Diabetic Kidney Disease - Shilpa Gadde MD, FACP Nephrology-Critical Care
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Diabetic Kidney Disease Shilpa Gadde MD, FACP Nephrology-Critical Care
I have no financial disclosures or conflicts to be said.
DM and CKD/ESRD
• DM is rampant and increasing worldwide (380 million)
• China (100 million), India (65 million), US (30 million, 100 million
pre‐diabetic)
• Diabetic kidney disease/nephropathy is the leading cause of
CKD and ESRD in the US (and other Western societies)
Montero et al. Nephrology 2015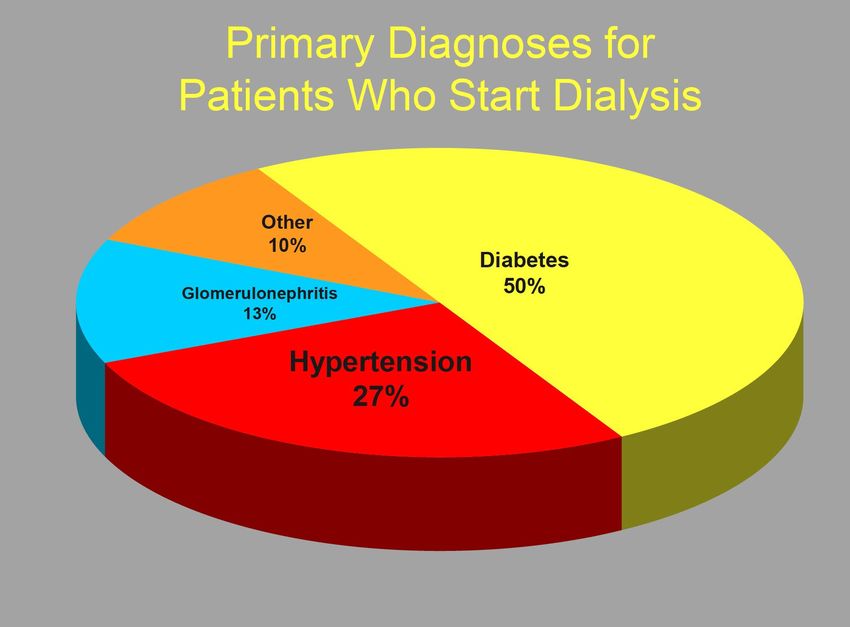
DN: Burden?
• Incidence
• Almost 50% of all new cases of ESRD in the U.S. due to diabetes
• Type 2 diabetes accounts for most cases of diabetic nephropathy
• Prevalence of nephropathy 57% after 25 years of type 2 diabetes
• Cost
• In U.S. alone, total annual spending for ESRD > $20 billion
• Cost / patient-year higher for diabetics ($70,000) than nondiabetics ($50,000)
• Mortality
• 1.5-2.5x greater mortality among diabetics with ESRD than
nondiabetics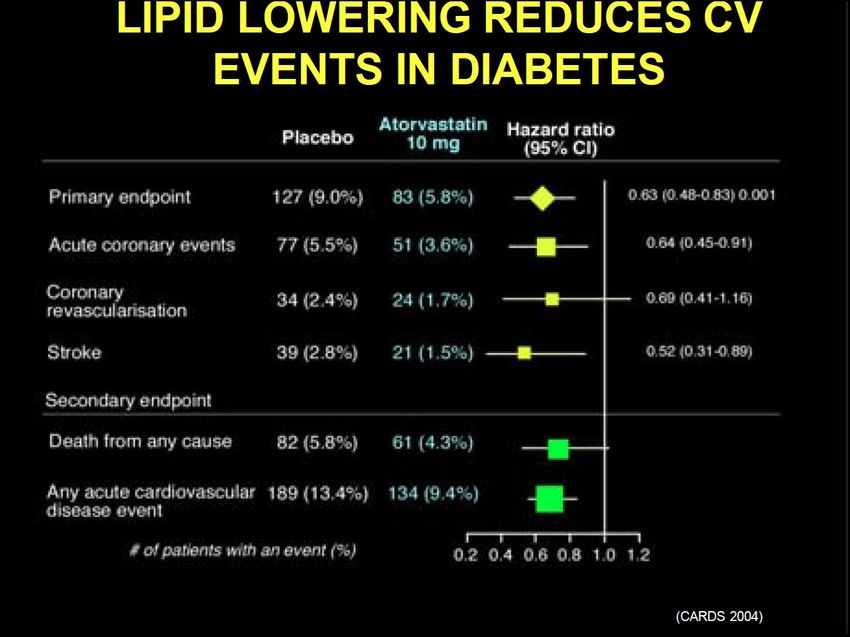
Screening for microalbuminuria • ADA recommends screening for microalbuminuria in all Type 2 diabetics at the time of diagnosis of diabetes, and annually thereafter • Recommend for Type 1 DM screening for microalbuminuria 5 years after the diagnosis of Type 1 DM and yearly thereafter
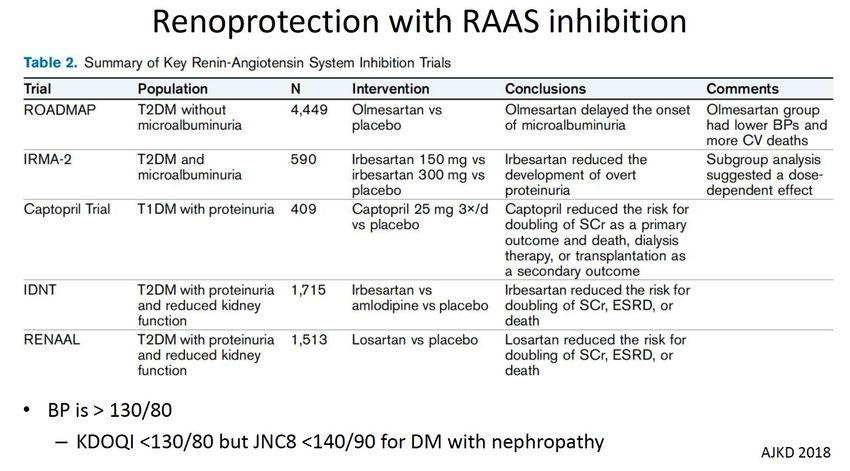
Stages of preventing progressive nephropathy • Glycemic control • Lipid lowering • Quit smoking/weight loss • Blood pressure control • Inhibition of renin angiotensin system
