of
cohort study in Western Europe6 – 10. The study has been subjects included in all EPIC centres took place between
supported from its beginning by the Europe Against 1992 and 2000.
Downloaded from https://www.cambridge.org/core. 03 Sep 2021 at 20:04:47, subject to the Cambridge Core terms of use.EPIC study description 1115
Source populations, invitation and study logistics participants received the non-dietary questionnaire by mail,
Participant eligibility within each cohort was based and were invited to a study centre for an examination that
essentially on geographic or administrative boundaries. included collection of the lifestyle questionnaire, venepunc-
The source populations were identified according to age, ture, anthropometry and blood pressure measurements (in
gender and, optionally, other criteria (Table 1)11 – 17. The Spain only in sub-sample of the cohort), as well as an
age range was generally from 35 to 70 years (Table 1). The interviewer-administered computer-driven dietary ques-
actual study populations are samples of convenience of tionnaire. Finally, in Greece, participants were initially
volunteers agreeing to participate, but not required to be invited by mail, sent a questionnaire, and asked to come for
random samples of defined populations; moreover, only an examination at a study centre; however, recruitment
some of the centres have maintained records of all the numbers were so low that active recruitment was initiated. In
individuals invited to participate. As shown in Table 1, in contrast to most other EPIC centres, actively recruited Greek
the majority of study centres, subjects were invited from participants had their EPIC study centre examination at
the general adult population residing in a given town or enrolment and all completed an interviewer-administered
geographical area. There were, however, exceptions to questionnaire on diet and a questionnaire on lifestyle. In
this recruitment scheme. The French cohort was based on Denmark and Malmö (Sweden), the participants filled in
members of the health insurance for teachers (with the aim dietary questionnaires at home and lifestyle questionnaires
of facilitating follow-up for incidence of cancer and other at the study centres. In Umeå (Sweden), both questionnaires
diseases); components of the Italian and Spanish cohorts were completed at the study centre. In Norway, participants
included members of local blood donor associations; the completed an initial mailed questionnaire unrelated to EPIC,
cohorts in Utrecht (The Netherlands) and Florence (Italy) completed a subsequent mailed questionnaire for EPIC, and
included women invited for a local population-based then had blood samples mailed to the study centre in Tromsø
breast cancer screening programme. In Oxford (UK) half for processing.
of the cohort was recruited among subjects who did not
eat meat, including vegans (who consume no animal Dietary intake assessments
products), lacto-ovo vegetarians and fish eaters (i.e. Dietary intake was assessed by a number of different
consumers of fish but not meat). In France, Norway, instruments that had been developed and validated
Utrecht (The Netherlands) and Naples (Italy) only women previously in a series of studies within the various source
were recruited. populations participating in EPIC (Table 3)19 – 23. Follow-
Centre-specific information on geographical/political ing the results of the methodological studies and taking
area, source population, eligibility criteria and enumer- into account the local context, three dietary assessment
ation of invited participants are shown in Table 1, while methods were adopted:
Table 2 provides centre- and gender-specific information
on study population size, enrolment dates and participant 1. Extensive self-administrated quantitative dietary ques-
age at enrolment. tionnaires, containing up to 260 food items and
As a rule, participants were invited to participate either estimating individual average portions systematically,
by mail or in person (Table 1). Individuals who agreed to were used in northern Italy, The Netherlands, Germany
participate signed an informed consent agreement and and Greece (where dietary questionnaires were
were mailed a questionnaire on diet and a questionnaire interviewer-administered). Questionnaires, similar in
on lifestyle. Most participants completed these question- content to the self-administered quantitative dietary
naires at home and were then invited to a study centre for questionnaires but structured by meals, were used in
an examination. This included collection of the two Spain, France and Ragusa (south Italy). To increase
completed questionnaires, venepuncture, anthropometry compliance, the centres in Spain and Ragusa
and measurement of blood pressure. For the blood performed a face-to-face dietary interview using a
pressure measurements, uniform procedures were rec- computerised dietary program, whereas the dietary
ommended but no standard method or common type of questionnaire was self-reported in France.
instrument was introduced18. Among the seven initial EPIC 2. Semi-quantitative food-frequency questionnaires (with
countries, the centres in Italy (except Ragusa), the UK the same standard portion(s) assigned to all subjects)
(except Oxford), The Netherlands and Germany followed were used in Denmark, Norway, Naples in Italy and
these procedures. In France, a study that started in 1990 Umeå in Sweden.
included lifestyle questions with self-reported anthropo- 3. Combined dietary methods were used in the UK and
metry measurements; the participants enrolled in EPIC are Malmö (Sweden). The two British centres used both a
those who answered the dietary questionnaire. A subset of semi-quantitative food-frequency questionnaire and a
the French cohort (20 725 women close to a metropolitan 7-day record, whereas a method combining a short
area) later came to a field centre, donated a blood sample, non-quantitative food-frequency questionnaire with a
and underwent blood pressure and anthropometry 14-day record on hot meals (lunches and dinners) was
measurements. In Spain and Ragusa (Italy), the recruited developed in Malmö.
