European Heart Rhythm Association (EHRA)/Heart Rhythm Society (HRS)/Asia Pacific Heart Rhythm Society (APHRS)/Latin American Heart Rhythm Society ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

European Heart Rhythm Association (EHRA)/Heart
Rhythm Society (HRS)/Asia Pacific Heart Rhythm
Society (APHRS)/Latin American Heart Rhythm
Society (LAHRS) expert consensus on arrhythmias and
cognitive function: what is the best practice?
Nikolaos Dagres (EHRA Chair),1,* Tze-Fan Chao (APHRS Co-Chair),2
Guilherme Fenelon (LAHRS Co-Chair),3 Luis Aguinaga,4 Daniel Benhayon,5
Emelia J. Benjamin,6 T. Jared Bunch,7 Lin Yee Chen,8 Shih-Ann Chen,2
Francisco Darrieux,9 Angelo de Paola,10 Laurent Fauchier,11 Andreas Goette,12
Jonathan Kalman,13 Lalit Kalra,14 Young-Hoon Kim,15 Deirdre A. Lane,16,17
Gregory Y.H. Lip,16,17 Steven A. Lubitz,18 Manlio F. Marquez,19 Tatjana Potpara,20,21
Domingo Luis Pozzer,22 Jeremy N. Ruskin,18 Irina Savelieva,23 Wee Siong Teo,24
Hung-Fat Tse,25 Atul Verma,26 Shu Zhang,27 Mina K. Chung (HRS Co-Chair)28
Reviewers: William-Fernando Bautista-Vargas (Colombia), Chern-En Chiang (Taiwan),
Alejandro Cuesta (Uruguay), Gheorghe-Andrei Dan (Romania), David S. Frankel (USA),
Yutao Guo (People’s Republic of China), Robert Hatala (Slovakia), Young Soo Lee (Republic
of Korea), Yuji Murakawa (Japan), Cara N. Pellegrini (USA), Claudio Pinho (Brazil), David J.
Milan (USA), Daniel P. Morin (USA), Elenir Nadalin (Brazil), George Ntaios (Greece), Mukund
A. Prabhu (India, Australia), Marco Proietti (UK, Italy), Lena Rivard (Canada), Mariana
Valentino (Argentina), and Alena Shantsila (Reviewer Coordinator) (UK)
From the 1Department of Electrophysiology, Heart Center Leipzig, Str€umpellstr. 39, 04289 Leipzig, Germany,
2
Taipei Veterans General Hospital, Taipei, Taiwan, 3Hospital Israelita Albert Einstein, S~ao Paulo, Brazil,
4
Centro Privado de Cardiología, Tucum an, Argentina, 5Cardiac and Vascular Institute, Memorial Health,
6
Hollywood, FL, USA, Boston University Schools of Medicine and Public Health, Framingham Heart
Study, Boston, MA, USA, 7Intermountain Medical Center, Murray, UT, USA, 8Cardiovascular Division,
Department of Medicine, University of Minnesota, Minneapolis, MN, USA, 9University of Sao Paulo
Medical School, Sao Paulo, Brazil, 10Escola Paulista de Medicina, Universidade Federal de S~ao Paulo,
S~ao Paulo, Brazil, 11Service de Cardiologie, Centre Hospitalier Universitaire Trousseau, Université
François Rabelais, Tours, France, 12Department of Cardiology and Intensive Care Medicine, St.
Vincenz-Hospital Paderborn, Working Group: Molecular Electrophysiology, University Hospital
Magdeburg, Germany, 13University of Melbourne, Royal Melbourne Hospital, Melbourne, Victoria,
Australia, 14King’s College London, London, UK, 15Korea University Medical Center, Seoul, Republic of
Korea, 16Institute of Cardiovascular Sciences, University of Birmingham, Birmingham, UK,
KEYWORDS Arrythmias; Asia Pacific Heart Rhythm Society; Cognitive; De- differences in keeping with each journal’s style. Either citation can be
mentia; European Heart Rhythm Association; Heart Rhythm Society; Latin used when citing this article. For copies of this document, please contact
American Heart Rhythm Society (Heart Rhythm 2018;-:e1–e24) the Elsevier Inc. Reprint Department (reprints@elsevier.com). Permis-
Developed in partnership with and endorsed by the European Heart sions: Multiple copies, modification, alteration, enhancement, and/or
Rhythm Association (EHRA), a registered branch of the European distribution of this document are not permitted without the express
Society of Cardiology (ESC); the Heart Rhythm Society (HRS); the Asia permission of the Heart Rhythm Society. Instructions for obtaining
Pacific Heart Rhythm Society (APHRS); and the Latin American Heart permission are located at https://www.elsevier.com/about/our-business/
Rhythm Society (LAHRS). This article has been co-published with policies/copyright/permissions. * Corresponding author: Dr Nikolaos
permission in EP Europace, HeartRhythm, and Journal of Arrhythmia. Dagres, Department of Electrophysiology, Heart Center Leipzig, Str€umpellstr. 39,
The articles are identical except for minor stylistic and spelling 04289 Leipzig, Germany. E-mail address: dagresnikolaos@gmail.com.
1547-5271/$-see front matter © 2018 The European Heart Rhythm Association, a registered branch of https://doi.org/10.1016/j.hrthm.2018.03.005
the European Society of Cardiology; the Heart Rhythm Society; the Asia Pacific Heart Rhythm
Society; and the Latin American Heart Rhythm Society (formerly SOLAECE). All rights reserved.
PGL 5.5.0 DTD HRTHM7508_proof 16 March 2018 1:12 am ce
e2 Heart Rhythm, Vol -, No -, - 2018
17
Aalborg Thrombosis Research Unit, Department of Clinical Medicine, Aalborg University, Aalborg,
Denmark, 18Massachusetts General Hospital, Boston, MA, USA, 19Department of Electrocardiography,
Instituto Nacional De Cardiologia, Mexico City, Mexico, 20School of Medicine, Belgrade University,
Belgrade, Serbia, 21Cardiology Clinic, Clinical Center of Serbia, Belgrade, Serbia,
22
Instituto de Cardiología de Corrientes, Corrientes, Argentina, 23Cardiology Clinical Academic Group,
Molecular and Clinical Sciences Research Institute, St. George’s University of London, London, UK,
24
National Heart Centre, Singapore, Singapore, 25Department of Medicine, The University of Hong Kong,
Hong Kong, China, 26Southlake Regional Health Centre, Ontario, Canada, 27Beijing Fuwai Hospital,
Beijing, People’s Republic of China, and 28Cleveland Clinic, Cleveland, OH, USA.