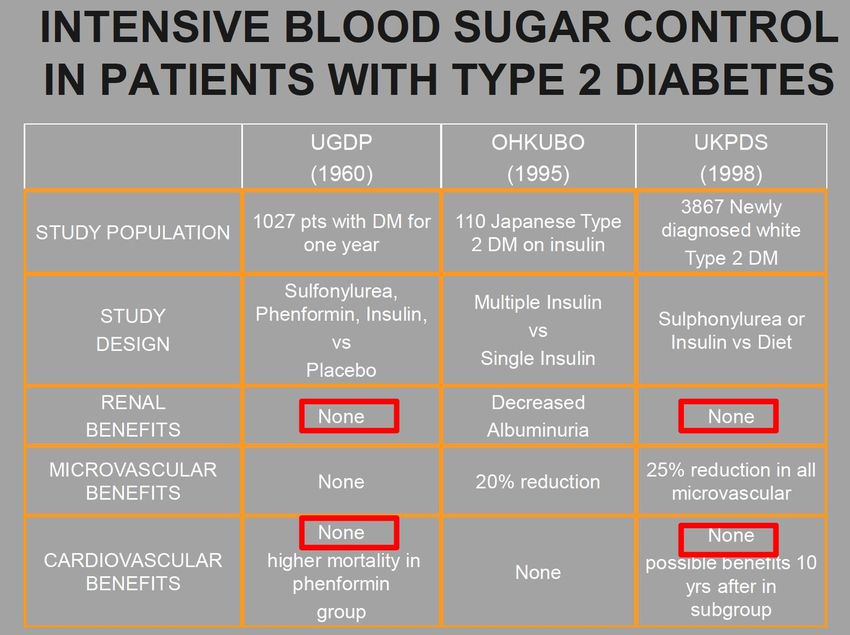
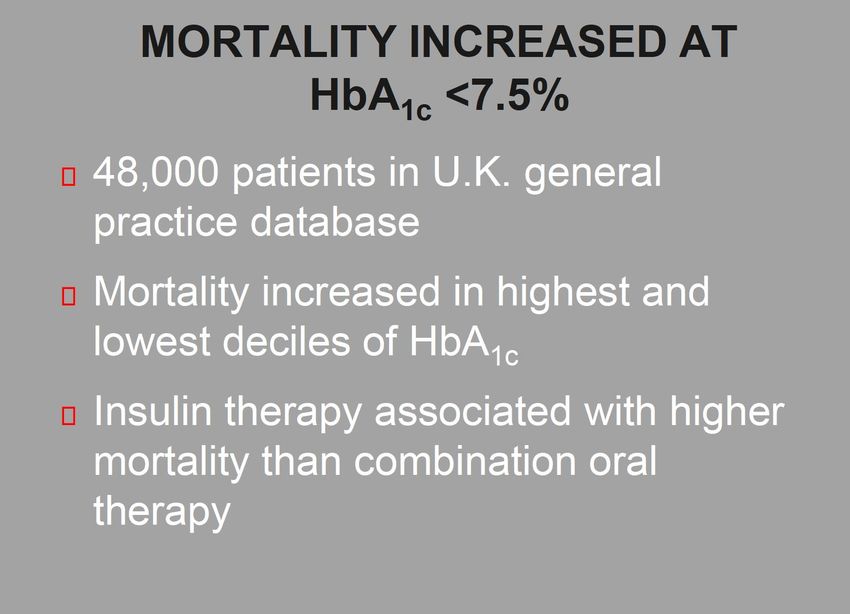
Glycemic control in Diabetes • Clear benefit of intensive blood sugar control in pts with Type 1 DM and early nephropathy • Unknown effectiveness and safety of intensive blood sugar control in pts with Type 2 DM and early or late nephropathy • If there is any benefit of intensive blood sugar control in pts with Type 2 DM, it is likely to be in select subpopulations and is not an appropriate guideline to be enforced in all patients • ADA recommends HgA1C
Stages of preventing progressive nephropathy • Glycemic control • Lipid lowering • Quit smoking/weight loss • Blood pressure control • Inhibition of renin angiotensin system
ADA 2021 guidelines
Stages of preventing progressive nephropathy • Glycemic control • Lipid lowering • Quit smoking/weight loss • Blood pressure control • Inhibition of renin angiotensin system
Stages of preventing progressive nephropathy • Glycemic control • Lipid lowering • Quit smoking/weight loss • Blood pressure control • Inhibition of renin angiotensin system
Stages of preventing progressive nephropathy • Glycemic control • Lipid lowering • Quit smoking/weight loss • Blood pressure control • Inhibition of renin angiotensin system
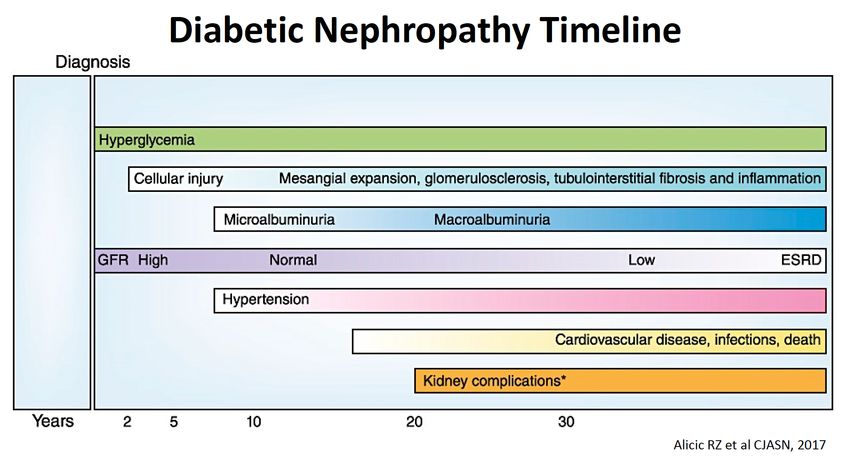