Downloaded from https://www.cambridge.org/core. 03 Sep 2021 at 20:04:47, subject to the Cambridge Core terms of use.1116
Table 1 Source populations, eligibility criteria and recruitment procedures of the cohorts: the European Prospective Investigation into Cancer and Nutrition (EPIC) study
Geographic/political Source Enumeration
Country area (centre) population* (description) Target eligibility criteria Initial contact of invited
Core initial EPIC cohorts
Greece Greece: nation-wide Active recruitment of the general Apparently healthy men and women In person and by No
population aged 25–82 mail
Spain Granada: province Blood donors, general population Residents: men aged 40–64, women In person and by No
(recruited through census, health centres) aged 35–64 mail
Murcia: region Blood donors and their partners Residents: men aged 40–65, women In person and by No
(67% of cohort), general population aged 35–65 mail
of two towns (23%), civil servants (5%),
employees of two companies (3%),
participants in a cardiovascular risk study (2%)
Navarra: Pamplona city Blood donors, general population Residents: men aged 40–65, women Mail Yes
and Navarra region aged 35–65
San Sebastian: city Blood donors, employees of selected Residents: men aged 40–65, women In person and by Yes
Downloaded from https://www.cambridge.org/core. 03 Sep 2021 at 20:04:47, subject to the Cambridge Core terms of use.
and Gipuzkoa province enterprises (recruited through census aged 35–65 mail
of selected municipalities)
Asturias: region Blood donors, regional civil servants Men aged 40– 64, women aged 35–64 Mail Yes
and general population
Italy Ragusa: province Local blood donors association, Residents: men aged 40–65, women Mail Yes
population-based recruitment in four aged 35–65
towns (Monterosso, Giarratana, Ispica
and Chiaramonte), local teachers union,
and other sources
Florence: province Breast cancer screening participants (CSPO), Residents: men aged 35–64, women In person and by No
men and women from the general population aged 35–64, without prevalent cancer mail
Turin: city Blood donors, employees, volunteers, medical Residents: men aged 40–74, women In person No
test users at national health service aged 35–74, without prevalent cancer
Varese: province Volunteers from resident general population, Men aged 40– 65, women aged 35–65 In person and by No
mostly an extension of an ongoing study mail
(ORDET)
France France Nation-wide health insurance programme Women aged 40–65 in 1990 with informed Mail Yes
(MGEN): teachers and school workers enrolled consent to obtain MGEN info on non-
in an ongoing study prior to EPIC respondents
E Riboli et al.Germany Heidelberg and General population Residents: men aged 40– 65, women Mail Yes
surrounding areas aged 35– 65, completed questionnaires
and examination
Potsdam and surrounding General population Residents: men aged 40– 65, women Mail Yes
areas aged 35– 65, completed questionnaires
and examination
Netherlands Bilthoven: Amsterdam, Population-based age- and sex-stratified Residents: men and women aged 20–60 in Mail Yes
Doetinchem and Maastricht samples of the general population Amsterdam and Maastricht, and aged
(three cities) 20–65 in Doetinchem
EPIC study description
Utrecht: district Population-based breast cancer screening Residents: women aged 49– 70 Mail Yes
participants
United Kingdom Cambridge: Norfolk Population-based patients of general Listed by general practitioners: men and Mail Yes
practitioners women aged 45– 74
Oxford: (1) local counties; (1) Population based in collaboration with (1) Listed by general practitioners: men Mail No
(2) ‘health-conscious’ from general practitioners; (2) vegetarians, and women aged 40–65; (2) men and
England, Wales, Scotland and vegans and other health-conscious individuals women aged 20+, but targeted at those
Northern Ireland in collaboration with vegetarian societies and aged 35+
magazines
Associated EPIC cohorts
Italy Naples Female volunteers from resident general Women aged 30– 69 In person and by No
population mail
Denmark Aarhus Population-based Born in Denmark: men and women Mail Yes
aged 50– 64, without prevalent cancer
Copenhagen Population-based Born in Denmark: men and women Mail Yes
aged 50– 64, without prevalent cancer
Sweden Malmö: city Population-based Residents: men aged 50– 72, women Mail Yes
aged 46– 72
Umeå: the Västerbotten county Population-based Residents: men and women aged Mail Yes
30, 40, 50 or 60
Norway Tromsø: national sample Population-based Women born in Norway between Mail Yes
1943 and 1957
* Under source population, the term ‘population-based’ implies that participants were invited as a random sample of their population, while the term ‘general population’ implies that volunteers were invited from the
Downloaded from https://www.cambridge.org/core. 03 Sep 2021 at 20:04:47, subject to the Cambridge Core terms of use.
general population.
