Demonstrating Efficacy via Surrogate Endpoints - May 2021 - Blue Matter ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Demonstrating Efficacy via
Surrogate Endpoints
May 2021
© 2021 Blue Matter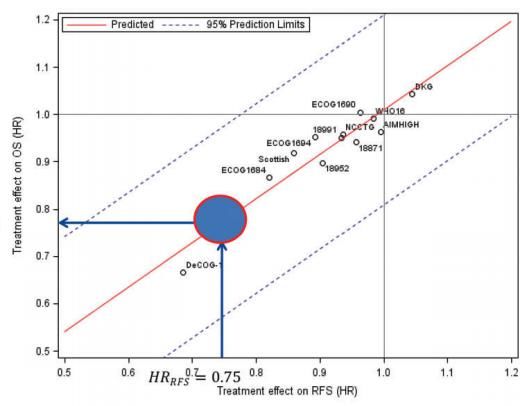
New Ideas. Better Results.
A strategic consulting firm serving the life science industry.
To learn more about Blue Matter, visit www.bluematterconsulting.com
© 2021 Blue Matter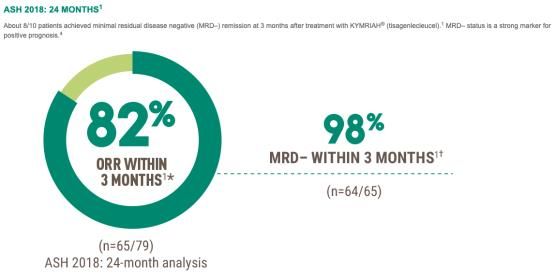
Introduction
Surrogate endpoints are expected to gain greater significance in reimbursement and access decisions, as better
diagnosis and treatment turn previously deadly diseases into chronic manageable conditions. However, many
challenges exist with surrogate validation, with regulators and different payers having inconsistent requirements.
In this now expanded review, we look at the regulatory and payer guidance on this topic, as well as several case studies
of successful and not-as-successful surrogate validation:
Disease Infectious
CV Oncology / hematology
areas disease
Keytruda Kymriah Polivy Gazyva
Sovaldi Praluent Perjeta Perjeta
Products NNRTI (pembrolizu- (tisagenlec (polutuzumab (obinutuzu
(sofosbuvir) (alirocumab) (pertuzumab) (pertuzumab)
mab) -leucel) vedotin) -mab)
Surrogate Virologic CR, PFS,
SVR12 LDL-c DFS RFS pCR CR, MRD MRD, PFS
endpoints response others
Lastly, we summarize current challenges and steps pharma could take to increase their chances of success with
product development via surrogate endpoints.
© 2021 Blue Matter 3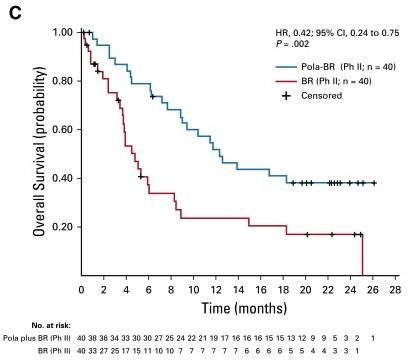
Glossary
AA accelerated approval ITT intention-to-treat
AE adverse event LDL low-density lipoprotein
ASMR improvement in medical benefit (amélioration du service médical rendu) MAA marketing authorization application
CADTH Canadian Agency for Drugs and Technologies in Health MoA mechanism of action
CDF Cancer drug fund NICE National Institute for Health and Care Excellence
CI confidence interval N+ lymph node positive
CV cardiovascular OS overall survival
DFS disease-free survival pERC pan-Canadian Oncology Drug Review expert review committee
eBC early breast cancer pCR pathological complete response
EFS event-free survival PFS progression-free survival
Joint federal committee of German public health agencies (Gemeinsamer
G-BA QALY quality-adjusted life year
Bundesausschuss)
HAS French National Authority of Health (Haute Autorité de Santé) R correlation coefficient
HCC hepatocellular carcinoma RCT randomized controlled trial
HCV hepatitis C virus RFS relapse-free survival
HR hazard ratio SoC standard of care
HR hormone receptor STE surrogate threshold effect
IFN interferon SVR sustained virologic response
Institute for Quality and Efficiency in Health Care (Institut für Qualität und
IQWIG Tx treatment
Wirtschaftlichkeit im Gesundheitswesen)
VR virological response
© 2021 Blue Matter 4
Table of
Contents
01 Background and Context
02 Payer Guidance
03 Case Studies
04 Challenges and Opportunities
© 2021 Blue Matter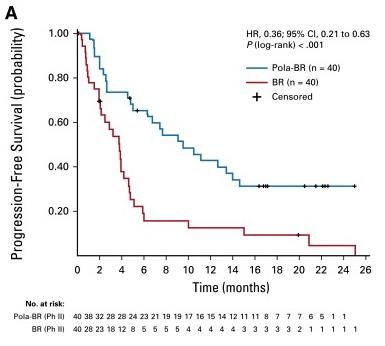
Surrogate endpoints are increasingly important as previously deadly diseases
become chronic conditions through better diagnosis and treatment
Surrogate “A clinical trial endpoint used as a substitute for a direct measure of how a patient feels, functions, or survives. When a
endpoint surrogate endpoint clearly predicts a beneficial effect through appropriate studies, its use generally allows for more efficient
drug development programs.” - FDA
Application in different disease areas:
In oncology / heme, better treatment In long-term diseases such as HCV, HIV and • For rare diseases, unmet medical needs
options are extending life and drug cardiovascular disease, surrogate are supportive of surrogate endpoints, but
development is increasingly moving to early endpoints are used, given challenges of data scarcity often means potential
stages of disease e.g., (neo)adjuvant measuring long-term outcomes (long surrogates are not well validated /
• Trials with OS are often unfeasible, and duration, rare events). understood.
