Effectiveness of Diabetes Self - Management Education in Thais with Type 2 Diabetes
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Effectiveness of Diabetes Self – Management Education in Thais with Type 2 Diabetes
Effectiveness of Diabetes Self – Management Education in Thais with
Type 2 Diabetes
Porntip Tachanivate**, Runya Phraewphiphat**, Hataiporn Tanasanitkul,** Rungrudee Jinnawaso, **
Chatvara Areevut**, Rangsima Rattanasila,** Orawan Pichitchaipitak,** Khaemanee Jantawee,**
Nampeth Saibuathong,** Sawitree Chanchat,** Araya Ha-upala,** Prapai Ariyaprayoon,**
Patcharavee Tanlakit,** Piyanuch Maitreejorn,** Chanyaphat Pompantakron,** Jariya Boonpattararaksa,**
Kanokporn Pabua, *** Oraluck Pattanaprateep, ** Sirimon Reutrakul, Ratanaporn Jerawatana*
Abstract: Diabetes is a major health problem and economic burden around the world including
Thailand. Patient self-management is an important key to help patients control their disease
and prevent complications. This study aimed to evaluate a self-management education program
in Thais with type 2 diabetes. A retrospective cohort study was performed in 488 people
with type 2 diabetes attending the diabetes self-management education program by multidisciplinary
team and 488 people who did not attend the program. Mean differences in hemoglobin A1c
and diabetes medication utilization as dispensed from the hospital’s pharmacy (adjusted to define
daily dose) between baseline and follow ups were computed using mixed-effect regression
analyses. Cost-benefit was analyzed as a difference between the direct cost of conducting
the program and the benefit. Satisfaction, diabetes knowledge and behavioral changes were
collected in the intervention group.
Results revealed that during the two-year follow up, mean differences in hemoglobin A1c
reduction were similar between the two groups. However, the intervention group had a statistically
significant reduction in diabetes medication utilization, compared to non-intervention group,
especially during the second year. Cost-benefit analysis demonstrated that the diabetes
self-management education program provided a cost saving. The intervention group increased
their diabetes knowledge, changed diabetes self-care behaviors, and had high satisfaction with
the program. Thus, this Diabetes Self-Management Education Program in Type 2 Diabetes is
effective and associated with cost savings. Self-management program should be integrated
as a routine nursing practice to improve outcomes in people with type 2 diabetes.
Pacific Rim Int J Nurs Res 2019; 23(1) 74-86
Keywords: Cost, Cost-benefit, Effectiveness, Hemoglobin A1c, Medication utilization,
Self-management education, Type 2 diabetes.
Received 6 August 2017; Accepted 18 April 2018 Sirimon Reutrakul Pratuangtham, MD, CDE, Associate Professor,
Division of Endocrinology, Diabetes and Metabolism University of
Illinois at Chicago, USA. And Visiting Scholar Program, Department
Introduction of Medicine, Faculty of Medicine Ramathibodi Hospital, Mahidol
University, Thailand. E-mail: sreutrak10800@gmail.com.
Diabetes mellitus is one of the most common Correspondence to: Ratanaporn Jerawatana*, RN, MS, Dip. APAGN,
non-communicable diseases affecting people around Division of Nursing, Faculty of Medicine Ramathibodi Hospital,
Mahidol University, Thailand. E-mail: ratanaporn.jer@gmail.com
the world. The International Diabetes Federation **Faculty of Medicine Ramathibodi Hospital, Mahidol University,
(IDF) estimated that 451 million people worldwide Thailand.
74 Pacific Rim Int J Nurs Res • January - March 2019Porntip Tachanivate et al.
had diabetes in 2017 and the number is expected to Review of Literature
rise to 693 million by 20451. Unfortunately, most
people with diabetes live in low- and middle-income DSME provides people with diabetes and
countries. Uncontrolled diabetes can lead to macrovascular caregivers or family members with knowledge and
and microvascular complications, including stroke, skills to perform self-care and lifestyle changes in
heart disease, blindness, renal failure, and lower limb order to manage diabetes more effectively2. In a
amputation2. In 2017 an estimated 5.0 million deaths systematic review, DSME was associated with a
worldwide were directly caused by diabetes1. World significant reduction in hemoglobin A1c (Hb A1c)
Health Organization (WHO) reported that 2.2 million levels, a marker of glycemic control, by 0.57%. 10
deaths were attributable to high blood glucose3. If maintained in the long term, this could translate to
Diabetes also causes a significant economic burden. a significant decrease in complications since a 1%
In 2012, an estimated 245 billion USD was spent on reduction in HbA1c was associated with 25%
diabetes in the United States alone4. Thailand, an reduction in microvascular complications and 21%
upper-middle income country, experiences a similar for death-related to diabetes8. In addition, a meta-
burden from diabetes. The prevalence has risen from analysis of randomized controlled trials found that
7.5% in 2009 to 8.9% in 2014 5,6. The cost of diabetes the delivery of DSME program was cost-effective.11
care in 2010 was estimated at 906,374 USD in Hendrie and colleagues 12 studied the cost and
Thailand or 11% of the total global health expenditure7. effectiveness of the diabetes management education
The most recent survey in 2014 revealed that only program (DMEP) in person with type 2 diabetes.