11171118 E Riboli et al.
Table 2 Characteristics of the cohorts: the European Prospective Investigation into Cancer and Nutrition
(EPIC) study
Enrolment Enrolment age (years)
Country Centre n* period (date) (1st– 99th percentile)
Core initial EPIC cohorts
Greece Male 11 954 1994–1999 30–76
Female 16 618 1994–1999 30–76
Spain Granada Male 1796 1992–1996 35–65
Female 6083 1992–1996 35–65
Murcia Male 2685 1992–1996 38–65
Female 5831 1992–1996 35–65
Navarra Male 3908 1992–1995 40–64
Female 4176 1992–1995 35–64
San Sebastian Male 4158 1992–1995 40–65
Female 4259 1992–1995 35–65
Asturias Male 3085 1992–1995 40–65
Female 5459 1992–1995 35–65
Italy Ragusa Male 3053 1993–1997 37–65
Female 3350 1993–1997 35–65
Florence Male 3514 1993–1998 35–65
Female 10 083 1992–1998 35–65
Turin Male 6047 1993–1998 35–65
Female 4557 1993–1998 35–65
Varese Male 2557 1995–1997 40–65
Female 9526 1993–1997 35–72
France Female 72 996 1993–1997 43–68
Germany Heidelberg Male 11 929 1994–1998 40–65
Female 13 617 1994–1998 35–65
Potsdam Male 10 904 1994–1998 38–65
Female 16 644 1994–1998 35–65
Netherlands Bilthoven Male 10 280 1993–1997 21–63
Female 12 435 1993–1997 21–64
Utrecht Female 17 357 1993–1997 49–70
United Kingdom Cambridge Male 13 698 1993–1998 41–76
Female 16 744 1993–1998 41–76
Oxford Male 13 214 1994–2000 22–83
Female 44 284 1993–2000 21–79
Associated EPIC cohorts
Italy Naples Female 5062 1993–1997 35–68
Denmark Aarhus Male 8433 1995–1997 50–65
Female 8721 1995–1997 50–65
Copenhagen Male 18 746 1993–1997 50–65
Female 21 154 1993–1997 50–65
Sweden Malmö Male 11 063 1991–1996 47–72
Female 17 035 1991–1996 45–73
Umeå Male 12 433 1992–1996 30–60
Female 13 299 1992–1996 30–60
Norway Tromsø Female 37 231 1998–1998 41–56
* By April 2002.
The EPIC study aims to increase the overall statistical sub-samples of 5–12% of study participants in each of
power of identifying diet – disease relationships by the sub-cohorts (about 1.5% in the British cohorts). In
combining study populations that have different types total, 24-hour recalls were collected from 36 900 EPIC
of diets and lifestyles and different cancer incidence participants24 – 26. The baseline dietary assessments
rates, resulting in increased overall ranges of dietary conducted on all EPIC participants, used locally to
exposures and cancer risks. Any global statistical estimate long-term usual dietary intake, will be used to
analysis that takes account of the total range of dietary rank subjects within centres, while the 24-hour dietary
exposures of all sub-cohorts combined requires that the recall can be used as a reference method to correct for
dietary assessments obtained in each of the sub-cohorts systematic between-centre over- or underestimations in
be comparable on an absolute scale. Such compar- the baseline dietary assessments27. The calibration
ability, however, can be compromised by the use of study, its rationale and its standardisation are described
different dietary assessment methods across the 23 EPIC in detail elsewhere25 – 31. A common food composition
centres. To overcome this problem, it was decided to database for a number of nutrients, standardised across
collect additional dietary intake data by a computer- the European countries involved in EPIC, is currently
assisted 24-hour dietary recall (EPIC-SOFT) in representative being developed32,33.
Downloaded from https://www.cambridge.org/core. 03 Sep 2021 at 20:04:47, subject to the Cambridge Core terms of use.EPIC study description 1119
Table 3 Baseline dietary assessment: the European Prospective Investigation into Cancer and Nutrition (EPIC) study
Number
Location Assessment tool(s) and its(their) structure Administered of items*
Core initial EPIC cohorts
France Quantitative dietary questionnaire structured by meals† Self 210
Northern Italy‡ Quantitative dietary questionnaire structured by meal courses§ Self 236
Italy, Ragusa Quantitative dietary questionnaire structured by meals, computer-driven† Face-to-face 266
Spain Quantitative dietary questionnaire structured by meals, computer-driven† Face-to-face 736{
United Kingdom (1) Semi-quantitative FFQk; (2) 7-day records (diaries) Self 170
Netherlands Quantitative dietary questionnaire§ Self 213
Greece Quantitative dietary questionnaire§ Face-to-face 260{
Germany Quantitative dietary questionnaire§ Self 254
Associated EPIC cohorts
Sweden, Malmö Combination of semi-quantitative FFQk and 14-day record of hot meals Self** 2443††
Sweden, Umeå Semi-quantitative FFQk Self 98
Denmark Semi-quantitative FFQk Self 173
Norway Semi-quantitative FFQk Self 88
Italy, Naples Semi-quantitative FFQk Face-to-face 158
FFQ – food-frequency questionnaire.
* Number of items is defined as the number of foods plus the number of standard mixed recipes.
† Questionnaire structured by main meals (breakfast, lunch, dinner, between-meal food consumption occasions) with meal-specific food frequency and
portion.
‡ Florence, Turin and Varese.
§ Individual average portion sizes were estimated using series of photographs, standard units and/or household measurements.
{ Open-ended sections in the questionnaire.
k The same standard portion(s) were assigned to all subjects. In Denmark, sex-specific mean portions were used to quantify standard mixed recipes.
** Self-reported during the main examination at the centre, and checked immediately by the interviewer.
†† Essentially open-ended dietary assessment method.