TABLE OF CONTENTS procedures and cognitive function ....... e15
Current knowledge gaps, future directions,
and areas for research ................................. e18
Table of Contents ........................................ e2 Recommendations ....................................... e18
Introduction ................................................. e2 Supplementary material .............................. e20
Evidence review ....................................... e3 References ..................................................... e20
Relationships with industry and other
conflicts .................................................... e3
Decline of cognitive function: terminology Introduction
and epidemiology ......................................... e3 This expert consensus statement of the European Heart
Terminology: cognitive decline, mild Rhythm Association (EHRA), Heart Rhythm Society
cognitive impairment, and dementia .... e3 (HRS), Asia Pacific Heart Rhythm Society (APHRS), and
Epidemiology of dementia ..................... e4 the Latin American Heart Rhythm Society (LAHRS) summa-
Methods for assessment of cognitive rizes the consensus of the international writing group and is
function ......................................................... e4 based on a thorough review of the medical literature regarding
Role of imaging ........................................... e4 cognitive function in arrhythmias. The document is intended
Atrial fibrillation and cognitive function ... e5 to describe the impact of different types of arrhythmias on
Atrial fibrillation, overt stroke, and cognitive function, to highlight possible risk markers for
cognitive function ................................... e5 cognitive decline and to formulate implications for clinical
Atrial fibrillation, silent stroke, and practice regarding follow-up methods, prevention and treat-
cognitive function ................................... e8 ment strategies. Our objective is to raise awareness of cogni-
Atrial fibrillation and cognitive function tive function among physicians treating patients with
in the absence of stroke ......................... e9 arrhythmias and to provide them with practical proposals
Assessment of cognitive function in that may lead to improvement of patient care in this regard.
atrial fibrillation patients in clinical This document reviews terminology and the epidemi-
practice ..................................................... e9 ology of cognitive dysfunction, methods for assessment of
Prevention of cognitive dysfunction in cognitive function and the role of imaging. Recent studies
atrial fibrillation patients ....................... e10 have suggested possible associations between cognitive
Other arrhythmias and cognitive decline and atrial fibrillation (AF). We review the reported
dysfunction ................................................... e12 literature on AF and cognitive function, including the sce-
Cognitive dysfunction in patients with narios of AF with overt stroke, silent stroke, or no stroke,
regular supraventricular tachycardias .. e12 and then make recommendations for assessment of cognitive
Cognitive impairment after cardiac function and prevention of cognitive decline in patients with
arrest ......................................................... e12 AF in clinical practice. The document also reviews the asso-
Brain injury after non-fatal cardiac ciation of other arrhythmias and cognitive dysfunction,
arrest .................................................... e12 including settings such as post-cardiac arrest, cardiac
Memory impairment after cardiac implantable devices, such as implantable cardioverter-
arrest .................................................... e13 defibrillators (ICDs) and pacemakers, or ablation procedures.
Therapeutic hypothermia to prevent Implications for electrophysiological procedures and cogni-
cognitive impairment after cardiac tive function are discussed. Long QT syndrome and cogni-
arrest .................................................... e13 tive function is not addressed in the document. For quick
Cardiac implantable electronic devices reference, sub-chapters are followed by a short section on
and cognitive dysfunction ...................... e13 consensus recommendations. The document concludes with
Catheter ablation .................................... e14 a summary of consensus statements, current knowledge
Implications for electrophysiological gaps, and future directions of research.
PGL 5.5.0 DTD HRTHM7508_proof 16 March 2018 1:12 am ceDagres et al EHRA/HRS/APHRS/LAHRS Expert Consensus on Arrhythmias and Cognitive Function e3
Evidence review supported by randomized trials based on a small number
Members of the Task Force were asked to perform a detailed of patients or which is not widely applicable. Treatment
literature review, weigh the strength of evidence for or strategies for which there is scientific evidence of potential
against a particular treatment or procedure, and include esti- harm and should not be used (“do not do this”) are indicated
mates of expected health outcomes for which data exist. by a red heart.
Patient-specific modifiers, co-morbidities, and issues of pa- Finally, this is a consensus document that includes evi-
tient preference that might influence the choice of particular dence and expert opinions from several countries. The phar-
tests or therapies are considered, as are frequency of follow- macological and non-pharmacological antiarrhythmic
up and cost-effectiveness. In controversial areas, or with approaches discussed may, therefore, include drugs that do
regard to issues without evidence other than usual clinical not have the approval of governmental regulatory agencies
practice, a consensus was achieved by agreement of the in all countries.
expert panel after thorough deliberations. This document
was prepared by the Task Force with representation from Relationships with industry and other conflicts
EHRA, HRS, APHRS, and LAHRS. The document was All members of the writing group, as well as reviewers, have
peer-reviewed by official external reviewers representing disclosed any potential conflict of interest in detail and is
EHRA, HRS, APHRS, and LAHRS. available in Supplementary material online.
Consensus statements are evidence-based and derived All recommendations were voted upon by the writing
primarily from published data or determined through committee independently and reached 80% consensus for
consensus opinion if data are not available. Current systems inclusion in recommendations tables. Each partner society
of ranking level of evidence are becoming complicated in a officially reviewed the document and all reviewer comments
way that their practical utility might be compromised.1 In were addressed. The final document and recommendations
contrast to guidelines, we opted for an easier and user- were approved by each partner society.
friendly system of ranking using “colored hearts” that
should allow physicians to easily assess the current status
of the evidence and consequent guidance (Table 1). This Decline of cognitive function: terminology and
EHRA grading of consensus statements does not have sepa- epidemiology
rate definitions of the level of evidence. This categorization, Terminology: cognitive decline, mild cognitive
used for consensus statements, must not be considered as impairment, and dementia
directly similar to that used for official society guideline rec- Cognitive decline that is greater than expected from normal
ommendations, which apply a classification (Class I–III) aging can be ascertained from changes in standardized cogni-
and level of evidence (A, B, and C) to recommendations tive test scores over time. Examples of standardized cognitive
used in official guidelines. tests that evaluate different cognitive domains include De-
Thus, a green heart indicates a “should do this” consensus layed Word Recall test (short-term memory),2 Digit Symbol
statement or indicated treatment or procedure that is based on Substitution test (executive function and processing speed),3
at least one randomized trial, or is supported by strong obser- and Word Fluency test (executive function and expressive
vational evidence that it is beneficial and effective. A yellow language).4
heart indicates general agreement and/or scientific evidence Mild cognitive impairment is an intermediate stage be-
favoring a “may do this” statement or the usefulness/efficacy tween the expected cognitive decline of normal aging and
of a treatment or procedure. A “yellow heart” symbol may be the more serious abnormality of dementia. Mild cognitive
Table 1 Scientific rationale of recommendations*
Definitions related to a treatment or procedure Consensus statement instruction Symbol
Scientific evidence that a treatment or procedure is beneficial and effective. Requires “Should do this”
at least one randomized trial, or is supported by strong observational evidence and
authors’ consensus (as indicated by an asterisk).
General agreement and/or scientific evidence favor the usefulness/efficacy of a “May do this”
treatment or procedure. May be supported by randomized trials based on a small
number of patients or which is not widely applicable.
Scientific evidence or general agreement not to use or recommend a treatment or “Do not do this”
procedure.
*This categorization for our consensus document should not be considered as being directly similar to that used for official society guideline recommendations,
which apply a classification (I–III) and level of evidence (A, B, and C) to recommendations.