23% of people with type 2 diabetes were considered The cost for the 6 month intervention period was 356
under good glucose control6. USD per person. They found that an individualized
Strong evidence suggests that good glucose DMEP was effective in reducing the number of
control can significantly reduce or delay microvascular hyperglycemia and hypoglycemia episodes with
complications.8 While there are numerous available incremental cost effectiveness ratio (ICER) of 39
diabetes medications, lifestyle modification consisting USD per glycemic-symptoms day avoided, compared
of diet and exercise remains a cornerstone in achieving with usual care. The study by Prezio and colleagues
good glycemic control.2 The person’s knowledge and 13
explored the long term effects of DSME intervention
ability to self-manage their disease is a vital part of program led by community health worker in uninsured
diabetes care. Therefore, it is recommended that people Mexican Americans on health outcomes and cost
with diabetes receive Diabetes Self-Management effectiveness. The results revealed a significant
Education (DSME), usually delivered by diabetes reduction in HbA1c levels and development of foot
educators or a multidisciplinary team, to enhance ulcers, compared to usual care. There was an average
essential skills and knowledge in managing their of 0.056 quality-adjusted life year (QALYs) gained
diabetes2. As medication cost contributes to a significant per person over 20 years with an ICER of 355 USD
expense in diabetes care, patients who are empowered per QALY, compared with usual care. 13
in their self-care and adopt a healthy lifestyle could Despite the growing burden of diabetes care
lead to reduced medication utilization2. This, along and evidence supporting the effectiveness of DSME,
with potential reduction in complications as a result such programs in Thailand are not uniform and the
of improved glycemic control, can lead to cost savings. national standard has not been established.14 A few
Therefore, cost benefit analysis and medication utilization studies have explored the efficacy of DSME programs
should be a part of DSME program’s evaluation9. in Thailand, up to 6-month follow up. There were
Vol. 23 No. 1 75Effectiveness of Diabetes Self – Management Education in Thais with Type 2 Diabetes
three studies that found a significant reduction in Study Aim:
HbA1c levels, between 0.14-0.59%. 15-17 But, the The aim of this study was to evaluate the
other studies did not find improvements.18-19 Self- effectiveness of the structured DSME program on
efficacy, self-management, knowledge and quality cost-benefit, medication utilization, glycemic control,
of life increased.18,19 Wattana and colleagues 16 studied diabetes knowledge, behavioral changes and satisfaction
the effects of a DSME program on glycemic control, in Thais with type 2 diabetes in a tertiary medical
coronary heart disease risk, and quality of life in 147 center in Thailand.
persons with type 2 diabetes. The findings indicated
that the intervention group, who received DSME Methods
program, had a significant reduction in HbA1c level
and coronary heart disease risk, and an increase in Design: Economic evaluation research design
quality of life compared to the non-intervention group. by a retrospective cohort study was used.
Another DSME program study in Thais with type 2 Sample and Setting: Participants in this study
diabetes by Jaipakdee and colleagues15 found that the had type 2 diabetes and were being followed up at
DSME program was associated with a significant one university hospital in Bangkok, Thailand from
reduction in HbA1c level (-0.14%), fasting plasma January 2014- December 2015. The inclusion criteria
glucose (-6.37 mg/dl), along with an increase in including having HbA1c values at follow up by
health behavior scores and quality of life. attending physicians at least once during this period.
When evaluating for health economic aspects, Exclusion criteria were people with non-type 2
four approaches are available20, cost-minimization, diabetes (i.e. gestational diabetes, type 1 diabetes, or
cost-benefit, cost-effectiveness, and cost-utility analysis. other types of diabetes) and those without HbA1c
Each of these methods has the same input and cost. values. The intervention group was composed of
The four techniques are different in output or outcome;
same outcome for cost-minimization, benefits in those who met the inclusion criteria and attended
monetary term for cost-benefit analysis, efficacy or the DSME program in addition to routine care. The
effectiveness in natural units (e.g. life years gained or non- intervention group was composed of those who
clinical values) for cost-effectiveness analysis, and met the same inclusion criteria but received only
natural units adjusted by utility (e.g. quality-adjusted routine care without DSME program.
