Developmental Differences in the Expression of Childhood Anxiety Symptoms and Fears
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Developmental Differences in the Expression of
Childhood Anxiety Symptoms and Fears
CARL F. WEEMS, PH.D. AND NATALIE M. COSTA, M.S.
ABSTRACT
Objective: To examine age differences in the expression of childhood fears and anxiety symptoms. Method: A cross-
sectional design was used to test recently formulated developmental hypotheses regarding the differential expression
of childhood anxiety symptoms and fears in a community sample of youths (N = 145). Three groups of youths were
compared: children aged 6–9 years (n = 47), preteens aged 10–13 years (n = 52), and adolescents aged 14–17 years
(n = 46). Symptoms of separation anxiety, generalized anxiety, and social anxiety were assessed using a dimensional
approach by both parent and child report. Fears were assessed by child report. Results: The results indicated that there
are systematic age differences in the expression of childhood fears and anxiety symptoms. Results also point toward spe-
cific symptoms predominant at certain ages (i.e., separation anxiety symptoms in youths aged 6–9 years, death and danger
fears in youths aged 10–13 years, and social anxiety symptoms as well as failure and criticism fears in youths aged 14–17
years) in partial support of predictions. Conclusions: Models of the etiology of childhood anxiety disorders tracing con-
tinuity and change over time should consider differences in the developmental expression of childhood fears and anxiety
symptoms. Attention to developmental issues concerning symptom expression may be important in the clinical understand-
ing of childhood anxiety. J. Am. Acad. Child Adolesc. Psychiatry, 2005;44(7):656–663. Key Words: childhood anxiety,
fears, separation anxiety, generalized anxiety, social anxiety.
Understanding the processes responsible for childhood expression of childhood anxiety symptoms and very lim-
anxiety disorders represents a clinically and theoretically ited use of developmental information in the classifica-
important task given their potential for having a negative tion of childhood anxiety and phobic disorders (Curry
impact on children’s lives (Pine et al., 1998; Silverman et al. 2004; Scheeringa et al., 2001). The purpose of this
and Treffers, 2001). However, unlike the disruptive be- study was to extend the existing research on age differ-
havioral disorders, there are no well-defined etiological ences in anxious symptoms by testing recently formu-
pathways outlining continuity and change for child- lated developmental theories regarding the systematic
hood anxiety disorders (Vasey and Dadds, 2001; War- differential expression of childhood fears and anxiety
ren and Sroufe, 2004). Longitudinal research on the symptoms across age groups.
stability of childhood anxiety disorders has often pro- Drawing on data regarding normative emotional de-
duced inconsistent results (Last et al., 1996; Newman velopment as well as psychosocial developmental theory
et al., 1996). One reason may be because of a lim- regarding critical developmental stages (e.g., Loevinger,
ited understanding of developmental differences in the 1976), both Westenberg et al. (2001) and Warren and
Sroufe (2004) have presented models that posit specific
age differences in the expression of the symptoms of
Accepted February 15, 2005. childhood anxiety and phobic disorders. Although symp-
From the Department of Psychology, University of New Orleans.
This research was supported in part by a grant from the NIMH (MH067572)
toms alone do not constitute an anxiety disorder or phobia,
awarded to Carl F. Weems. symptoms have been used to identify and differentiate
Correspondence to Dr. Carl F. Weems, Department of Psychology, University the various anxiety disorders (Warren and Sroufe, 2004).