Questionnaire data on non-dietary variables Anthropometric measurements
Apart from diet, questionnaire data were collected on a In all EPIC centres, except France, the Oxford cohort and
large number of lifestyle and health factors that are of Norway, height, weight, and waist and hip circumference
interest in studies on nutrition and cancer, as they may were measured on all subjects using similar protocols (in
be related to nutritional status or may be known or Umeå, only weight and height were measured). In
suspected cancer risk factors. For the seven initial EPIC addition, in Italy, Spain, Utrecht, Greece, Germany and
countries, a common set of questions and possible Denmark, sitting height was measured. In France and
answers was agreed upon and translated into national Oxford, weight, height, waist and hip (and sitting height in
questionnaires. This included questions on education France) were measured only for a restricted number of
and socio-economic status; current job, current and past participants, but self-reported weight and height were
occupation which might have led to exposure to obtained from all individuals. In Oxford, self-reported
carcinogens; history of previous illness, disorders or measurements also included waist and hip circumfer-
surgical operations; lifetime history of tobacco smoking; ences. In Norway only self-reported height and weight are
lifetime history of consumption of alcoholic beverages; available34.
physical activity (occupational, walking, cycling, gar-
dening, housework, physical exercise, climbing stairs); Biological samples
menstrual and reproductive history; and use of Biological samples including blood plasma, blood serum,
exogenous hormones for contraception and postmeno- white blood cells and erythrocytes were collected from
pausal replacement therapy (Table 4). In Denmark, 385 747 of the 519 978 EPIC study participants (Table 5).
Sweden and Norway and in the Naples centre in Italy, The procedure for storage of blood samples differed
which joined EPIC at a later stage, questionnaires on between the seven initial EPIC countries and the three
non-dietary variables had been developed quite Scandinavian countries that joined EPIC at a later stage.
independently of those in the initial EPIC countries. In the former countries and in Naples (Italy), blood
Nevertheless, their questionnaires do cover to a large samples were aliquoted into 28 plastic straws containing
extent the same variables, even if these were not 0.5 ml each (12 plasma with sodium citrate, eight serum,
defined in exactly the same manner as for the rest of four erythrocytes, four buffy coat for DNA). To ensure a
EPIC. A comprehensive re-coding scheme was devel- high degree of standardisation, the same materials
oped for standardisation of the questionnaire variables (syringes, straws, etc.) were purchased centrally and
from these study centres, to make the codes as close as distributed to the centres. The samples were then split into
possible to those of the core EPIC lifestyle questions. two mirror halves of 14 aliquots each. One set was stored
Downloaded from https://www.cambridge.org/core. 03 Sep 2021 at 20:04:47, subject to the Cambridge Core terms of use.1120 E Riboli et al.
Table 4 Non-dietary information: the European Prospective Investigation into Cancer and Nutrition (EPIC) study
Anthropometry All centres except Umeå (Sweden) and Tromsø (Norway) have either self-reported (France and
part of the UK) or measured information on weight, height, hip circumference and waist circumference.
In Umeå (Sweden) and Tromsø (Norway) information is available on weight and height only.
Sitting height measurements were obtained in France, Italy, Spain, Utrecht, Greece, Germany and Denmark
Reproductive history All core* centres (except Bilthoven, which has limited information) have detailed information
including, but not limited to, information on menopausal status, pregnancies, miscarriages, induced
abortion, infertility, and hormone use for both birth control and menopause. Of the associated
participants, the Danish and Norwegian centres have complete information, the centre in
Malmö (Sweden) has the majority of information, and the centre in Umeå (Sweden) has this
information on about half of the cohort, which is now increasing via follow-up
Physical activity All core* centres have information on type of physical activity at work, physical exercise
to keep fit and vigorous physical activity, as well as time spent on specific activities including walking, cycling,
gardening, housework, and number of stairs climbed per day. Of the associated
participants, the Danish centres have complete information, the centre in Malmö (Sweden) has the
majority of the information, and the centre in Umeå (Sweden) is limited to information on
type of physical activity at work. The centres in Umeå and Tromsø have additional questions on
physical activity, which are not completely adapted to the core questionnaire
Tobacco smoking All centres have information on smoking status (current, past, never), as well as information on
amount of cigarettes smoked. In addition, all centres (except those in The Netherlands and Norway)
have information on current and past cigar and pipe smoking
Alcohol consumption The core* centres have information on past amount of wine, beer/cider, fortified wine and
spirit/liquor consumed. In addition, for Cambridge, Bilthoven and Greece, information on current
levels of consumption for each of these types of alcohol is available as non-dietary variable.
Of the associated participants, the Danish and Naples centres have complete information whereas
the centres in Malmö (Sweden) and Norway have information on current alcohol consumption only.
No information on past alcohol consumption is available in Umeå (Sweden). However, for all EPIC centres,
additional information on current alcohol consumption is available from the dietary questionnaires
Occupational history The centres in Italy, Spain, Cambridge, Greece, Germany and Denmark have information
on occupational history. The Norwegian centre has information on current occupation
Socio-economic status All centres have information on highest school level achieved
Previous illnesses All centres have information on heart disease and diabetes, while the majority (both core* and
associated participants) of centres have information on stroke, hypertension, hyperlipidaemia, gall
stones, polyps of the large bowl, hysterectomy, oopherectomy and breast surgery, as well as
information on age of onset of each of these events
* Core centres include centres in France, Italy (except Naples), Spain, UK, The Netherlands, Greece and Germany. The associated participants include
centres in Sweden, Denmark, Norway and Naples (Italy).