life years (QALYs) or disability- adjusted life years During this period, there were 613 people
(DALYs) for cost-utility analysis. However, there has with type 2 diabetes who received the DSME program.
not been a study evaluating cost-benefit of such programs Of these, 448 met all the inclusion criteria and were
in Thailand, or a study with a longer follow up period. allocated to the intervention group. The non-intervention
This is an essential component of the program’s evaluation, group was retrieved by electronic medical records.
especially at the current study site which is a tertiary For this, electronic medical records from January
care hospital in a university setting, providing care 2014- December 2015 were searched for persons
for over 10,000 people with diabetes each year. with diagnosis code ICD-10 E1. This yielded 11,
Research Question: 134 persons. They were matched with each individual
Is structured DSME program in Thailand in the intervention group at a 1:1 ratio by age (± 5 years),
associated with cost savings, reduced medication gender and the same time of follow up at the clinic.
utilization, improved glycemic control, increased In addition, further matching of HbA1c levels was
diabetes knowledge, behavioral changes and satisfaction attempted to minimize the differences between the
in people with type 2 diabetes? two groups. The sample and setting are shown in Figure 1.
76 Pacific Rim Int J Nurs Res • January - March 2019Porntip Tachanivate et al.
Figure 1 Flow of the study
Ethical considerations: The study protocol diabetes knowledge scores (before and after the
was approved by the Institutional Review Board Committee, class), satisfaction scores, and whether they met their
Faculty of Medicine Ramathibodi Hospital, Mahidol behavioral goals upon follow ups. Ramathibodi’s
University. (The approval number COA no. 04-59-60, Diabetes Self-Management Education record form
date May 13, 2016). developed by two advanced practice nurses (APNs)
Instruments and outcomes Measure: and one physician who specialized in diabetes for use
Medical records of the intervention groups in routine practice in DSME program, consist of 4
were retrospectively reviewed regarding their parts:
Vol. 23 No. 1 77Effectiveness of Diabetes Self – Management Education in Thais with Type 2 Diabetes
1) Personal information sheet, used to amount of drug per item) / World Health Organization
obtain data on the demographic characteristic such as (WHO) DDD; where WHO DDD is the assumed
age, sex, education background, duration of disease, average daily maintenance dose for a medication
complications, comorbidities including the diagnoses utilization for its main indication in adults,
of hypertension, dyslipidemia, diabetes retinopathy independently of price and dosage form.21
and ischemic heart disease/ stroke. Cost of daily diabetes medications per patient
2) DSME/S sheets, used to obtain data on was calculated at 8 time points. The direct cost of
any prior diabetes education, outline the DSME conducting the DSME program was calculated as
contents along with behavior goal setting/ evaluation. cost per patient per program and consisted of the
3) Satisfactory evaluation sheet, a one-item following: facility cost, teaching supplies, office
survey asking the participants to rate their overall equipment, telephone follow-up cost, staff’s salaries
satisfaction of the program with a score ranging from and data management cost. Other potential costs
0 to 5, with 5 being most satisfied. including pre and post admission costs were not
4) Diabetes knowledge assessment (pre/ included in this analysis.
posttest), simple 10 multiple choices/ true-false Intervention: The DSME program activities
questions (total 10 points) to assess the participants’ are shown in Table 1. The program was delivered by
diabetes knowledge before and after the session. a multidisciplinary team including endocrinologists,
Higher scores indicate higher knowledge. The reliability two APNs, staff nurses, and dieticians. The content
measured using Kuder-Richardson (KR-20) formula was based on the 7 skills of self-management,
in 30 persons with type 2 diabetes was 0.80. The including healthy eating, being active, monitoring,
content of Ramathibodi’s DSME record form was taking medications, problem solving, reducing risks,
validated by a endocrinologist, two advanced practice and healthy coping, as defined by the American
nurses and a nursing faculty who specialized in Association of Diabetes Educators9. Delivery techniques
diabetes care were a combination of lecture-based strategy and
HbA1c levels were obtained from laboratory individual assessments. The content took approximately
database of the same university hospital. HbA1c half a day to deliver, after which the participants were
assays were performed using the Turbidimetric given 1-2 behavior goals according to their medical
inhibition immunoassay (TINIA) method, which has and personal needs. The participants were then asked
been certified by where there have a standardization to follow up within 2-3 months, usually with their
and quality control from the National Glycohemoglobin next physician appointments. During the follow up
Standardization Program (NGSP). The unit of visits, they met with an APN to discuss the individual
measurement was reported in percent (%). goal achievements and assess any barriers. The APN
Diabetes medications used (i.e., drugs under continued to empower and motivate any further
the Anatomical Therapeutic Chemical group A10A behavioral changes as needed, or encourage the
or A10B), both oral and injectable forms, were participants to maintain their self-care behaviors.