A 29‐year‐old woman with T1DM for 10yr is evaluated by her PCP. She takes insulin and ergocalciferol. Vitals: BP 130/78, P 75, afebrile. Exam: Clear lungs, nl HS, benign abdomen, no edema Labs: Na 139, K 4.3, Cl 102, HCO3 23, BUN 16, sCr 1.0, Alb 3.8, U/A: normal, Urine spot alb/Cr: 110 mg/g (was 60 mg/g 6 months ago) Does this patient have underlying diabetic nephropathy and if so, what clinical stage? A. Does not have diabetic nephropathy B. Stage 1 with hyperfiltration and increased GFR C. Stage 2 with normoalbuminuria and normal GFR D. Stage 3 with microalbuminuria E. Stage 4 with overt clinical nephropathy
Microalbuminuria—1st clinical indicator • We don’t measure GFR, or biopsy • Urine Dipstick NOT SENSITIVE • MA must be confirmed on at least 2 occasions 3‐6 months apart –Time of day, BG control, Fever, exercise • MA diagnosed by Timed collections or Spot measurements – Microalbuminuria 20‐200 ugm/min – Microalbuminuria 30‐300 mg/day – Microalbuminuria 30‐300 mg/g creatinine – Macroalbuminuria >300 mg/day = Total Proteinuria >500 mg/day proteinuria = Dipstick proteinuria = Overt Nephropathy
Which of the following patients is least likely to have diabetic nephropathy: A. DMI for 15 years with retinopathy B. DM1 for 15 years without retinopathy C. DM2 for 15 years without retinopathy D. DM2 for 3 years with retinopathy
Which of the following patients is least likely to have diabetic nephropathy: A. DMI for 15 years with retinopathy—Classic presentation B. DM1 for 15 years without retinopathy—DMI Nephropathy rare w/o nephropathy C. DMII for 15 years without retinopathy---30% DMII w/ nephropathy have no retinopathy D. DMII for 3 years with retinopathy---3yrs may seem early but onset of DMII rarely is known