of New Orleans, New Orleans, LA 70148; e-mail: cweems@uno.edu. These models suggest that the predominant expression
0890-8567/05/4407–06562005 by the American Academy of Child
and Adolescent Psychiatry. of anxious and phobic symptoms is tied to normative de-
DOI: 10.1097/01.chi.0000162583.25829.4b velopmental periods and challenges. By integrating the
656 J. AM . ACAD. CH ILD ADOLESC. PSY CH IATRY, 44:7, JULY 20 05CH ILD HOOD ANX IETY models regarding the sequence and timing of symptom clinical samples do not precisely speak to the predom- expression for school-age youths (ages 6–17 years), one inance of symptom expression. Studies examining fears would hypothesize that separation anxiety (SA) symp- and anxiety symptoms dimensionally across age ranges toms and animal fears should be the predominant ex- provide more specific information about the symptoms pression in youths around ages 6–9 years, generalized that may be the predominant expression of anxiety at anxiety (GA) symptoms and fears concerning danger different ages. and death in youths around ages 10–13 years, and social In general, symptoms of anxiety and fears appear to anxiety (SCA) symptoms and social/performance related diminish or decrease longitudinally over time and in older fears in adolescents around ages 14–17 years. age groups in community samples (e.g., Ollendick, The link between normal development and the symp- et al., 1985, 1989; Weems et al., 2002). However, re- toms of anxiety and phobic disorders can be understood search examining specific anxious symptoms and fears as stemming from the idea that there are basic biological dimensionally across age ranges does provide some sup- and behavioral predispositions to anxiety disorders. port for the idea of sequential developmental differences These predispositions give rise to undifferentiated in the levels of specific fears and anxiety symptoms. For ‘‘anxiety.’’ The symptoms of specific anxiety disorders example, with regard to specific symptoms, Weems are shaped by various additional biological, cognitive, et al. (1999) found that child-reported animal fears behavioral, and social processes (Vasey and Dadds, and death and danger fears were negatively correlated 2001), and thus, the predominant expression of anx- with age, whereas fears of failure and criticism were iety may be tuned, in part, to sequential developmental not correlated with age in a clinic-referred sample of challenges in these domains. For example, children aged youths who met criteria for phobias (n = 120). Chorpita 6–9 years have begun the process of individuation and et al. (2000) found that SA symptoms decreased with are realizing their autonomy from parents. Along with school grade level, whereas SCA symptoms increased this developing sense of self as separate from parents is with grade in a large school-based sample of youths the contrasting realization of dependence on parents. (N = 1,641) in grades 3 through 12. Research by The developmental challenge is eventual secure self- Ollendick and colleagues (1985, 1989) in normative reliance, but this challenge likely gives rise to concerns samples suggests higher rates of animal fears in children about separation from or loss of parents. Similarly, youths compared with adolescents; however, these studies have aged 10–13 years are gaining insight into mortality and also found decreases in fears of failure and criticism as broader world concerns that may give rise to death and well. Such results might seem to be in partial contradic- danger fears and the worries characteristic of generalized tion of predictions from the Westenberg et al. (2001) anxiety. Finally, the emerging social understanding and and Warren and Sroufe (2004) models. However, sim- comprehension of adolescents may lead to a predomi- ple comparisons of different age groups on symptom nance of social and evaluative concerns in this age group levels do not precisely test the hypothesis that there (Warren and Sroufe, 2004; Westenberg et al., 2001). are systematic differences in the symptoms that are Epidemiological data in community samples on the the predominant expression of anxiety across ages. In age at onset of anxiety disorders is fairly consistent with the context of age-related declines in overall anxiety lev- this prediction, with somewhat differing results across els and fears, the differential expression of specific fears studies (Costello et al., 2004) and thus provide some and symptoms may be obscured by the general trend empirical evidence. In addition, research on clinical (Westenberg et al., 2004). More precise statistical pro- samples suggests that SA disorder is more common in cedures are needed to test this hypothesis. With the ex- children, whereas social phobia is more common in ado- ception of Westenberg et al. (1999, 2004), few studies lescents. For instance, Weems et al. (1998) reported dif- have provided specific a priori tests of the developmen- ferences in the distribution of anxiety disorders, with SA tal models presented above. Westenberg and colleagues disorder more common in children (ages 6–11 years), (1999) have reported that SA disorder developmentally whereas social phobia was more common in older youths precedes overanxious disorder (using DSM-III-R crite- (ages 12–17 years) in a sample of 280 youths who met ria [American Psychiatric Association, 1987] versus diagnostic criteria for anxiety disorders. However, age at DSM-IV [American Psychiatric Association, 1994]). onset studies and distributions of anxiety disorders in Westenberg et al. (2004) found that child-reported fears J. AM. ACAD. CH ILD ADO LESC. PSY CH IAT RY, 44:7, JULY 200 5 657
WEEMS AND COS TA
of physical danger and punishment decrease with age or others (only one child was excluded: pervasive developmental dis-
and that fears of social and achievement evaluation in- order not otherwise specified). Interested families were informed
that we were conducting a study of youth behaviors, emotions,
crease with age when controlling for overall fears. and anxiety and that they could receive a free screening for anxiety-
In this study, a cross-sectional design was used to test related problems. However, potential subjects were told that families
the hypothesis of sequential differences in the predom- are eligible to participate regardless of whether they have anxiety
problems or not. This recruitment process was designed to help nor-
inant expression of fears and anxiety symptoms using malize the distribution of anxiety symptoms to facilitate the use of
a community sample of youths. Three groups of youths parametric statistics. Only 6% of children and 5% of mothers were
were compared: children aged 6–9 years, preteens aged currently on any form of psychotropic medications. All data used in
this study were collected before families were referred to or enrolled
10–13 years, and adolescents aged 14–17 years. Symp- in intervention services (6%).