obtained from the electronic medical records. This Lastly, additional information and resources, and
was derived from the actual filled medications at the plan for the future self-care goal were offered as
hospital’s pharmacy. It was a normal practice for needed. The patients continued to receive their usual
most, but not all patients at our hospital. The diabetes care from their physicians during this period
medication utilization was adjusted to defined daily (Table 1).
dose (DDD). DDD was calculated as (items issued x
78 Pacific Rim Int J Nurs Res • January - March 2019Porntip Tachanivate et al.
Table 1: Content and activities of the DSME program
Session/time Content/Activity Multidisciplinary
(7skill of self-management)
FIRST VISIT
Session1 (30 min) Activity: Lecture with PowerPoint presentation. Question and Endocrinologist
answer session at the end, using two way communication APN
-What is diabetes? Content: The pathophysiology of diabetes , complications, treatments,
-Reducing risks self-management, sick day care, Immunization, reducing risk
and monitoring
Session 2 (30min) Activity: watching VDO on foot care Nurse
-Foot care Content: Diabetic foot complication and foot care Foot care VDO
Session 3 (30min) Activity: Exercise practice led by APN, along with supplemental APN
exercise VDO Exercise VDO
-Being active/Exercise Content: The benefits of exercise and physical activity, type of
exercise, discussing barriers, exercise cautions, encourage participants
to choose an appropriate exercise/physical activity, and practice
exercising
Session4 (70 min) Activity: Skill training / practice Multidisciplinary
(15 min/station) Content: participants were divided into 4 groups for skill training -APN
and practice. Each station contains behavior assessments, barriers -Nurses
4 training stations and facilitator evaluation, educating and skill training based on -Dieticians
-Healthy eating individualized needs.
-Taking medication Healthy eating: Food 24 hr recall, food exchange, healthy plate,
-SMBG/hypoglycemia and individualized meal plan.
(Monitoring) Taking medication: Action of oral medications and insulin as
-Foot screening used by the participants, food and drug relationship, proper
(Monitoring) medication taking and compliance, insulin injection techniques.
SMBG/hypoglycemia: SMBG skill and technique, interpret and
record SMBG data, hypoglycemia recognition and treatment:
15 -15 rule, preventing and monitoring hypo/hyperglycemia.
Foot screening: risk assessment of diabetic foot ulcer, self-monitoring
skill. Those deemed at high risk of diabetic foot complication were
referred to surgical clinic specializing in diabetic foot at the
same hospital
Session 5 (10 min) Goal setting: two behavioral goals were set in mutual agreement Multidisciplinary
with each participants. These goals were based on individual -APN
-Problem solving problems as evaluated from the sessions. One goal is typically -Nurses
-Healthy coping related to dietary intake, and the other was based on individual -Dieticians
-Reducing risks needs. The participant received a short note containing these
goals as a reminder.
Participants completed knowledge assessment test and satisfaction
survey before leaving.
SECOND VISIT (FOLLOW UP VISIT: in 2-3 months)
Session 6 (30 min) Follow up: discuss the individual goal achievements and assess APN
any barriers. APN continued to empower and motivate any further
-All skill evaluation behavioral changes as needed, or encourage the participants to
maintain their self-care behaviors. Additional information and
resources, and plan for the future self-care goal were offered
as needed.
Vol. 23 No. 1 79Effectiveness of Diabetes Self – Management Education in Thais with Type 2 Diabetes
Data collection the DSME program as input or incremental cost, and
difference of diabetes medication cost in monetary
Since this study was a retrospective cohort study term as outcome or incremental benefit. The direct cost
all information was extracted from medical records. included the staff’s salaries, calculated in proportion
Data related to personal information was extracted to the time they devoted to the program, facility cost,
once at the beginning of the first visit (session 1-4 and any miscellaneous cost of conducting the program.
of the program). The diagnoses of hypertension, The difference between the incremental benefit and
dyslipidemia, diabetes retinopathy and ischemic heart the incremental cost was then calculated per person and
disease/ stroke were obtained from ICD10. Diabetic compared. In detail, the incremental benefit was the
knowledge was obtained before and after the first difference in diabetes medication cost between baseline
visit of the program, whereas satisfaction with the and 24 months in the intervention and non-intervention
program was obtained at the end of the program. HbA1c groups, as follows: [(average daily medication cost in
levels, diabetes medication utilizations were extracted the intervention group at 24 month - baseline) - (average
from medication records every 2-3 months at the time daily medication cost in the non-intervention group at
of follow up till 24 months for eight times. Estimated 24 month- baseline)] x 730. Costs are expressed in Thai
glomerular filtration rates (eGFR) were extracted from Baht (THB) and converted to USD using 35 Baht/US$22.