PGL 5.5.0 DTD HRTHM7508_proof 16 March 2018 1:12 am cee4 Heart Rhythm, Vol -, No -, - 2018
impairment is characterized by declines in cognitive function For assessment of cognitive impairment, a combination of
and objective long-term cognitive deficit that does not affect tools and methods are used (Table 3).
activities of daily living.5 During the assessment, particular attention needs to be
Dementia is defined as deficits in 2 cognitive domains paid to aspects such as vagueness with dates and events, repe-
that represent a decline from previous level of functioning tition, inappropriate, or fixed ideas. A collateral account from
and that are sufficiently severe to affect activities of daily a caregiver can provide clarification of symptoms and their
living. Both mild cognitive impairment and dementia can duration. Specific areas requiring attention include features
be further classified into subtypes.6 Mild cognitive impair- of depression, neurological or psychiatric diseases, drug/
ment can be sub-typed into four groups (based on the scheme medication use, uncorrected visual and hearing problems, in-
adopted by the National Institute on Aging Alzheimer’s Dis- fections, cardiac/respiratory/renal failure, or fast AF, all of
ease Centers Program for the Uniform Data Set) as amnestic which potentially affect cognitive function. Investigations
or non-amnestic, single or multiple domain.5 Dementia can include complete blood count, blood glucose, creatinine,
be classified into etiologic diagnoses: Alzheimer’s disease, electrolytes, calcium, liver and thyroid function tests, serum
vascular dementia, Lewy body dementia, frontotemporal de- folate, and B12 levels. Syphilis serology should be checked
mentia, and other dementias.6 in high-risk patients. Magnetic resonance imaging can be
helpful to estimate cerebrovascular and degenerative disease
Epidemiology of dementia load and exclude tumours or normal pressure hydrocephalus.
A recent systematic review provided some insights into the A list of cognitive assessment tools is provided in Table 4.
contemporary (1980–2009) prevalence of dementia in indi- Several tools are available for cognitive assessment, but there
viduals aged 60 years in 21 Global Burden of Disease re- is no consensus on a preferred approach. The choice of tool
gions: age-standardized prevalence for those aged should vary with the purpose of testing and other factors,
60 years varied in a narrow band (5–7% in most world re- such as availability, familiarity, and feasibility.48 Common
gions), with a higher prevalence in Latin America (8.5%), assessment tools are the two-step general practitioner assess-
and a lower prevalence in the four sub-Saharan African re- ment of cognition (GPCOG) and the Informant Question-
gions (2–4%).7 Approximately 35.6 million people lived naire for Cognitive Decline in the Elderly (IQCODE), both
with dementia worldwide in 2010, with numbers expected of which have been validated in large populations.49–51
to almost double every 20 years, to 65.7 million in 2030 Standardized assessment tools are not diagnostic
and 115.4 million in 2050.7 In 2010, 58% of all people instruments and results need to be interpreted in the context
with dementia lived in countries with low or middle incomes, of all available evidence.
with this proportion anticipated to rise to 63% in 2030 and
71% in 2050.7 Thus, dementia is a burgeoning global public
health problem that prompts an urgent and more comprehen- Role of imaging
sive understanding of its risk factors with the aim to discover Brain imaging studies can identify vascular disease as a cause
novel prevention strategies. of dementia. In an autopsy study of patients with dementia,
The burden of dementia is rapidly increasing owing to the pathologic diagnoses implicated vascular disease in about
aging of the population. Other than advancing age, risk fac- 25% of subjects, half of whom had pure vascular disease.52
tors for dementia, particularly vascular dementia, have been The three main causes of vascular cognitive impairment are
extensively studied from an epidemiological perspective. large vessel strokes, small vessel disease (SVD), and
Broadly, they can be classified as dementia due to non- micro-hemorrhages. The preferred imaging modality, mag-
modifiable risk factors, lifestyle factors, physiological risk netic resonance imaging (MRI), has high specificity and
factors, or clinical cardiovascular or cerebrovascular disease. sensitivity for detecting these changes and is an important
Selected risk factors are shown in Table 2 and include many adjunct to clinical and psychometric assessments. However,
of the risk factors included in stroke risk scores in AF. imaging findings need to be interpreted in the clinical context
because of uncertain correlation with symptoms or psycho-
metric test performance.53
Methods for assessment of cognitive function Structural imaging is undertaken using T1- and T2-
Impairments of cognitive function often can be subtle and weighted spin echo sequences to identify infarcts and
insidious, presenting as missed appointments, mislaying ob- macro-hemorrhages, T2*-weighted gradient echo sequences
jects, or minor problems at work or home, which are often for micro-hemorrhages, fluid-attenuated inversion recovery
attributed to stress, age, or pressure of work. Any difference imaging for incomplete infarcts and leukoaraiosis and
in appearance, behavior or functioning reported by the pa- diffusion-weighted imaging (DWI) for visualising the integ-
tient or the family should alert the physician to the need for rity of functional network fiber tracts not captured by other
a formal assessment. The aim of this assessment is to imaging techniques. Magnetic resonance imaging provides
examine higher cortical functions (attention, orientation, several markers of micro- and macrostructural organization
memory, language, praxis, and executive function) from pa- that are sensitive to change, related to clinical endpoints
tient narrative, collateral information from families, clinical and has the potential to predict cognitive trajectories in indi-
examination, and standardized tests of cognitive function.30 vidual patients.53
PGL 5.5.0 DTD HRTHM7508_proof 16 March 2018 1:12 am ceDagres et al EHRA/HRS/APHRS/LAHRS Expert Consensus on Arrhythmias and Cognitive Function e5
Table 2 Selected risk factors for dementia
Comments
Non-modifiable risk factors
Demographic factors
Age Dementia prevalence increases exponentially with age8
Sex Dementia prevalence greater in women than men7
Ethnicity VaD risk greater in blacks than whites9
Genetic factors Genetic alterations may affect cognitive function, e.g. apolipoprotein E ε4 allele and ABCA7 are
associated with increased risk of AD; C9ORF72, MAPT, GRN gene mutations associated with
frontotemporal dementia; rs12007229 is associated with VaD10
Lifestyle factors
Education Lower education is associated with higher VaD risk11
Physical activity Increased physical activity is associated with lower risk of general dementia, Alzheimer’s dementia, and
VaD risk, which was attenuated with further adjustment for baseline cognitive, psychosocial, and
vascular factors. Review reported that seven out of eight studies found an association between
increased physical activity and lower risk of cognitive decline12
Body mass index U-shaped association between body mass index and dementia, with dementia risk higher in individuals
who were obese or underweight13
Smoking Meta-analysis reported that current smokers have higher risk of cognitive decline and dementia over
follow-up, than non-smokers or former smokers14
Social support and networks Compared with small social networks, larger social networks were associated with a lower risk of incident
dementia over time.15
Cardiovascular risk factors
Blood pressure Higher mid-life blood pressure was associated with higher dementia risk16 and cognitive decline17
Blood glucose Diabetes was associated with increased dementia risk18 and cognitive decline19
Lipids Higher total serum cholesterol was associated with higher VaD and AD risk20,21
Clinical cardiovascular or cerebrovascular disease
Stroke Stroke is associated with increased dementia risk22,23
AF AF is associated with increased dementia risk24,25
Vascular/peripheral Carotid arterial disease is associated with incident dementia risk and cognitive decline26,27
arterial disease Lower ankle brachial index is associated with increased dementia risk28
Sleep apnea Sleep-disordered breathing is associated with an increased risk of cognitive impairment and a small
worsening in executive function.29
ABCA7, ATP-binding cassette transporter A7; AD, Alzheimer’s disease; AF, atrial fibrillation; C9ORF72, chromosome 9 open reading frame 72; GRN, granulin;
MAPT, microtubule-associated protein tau; VaD, vascular dementia.