toms of SA, GA, and SCA were assessed using a dimen-
sional approach by both parent and child report. Fears
Measures
were also assessed by child report. Based on previous
The Revised Child Anxiety and Depression Scales (RCADS)
research, we predicted age and gender differences in (Chorpita et al., 2000) were used to assess symptoms of SA, GA,
the overall level of anxiety symptoms and fears. Specif- and SCA. The RCADS is a 47-item instrument that assesses symp-
ically, that older youths and boys would report fewer toms of childhood anxiety disorders (except posttraumatic stress dis-
anxiety symptoms and fears. Based on Westenberg order and specific phobias) and depression based on DSM-IV criteria
(American Psychiatric Association, 1994). Each symptom on the
et al. (2001) and Warren and Sroufe (2004), we predicted scale is scored 1, ‘‘never’’; 2, ‘‘sometimes’’; 3, ‘‘often’’; and 4,
that the predominant symptom would systematically ‘‘always’’ and contains a total anxiety score (i.e., the sum of all anx-
differ across ages but not gender (the developmental iety symptoms) as well as subscales for the symptoms tested in this
study. Chorpita et al. (2000) reported an item set and factor defi-
challenges thought to drive differences in the predom- nitions that were consistent with DSM-IV anxiety disorders and de-
inant expression of anxiety and fear should influence pression. Moreover, the RCADS demonstrated convergent validity
both boys and girls). Further drawing from their mod- with existing measures of childhood anxiety and anxiety disorders
(Chorpita et al., 2000). Because the RCADS is a relatively new in-
els, it was predicted that SA would emerge as the prom- strument, internal consistency (coefficient a) and convergent valid-
inent manifestation of anxiety in youths aged 6–9 years, ity (Pearson’s r) estimates for the RCADS total anxiety score were
GA in youths aged 10–13 years, and SCA in youths computed in this study’s sample as well as for younger children and
aged 14–17 years. It was predicted that animal fears older youths. Internal consistency was .93 in the full sample, .92 in
youths aged 6–11 years, and .93 in youths aged 12–17 years. Con-
would emerge as the prominent manifestation of fears vergent validity was assessed using the Revised Children’s Manifest
in youths aged 6–9 years, death and danger fears in Anxiety Scale (RCMAS) (Reynolds and Richmond, 1978) total
youths aged 10–13 years, and social/performance-related score. Convergent association with the RCMAS was .74 in the full
sample, .71 in youths aged 6–11 years, and .81 in youths aged 12–17
fears in youths aged 14–17 years. years (all p valuesCH ILD HOOD ANX IETY
subscales used in this study assessed fear of animals, fear of danger an approach is consistent with recent theoretical discussion on
and death, and fear of failure and criticism. These factors have been the valid use of ANCOVA (Tabachnick and Fidell, 2001). Visual
shown to have satisfactory internal consistency test-retest reliability inspection of mean standardized values across symptoms and age
and to be stable across cultures (Ollendick et al., 1985, 1996). Parent groups was used to test consistency with predicted order and a series
report of child fear was not used because our previous research in- of single degree of freedom contrasts with a Bonferroni a adjustment
dicates poor correspondence between parents and children in terms (Jaccard and Guilamo-Ramos, 2002) were conducted to test the spe-
of death and danger fears and failure and criticism fears (Weems cific age group hypotheses. Supplemental follow-up comparisons
et al., 1999). were made within age groups using a confidence interval approach
for testing differences among symptoms. Specifically, 90% confi-
dence intervals were computed because these supplemental tests
Procedures are not covariate adjusted and because of clear a priori hypotheses
Data were collected via a UNO Institutional Review Board– about directionality of the mean difference in the symptom’s stan-
approved study. Informed consent was obtained from the parent dardized score relative to all other anxious (or fear) symptoms. Con-
and informed assent was obtained from the child before any of fidence intervals not including zero are considered meaningful, and
the assessment procedures took place. Completion of the assess- this approach capitalizes on the use of the standardized Z scores (e.g.,
ments took place in a quiet clinic setting, and the child completed consistency in findings across studies can be examined).