laboratory database. In addition, one-way sensitivity analysis was
Statistical analyses: performed by varying the cost of diabetes medications
Data are presented as mean ± SD or frequency (generic vs. original formula), staff salaries (±10%),
(%). Independent t-tests or Chi square were used to facility cost (±10%), and the number of patients (±10%).
compare differences in characteristics between groups,
as appropriate. Results
Mixed-effect regression analyses were performed,
adjusting for hypertension and dyslipidemia, to evaluate The study flow chart is shown in Figure 1 and
the mean differences (MD) between intervention and the characteristics of the participants in the intervention
non-intervention groups in their changes in HbA1c and non-intervention group are shown in Table 2.
levels and DDD between baseline and each time point. There were no statistically significant differences between
The analyses were performed using Stata, version 14.2. groups with the exception that more participants in
Cost-benefit analysis was performed from the the intervention group had retinopathy than those in
hospital perspective to compare direct cost of conducting the non-intervention group (pPorntip Tachanivate et al.
For the intervention group, diabetes knowledge up period, while the non-intervention group had an
increased significantly after the education session increase. The intervention group had a significant reduction
(8.9 ± 2.0 vs. 9.9 ± 1.4, pEffectiveness of Diabetes Self – Management Education in Thais with Type 2 Diabetes
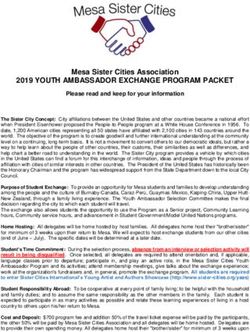
0.1
0.05
0
Changes in DDD
0 3 12 15 18 21 24 month
-0.05 6 9
-0.1
-0.15
-0.2
Non-intervention Intervention * pPorntip Tachanivate et al.
generic vs. original formula, saving 202.84 THB increase in diabetes medication utilization, especially
(approximately 6 USD) vs. 16.516.62 THB (approximately during the second year. This is consistent with a known
472 USD). The savings did not vary greatly when progressive nature of type 2 diabetes mellitus. While
considering staff’s salaries, facility cost and the number the actual reasons for a lesser increase in medication
of the patients (±10%). utilization in the intervention group were not explored
in this study, this was likely due to behavioral changes
Discussion and a better understanding of their diabetes, as reflected
by increased diabetes knowledge and reportedly meeting
In this retrospective cohort study of 976 people the behavioral goals among the participants (although
with type 2 diabetes in a tertiary care setting in Thailand, the details of how each participant monitored their diabetes
we found that those receiving structured DSME had were not available). Previous research demonstrated
improved glycemic control, which was sustained that that DSME led to better self-care including diet,
during a 2-year follow up, similarly to those who did exercise and improved medication adherence26. Reduction
not receive DSME but were receiving care at the in medication utilization could be possibly associated
same facility during the same period. However, the with less adverse effects including hypoglycemia,
DSME program was associated with a reduction in which should be explored in future studies.
daily diabetes medication utilization, and cost savings Given the reported average cost of diabetes
of 3,135.08 THB/person/program (approximately care in Thailand between 1,328- 6,331 THB per patient
90 USD) over the 2-year period. Additionally, satisfaction per year (37.94-180.89 USD)7,27, this cost-saving
with the program was high, diabetes knowledge increased, could be quite significant, especially if confirmed in
and behavioral goals were met in a majority of the a larger study involving other health care facilities in
participants. This result supported the feasibility, the country. This saving varies depending upon the
effectiveness and cost-benefit of a structured DSME formula of the medications, which in this study was
program in Thailand, an upper-middle income calculated as the actual medication cost, and to a lesser
country with growing burden of diabetes care. degree the administrative cost of the program delivery.
In the current study, the degree of glycemic This finding was consistent with those previously
improvement associated with DSME, 0.6-0.7% reduction reported in Mexican Americans that diabetes education
in HbA1c, was similar to those previously reported in delivered by community health workers was associated
Western countries10, as well as in Thailand.16 This effect with an incremental cost-effectiveness ratio of USD
size could translate into a significant reduction in 355 per quality-adjusted life year gained13, attributed
microvascular complications if maintained in the by better glycemic control, lower foot ulcerations and
long term8, and is equivalent to the potency of some amputations. In our study, only medication utilization
of diabetes medications.2 The efficacy was maintained was considered, therefore, the potential savings could
during the 2-year follow up, which consistent with include further reduction in complications and
some previous studies23,24, although not all demonstrated hospitalization cost, especially if the glycemic control
such long-lasting effects.25 However, the glycemic is maintained. This should be further explored.