Which of the following statements is true? A. Better blood glucose control has only been shown to prevent renal disease in T2 DM B. APOL1 high risk alleles is associated with risk of nephropathy in T2DM C. Smoking increases the risk for and the progression of diabetic nephropathy D. Race only influences the risk of diabetic nephropathy but not progression
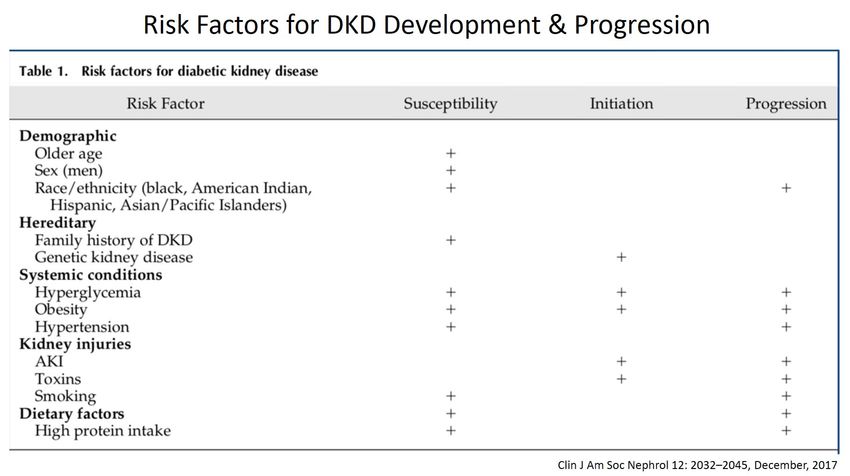
Which of the following statements is true? A. Better blood glucose control has only been shown to prevent renal disease in T2 DM-- BG control is effective in Both T1 and T2 DM B. APOL1 high risk alleles is associated with risk of nephropathy in T2DM- APOL1 is NOT associated with the development of renal disease in DM C. Smoking increases the risk for and the progression of diabetic nephropathy D. Race only influences the risk of diabetic nephropathy but not progression- Black, Native American, Hispanic, Asian/Pacific Islanders all have increased risk for development and progression of Diabetic Nephropathy
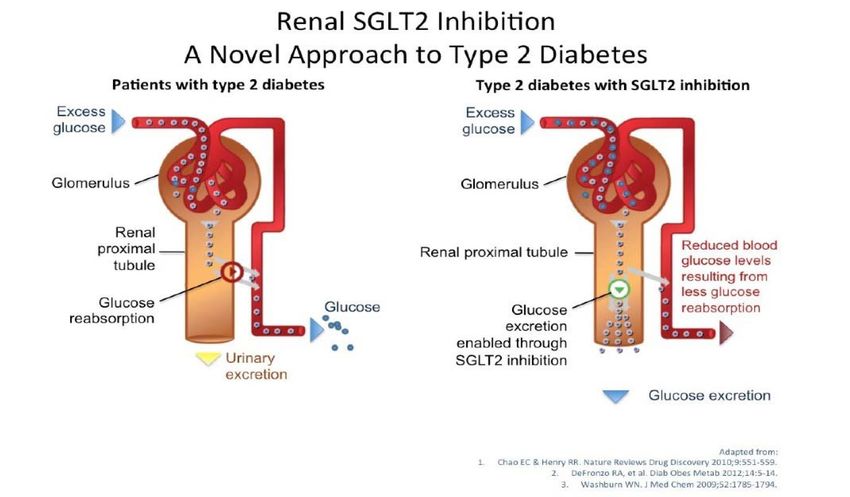
A 49 year‐old male with type 2 DM and a recent hemoglobin A1c of 8.9% was recently started by you on empagliflozin. Which of the following is true regarding empagliflozin? A. Empagliflozin is effective in patients with an eGFR < 20 ml/min/per 1.73 m2 B. The risk of urinary tract infections is not increased with empaglifozin C. There is an increased risk of ketoacidosis with empaglifozin D. The risk of genital fungal infection is not increased with empaglifozin