the assessment in a separate room from the parent. The measures
used in this study were part of a comprehensive assessment battery
for youth emotions and behaviors. Both the youth and parent were
given a general overview of the assessment procedures. Standardized RESULTS
specific instructions were then given to the parent and child sepa-
rately. Youths completed the measures and were assisted by trained Means and SDs for total nontransformed scores on
research assistants (e.g., young participants were read the assessment each of the measures (RCADS, RCADS-P, FSSC-R)
battery by research assistants who monitored the child’s comprehen- by age and gender are presented in Table 1. Examina-
sion of the questions and level of attention and fatigue). At the con-
clusion of the study, all participants were debriefed and given a small tion of the symptom scores’ ranges and skew indicated
monetary reward. Two children were missing RCADS ratings and acceptable levels for the planned analyses. Consistent
three were missing RCADS-P and FSSC-R ratings. Participants with with our recruitment strategy, symptom scores were less
missing data did not systematically differ from those without miss-
ing data on the other variables in this study. Analysis-wise deletion of positively skewed than typical normative samples. Re-
missing cases was used in instances of missing data. sults of a 2 (gender) 3 3 (age group) multivariate anal-
ysis of variance indicated a significant effect of age group
Data Analytic Strategy (Wilks multivariate F 6,258 = 7.31, p < .001, h2 = 0.15)
Descriptive statistics were used to screen the data before analysis. and gender (Wilks multivariate F 3,129 = 9.13, p < .001,
Age groups (‘‘children’’ [ages 6–9 years], ‘‘preteens’’ [ages 10–13 h2 = 0.18) on the measures but no significant interac-
years], and ‘‘adolescents’’ [ages 12–17]) were formed. Preliminary tion. Follow-up analyses of variance indicated that the
analyses compared the age groups using factorial (age by gender)
multivariate analysis of covariance with follow-up analyses of vari- age groups as well as boys and girls differed on total
ance on the measures’ total scores. For testing the hypotheses, sub- RCADS and FSSC-R scores in expected directions.
scale scores for SA, GA, and SCA as well as fears of animals, death To test the differential expression hypothesis,
and danger, and failure and criticism were computed across the en-
tire sample as SD scores (Z scores) so direct valid comparisons could
RCADS, RCADS-P, and FSSC-R symptom scales (Z
be made using a within-subjects design model (i.e., differences in the score–transformed scale scores) were examined using
various scale ranges would confound results if not standardized). three separate mixed-design repeated-measures ANCO-
Mixed factorial within-subjects (type of symptom [as the within- VAs (i.e., one for RCADS SA symptoms, GA symptoms,
subjects measure] by age group by gender [as between-subjects fac-
tors]) analyses of covariance (ANCOVAs) were used to test the hy- SCA symptoms; one for RCADS-P SA symptoms, GA
potheses. Confirmation of hypotheses is a significant effect of age symptoms, SCA symptoms; and one for FSSC-R ani-
group and a significant type of symptom by age group interaction mal fears, death and danger fears, and failure and crit-
with the predicted symptom predominant in the predicted age
group. The total score on the measure was used as the covariate icism fears). Age group and gender were between-subjects
and was controlled to account for overall differences in anxious independent variables, specific symptoms (e.g., SA, GA,
symptoms. Statistically, the hypothesis is that, controlling for any SCA) were the within-subjects independent variable, and
general trends in anxiety symptoms, specific anxiety symptoms will
be predominant at different ages. This statistical model was adapted
total score (RCADS total) was the covariate. ANCOVA
from structural magnetic resonance imaging and functional magnetic on RCADS revealed a significant effect of age group
resonance imaging analysis of brain data. The analogy is in tests of (F 2,136 = 3.78, p = .025, h2 = 0.05), and age group by
laterally different brain volume or activation (e.g., hemisphere is symptom interaction (F 4,136 = 11.19, p < .001, h2 =
used as a within-subjects factor controlling for total brain volume
to identify significant differences in a particular region such as 0.14). Total score was a significant covariate (F 4,136 =
the frontal lobe or the amygdala [see Carrion et al., 2001]). Such 1,569.91, p < .001, h2 = 0.92), and, as expected,
J. AM. ACAD. CH ILD ADO LESC. PSY CH IAT RY, 44:7, JULY 200 5 659WEEMS AND COS TA
TABLE 1
Means & Standard Deviations for Measures Total by Age and Gender and Summary of Planned Age Group Contrasts
Age 6–9 yr Age 10–13 yr Age 14–17 yr Boys Girls
Mean (SD) Mean (SD) Mean (SD) Mean (SD) Mean (SD)
Measure (n = 47) (n = 52) (n = 46) (n = 66) (n = 79)
RCADSa,b 72.09 (16.7) 63.64 (15.9) 57.11 (15.2) 59.84 (16.4) 67.59 (16.6)
RCADS-P 52.40 (9.3) 53.15 (12.2) 48.97 (10.6) 51.56 (10.7) 51.53 (10.3)
FSSC-Ra,b 151.25 (27.4) 137.94 (24.7) 119.24 (26.3) 125.00 (28.0) 144.87 (26.7)
Mean Difference SE F p LL UL
RCADS
6–9 > 10–17 on SA 0.56 0.10 32.5 >.001c 0.37 0.75
10–13 > 6–9 and 14–17 on GA 0.07 0.11 0.45 .509 –.14 0.28
14–17 > 6–13 on SCA 0.45 0.11 17.8 >.001c 0.24 0.66
RCADS-P
6–9 > 10–17 on SA 0.40 0.12 11.9 .001c 0.17 0.62
10–13 > 6–9 and 14–17 on GA –0.10 0.10 1.1 .299 –.29 0.09
14–17 > 6–13 on SCA 0.13 0.09 1.9 .171 –.06 0.31
FSSC-R
6–9 > 10–17 on AN –0.08 0.09 1.0 .325 –.26 0.08
10–13 > 6–9 and 14–17 on D&D 0.32 0.11 8.5 .004c 0.10 0.53
14–17 > 6–13 on F&C 0.20 0.12 2.9 .093 –.03 0.43
Note: RCADS = Revised Child Anxiety and Depression Scales anxiety total score; P = parent-completed anxiety total; FSSC-R = Fear Survey
Schedule for Children-Revised total; LL = lower limit 95% confidence interval; UL = upper limit; SA = separation anxiety; GA = generalized
anxiety; SCA = social anxiety; AN = animal fears; D&D = death and danger fears; F&C = failure and criticism fears.