improvement seen in the intervention group was not Strengths and Limitation:
different from those not attending DSME but who Our study has strengths of being the first to
were receiving care at the same hospital. The improvement explore the cost-saving of DSME program in Thailand,
in glycemic control in the non-intervention group, including a relatively large number of participants,
however, was achieved at the expense of a continuous and a follow up period of 2 years. However, there are
Vol. 23 No. 1 83Effectiveness of Diabetes Self – Management Education in Thais with Type 2 Diabetes
limitations. This was not a randomized controlled trial Implications for Nursing Practice:
as we did not feel that not delivering DSME in research The diabetes self-management education
participants was appropriate. Despite the attempt to match program should be a part of diabetes care in hospitals
the participants, the intervention groups appeared to at all levels in Thailand, and should be adopted as a
have more severe disease, as they had more medication policy at the national level. Currently, some hospitals
utilization at baseline despite having similar HbA1c have diabetes nurses or advance practiced nurses but
levels to the non-intervention group. Nevertheless, some do not. However, to provide effective DSME,
the study revealed that they had a smaller increase in all hospitals should be staffed with a diabetes nurse,
their medication utilization over the two-year period, along with a multidisciplinary team, who are trained
compared to the non-intervention group. Data on in diabetes self-management education and support.
diabetes medication utilization were not available in This will allow individualized support for people
all participants, which could be due to the fact that with diabetes as they have different characteristics,
they were diet-controlled or received their medications problems and need different nursing interventions.
outside our hospital. However, the numbers of participants The current program could also serve as a model of
without medication utilization information were similar care for other chronic diseases.
between the two groups. Nonetheless, the study
demonstrated effectiveness of the DSME program in Acknowledgements
our patient group. In addition, the current structured
DSME program was established in late 2013. Prior The authors acknowledge the contributions of
to that, DSME was delivered but not in a systematic the experts and health care providers who were
fashion. We could not exclude the possibility that the involved in this study. We also thank the participants
non-intervention participants had received DSME in this study.
prior, or from other sources outside the program. The
expense of the program also did not include indirect Reference
costs from the patients and their families. The study was
1. Cho NH, Shaw JE, Karuranga S, Huang Y, da Rocha Fernandes
conducted in only one tertiary medical center and the JD, Ohlrogge AW, et al. IDF Diabetes Atlas: Global estimates
findings may not be generalized to other patient groups. of diabetes prevalence for 2017 and projections for 2045.
Lastly, other outcomes such as quality of life or other Diabetes research and clinical practice. 2018.
complications were not explored in the current study. 2. American Diabetes Association. Standards of medical care
in diabetes-2017. Diabetes Care. 2017;40:S1-S142.
Conclusion 3. World health organization. Global report on diabetes 2016.
[cited 2017 March13]. Available form http://apps.who.
A structured DSME program in Thailand was int/iris/bitstream/10665/204871/1/9789241565257
associated with a slower increment in diabetes medication 4. Centers for disease control and prevention. diabetes 2014
utilization and cost-savings, along with increased patients’ report card. .[cited 2017 April 4]. Available form http://
www.cdc.gov/diabetes/pdfs/library/diabetesreport
diabetes knowledge and satisfaction. This could serve card2014.pdf
as a model for developing countries where diabetes 5. Aekplakorn W, Chariyalertsak S, Kessomboon P,
continues to be a significant health and economic burden. Sangthong R, Inthawong R, Putwatana P, et al. Prevalence
Further research should explore the benefit of such and management of diabetes and metabolic risk factors in
program in other parts of Thailand, along with other Thai adults: the Thai National Health Examination Survey
outcomes such as complications and quality of life. IV, 2009. Diabetes Care. 2011;34(9):1980-5.
84 Pacific Rim Int J Nurs Res • January - March 2019Porntip Tachanivate et al.
6. Aekplakorn W. Thai national health examination survey 17. Saengtipbovorn S, Taneepanichskul S. Effectiveness of
V. Institute. Nonthaburi: Health Systems Research; 2016 lifestyle change plus dental care (LCDC) program on
7 Zhang P, Zhang X, Brown J, Vistisen D, Sicree R, Shaw improving glycemic and periodontal status in the elderly
J, et al. Global healthcare expenditure on diabetes for 2010 with type 2 diabetes. BMC Oral Health. 2014;14(1):72.
and 2030. Diabetes research and clinical practice. 2010; 18. Wichit N, Mnatzaganian G, Courtney M, Schulz P, Johnson
87(3):293-301. M. Randomized controlled trial of a family-oriented self-
management program to improve self-efficacy, glycemic
8. UK Prospective Diabetes Study (UKPDS) Group. Intensive
control and quality of life among Thai individuals with Type 2
blood-glucose control with sulphonylureas or insulin diabetes. Diabetes Res Clin Pract. 2017;123:37-48.
compared with conventional treatment and risk of 19. Ounnapiruk L, Wirojratana V, Meehatchai N, Turale S.
complications in patients with type 2 diabetes (UKPDS 33). Effectiveness of a behavior modification program for older
Lancet 1998;352(9131):837-53. people with uncontrolled type 2 diabetes. Nurs Health Sci.