Magnetic resonance imaging signs that predict potential Atrial fibrillation and cognitive function
cognitive impairments include (i) large or bilateral infarcts Atrial fibrillation, overt stroke, and cognitive
due to large vessel disease; (ii) strategic infarcts secondary function
to embolization in regions as hippocampus, dominant thal- Evidence suggests that AF is associated with a higher risk for
amus, medial temporal, and deep frontal; (iii) lacunes, white cognitive impairment and dementia, with or without a history
matter hyperintensities (leukoaraiosis) and hemorrhages of clinical stroke. Two meta-analyses that included both cross-
associated with SVD; and (iv) lobar micro-hemorrhages sectional and prospective studies specifically examined the
representative of amyloid angiopathies. In addition, although incidence of dementia in patients with AF and strokes.24,25
global cerebral atrophy and/or medial-temporal lobe atrophy These meta-analyses found similar estimates of the risk ratios
may suggest an element of Alzheimer’s disease (mixed of cognitive impairment or dementia of 2.4324 and 2.7025
cognitive impairment), subcortical infarcts, per se, may (Table 6).
trigger progressive focal thinning and grey matter atrophy It is uncertain whether or not the risk of cognitive impair-
in connected temporal and frontal cortical areas.48 ment and dementia varies in paroxysmal compared with
Imaging of cerebral blood flow using arterial spin labelling,
metabolic imaging with proton magnetic resonance spectros- Table 3 Assessment of cognitive impairment
copy and dynamic contrast-enhanced MRI can help estimate Suspect Patient history, appearance, changes in behavior
the extent of injury, vessel permeability, and inflammation. Confirm Collateral history from family
Although these can differentiate between dementias and sepa- Examine Full medical examination, brief screening assessment
rate pathological changes from those due to aging, they remain Investigate Renal/liver/respiratory/thyroid compromise, B12,
folate; syphilis serology (in high-risk patients)
research techniques with limited clinical application. Exclude Depression, neurological/psychiatric disease,
Positron emission tomography scans have also been used to medication/drug use
assess brain metabolic function, inflammation, amyloid or tau Measure Psychometric testing using validated battery
protein, which may be helpful in differentiating some types of Image Multimodal MRI (T1, T2, T2*, DWI) for brain changes
dementia.53 An overview of commonly used imaging modal- Establish Diagnosis based on clinical 1 psychometric 1 imaging
ities in cognitive impairment is provided in Table 5. DWI, diffusion-weighted imaging; MRI, magnetic resonance imaging.
PGL 5.5.0 DTD HRTHM7508_proof 16 March 2018 1:12 am cee6
Table 4 Comparison of commonly used brief cognitive assessment tools and a list of more complex cognitive assessments
Range
Average Cognitive domains assessed of scores*
completion time
Cognitive in elderly (65 Memory Visuospatial/
assessment Number years) patients, constructional Frontal/ Attention/ Informant Cut-off indicating
tool of items minutes Equipment required Semantic STM Remote praxis executive Orientation calculation Language component cognitive impairment†
AMT4 31
4 1 Verbal 2 2 1 2 2 1 2 2 2 0–4*
CDT32 3 2 Pen and paper 1 2 2 11 1 2 1 2 2 0–3*
SIS33 6 2 Verbal 2 1 2 2 2 1 2 2 2 0–6*
333,† 434,†
PGL 5.5.0 DTD HRTHM7508_proof 16 March 2018 1:13 am ce
Mini-Cog35 6 3 Pen and paper 1 1 2 11 1 2 1 2 2 0–5*
,4†
AMT31 10 3 Verbal 1 1 1 2 2 11 11 2 2 0–10*
,8†
MIS36 4 4 Verbal 2 1 2 2 2 2 2 2 2 0–8*
4†
6CIT37 6 5 Verbal 2 11 2 2 2 11 11 2 2 0–28*
8†
GPCOG38 9 5–6 Pen and paper 1 11 2 11 1 1 1 2 1 0–9*
0–4†; 5–8 proceed with
InQ
MMSE39,z 30 8 Pen, paper, and watch 2 1 2 1 2 111 11 11 2 0–30*
,24z (23 if 12
years education;
25 if higher
education)
MOCA40 30 10 Pen and paper 2 11 2 111 11 111 111 111 2 0–30*
,26†; add 1 point if
12 years education
OCS41 10 tasks 15–20 Pen and paper 1 111 11 111 111 111 111 111 2 21 to 111*
ACE42 100 20 Pen, paper, watch and 11 111 11 111 11 111 11 111 2 ,87†
specific pictures
Heart Rhythm, Vol -, No -, - 2018
More complex and extended cognitive examinationsx
3MS43: extension of MMSE including verbal fluency and further memory testing; overall score 0–100; score ,78 for those aged 65 years
CAMCOG44: 80 min, structured history taking from patient and informant, structured examination and mental state assessment
CASI45: questions form MMS and 3MS; scored 0–100 takes 15–20 min to complete
IQCODE46: 16-item informant questionnaire comparing patient cognition now to 10-years ago; each rated on five-point Likert scale
2, not specifically tested; 1, minimal assessment; 11, moderate assessment; 111, relatively extensive assessment; 3MS, Modified Mini Mental Status Examination; 6CIT, 6-item Cognitive Impairment Test; ACE,
Addenbrooke’s Cognitive Examination; AMT, Abbreviated Mental Test; CAMCOG, Cambridge Cognitive Examination; CASI, Cognitive Abilities Screening Instrument; CDT, Clock-Drawing Test; GPCOG, general practitioner
assessment of cognition; InQ, Informant Questionnaire; IQCODE, Informant Questionnaire for Cognitive Decline in the Elderly; MIS, Memory Impairment Screen; MMSE, Mini Mental State Examination; MOCA, Montreal
Cognitive Assessment; OCS, Oxford Cognitive Screen; SIS, Six-Item Screener; STM, short-term memory.
*Range of scores.
†
Cut-off indicating cognitive impairment.
z
Standardized MMSE is also available.
x
Not an exhaustive list.