locally, and one transported to IARC to be stored in liquid Follow-up for changes in lifestyle and health
nitrogen (at 21968C) in a central biorepository. conditions
In Norway the biological samples were collected in After their initial enrolment, cohort members are contacted
twenty 0.5 ml plastic straws; for 9197 subjects, 12 of the 16 at regular intervals every 3 –4 years to obtain information
plasma and two of the four buffy coat samples were on various aspects of lifestyle that are known or strongly
shipped to IARC for storage in the central repository. In suspected of being related to cancer risk, and that may
Sweden and Denmark, blood samples were stored in change over time. This includes tobacco smoking, alcohol
tubes (not in plastic straws) and for practical reasons are drinking, physical activity, weight, menstruation, preg-
stored only in local repositories (the central EPIC nancies, menopause, and other variables. In addition, a
repository at IARC is not suitable for storing tubes). In series of questions was added on whether the subjects had
Sweden, the samples are kept in freezers at 2708C, and in suffered from any major diseases. In most EPIC centres,
Denmark in nitrogen vapour (2 1508C). the first follow-up is currently ongoing and in several it has
The central biological bank located at IARC currently been completed.
contains around 3.8 million straws with blood aliquots
from 275 861 EPIC participants. The straws of each Follow-up for cancer incidence and overall
participant are stored together successively inside a tube, mortality
goblet, canister and container. The canisters are arranged Follow-up aimed at identifying cancer cases occurring
in colour-coded concentric circles located in each of 33 among the EPIC cohort is based on population cancer
liquid nitrogen containers. Each straw is labelled with the registries in seven of the participating countries (Denmark,
participant’s ID and colour-coded to indicate its contents; Italy, The Netherlands, Norway, Spain, Sweden and the
in addition, the tube, goblet and canister are colour-coded UK) and on a combination of methods including health
to aid in identifying the samples. Finally, a computer insurance records, cancer and pathology registries, and on
software program indicates the container, canister, goblet, active follow-up through study subjects and their next-of-
and the location of the goblet and the canister within each kin in three countries (France, Germany and Greece). A
container to track the stored biological samples of each working group created in 1996 (End-Point Committee)
participant. prepared a detailed protocol for the collection and
Downloaded from https://www.cambridge.org/core. 03 Sep 2021 at 20:04:47, subject to the Cambridge Core terms of use.EPIC study description 1121
Table 5 Biological samples: the European Prospective Investigation into Cancer and Nutrition (EPIC) study
Samples collected† Storage
(number of 0.5 ml straws desired) location
White
Age range (years) Female Achievement blood
Centre n (1st– 99th percentile) (%) rate* (%) Plasma Serum cells Erythrocytes IARC Local
Core EPIC cohorts
Greece Nation-wide 28 500 29–76 58.2 99.8 12 8 4 4 Yes Yes
Spain Granada 6892 35–66 77.0 87.5 12 8 4 4 Yes Yes
Murcia 8146 35–65 68.7 95.7 12 8 4 4 Yes Yes
Navarra 7799 36–64 51.5 96.5 12 8 4 4 Yes Yes
San Sebastian 8325 36–65 50.6 98.9 12 8 4 4 Yes Yes
Asturias 8417 35–65 64.0 98.5 12 8 4 4 Yes Yes
Italy Ragusa 6396 35–65 52.3 99.9 12 8 4 4 Yes Yes
Florence 13 597 35–65 74.2 100.0 12 8 4 4 Yes Yes
Turin 10 604 35–64 43.0 100.0 12 8 4 4 Yes Yes
Varese 12 073 36–72 78.9 99.9 12 8 4 4 Yes Yes
France 20 725 43–68 100.0 31.0‡ 12 8 4 4 Yes Yes
Germany Heidelberg 24 235 36–64 52.6 94.9 12 8 4 4 Yes Yes
Potsdam 26 444 35–66 59.8 95.9 12 8 4 4 Yes Yes
Netherlands Bilthoven 19 388 21–64 54.0 93.1§ 12 8 4 4 Yes Yes
Utrecht 16 930 49–69 100.0 96.9 12 8 4 4 Yes Yes
United Kingdom Cambridge 24 035 41–76 54.3 93.8{ 12 8 4 4 Yes Yes
Oxford 19 103 23–73 76.7 96.1k 12 8 4 4 Yes Yes
Associated EPIC cohorts
Italy Naples 5055 34–68 100.0 99.9 12 8 4 4 No Yes
Denmark Aarhus 17 094 50–65 50.8 99.7 Tb Tb Tb Tb No Yes
Copenhagen 39 037 50–65 52.7 97.8 Tb Tb Tb Tb No Yes
Sweden Malmö 28 023 46–73 60.6 99.7 Ta Ta Ta Ta No Yes
Umeå 25 732 30–61 51.7 100.0 Ta Ta Ta Ta No Yes
Norway Tromsø 9197 40–55 100.0 ,60.0** 16 NC 4 NC Yes Yes
Ta – stored in 2 ml tubes at 2 808C; Tb – stored in 1 ml tubes in nitrogen vapour at a temperature between 2 1508C and 2 1608C; NC – not collected.
* In all centres, except those in France, the UK, Bilthoven (Netherlands) and Norway, all EPIC participants were invited to donate blood (Table 2 contains
the denominator used to calculate the achievement rate, which represents the percentage of participants with partial or complete stored biological samples
out of those asked to donate blood).
† In the core centres, biological samples are distributed equally between IARC and local storage, and are stored in straws at 2 1968C.