a
Significant age group difference.
b
Significant gender difference.
c
Contrast significant with Bonferroni correction.
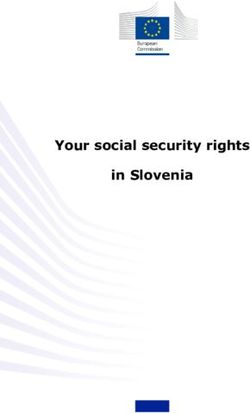
controlling for total score, there was no main effect of age group by symptom interaction (F 4,136 = 3.25, p =
gender, symptom, or three-way interaction. Mean stan- .013, h2 = 0.05). Total score was a significant covariate
dardized symptom scores across the age groups are pre- (F 4,136 = 2,812.03, p < .001, h2 = 0.95), and there was
sented in Figure 1A and show the group differences in no main effect of gender, symptom, or three-way inter-
the expression of symptoms. Planned age group con- action. Mean standardized symptom scores across the
trasts are summarized in Table 1 and indicate that chil- age groups are presented in Figure 1B and show group
dren aged 6–9 years reported greater SA than youths in differences in the expression of symptoms. Planned age
the other age groups and that adolescents aged 14–17 group contrasts are summarized in Table 1 and indicate
reported greater SCA than youths in the other age that the parents of children aged 6–9 years reported
groups. Supplemental within-group comparisons sug- greater SA in their children than those with children
gest that there were differences in standardized scores in the other age groups. Follow-up within-group com-
within age groups as predicted for SA and SCA but parisons indicated that there were clear differences in
not GA. SA was more predominant relative to all other standardized scores within the 6–9 years age group as
anxiety symptoms in children aged 6–9 years (mean dif- predicted for SA. SA was more predominant relative
ference = 0.26, SEM = 0.10, 90% confidence interval to other anxiety symptoms in children aged 6–9 years
for difference 0.06–0.46), and SCA was more predom- (mean difference = 0.20, SEM = 0.07, 90% confidence
inant relative to all other anxiety symptoms in adoles- interval for difference 0.09–0.32).
cents aged 14–17 years (mean difference = 0.36, SEM = ANCOVA on FSSC-R revealed a significant effect
0.07, 90% confidence interval for difference 0.24–0.49). of age group (F 2,136 = 5.33, p = .006, h2 = 0.07), and
ANCOVA on RCADS-P revealed a significant effect age group by symptom interaction (F 4,136 = 2.51, p =
of age group (F 2,136 = 10.53, p < .001, h2 = 0.14) and .042, h2 = 0.04). Total score was a significant covariate
660 J. AM . ACAD. CH ILD ADOLESC. PSY CH IATRY, 44:7, JULY 20 05CH ILD HOOD ANX IETY
death and danger was more predominant relative to other
anxiety symptoms in children aged 10–13 years (mean
difference = 0.19, SEM = 0.10, 90% confidence interval
for difference 0.02–0.66). Fear of failure and criticism was
more predominant relative to other anxiety symptoms
in adolescents aged 14–17 years (mean difference = 0.23,
SEM = 0.09, 90% confidence interval for difference
0.08–0.39). Because the FSSC-R subscale for animals
also contains a small number of ‘‘minor injury’’ items
(e.g., getting a cut), the analysis was run deleting those
items from the scale; however, results were virtually
identical.