Adapted from Woodford and George.47Dagres et al EHRA/HRS/APHRS/LAHRS Expert Consensus on Arrhythmias and Cognitive Function e7
Table 5 Commonly used brain imaging modalities in cognitive interest, the Framingham Heart Study has examined temporal
impairment trends in the incidence of dementia and noted that the risk of
Modality Use dementia associated with AF declined over three decades
(1970s to the early 2010s).58 One speculation is that
CT Large infarcts/hemorrhage, established small improved anticoagulation and treatment of risk factors were
vessel disease, other pathologies, limited
application
responsible for the declining incidence of dementia in indi-
MRI Imaging of choice for assessment of cognitive viduals with AF. Another piece of inferential evidence, sup-
impairment54 porting the benefit of preventing stroke as a strategy to
T1 and T2 MRI Highly sensitive to old and new infarcts, prevent dementia in individuals with AF, are observational
estimation of white matter disease load, meta-analyses (Table 6). In individuals with AF but without
other pathologies (e.g. malignancies,
cerebral edema)
stroke at baseline the risk of dementia and cognitive decline is
T2* MRI Blood and blood products (e.g. hemorrhages), more modest [relative risk (RR) 1.37, 95% confidence inter-
micro-hemorrhages, hemosiderin val (CI) 1.08–1.73] than in individuals with both AF and a
deposition, amyloid angiopathies history of stroke (RR 2.7, 95% CI 1.82–4.00).25
DWI MRI Extremely sensitive to early ischemic changes Systemic anticoagulation remains the cornerstone of
(recent infarcts including micro-infarcts),
integrity of fiber tracts, extensively used for
stroke prevention treatment. By meta-analysis, adjusted-
tractography assessing the structural dose warfarin is associated with a 64% (95% CI 49–74%)
integrity of connecting white matter tracts significantly lower risk of stroke (Table 7), whereas aspirin
1H-MRS Measurement of neuronal damage, alone was associated with a 19% (95% CI 21 to 35%)
inflammation, gliosis, differentiation non-significant lower stroke risk.59 In studies comparing
between pathology and normal aging
warfarin and aspirin, warfarin was associated with a 38%
1H-MRS, proton magnetic resonance spectroscopy; CT, computed tomog- (95% CI 18–52%) stroke reduction, when compared with
raphy; DWI, diffusion-weighted imaging; MRI, magnetic resonance imaging. aspirin alone.59
A meta-analysis of the four randomized trials comparing
persistent AF. Many of the studies examining AF type were the non-vitamin K antagonist oral anticoagulants (NOACs)
small and underpowered and the factors that impact progres- to warfarin, demonstrated that the NOACs were associated
sion, such as rhythm control approaches and physician with a significant risk reduction (RR 0.81, 95% CI 0.73–
approach to the patient management, can introduce study 0.91) in overall stroke and systemic emboli, in part driven
biases. In a small hypothesis generating cross-sectional study by the significant risk reduction (RR 0.48, 95% CI 0.39–
from the Atherosclerosis Risk in Communities (ARIC) 0.59) in hemorrhagic stroke.60
Cohort55 persistent but not paroxysmal AF classified by Since a prior stroke represents the strongest predictor of
ambulatory telemetry monitoring was associated with lower stroke recurrence, all patients who have AF and have had
cognitive function. Another small cross-sectional study re- an ischemic stroke should be anticoagulated, unless an abso-
ported that cognitive performance did not significantly differ lute contraindication exists.61 Of interest, a recent observa-
by AF burden, but the number of subclinical cerebral tional study using a propensity score-matched analysis
ischemia areas was higher in individuals with persistent reported that in individuals with a history of AF and demen-
compared with paroxysmal AF.56 More conclusive under- tia, persistent use of warfarin therapy was uncommon (16%),
standing of the relation of AF burden to cognitive decline but was associated with the prevention of stroke [hazard ratio
and dementia will require larger and longitudinal studies. (HR) HR 0.74, 95% CI 0.54–0.996; P 5 0.047] and death
The relation between AF type and cognitive impairment (HR 0.72, 95% CI 0.67–0.87; P , 0.001).62 A recent updated
and dementia is further complicated by the sometimes arbi- meta-analysis reported a significant reduction of stroke,
trary definition of the AF type in the individual patient. stroke or systemic embolism, hemorrhagic stroke, and intra-
Unfortunately there are no randomized data examining the cranial bleeding in AF patients with previous stroke or tran-
efficacy of therapies and in particular of individualized man- sient ischemic attack (TIA) receiving NOACs compared with
agement to prevent dementia in individuals with AF.57 Of warfarin.63
Table 6 Meta-analyses relating atrial fibrillation to dementia and cognitive impairment
Author Study design Outcome Inclusions/exclusions Risk
24
Kwok et al. Meta-analysis cross-sectional Dementia Patients with H/o stroke, OR 2.43; 95% CI 1.70–3.46;
and prospective studies 7 studies; n 5 2425 P , 0.001; I2 5 10%
Kalantarian et al.25 Meta-analysis cross-sectional Cognitive impairment Patients with H/o stroke, RR 2.70; 95% CI 1.82–4.00;
and prospective studies and dementia 7 studies; n 5 2409 I2 5 32.3%; P 5 0.18
Excluding patients with or RR 1.34; 95% CI 1.13–1.5
adjusting for H/o stroke
10 studies
H/o, history of; OR, odds ratio; RR, relative risk.
PGL 5.5.0 DTD HRTHM7508_proof 16 March 2018 1:13 am cee8 Heart Rhythm, Vol -, No -, - 2018
Table 7 Meta-analyses examining anti-coagulation strategies in atrial fibrillation relating to stroke
Author Study design Outcome Inclusions/exclusions Risk
59
Hart et al. Meta-analysis adjusted-dose Stroke 6 RCTs warfarin vs. placebo;
RR 64% reduction, 95% CI 49–74%;
warfarin and aspirin n 5 2900 Absolute
reduction:
1 prevention 2.7% per year,
2 prevention 8.48% per year
7 RCTs aspirin vs. placebo or RR 19%
reduction, 95% CI 21 to 35%;
no Rx; n 5 3900 1 prevention 0.8% per year,
2 prevention 2.5% per year
8 RCTs warfarin vs. aspirin Rx; RR 38%
reduction, 95% CI 18–52%;
n 5 3647 1 prevention 0.7% per year,
2 prevention 7.0% per year
Ruff et al.60 Meta-analysis phase 3 RCTs: Stroke and systemic n 5 29 312 NOAC; n 5 29 272 RR 0.81, 95% CI 0.73–0.91; P , 0.0001;
emboli warfarin I2 5 47%; P 5 0.13
RE-LY, ROCKET AF, n 5 41 257, no prior stroke; RR 0.85, 95% CI 0.72–1.01
ARISTOTLE, ENGAGE n 5 17 269, prior stroke RR 0.89; 95% CI 0.77–1.02;
AF–TIMI 48 Pinteraction 5 0.30
Ischemic stroke n 5 29 292 NOAC; n 5 29 221 RR 0.92, 95% CI 0.83–1.02; P 5 0.10;
warfarin I2 5 32%; P 5 0.22
Hemorrhagic stroke n 5 29 292 NOAC; n 5 29 221 RR 0.49, 95% CI 0.38–0.64; P , 0.0001;
warfarin I2 5 34%; P 5 0.21
H/o, history of; NOAC, non-vitamin K antagonist oral anticoagulant; RCT, randomized clinical trial; RR, relative risk.