9. American Association of Diabetes Educators. The art and 2014;16(2):216-23.
science of diabetes self-management education desk reference. 20. Drummond MF SM, Claxton K, Stoddart GL, and Torrance
2nd ed. Chicago: American Association of Diabetes Educators; GW. Methods for the economic evaluation of health care
2011. programmes. New York: Oxford University Press; 2015.
10. Chrvala CA, Sherr D, Lipman RD. Diabetes self- 21. Norwegian Institute of Public Health .Guidelines for ATC
management education for adults with type 2 diabetes classification and DDD assignment 2017. [cited 2017
mellitus: A systematic review of the effect on glycemic May 13]. Available from https://www.whocc.no/
filearchive/publications_guidelines_web.pdf.
control. Patient Educ Couns. 2016;99(6):926-43.
22. Bank of Thailand. Rates exchange of commercial banks
11. Lian JX, McGhee SM, Chau J, Wong CKH, Lam CLK, [cited 2017 May 13]. Available from https://www.bot.
Wong WCW. Systematic review on the cost-effectiveness or.th/english/_layouts/application/exchangerate/
of self-management education programme for type 2 exchangerate.aspx
diabetes mellitus. Diabetes Res Clin Pract. 2017;127:21-34. 23. Williams IC, Utz SW, Hinton I, Yan G, Jones R, Reid K.
12. Hendrie D, Miller TR, Woodman RJ, Hoti K, Hughes J. Enhancing diabetes self-care among rural African
Cost-effectiveness of reducing glycaemic episodes through Americans with diabetes: results of a two-year culturally
community pharmacy management of patients with type 2 tailored intervention. The Diabetes Educator.
diabetes mellitus. The Journal of Primary Prevention. 2014;40(2):231-9.
2014;35(6):439-49. 24. Piatt GA, Anderson RM, Brooks MM, Songer T, Siminerio
13. Prezio EA, Pagán JA, Shuval K, Culica D. The community LM, Korytkowski MM, et al. 3-Year follow-up of clinical
diabetes education (CoDE) program: cost-effectiveness and behavioral improvements following a multifaceted
diabetes care intervention. The Diabetes Educator.
and health outcomes. Am J Prev Med. 2014;47(6):771-9.
2010;36(2):301-9.
14. Reutrakul S, Deerochanawong C. Diabetes in Thailand: 25. Tang TS, Funnell M, Sinco B, Piatt G, Palmisano G,
Status and Policy. Curr Diab Rep. 2016;16(3):28. Spencer MS, et al. Comparative effectiveness of peer
15. Jaipakdee J, Jiamjarasrangsi W, Lohsoonthorn V, leaders and community health workers in diabetes self-
Lertmaharit S. Effectiveness of a self‐management support management support: results of a randomized controlled
program for Thais with type 2 diabetes: Evaluation trial. Diabetes Care. 2014;37(6):1525-34.
according to the REAIM framework. Nurs Health Sci. 26. Murray CM, Shah BR. Diabetes self-management
2015;17(3):362-9. education improves medication utilization and retinopathy
16. Wattana C, Srisuphan W, Pothiban L, Upchurch SL. Effects screening in the elderly. Primary Care Diabetes. 2016;
of a diabetes self‐management program on glycemic 10(3):179-85.
control, coronary heart disease risk, and quality of life 27. Riewpaiboon A, Pornlertwadee P, Pongsawat K. Diabetes
among Thai patients with type 2 diabetes. Nurs Health Sci. cost model of a hospital in Thailand. Value Health.
2007;10(4):223-30.
2007;9(2):135-41.