surrogates are used • Given the complexity of developing
• The proportion of oncology marketing endpoints for rare diseases, we will
authorization applications (MAAs) which address this in a separate analysis.
had immature OS doubled between 2009-
2013 (19%) and 2013-2017 (39%)1
© 2021 Blue Matter 6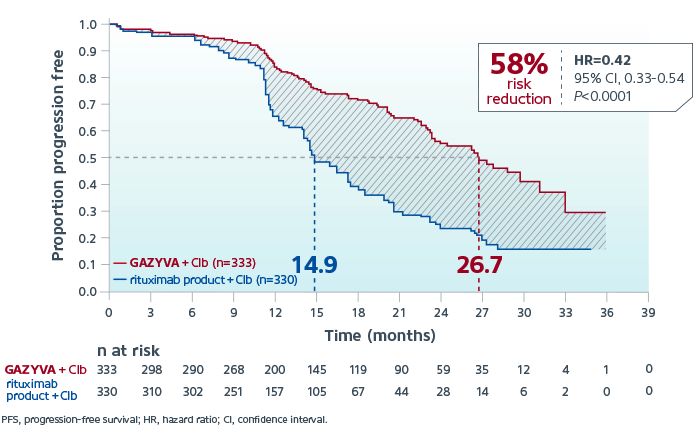
Regulators accept many surrogate endpoints for traditional and accelerated/
conditional approvals
100 89
80
60
80% 100% 40
17
20 11
0
80% of accelerated 100% of
Traditional approval Accelerated approval Traditional or
assessments conditional approvals accelerated
between 2011-2018 were based on surrogates1 The FDA has accepted >120 surrogate endpoints2-4
© 2021 Blue Matter 7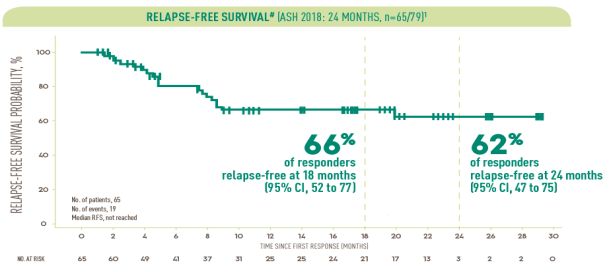
Validation of surrogates requires patient-level and trial-level data; clear rationale and
biological plausibility are also supportive of validation
Considerations for surrogate validation5-8
True endpoint (e.g., OS)
Statistical evidence:
Rationale: why surrogate endpoint Patient-level association: the surrogate
is preferred (e.g., high unmet need, and the true endpoint correlate on a patient-
rare events, long follow-up, difficult level irrespective of treatment. This can be
to measure true endpoint) done in a single trial and is of prognostic Regression
value (e.g. useful for patient management) Patient
Surrogate endpoint (e.g., DFS)
true endpoint (e.g., OS HR)
Statistical evidence:
Treatment effect in
Biological plausibility: association Trial-level association: treatment effect on
between disease mechanism, the surrogate correlates the treatment effect
surrogate and true endpoint (e.g., on the true endpoint. Meta-analysis required,
epidemiologic evidence, animal ideally with data from similar studies (class
models, disease pathogenesis, drug of drug, treatment duration etc). It is of Regression
mechanism) predictive value and useful for assessing the Trial
benefit of new treatments Treatment effect in surrogate (e.g., DFS HR)
Strength of evidence:
Limited
© 2021 Blue Matter High 8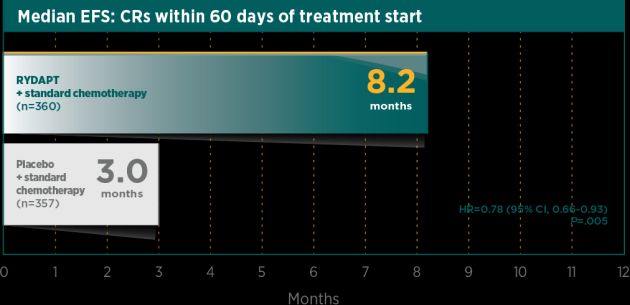
Where trial-level association is insufficiently clear, the Surrogate Threshold Effect
(STE) can be used to demonstrate validity
Surrogate Threshold Effect (STE)9
STE: Threshold by which treatment effect on the surrogate would predict
a statistically significant effect on the true endpoint. It is particularly STE
useful when trial-level association is considered insufficient.