Atrial fibrillation, silent stroke, and cognitive silent infarct distribution is similar to that seen in vascular
function dementia, in which most silent strokes affect frontal circuit
It is well established that AF increases the risk of clinical components (frontal cortex, basal ganglia, and thalamus)
stroke by four- to five-fold, and patients with a clinical his- that play an important role in executive functioning.73
tory of stroke are at increased risk of developing demen- Thus, the term “silent infarct” is probably a misnomer.
tia.64–67 However, AF is also associated with cognitive Because of their small size and location away from speech
dysfunction ranging from mild impairment to overt and motor centers, these micro-injuries do not cause clini-
dementia, independently of clinical stroke as well as cally apparent acute focal neurological deficits. However,
multiple shared risk factors.64,67 It is also well established with the accumulation of silent infarcts and associated repet-
that AF and cognitive impairment share common risk itive brain injuries over time, micro-injuries may contribute
factors, including advanced age, diabetes, hypertension, to the development of cognitive impairment. At least one
sleep apnea, and chronic heart failure. Moreover, data have study has specifically addressed the role of subclinical cere-
demonstrated a significant (34%) increase in the risk of brovascular disease as a mediator between AF and cognitive
cognitive impairment in patients with AF in the absence of impairment. In a subset of stroke-free participants in the
clinical stroke, even after adjustment for shared risk ARIC study who underwent repeat brain MRI after approxi-
factors.25,64 Thus, additional mechanisms beyond clinically mately 12 years, AF was associated with cognitive decline
recognized stroke and shared risk factors may link AF and only in those patients who had developed incident silent ce-
cognitive impairment. One of the leading potential rebral infarcts.74
mechanisms is the occurrence of silent cerebral infarcts, There is a paucity of evidence regarding the effect of anti-
which occur significantly more frequently than clinical coagulation on silent cerebral infarcts and the risk of cogni-
stroke and are particularly common in patients with AF.68,69 tive impairment. One recent study addressed this issue by
Detection of cerebral ischemic events on MRI is based on evaluating the time in therapeutic range (TTR) as an indicator
acute hyperintense lesions on DWI. Brain MRIs reveal evi- of the effectiveness of warfarin anticoagulation in patients
dence of silent cerebral infarcts in a significant percentage with AF. These investigators observed a consistent increase
of patients with AF.69 The incidence is related to specifica- in the risk of dementia as the percentage of TTR decreased.75
tions of MRI and depends on the definition applied.70 Atrial The association between warfarin therapy and dementia was
fibrillation is associated with a more than two-fold increase in “U”-shaped, with increased risk of dementia among patients
the risk of developing silent cerebral infarcts.69 Although si- with overexposure and underexposure to warfarin [i.e. supra-
lent infarcts are not associated with clinically apparent acute therapeutic and sub-therapeutic international normalized ra-
neurologic deficits, data suggest a significant association be- tios (INRs)].75 This may be due to cumulative brain injury
tween silent infarcts and the development of cognitive from cerebral micro-bleeds and silent infarcts, respectively.
decline and dementia.56,71,72 Silent infarcts in patients with Recent observational data also suggest that delaying warfarin
AF are believed to be micro-embolic in origin and are iden- therapy in patients with AF and no history of dementia,
tified as small, well-demarcated lesions, often in clusters, including patients at low as well as high risk for stroke,
and are most prevalent in the frontal lobes.56 The pattern of significantly increases the risk for developing incident
PGL 5.5.0 DTD HRTHM7508_proof 16 March 2018 1:13 am ceDagres et al EHRA/HRS/APHRS/LAHRS Expert Consensus on Arrhythmias and Cognitive Function e9
dementia.12,76 Whether the use of the NOACs will offer of elderly patients with AF causing a specific atrial cardiomy-
greater protection than warfarin in preventing AF-related opathy classified as EHRAS IVa.90,91 However, if AF and
cognitive impairment and dementia remains to be deter- Alzheimer’s disease share a common link with regards to
mined. The significantly lower intracranial hemorrhage and protein misfolding and amyloidgenesis, it does not appear
micro-hemorrhage rates,77 the lower risk of mortality with to be through the APOE ε4 allele.92 Other studies suggest
intracranial hemorrhage with use of NOACs compared with that the occurrence of Alzheimer’s disease is related to hypo-
warfarin,78 coupled with comparable degrees of protection perfusion, inflammation, oxidative stress, and endothelial
against thromboembolic stroke and substantially lower vari- dysfunction.93–95 All these factors may be induced by
ability in therapeutic anticoagulation effect over time with several non-cardiac diseases resulting in an atrial cardiomy-
NOACs, offer reasons to hypothesize that these agents opathy which in turn, leads to AF91 in the sense of both AF
may be advantageous to warfarin regarding protection and Alzheimer’s disease being the result of third confounding
against cognitive impairment in patients with AF but this factors. Additionally, several circulating biomarkers of
requires confirmation. Initial findings seem to confirm this oxidative stress, inflammation, and endothelial dysfunction
hypothesis.79 are elevated during AF.91,96,97 These factors are also linked
to cerebral SVD; therefore, AF may provide a specific
Atrial fibrillation and cognitive function in the milieu for non-stroke related cognitive decline and dementia.
absence of stroke For example, hippocampal atrophy in AF patients may be
Longitudinal studies have shown that dementia is more com- mediated by altered cerebral perfusion due to irregular R-R
mon in patients diagnosed with AF80,81 even in the absence intervals, abnormal or rapid heart rate, and reduced blood
of stroke. A meta-analysis of eight prospective studies eval- pressure caused by AF, since the hippocampus is one of
uating the relationship between AF and incident dementia in the most perfusion-sensitive structures of the brain.94,98–101
patients without stroke and baseline normal cognitive func- Interestingly, patients with AF had lower total brain vol-
tion included a total of 77 668 patients of whom 15% had ume when compared with those without AF, independent
AF. After a mean follow-up of about 8 years, 6.5% of patients of cerebral emboli in a large cross-sectional study.102 In addi-
developed dementia. Atrial fibrillation was independently tion, recently, AF was associated with a decrease in total ce-
associated with increased risk of incident dementia (HR rebral blood flow and brain perfusion in an unselected elderly
1.42, 95% CI 1.17–1.72; P , 0.001).82 This result was cohort.103 These results may, at least in part, explain the as-
confirmed by a longitudinal analysis from the Cardiovascular sociation of AF with reduced relative brain volume and
Health Study including 5150 participants without baseline cognitive impairment.
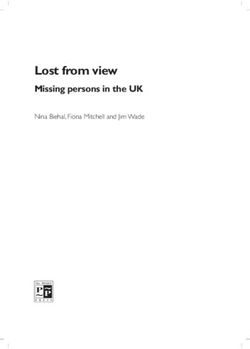
history of stroke.83 Incident AF occurred in 11% of patients, A schematic overview of the various mechanisms,
with faster decline in mean cognitive function scores, through which AF may lead to cognitive impairment is illus-
measured using the Modified Mini Mental State Examination trated in Figure 1.
(3MSE), compared with patients in sinus rhythm. Although A number of trials are currently examining, as the primary
both AF and dementia are diseases of aging, in two large or secondary outcome, the effect of different therapies
observational studies the highest RR of dementia was including anticoagulation and of different interventions on
observed in younger AF patients ,70 years of age.84,85 A cognitive function in patients with AF. A non-exhaustive
recent cross-sectional study indicated that in individuals list of such studies is found in Table 8.
with heart failure with reduced and preserved systolic ejec- The results of these studies will help to improve our under-
tion fraction, AF was associated with an adjusted higher standing of the relationship between AF and cognitive func-
odds of presence and severity of prevalent cognitive impair- tion and provide us with more data for possible prevention of
ment.86 (80 years) the relationship between AF and demen- cognitive decline by treatment of AF.
tia seems to be mostly mediated by concomitant risk It should also be noted that, conversely, impairment of
factors.87 cognitive function per se might have a negative impact on
The relationship between AF and cognitive decline may therapy adherence and medication intake104,105 and might
occur through a variety of pathological mechanisms. Given thus adversely affect treatment effectiveness and outcome
the relationship between AF and stroke, vascular dementia in patients with arrhythmias.