Vol. 23 No. 1 85Effectiveness of Diabetes Self – Management Education in Thais with Type 2 Diabetes
ประสิทธิผลของโปรแกรมการสร้างความรูแ้ ละทักษะการดูแลตนเองในผูเ้ ป็น
เบาหวานชนิดที่ 2 ของไทย
พรทิพย์ เตชะนิเวศน์** รัญญา แพรวพิพัฒน์** หทัยพร ธนาสนิทกุล** รุง่ ฤดี จิณณวาโส**
ฉัตรวรา อารีวฒ ุ *ิ * รังสิมา รัตนศิลา** อรวรรณ พิชติ ไชยพิทกั ษ์** แขมณี จันทร์เทวี** น�ำ้ เพชร สายบัวทอง**
สาวิตรี ชาญชาติ** อารยา หาอุปละ** ประไพ อริยประยูร** พัชรวีร์ ทันละกิจ** ปิยานุช ไมตรีจร
** ชัญญาพัชร์ พรหมพันธกรณ์** จริยา บุญภัทรรักษา** กนกพร พาบัว** อรลักษณ์ พัฒนาประทีป**
สิริมนต์ ริ้วตระกูล ประเทืองธรรม รัตนาภรณ์ จีระวัฒนะ*
บทคัดย่อ: โรคเบาหวานเป็นปัญหาสุขภาพ และภาระเศรษฐกิจทั่วโลกและประเทศไทย การดูแล
จัดการตนเองของผู้เป็นเบาหวานเป็นกุญแจส�ำคัญในการควบคุมโรค และป้องกันภาวะแทรกซ้อน การ
วิจัยนี้เพื่อศึกษาประสิทธิผลของโปรแกรมการสร้างความรู้และทักษะการดูแลตนเองในผู้เป็นเบาหวาน
ชนิดที่ 2 เป็นการศึกษาวิเคราะห์ยอ้ นหลังในผูเ้ ป็นเบาหวานชนิดที่ 2 จ�ำนวน 488 รายทีเ่ ข้ารับโปรแกรม
โดยทีมสหสาขาวิชาชีพ และผู้ที่ไม่ได้รับโปรแกรม เพื่อเปรียบเทียบค่าน�้ำตาลเฉลี่ยสะสม และการใช้ยา
ของผูป้ ว่ ย (แปลงเป็นหน่วยขนาดยามาตรฐานต่อวัน) ระหว่างก่อน และหลังเข้าโปรแกรม ความคุม้ ค่าของ
การบริการ และเก็บข้อมูลความพึงพอใจ ความรู้ และการปรับเปลีย่ นพฤติกรรม วิเคราะห์ขอ้ มูลโดยสถิติ
ถดถอยการเปรียบเทียบตัวแปรแบบผสม
ผลการศึกษาพบว่าหลังได้รับโปรแกรม 2 ปี ค่าน�้ำตาลเฉลี่ยสะสมลดลงใกล้เคียงกันทั้ง 2 กลุ่ม
กลุ่มที่ได้รับโปรแกรมมีการใช้ยาเบาหวานลดลงอย่างมีนัยส�ำคัญเมื่อเทียบกับกลุ่มที่ไม่ได้รับโปรแกรม
โดยเฉพาะในปีที่ 2 โปรแกรมนี้ประหยัดค่าใช้จ่ายเมื่อเทียบต้นทุนและประโยชน์ที่ได้รับ กลุ่มที่ได้รับ
โปรแกรม มีความรู้เพิ่มขึ้น มีการปรับเปลี่ยนพฤติกรรมการดูแลตนเอง และมีความพึงพอใจสูงขึ้น ดังนั้น
โปรแกรมการสร้างความรู้และทักษะการดูแลตนเองในผู้เป็นเบาหวานมีประสิทธิภาพและลดค่าใช้จ่าย
จึงควรบูรณาการโปรแกรมนี้สู่การปฏิบัติการพยาบาล เพื่อพัฒนาผลลัพธ์ในการดูแลผู้เป็นเบาหวาน
ชนิดที่ 2
Pacific Rim Int J Nurs Res 2019; 23(1) 74-86
ค�ำส�ำคัญ: ค่าใช้จ่าย, ความคุ้มค่าของการบริการ, ประสิทธิผล, ค่าน�้ำตาลเฉลี่ยสะสม, การใช้ยา,
สร้างความรู้และทักษะการดูแลตนเอง, เบาหวานชนิดที่ 2
สิรมิ นต์ ริว้ ตระกูล ประเทืองธรรม MD, CDE, Associate Professor, Division of
Endocrinology, Diabetes and Metabolism University of Illinois at Chicago,
USA. และ อาจารย์ คณะแพทยศาสตร์โรงพยาบาลรามาธิบดี มหาวิทยาลัยมหิดล
ประเทศไทย Email: sreutrak10800@gmail.com.
ติดต่อที่ : รัตนาภรณ์ จีระวัฒนะ* RN, MS, Dip. APAGN, คณะแพทยศาสตร์
โรงพยาบาลรามาธิบดี มหาวิทยาลัยมหิดล ประเทศไทย
E-mail: ratanaporn.jer@gmail.com
**คณะแพทยศาสตร์โรงพยาบาลรามาธิบดี มหาวิทยาลัยมหิดล ประเทศไทย
86 Pacific Rim Int J Nurs Res • January - March 2019You can also read