‡ In France, 66 858 EPIC participants living near a metropolitan area were asked to give blood.
§ In Bilthoven, 13 451 EPIC participants recruited from Amsterdam or Doetinchem after 11 May 1993, and 7364 EPIC participants recruited from Maastricht
after 2 June 1993, were asked to donate blood.
{ In Cambridge (UK), 25 633 EPIC participants who attended a study exam were asked to give blood.
k In Oxford (UK), enrolment of the participants recruited by general practitioners from the local counties was based on a willingness to donate blood and the
achievement rate is 96.1%; among the ‘health-conscious’ sub-cohort, 24.4% donated blood.
** In Norway, collection of biological samples is currently underway and will continue until samples have been collected from 12 000 participants.
standardisation of clinical and pathological data on each ORACLE database, using the centre-specific variable
cancer site: Guidelines for Collection of End-point Data in names and formats as well as variable names and formats
the EPIC Study (IARC, 1998). In parallel, data on total and standardised across EPIC. Centre-specific data were
cause-specific mortality are collected at the EPIC study loaded into the ORACLE system, and transformed into
centres through mortality registries or active follow-up and the standard EPIC variables on which logical and
death-record collection. substantive quality control checks were then run.
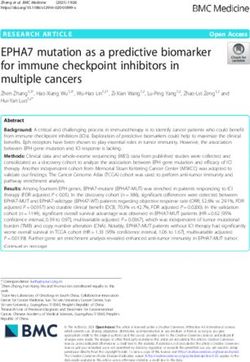
Figure 1 summarises the process.
Storage, management and quality control of the For dietary data, a common format and classification
EPIC database system was proposed to enable centralised data manage-
The EPIC data are housed centrally at IARC in the EPIC ment and a series of pooled analyses. The food items
ORACLE database. For practical reasons, 14 centres in the reported in each EPIC dietary questionnaire were
10 participating countries act as co-ordinating centres that classified in their respective food groups using the same
interact with IARC for centralisation of the EPIC data (in system as that used to classify the food items reported in
particular, all Spanish and Italian data are centralised in the EPIC-SOFT 24-hour dietary recalls (the so-called EPIC-
Barcelona and Milan, respectively). The database com- SOFT food classification system)35. However, other
prises individual EPIC data, as well as the computer classification criteria may be considered on an individual
software (ORACLE) and the programs that store, track and basis depending on the purposes of specific analyses. In
manage the database. addition, the frequency of consumption of each item, the
The EPIC core information concerning non-dietary number of portions consumed on each occasion and the
lifestyle variables and anthropometry is stored in the EPIC (standard) portion sizes were also stored in the central
Downloaded from https://www.cambridge.org/core. 03 Sep 2021 at 20:04:47, subject to the Cambridge Core terms of use.1122 E Riboli et al.
Fig. 1 Flow chart of lifestyle and personal data: the European Prospective Investigation into Cancer and Nutrition study
ORACLE database; hence, the total quantity of each food baseline information and biological samples have been
was calculated from this information as grams consumed collected, centralised and, when applicable, standardised.
per day. For the 24-hour dietary recalls, used as common As a large prospective cohort with stored biological
reference calibration measurements, the same standar- samples, EPIC is now starting to generate specific studies
dised software (i.e. EPIC-SOFT) methodology was used in investigating cancer aetiology in relation to diet and
all centres to collect and subsequently store, retrieve and lifestyle factors, and this will continue over the next 10
export these data. The same format file was therefore used years and beyond. When biological samples are involved,
to load and store the 24-hour dietary recall data in the these studies mostly use the nested case – control
central EPIC database. approach. In addition, information on vital status and
The storage, management and interrelationships cause of death can be used to address endpoints other
between the various components of the EPIC dietary than cancer, in particular cardiovascular diseases, as well
data are shown schematically in Fig. 2. as survival after cancer diagnosis.
Personal identifying information, as available at local The very magnitude of the individual and total cohorts,
centres, is not transferred to the IARC co-ordinating centre. the related lengthy period of subject recruitment and the
Informed consent was provided by each participant, and variety of local facilities have made it impossible to
projects using the EPIC resource need to be cleared by standardise all of the procedures strictly, as would be
both the IARC and local ethical review committees. possible for smaller studies. However, considerable effort
has been put into ensuring maximum comparability within
Concluding remarks and between cohorts, in particular where dietary
information is concerned, by means of the large
Approximately 10 years after its inception, the EPIC study calibration sub-sample. The storage of biological samples
Fig. 2 Flow chart of dietary data: the European Prospective Investigation into Cancer and Nutrition study
Downloaded from https://www.cambridge.org/core. 03 Sep 2021 at 20:04:47, subject to the Cambridge Core terms of use.EPIC study description 1123
in multiple aliquots in liquid nitrogen represents the best 3 Doll R, Payne P, Waterhouse J. Cancer Incidence in Five
Continents. Berlin: Springer, 1970.
available technology for maintaining long-term stability. 4 Armstrong B, Doll R. Environmental factors and cancer
A multi-centre cohort the size of EPIC offers the incidence and mortality in different countries, with special
substantial advantage of enabling informative studies on reference to dietary practices. Int. J. Cancer 1975; 15:
common cancers (as well as other common causes of 617 –31.