may be an obvious contributor to cognitive decline, encom-
passing both multi-infarct dementia and SVD demen-
tia.80–83,88 The second form of dementia in AF patients is Assessment of cognitive function in atrial
Alzheimer’s disease, which is the most common type of fibrillation patients in clinical practice
dementia overall. Atrial fibrillation has been identified as a Despite increasing awareness about the relationship between
risk factor for Alzheimer’s disease.84,89 Alzheimer’s AF and cognitive decline,74,98,106,107 clinical guidelines for
disease is the result of accumulation of abnormally folded the management of AF do not specifically include
beta-amyloid and tau proteins forming cerebral plaques assessment of cognitive function in the diagnostic work-up.
which exert cytotoxic effects leading to cerebral atrophy. With increasing prevalence of cognitive impairment in the
Interestingly, misfolded atrial natriuretic peptides may lead elderly108 and given that the highest RR of cognitive decline
to development of amyloid fibrils and deposits in the atria is in AF patients .70 years of age, health care professionals
PGL 5.5.0 DTD HRTHM7508_proof 16 March 2018 1:13 am cee10 Heart Rhythm, Vol -, No -, - 2018
AGE, HTN, DM, HF, OSA
Silent
Infarct
Anticoagulation
1. Hypercoagulable
state Thrombus Formation
Virchow Triad &/or
2. Circulatory stasis Macro/Microemboli
Atrial Statins, Anti-
3. Endothelial injury Brain
Fibrillation inflammatory Cognitive
Morphometric
medications Clinical Impairment
Changes*
Stroke
Sup.Frontal
Thalamus
Inflammation ↑ CRP, ?IL-6 MiddleFrontal cortex
cortex
Inf. Frontal cortex
Rhythm and
rate control Sun.Temporal
strategies cortex
MiddleTemporal
cortex
Beat-to-Beat
Inf. Temporal
Variability & ↓ Cerebral Blood Flow cortex ↓Hippocampus Globus
↓ CO Pallidus
volume
Putame
Figure 1 Different mechanisms through which atrial fibrillation may contribute to cognitive impairment. Potential interventions are shown in red. aSome of the
reported brain morphometric changes include hippocampus atrophy, white matter hyperintensities, and frontal medial lobe atrophy. Reproduced with modifica-
tion after permission from Ref.64 CO, cardiac output; CRP, C-reactive protein; DM, diabetes mellitus; HF, heart failure; HTN, hypertension; IL, interleukin; OSA,
obstructive sleep apnea.
who treat AF patients should be able to diagnose, and assess lished. Considering the mechanisms of cognitive impairment
risk factors for cognitive impairment appropriately. described in the sections above, several therapies may be
Assessment of cognitive function should be multifaceted considered (see “Recommendations”). Both disease states
(see Table 3), and psychometric testing is just one compo- share common risk factors that include aging, smoking, hy-
nent. Numerous validated tools are available to assess cogni- pertension, diabetes, sleep apnea, physical inactivity,
tive function, varying from brief screening tools, which take vascular disease, inflammation, and heart failure. Many of
1–8 min to complete among elderly patients, to more com- these risk factors represent modifiable targets for preventa-
plex time-consuming neuropsychological batteries (see tive therapies and if treated early may lower the risk of
Table 4). Brief screening tools may be most applicable both diseases.
when cognitive impairment is suspected among AF patients, Stroke prevention is the principal priority in the manage-
whereas more comprehensive assessments may be performed ment of AF and integrated approaches such as the Atrial
after appropriate referral to a geriatrician or neurologist. fibrillation Better Care (ABC) pathway (Avoid stroke, Better
Other factors determining the choice of test include the symptom management, Cardiovascular and comorbidity risk
time available with the patient, the setting (office-based or reduction) may improve AF management.110 Stroke preven-
inpatient), the patient’s ability to speak English (some tools tion therapy, particularly oral anticoagulation, applied to the
are not translated and/or validated in other languages), and appropriate patients according to risk stratification proposed
the purpose of the assessment (screening vs. confirmatory). in scientific guidelines107 may reduce the risk of dementia.
In practical terms, any of the brief tests could be used, Fridberg and Rosenqvist111 studied 444 106 AF patients
although the most common is the GPCOG.38 In research set- over 1.5 million years at risk. Anticoagulation use was in
tings, the Mini Mental State Examination (MMSE) and Mon- 202 946 (46%) of the patients with the primary anticoagulant
treal Cognitive Assessment (MOCA) have been commonly used warfarin (94%). In AF patients not treated with antico-
used.39,40,109 Informant questionnaires, such as the second agulation, 60% were on aspirin. In multivariate analysis, the
step of GPCOG or the IQCODE,46 provide important addi- strongest predictors of dementia were in order: age (HR per
tive information, since they assess a patient’s change over decade 2.19, 95% CI 2.16–2.22), Parkinson’s disease (HR
time from someone who knows the person well. This level 2.46, 95% CI 2.25–2.69), absence of oral anticoagulation
of detail may not always be feasible, however, and may be treatment (HR 2.08, 95% CI 1.73–2.53), and alcohol abuse
more suited for comprehensive geriatric or neurological (HR 1.53, 95% CI 1.41–1.66).
assessment. In patients managed long term with vitamin K antagonists
(VKAs), for example, TTR is inversely associated with new-
onset dementia.75 Risk of dementia is augmented in AF
Prevention of cognitive dysfunction in atrial patients who are frequently over anticoagulated or receiving
fibrillation patients antiplatelet therapy.112 However, dementia can have a con-
Since the precise mechanism(s) of cognitive disorders in pa- founding effect on maintenance of TTR, and oral anticoagu-
tients with AF is not fully known, the optimal way to prevent lation in AF patients has not been consistently associated
cognitive dysfunction for a given patient remains to be estab- with either improved cognitive function or less hippocampal
PGL 5.5.0 DTD HRTHM7508_proof 16 March 2018 1:13 am ceDagres et al
EHRA/HRS/APHRS/LAHRS Expert Consensus on Arrhythmias and Cognitive Function
Table 8 Studies that are currently examining the effect of different therapies and interventions on cognitive function in patients with AF or atrial tachyarrhythmias
Study name Target population Intervention Cognitive function as outcome
PGL 5.5.0 DTD HRTHM7508_proof 16 March 2018 1:13 am ce
Impact of Anticoagulation Therapy on the Cognitive Decline Non-valvular AF Randomization to dabigatran or warfarin Primary outcome: incident dementia and
and Dementia in Patients With Non-Valvular Atrial moderate decline in cognitive function
Fibrillation (CAF), NCT03061006
Comparison of Brain Perfusion in Rhythm Control and Rate Persistent AF Randomization to rhythm or rate control Primary outcome: cognitive assessment
Control of Persistent Atrial Fibrillation, NCT02633774
Cognitive Impairment Related to Atrial Fibrillation AF patients .65 years old and Randomization to dabigatran or warfarin Primary outcome: cognitive impairment
Prevention Trial (GIRAF), NCT01994265 CHA2DS2-VASc .1
Early Treatment of Atrial Fibrillation for Stroke Prevention AF patients Randomization to early standardized Secondary outcome: cognitive function
Trial (EAST), NCT01288352 rhythm control or usual care
Apixaban During Atrial Fibrillation Catheter Ablation: Patients undergoing catheter Randomization to vitamin K antagonists Secondary outcome: cognitive function
Comparison to Vitamin K Antagonist Therapy (AXAFA), ablation of non-valvular AF or apixaban change
NCT02227550
NOACs for Stroke Prevention in Patients With Atrial Patients with a high-risk of AF and Randomization to non-vitamin K Secondary outcome: cognitive function
Fibrillation and Previous ICH (NASPAF-ICH), NCT02998905 previous intracerebral hemorrhage antagonist oral anticoagulant or
acetylsalicylic acid
Non-vitamin K Antagonist Oral Anticoagulants in Patients Patients with atrial high rate episodes Randomization to edoxaban or Secondary outcome: cognitive function
With Atrial High Rate Episodes (NOAH), NCT02618577 and at least two stroke risk factors acetylsalicylic acid or placebo
but without AF
Optimal Anticoagulation for Higher Risk Patients Post- Patients having undergone a Randomization to rivaroxaban or Secondary outcome: neuropsychological
Catheter Ablation for Atrial Fibrillation Trial (OCEAN), successful AF catheter ablation acetylsalicylic acid testing
NCT02168829
Blinded Randomized Trial of Anticoagulation to Prevent Patients with non-valvular AF and Randomization to rivaroxaban or Primary outcome: composite endpoint of
Ischemic Stroke and Neurocognitive Impairment in AF with low risk of stroke acetylsalicylic acid stroke, TIA and neurocognitive decline
(BRAIN-AF), NCT02387229 Secondary outcomes: neurocognitive decline,
new onset of cognitive impairment
AF, atrial fibrillation; NOACs, non-vitamin K antagonist oral anticoagulant; TIA, transient ischemic attack.