DISCUSSION
This study adds to the existing research and provides
support for theories regarding developmental differences
in the expression of childhood fears and anxiety symp-
toms. In terms of general age and gender trends in anx-
iety symptoms and fears, the preliminary results were
consistent with those of previous research indicating
both age and gender differences in anxiety levels and
fears (e.g., Ollendick et al., 1989). Moreover, results were
highly consistent with the theorizing of Westenberg et al.
(2001) and Warren and Sroufe (2004), who have sug-
gested specific age differences in the expression of child-
hood anxiety. Overall, results supported the theory of
differential expression of symptoms across age groups
across each of the measures. In terms of specific symp-
toms, consistent with our integration of Westenberg
Fig. 1 A: Covariate-adjusted standardized symptom scores across age groups et al. (2001) and Warren and Sroufe (2004), SA ap-
for child Revised Child Anxiety and Depression Scale (RCADS) ratings. B:
peared to be the predominant expression of anxiety
Covariate-adjusted standardized symptom scores across age groups for parent
RCADS-P ratings. C: Covariate-adjusted standardized symptom scores in children aged 6–9 years. Results were consistent
across age groups for Revised Fear Survey Schedule for Children (FSSC-R). across both parent and child report of anxious symp-
toms as well as in the specific supplemental compari-
(F 4,136 = 1,545.21, p < .001, h2 = 0.92), and there was sons. Such findings are consistent with the notion that
no main effect of gender, symptom, or three-way inter- the developing sense of self-reliance and developing
action. Mean standardized symptom scores across the sense of autonomy from parents may lead to SA as a pre-
age groups are presented in Figure 1C and show the dominant expression of anxiety in this age group (Warren
group differences in the expression of fears. Planned and Sroufe, 2004). However, the evidence that animal
age group contrasts are summarized in Table 1 and in- fears were the predominant fear symptoms in this youn-
dicate that children aged 10–13 years reported greater gest age group was weak. The only support comes from
death and danger fears than youths in the other age examination of Figure 1 in that the mean scores for fear
groups. Follow-up within-group comparisons indicated of animals were higher (although still below the average)
that there were clear differences in standardized scores than the other symptoms (i.e., no other fear was prom-
within the 10–13 and 14–17 years age groups as pre- inent). It may be that the onset of animal fear occurs
dicted for death and danger and for failure and criticism early in development, but it does not take on a develop-
but not animal fears in the 6–9 years age group. Fear of mentally predominant role.
J. AM. ACAD. CH ILD ADO LESC. PSY CH IAT RY, 44:7, JULY 200 5 661WEEMS AND COS TA Only modest evidence was also found suggesting GA that looks at both age at onset of disorder and predom- symptoms as a dominant expression of anxiety in youths inant symptoms in community samples to help clarify aged 10–13 years. Results were somewhat consistent timing issues as well as definitional issues as to what con- with predictions based on child report; however, the he- stitutes a developmentally defined disorder. gemony of GA symptoms in youths aged 10–13 years was not as visually clear as SA at ages 6–9 years, nor Clinical Implications was it confirmed by the planned contrasts or follow-up The salient clinical implication of this study is that within-age group comparisons. In addition, based on greater attention may need to be paid to developmental parent report, Figure 1 suggests SA is still relatively domi- differences in the expression of symptoms in the nant to the other anxious symptoms. Such results are understanding and classification of childhood anxiety consistent with some epidemiological data on the age problems. Emerging research indicates that adult defi- at onset of anxiety disorders that suggest that the average nitions of anxiety disorders such as posttraumatic stress age at onset of GA disorder may sometimes precede that disorder may be inadequate (Carrion et al., 2002) and of SA disorder (Costello et al., 2004). However, fears that developmentally and theoretically based assessment concerning danger and death were clearly the predom- of anxiety disorder symptoms may provide a more sen- inant fear in youths aged 10–13 years. Such findings are sitive assessment than the DSM-IV criteria in young consistent with the idea that the developmental salience children (e.g., Scheeringa et al., 1995, 2001). Although and understanding of mortality in this age group makes this study only examined symptoms and not other death and danger fears dominant. It may be that the diagnosis-relevant information such as interference and broader symptoms of GA do not tap the