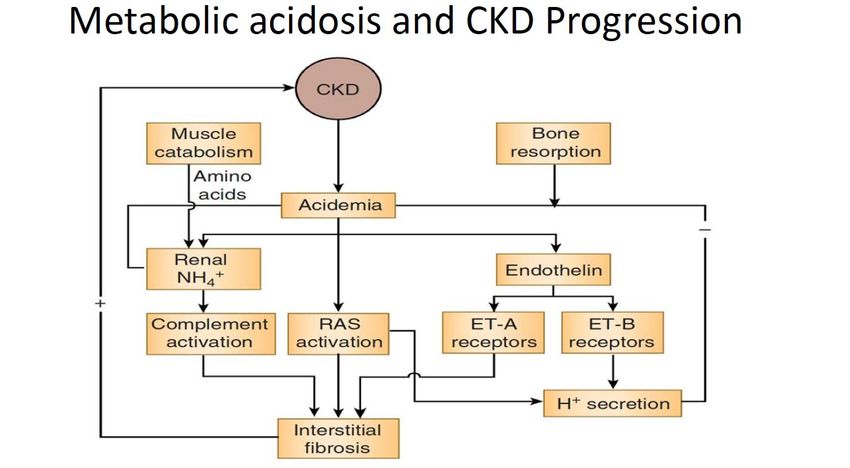
A 63‐year‐old man T2 DM is seen in the office for CKD from diabetic nephropathy. He has stage 3 CKD, gout, HTN, anemia. He takes glipizide, losartan, iron sulfate, amlodipine. Vitals: BP 128/78, P 68, afebrile Exam: Clear lungs, S4 gallop, benign abdomen, trace pedal edema Labs: Na 138, K 5.4, Cl 112, HCO3 16, BUN 85, sCr 1.7, Calcium 9.2, Phosphate 5.0, Alb 3.7, Uric acid 7.6, iPTH 70 (nl 20‐65), U/A: 1+ Pro Which of the following is the most appropriate addition to his current medical regimen? A. Allopurinol B. Phosphate binder C. Sodium polystyrene D. Sodium bicarbonate
A 62‐year‐old woman with T2 DM for 9 yrs is sent to your office for evaluation of HTN. Medications include metformin and a CCB. BP 148/94, P 72, BMI 28. Exam with S4 gallop and trace edema. Labs: HbA1c 7.1%, K 4.8, BUN 17, HCO3 22, sCr 1.1, glucose 131 Urine: 1.012, pH 5.5, Protein 4+, Blood –. Urine Prot/Cr‐ 900mg/gm In addition to reducing dietary sodium intake, which of the following is the most appropriate next step? A. Add an ACE inhibitor or ARB B. Add an ACE inhibitor and then an ARB C. Add a thiazide diuretic D. Add a loop diuretic E. Monitor BP to see response to dietary sodium restriction
References
• Rodby, Diabetic kidney disease cases. Rush university IL, 2020.
• Alicic et al. Clin J Am Soc Nephrol. 2017 Dec 7;12(12):2032-2045. doi: 10.2215/CJN.11491116. Epub 2017.
• Clinical significance of microalbuminuria and evaluation of the micral-test. https://doi.org/10.1016/0009-9120(93)90126-Q.