e11e12 Heart Rhythm, Vol -, No -, - 2018
atrophy.98,109,113 Anticoagulation with warfarin neither R-R interval and heart rate has been shown, in a small study,
influenced the reduction of total brain volume nor cognitive to improve frontal and temporal blood flow and improve
function in individuals with AF.102 Non-vitamin K antago- memory and learning.124
nist oral anticoagulant therapy may reduce the incidence of Recommendations on the prevention of cognitive
brain micro-hemorrhage compared with VKAs,60 but dysfunction in AF patients are made in the Recommendations
whether NOACs improve long-term cognitive function is section. Most of these recommendations are consistent with
currently unknown. A recent community-based study pro- those of international guidelines107 and are not necessarily
vided some optimism in this regard and found that NOAC unique to those patients with AF and cognitive dysfunction.
therapies were associated with lower stroke and dementia
rates compared with warfarin.114 Considering the incidence
Other arrhythmias and cognitive dysfunction
of dementia in AF, only trials with large numbers of patients
Cognitive dysfunction in patients with regular
and extended long-term follow-up would be able to firmly
establish the possible benefit of oral anticoagulation on the supraventricular tachycardias
subsequent risk of cognitive decline. Recurrent supraventricular tachycardias in children and ado-
Preventing early onset of AF through lifestyle or risk fac- lescents, mediated by AV nodal re-entry or by accessory
tor modification could delay the onset and progression of pathways, were shown to be associated with cognitive defi-
cognitive decline. Prevention and early management of cits in 48% of such patients, when assessed prior to catheter
smoking, excess alcohol consumption, hypertension, obesity, ablation.125 Whether an early catheter ablation of supraven-
diabetes, and sleep apnea may reduce the onset and/or pro- tricular arrhythmia would affect the cognitive status of such
gression of AF115 with concomitant reductions in stroke patients needs further investigation.
and possibly cognitive function. However, such risk factor
modifications may have independent positive effects on Cognitive impairment after cardiac arrest
cognitive function regardless of the development of AF. It Brain injury after non-fatal cardiac arrest
is also unclear if aggressive modification should start at the Cardiac arrest occurs in two different settings, in-hospital and
time of onset of AF. Lifestyle modification may also reduce out-of-hospital, with completely different prognosis, for
the risk of cognitive decline in AF patients. Prevention of obvious reasons. As cardiac arrests that occur in a hospital
cognitive dysfunction may include general measures pro- context are usually immediately attended, the primary focus
posed in the treatment and management of vascular dementia of the study of brain injury after cardiac arrest has been
or Alzheimer’s disease. Several trials have tested the effects among survivors of out-of-hospital cardiac arrest
of physical activity and cognitive training in Alzheimer’s (OHCA).126 In this setting, brain damage is caused by cere-
disease and have shown some evidence of efficacy on bral hypoperfusion and its severity depends on the time of
cognitive endpoints.116 Most of the trials, however, had short such deficit127; the proportion of cardiac arrest survivors
follow-up periods. Further evidence is needed to confirm the who present with some degree of brain damage ranges
optimal design and dose of interventions, the appropriate from 35% to 100%.128,129 The working group of Chun-Lim
target population, and the efficacy of such interventions. and colleagues has delineated three scenarios that are clearly
Innovations such as the development of multi-domain inter- related to the duration of brain hypoperfusion: (i) patients
ventions and the use of biomarkers or genetic profiles to with early recovery of brain function without any sequelae,
better target higher-risk patients are being assessed in usually associated with opportune resuscitation and/or early
ongoing trials. However, differentiating the AF-dependent recovery of consciousness (,3 days after OHCA); (ii) pa-
or AF-independent effects of lifestyle and risk factor modifi- tients with extensive damage, associated with prolonged
cations remains a major challenge. coma (.7 days after OHCA); and (iii) an intermediate group
There are no robust data to affirm that therapy for rhythm between those extremes.130 They report that a coma duration
control with medication or “successful” AF catheter ablation of less than 3 days results in a better quality of life at 3- and
can prevent cognition disorders in AF patients. Atrial fibrilla- 12-month follow-up, and that the manifestation of severe
tion catheter ablation may not eliminate AF in the majority of cognitive impairment early on in recovery results in higher
patients, but rather attenuate overall AF burden. Follow-up risk for permanent memory and motor impairment.
data beyond 5 or 10 years are limited, and suggest that 2– Clinical sequelae of brain damage after OHCA may range
5% of “successfully” ablated patients will have recurrences from mild memory impairment to severe physical and mental
annually.117–120 Furthermore, many of these recurrences disability. As expected, if brain damage persists, it negatively
may be asymptomatic and the prognostic implication of impacts patients’ quality of life.130,131 Cognitive impairment
asymptomatic episodes on both stroke risk and cognitive could include limited attention span, personality
function is unknown.121–123 Catheter ablation as a specific disturbances, movement disorders (i.e. Parkinsonism), and
therapeutic approach to lower risk of stroke and dementia even dementia; however, memory seems to be the
is discussed in the Catheter Ablation section. cognitive function most affected in survivors of cardiac
In patients with persistent AF for whom which rhythm arrest. Neuropsychological studies have shown deficits in
control is not pursued, atrioventricular (AV) node ablation different cognitive areas including memory (64.3%),
with pacemaker implantation that restores a predictable executive functioning (21.4%), language (21.4%), and
PGL 5.5.0 DTD HRTHM7508_proof 16 March 2018 1:13 am ceYou can also read