developmental time frames, it points to the need to test whether the processes as well as the more circumscribed fears of diagnostic criteria for SA and SCA could be improved death and danger. by further developmental modifications. For instance, SCA symptoms and social/performance-related fears clinical tests of the diagnostic criteria for SA disorder were clearly predominant in adolescents aged 14–17 may benefit from examining whether the clinical or pre- years, and results were fairly similar across both child dictive utility of the diagnosis can be improved by, for and parent report of SCA. These findings are consistent example, requiring children aged 6–9 years to display with the idea that emerging social understanding and more symptoms. Indeed dimensional systems for iden- comprehension in adolescence leads to social and eval- tifying pathological internalizing states have recognized uative concerns as the predominant expression of anx- the importance of age differences in the construction of iety in this age group. Such results are very consistent clinical cutoffs (e.g., Achenbach, 1991). The time may with developmental theorizing but do contrast with some be ripe for inclusion of age differences in symptom ex- epidemiological data on the age at onset of SCA disorder pression within categorical systems such as the DSM (Costello et al., 2004). as well. However, clinical tests of this notion that in- Overall, the fairly consistent pattern of results across clude other diagnosis-relevant information are needed reporters depicted in Figure 1 is somewhat remarkable before firm conclusions can be drawn regarding diag- given the low correlation between the parent and child nostic criteria. reports. Taken together with previous research, the re- sults were consistent with theory and suggest that longi- tudinal prospective models of the etiology of childhood Limitations anxiety disorders tracing continuity and change over Despite the important contributions that this inves- time should consider differences in the developmental tigation makes to the understanding of developmental expression of childhood fears and anxiety symptoms. differences in the expression of anxiety and fears in For example, lack of continuity or stability in anxiety youths, the study is not without limitations. In par- disorders over time (e.g., Last et al., 1996) may be due ticular, the models of Westenberg et al. (2001) and to differences in the expression of anxiety at different Warren and Sroufe (2004) posit differential expression ages. The results also point to the utility of a dimensional in children younger than 6 years and youths older than within-subjects approach to identifying developmen- 17 years. Future research is needed to examine, for in- tally predominant symptoms. However, research is needed stance, whether panic symptoms become predominant 662 J. AM . ACAD. CH ILD ADOLESC. PSY CH IATRY, 44:7, JULY 20 05
CH ILD HOOD ANX IETY
in youths older than 17 years as predicted. In addition, Last CG, Perrin S, Hersen M, Kazdin AE (1996), A prospective study of child-
hood anxiety disorders. J Am Acad Child Adolesc Psychiatry 35:1502–1510
it is possible that the developmental expression of anx- Loevinger J (1976), Ego Development: Conceptions and Theories. San Francisco:
ious symptoms is different in youths with different vul- Jossey-Bass
Newman DL, Moffitt TE, Caspi A, Magdol L, Silva PA, Stanton WR
nerabilities for anxiety disorders (e.g., family history (1996), Psychiatric disorder in a birth cohort of young adults: prevalence,
may differentially shape expression). Moreover, our re- comorbidity, clinical significance, and new case incidence from ages 11–21.
cruitment strategy helped normalized anxiety symptom J Consult Clin Psychol 64:552–562
Ollendick TH (1983), Reliability and validity of the revised Fear Survey
distribution (i.e., improved the internal validity of the Schedule for Children (FSSC-R). Behav Res Ther 21:685–692
study) but may be biased compared with a truly epide- Ollendick TH, King NJ, Frary RB (1989), Fears in children and adolescents:
reliability and generalizability across gender, age, and nationality. Behav
miological sampling strategy. Thus, replication in var- Res Ther 27:19–26
ious community, clinical, and at-risk samples is needed. Ollendick TH, Matson JL, Helsel WL (1985), Fears in children and ado-
lescents: normative data. Behav Res Ther 23:465–467
This study is also limited by the cross-sectional nature of Ollendick TH, Yang B, King NJ, Dong Q, Akande A (1996), Fears in
the investigation. Although part of the purpose of this American, Australian, Chinese, and Nigerian children and adolescents:
a cross-cultural study. J Child Psychol Psychiatry 37:213–220
study was to provide a cross-sectional explanation for Pina A, Silverman WK, Saavedra LS, Weems CF (2001), An analysis of the
inconsistencies in longitudinal findings, studies are RCMAS lie scale in a clinic sample of anxious children. J Anxiety Disord