5 World Cancer Research Fund/American Institute of Cancer
deaths) not only overall but also in specific subsets of the
Research (WCRF/AICR). Food, Nutrition and the Prevention
total population, within which aetiological factors may of Cancer: A Global Perspective. Washington, DC:
differ. Also, sufficient numbers will accrue to enable WCRF/AICR, 1997.
meaningful investigation of rarer cancers. Finally, the 6 Riboli E. Nutrition and cancer: background and rationale of
the European Prospective Investigation into Cancer and
variations in disease rates, diet and lifestyles across the
Nutrition (EPIC). Ann. Oncol. 1992; 3: 783 – 91.
populations included in EPIC raise interesting methodo- 7 Riboli E. The European Prospective Investigation into
logical issues on the one hand and, on the other, the Cancer and Nutrition: perspectives for cancer prevention.
opportunity to capitalise simultaneously on the within- Nestle Nutr. Workshop Ser. Clin. Perform. Programme 2000;
4: 117–30.
and between-centre variability to increase the capacity of
8 Riboli E. The European Prospective Investigation into
the study to clarify the complex role of nutrition in the Cancer and Nutrition (EPIC): plans and progress. J. Nutr.
causation and prevention of cancer. 2001; 131: 170S –5S.
9 Riboli E, Kaaks R. The EPIC Project: rationale and study
design. European Prospective Investigation into Cancer and
Acknowledgements Nutrition. Int. J. Epidemiol. 1997; 26(Suppl. 1): S6– 14.
10 Riboli E, Kaaks R. Invited commentary: the challenge of
multi-center cohort studies in the search for diet and cancer
The work described in this paper was carried out with links. Am. J. Epidemiol. 2000; 151: 371 – 4.
financial support of the ‘Europe Against Cancer’ Pro- 11 Berglund G, Elmstahl S, Janzon L, Larsson SA. The Malmö
gramme of the European Commision (SANCO); Ligue Diet and Cancer Study. Design and feasibility. J. Intern. Med.
contre le Cancer (France); Société 3M (France); Mutuelle 1993; 233: 45– 51.
12 Clavel-Chapelon F, van Liere MJ, Giubout C, Niravong MY,
Générale de l’Education Nationale; Institut National de la Goulard H, Le Corre C, et al. E3N, a French cohort study on
Santé et de la Recherche Médicale (INSERM); Institute cancer risk factors. E3N Group. Etude Epidémiologique
Gustave Roussy; German Cancer Aid; German Cancer auprès de femmes de l’Education Nationale. Eur. J. Cancer
Research Centre; German Federal Ministry of Education Prev. 1997; 6: 473–8.
13 Hjartåker A, Lund E. Relationship between dietary habits,
and Research; Danish Cancer Society; Health Research age, lifestyle, and socio-economic status among adult
Fund (FIS) of the Spanish Ministry of Health; the Spanish Norwegian women. The Norwegian Women and Cancer
Regional Governments of Andalucia, Asturias, Basque Study. Eur. J. Clin. Nutr. 1998; 52: 565– 72.
Country, Murcia and Navarra; Cancer Research UK; 14 Boeing H, Wahrendorf J, Becker N. EPIC –Germany – a
source for studies into diet and risk of chronic diseases. Ann.
Medical Research Council, UK; Stroke Association, UK; Nutr. Metab. 1999; 43: 195–204.
British Heart Foundation; Department of Health, UK; Food 15 Boeing H, Korfmann A, Bergmann MM. Recruitment
Standards Agency, UK; Wellcome Trust, UK; Greek procedures of EPIC – Germany. European Investigation into
Ministry of Health; Greek Ministry of Education; Italian Cancer and Nutrition. Ann. Nutr. Metab. 1999; 43: 205–15.
16 Day N, Oakes S, Luben R, Khaw KT, Bingham S, Welch A,
Association for Research on Cancer; Italian National et al. EPIC– Norfolk: study design and characteristics of the
Research Council; Dutch Ministry of Public Health, Welfare cohort. European Prospective Investigation of Cancer. Br.
and Sports; Dutch Prevention Funds; LK Research Funds; J. Cancer. 1999; 80(Suppl. 1): 95– 103.
Dutch ZON (Zorg Onderzoek Nederland); World Cancer 17 Keinan-Boker L, van Noord PAH, van der Schouw YT, Koot
NVCM, Bueno-de-Mesquita HB, Riboli E, et al. Prospect –
Research Fund; Swedish Cancer Society; Swedish Scien- EPIC Utrecht: study design and characteristics of the cohort
tific Council; Regional Government of Skane, Sweden; population. Eur. J. Epidemiol. 2002; in press.
Norwegian Cancer Society; Norwegian Research Council. 18 Schulze MD, Kroke A, Saracci R, Boeing H. The effect of
Partial support for the publication of this supplement was measurement procedure differences on the comparability of
blood pressure estimates in multi-centre studies. Blood Press.
provided by the Centre de Recherche et d’Information Monit. 2000; 7: 95– 104.
Nutritionnelles (CERIN). 19 Overvad K, Tjønneland A, Haraldsdóttir J, Bang S, Ewertz M,
In addition, we wish to thank all study participants for Møller-Jensen O. Development of a semi-quantitative food
their co-operation and all interviewers who participated in frequency questionnaire to assess food, energy and nutrient
intake in Denmark. Int. J. Epidemiol. 1991; 20: 906 –12.
the fieldwork studies in each EPIC centre. 20 Bingham SA, Gill C, Welch A, Day K, Cassidy A, Khaw KT,
et al. Comparison of dietary assessment methods in
References nutritional epidemiology: weighted records v. 24 h recalls,
food-frequency questionnaires and estimated-diet records.