• Ohkubo. Intensive insulin therapy prevents the progression of diabetic microvascular complications in Japanese patients with non-insulin-
dependent diabetes mellitus: a randomized prospective 6-year study. Diabetes Res Clin Pract. 1995 May;28(2):103-17. doi:
10.1016/0168-8227(95)01064-k
• UKPDS. Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS
34). UK Prospective Diabetes Study (UKPDS) Group. Lancet. 1998 Sep 12;352(9131):854-65.
• Colhoun et al. Primary prevention of cardiovascular disease with atorvastatin in type 2 diabetes in the Collaborative Atorvastatin Diabetes
Study (CARDS): multicentre randomised placebo-controlled trial. Lancet. 2004 Aug 21-27;364(9435):685-96. doi: 10.1016/S0140-
6736(04)16895-5.PMID: 15325833
• Lewis EJ, et al. The effect of angiotensin-converting-enzyme inhibition on diabetic nephropathy. The Collaborative Study Group. N Engl J
Med. 1993. PMID: 8413456 Clinical Trial.
• Harris, Diabetic kidney disease. Vanderbilt, 2019.
• IRMA 2, 2001. The effect of irbesartan on the development of diabetic nephropathy in patients with type 2 diabetes. N Engl J Med. 2001
Sep 20;345(12):870-8. doi: 10.1056/NEJMoa011489.
• ADA 2021 guidelines 10. Cardiovascular Disease and Risk Management: Standards of Medical Care in Diabetes—2021
• American Diabetes Association, Diabetes Care 2021 Jan; 44(Supplement 1): S125-S150. https://doi.org/10.2337/dc21-S010.
https://care.diabetesjournals.org/content/44/Supplement_1/S125You can also read