now needed that examine differential symptom expres- 15:443–457
Pine DS, Cohen P, Gurley D, Brook J, Ma Y (1998), The risk for early-
sion over time and examine both the onset and the dif- adulthood anxiety and depressive disorders in adolescents with anxiety
ferential expression of anxiety. Cross-sequential designs and depressive disorders. Arch Gen Psychiatry 55:56–64
Reynolds CR, Richmond BO (1978), What I think and feel: a revised mea-
examining both age group differences and longitudinal sure of children’s manifest anxiety. J Abnorm Child Psychol 6:271–280
trends would be particularly useful in this regard. Scheeringa MS, Zeanah CH, Drell MJ, Larrieu JA (1995), Two approaches
to the diagnosis of posttraumatic stress disorder in infancy and early
childhood. J Am Acad Child Adolesc Psychiatry 34:191–200
Disclosure: The authors have no financial relationships to disclose. Scheeringa MS, Peebles CD, Cook CA, Zeanah CH (2001), Toward estab-
lishing procedural, criterion, and discriminant validity for PTSD in early
childhood. J Am Acad Child Adolesc Psychiatry 40:52–60
Silverman WK, Treffers PDA, eds. (2001), Anxiety Disorders in Children and
REFERENCES Adolescents: Research, Assessment and Intervention. Cambridge, UK:
Cambridge University Press
Achenbach TM (1991), Manual for the Child Behavior Checklist/4-18 and Tabachnick G, Fidell LS (2001), Using Multivariate Statistics, 4th ed. Boston:
1991 Profile. Burlington: University of Vermont, Department of Psychiatry Allyn & Bacon
American Psychiatric Association (1987), Diagnostic and Statistical Manual of Vasey MW, Dadds MR, eds. (2001), The Developmental Psychopathology of
Mental Disorders, 3rd edition-revised (DSM-III-R). Washington, DC: Anxiety. London: Oxford University Press
American Psychiatric Association Warren SL, Sroufe LA (2004). Developmental issues. In: Phobic and Anxiety
American Psychiatric Association (1994), Diagnostic and Statistical Manual of Disorders in Children and Adolescents: A Clinician’s Guide to Effective Psy-
Mental Disorders, 4th edition (DSM-IV). Washington, DC: American chosocial and Pharmacological Interventions, Ollendick TH, March JS,
Psychiatric Association eds. New York: Oxford University Press, pp 92–115
Carrion VG, Weems CF, Eliez S et al. (2001), Attenuation of frontal lobe Weems CF, Hammond-Laurence K, Silverman WK, Ginsburg GS (1998),
asymmetry in pediatric PTSD. Biol Psychiatry 50:943–951 Testing the utility of the anxiety sensitivity construct in children and ado-
Carrion VG, Weems CF, Ray R, Reiss AL (2002), Towards an empirical lescents referred for anxiety disorders. J Clin Child Psychol 27:69–77
definition of pediatric PTSD: the phenomenology of PTSD symptoms Weems CF, Hayward C, Killen JD, Taylor CB (2002), A longitudinal in-
in youth. J Am Acad Child Adolesc Psychiatry 41:166–173 vestigation of anxiety sensitivity in adolescence. J Abnorm Psychol
Chorpita BF, Yim L, Moffitt C, Umemoto LA, Francis SE (2000), 111:471–477
Assessment of symptoms of DSM-IV anxiety and depression in chil- Weems CF, Silverman WK, Saavedra LS, Pina AA, Lumpkin PW (1999),
dren: a revised child anxiety and depression scale. Behav Res Ther 38: The discrimination of children’s phobias using the Revised Fear Survey
835–855 Schedule for Children. J Child Psychol Psychiatry 40:941–952
Costello EJ, Egger HL, Angold A (2004), Developmental epidemiology of Westenberg PM, Drewes MJ, Siebelink BM, Treffers PDA (2004), A devel-
anxiety disorders. In: Phobic and Anxiety Disorders in Children and Ado- opmental analysis of self-reported fears in late childhood through mid-
lescents: A Clinician’s Guide to Effective Psychosocial and Pharmacological adolescence: social-evaluative fears on the rise? J Child Psychol Psychiatry
Interventions, Ollendick TH, March JS, eds. New York: Oxford Univer- 45:481–496
sity Press, pp 61–91 Westenberg PM, Siebelink BM, Treffers PDA (2001), Psychosocial devel-
Curry JF, March JS, Hervey AS (2004), Comorbidity of childhood and ad- opmental theory in relation to anxiety and its disorders. In: Anxiety
olescent anxiety disorders. In: Phobic and Anxiety Disorders in Children Disorders in Children and Adolescents: Research, Assessment and Interven-
and Adolescents: A Clinician’s Guide to Effective Psychosocial and Pharma- tion, Silverman WK, Treffers PDA, eds. Cambridge, UK: Cambridge
cological Interventions, Ollendick TH, March JS, eds. New York: Oxford University Press, pp 72–89
University Press, pp. 116–140 Westenberg PM, Siebelink BM, Warmenhoven NJ, Treffers PDA (1999),
Jaccard J, Guilamo-Ramos V (2002), Analysis of variance frameworks in clini- Separation anxiety and overanxious disorders: relations to age and level
cal child and adolescent psychology. J Clin Child Psychol 31:130–146 of psychosocial maturity. J Am Acad Child Adolesc Psychiatry 38:1000–1007
J. AM. ACAD. CH ILD ADO LESC. PSY CH IAT RY, 44:7, JULY 200 5 663You can also read