Br. J. Nutr. 1994; 72: 619 – 43.
1 Tannenbaum A. Initiation and growth of tumors; introduc- 21 Margetts BM, Pietinen P, Riboli E, eds. EPIC: European
tion: effects of underfeeding. Am. J. Cancer 1940; 39: Prospective Investigation into Cancer and Nutrition: validity
335 – 50. studies on dietary assessment methods [special issue]. Int.
2 Doll R, Payne P, Waterhouse J. Cancer Incidence in Five J. Epidemiol. 1997; 26(Suppl. 1): S1–189.
Continents: A Technical Report. Berlin: Springer, 1966. 22 Riboli E, Elmståhl S, Saracci R, Gullberg B, Lindgärde F. The
Downloaded from https://www.cambridge.org/core. 03 Sep 2021 at 20:04:47, subject to the Cambridge Core terms of use.1124 E Riboli et al.
Malmö Food Study: validity of two dietary assessment multicenter cohort studies on diet and cancer: a calibration
methods for measuring nutrient intakes. Int. J. Epidemiol. approach. Am. J. Clin. Nutr. 1994; 59: 245S – 50S.
1997; 26: S161 – 71. 29 Kaaks R, Riboli E, Esteve J, van Kappel AL, van Staveren WA.
23 Kroke A, Klipstein-Grobusch K, Voss S, Moseneder J, Estimating the accuracy of dietary questionnaire assess-
Thielecke F, Noack R, et al. Validation of a self-administered ments: validation in terms of structural equation models.
food-frequency questionnaire administered in the European Stat. Med. 1994; 13: 127– 42.
Prospective Investigation into Cancer and Nutrition (EPIC) 30 Kaaks R, Riboli E, van Staveren W. Sample size requirements
Study: comparison of energy, protein, and macronutrient for calibration studies of dietary intake measurements in
intakes estimated with the doubly labeled water, urinary prospective cohort investigations. Am. J. Epidemiol. 1995;
nitrogen, and repeated 24-h dietary recall methods. Am. 142: 557 – 65.
J. Clin. Nutr. 1999; 70: 439 –47. 31 Kaaks R, Riboli E, van Staveren W. Calibration of dietary
24 Slimani N, Deharveng G, Charrondière RU, van Kappel AL, intake measurements in prospective cohort studies. Am.
Ocké MC, Welch A, et al. Structure of the standardized J. Epidemiol. 1995; 142: 548 – 56.
computerized 24-h diet recall interview used as reference 32 Slimani N, Charrondière UR, van Staveren W, Riboli E.
method in the 22 centers participating in the EPIC project. Standardization of food composition databases for the
European Prospective Investigation into Cancer and Nutri-
European Prospective Investigation into Cancer and Nutri-
tion. Comput. Meth. Programs Biomed. 1999; 58: 251– 66.
tion (EPIC): general theoretical concept. J. Food Comp. Anal.
25 Slimani N, Ferrari P, Ocké M, Welch A, Boeing H, Liere M,
2000; 13: 567 –84.
et al. Standardization of the 24-hour diet recall calibration
method used in the European Prospective Investigation into 33 Charrondière UR, Vignat J, Møller A, Ireland J, Becker W,
Cancer and Nutrition (EPIC): general concepts and Church S, et al. The European Nutrient Database (ENDB) for
preliminary results. Eur. J. Clin. Nutr. 2000; 54: 900 – 17. nutritional epidemiology. J. Food Comp. Anal. 2002; 15(4):
26 Slimani N, Kaaks R, Ferrari P, Casagrande C, Clavel-Chapelon 435 – 51.
F, Lotze G, et al. European Prospective Investigation into 34 Haftenberger M, Lahmann PH, Panico S, González CA,
Cancer and Nutrition (EPIC) calibration study: rationale, Seidell JC, Boeing H, et al. Overweight, obesity and body fat
design and population characteristics. Public Health Nutr. distribution in 50- to 64-year-old participants in the
2002; 5(6B): 1125 –45. European Prospective Investigation into Cancer and Nutri-
27 Kaaks R, Riboli E. Validation and calibration of dietary intake tion (EPIC). Public Health Nutr. 2002; 5(6B): 1147 – 62.
measurements in the EPIC project: methodological con- 35 Ireland J, van Erp-Baart AMJ, Charrondière UR, Møller A,
siderations. European Prospective Investigation into Cancer Smithers G, Trichopoulou A, for the EFCOSUM Group.
and Nutrition. Int. J. Epidemiol. 1997; 26(Suppl. 1): S15 – 25. Selection of a food classification system and a food
28 Kaaks R, Plummer M, Riboli E, Esteve J, van Staveren W. composition database for future food consumption surveys.
Adjustment for bias due to errors in exposure assessments in Eur. J. Clin. Nutr. 2002; 56(Suppl. 2): S33 – 45.
Downloaded from https://www.cambridge.org/core. 03 Sep 2021 at 20:04:47, subject to the Cambridge Core terms of use.You can also read