No significant effect
on true endpoint
Significant effect
on true endpoint
true endpoint (e.g., OS HR)
Treatment effect in
Example: A meta-analysis of the correlation between OS and PFS in
metastatic breast cancer finds that the STE for HR PFS = 0.6. This means
that if a treatment (of the same class and in the same indication) achieves 1.0
HR PFS of below 0.6, this predicts a significant, positive effect on OS. Regression
95% CI
No effect on OS
G-BA/IQWIG has an additional, stricter preference that the entire 95% CI Treatment effect in surrogate
(e.g., DFS HR)
of HR PFS should be below the STE, not just the HR PFS itself 10 (please
see slide 13). The aim is to decrease false positives, but in practice, it is
extremely difficult for studies to fulfil the G-BA/IQWIG requirements.
© 2021 Blue Matter 9
Assessment by Cortazar et al., on pCR was an early example of patient and trial level
analysis and highlights need for trial-level association
Patient-level
• Cortazar et al.11(at the FDA) investigated the validity of pathological complete response (pCR) as
a surrogate for OS in breast cancer treated with neoadjuvant chemo
• The study included data from 12 international neoadjuvant trials (11955 patients for patient-level
analysis and 9440 patients for trial-level analysis)
– Patients who achieved pCR had higher OS with a HR of 0.36 on patient-level association
– However, trial-level analysis showed that change in pCR did not correlate with change in OS
Trial-level
• This suggest that while pCR is of prognostic value for individual patients, there is limited predictive
value for therapies. There are several explanations of why this may be the case:
– Heterogeneity in breast cancer types, which may respond differentially to treatment
– Absolute differences in pCR was relatively small in most trials (chemo only), which could have
obscured association R2 = 0.24
FDA and EMA both approved Perjeta in this setting based on pCR data. However, this acceptance is challenged in the
academic literature12,13 and by payers (please see case study of Perjeta).
© 2021 Blue Matter 10Payer Guidance on Surrogates
© 2021 Blue MatterEUnetHTA has published guidelines on surrogate endpoint assessment, outlining
three-levels of validation based on trial/patient association and biological plausibility
Similar to regulators, EUnetHTA (2013) suggest a three-level categorization14, 15:
no consensus, but correlation values
Level 1 Trial-level association (meta-analysis of multiple RCTs) of 0.85 to 0.95 often discussed; STE
can be used if correlation is lower
Patient-level association (epidemiological/observational studies/single
Level 2
RCT)
Important but insufficient15
Biological plausibility (pathophysiological studies and/or understanding of
Level 3
disease process)
EUnetHTA considers the the validation of surrogates to be:
✔ Disease-specific (stage of disease-specific) ✘ Never definite (can change based on new data)
✔ Population-specific e.g. age, gender, comorbidities
✔ Technology(/drug class)-specific
© 2021 Blue Matter 12Some national payer agencies have also developed guidance, with CADTH, IQWiG
and NICE providing the most detail on methodological requirements
Agency Methods for validation of surrogate endpoints16
Considers surrogates as valid if there is a “strong, independent, consistent association” with the true endpoint and there is “evidence from
randomized trials that […] improvement in the surrogate end point has consistently lead to improvement in the target outcome.” In oncology,
the use of a surrogate outcome in health technology assessments must be accompanied by extrapolations to OS. Three types of
relationships are possible depending on the best available evidence accompanied by appropriate justification:
• The surrogate outcome is entirely predictive of OS.
CADTH17
• The surrogate outcome is somewhat predictive of OS.
(Canada)
• The surrogate outcome has no proven relationship with OS.
Analysis of patient-level and trial-level association is the preferred method (including potential application of the STE), and trial-level
association is the most relevant for determining surrogacy in benefit assessments (summary of guideline on slide 18)
IQWiG10
(Germany)
No specific guidelines on surrogate validation but state that “the uncertainty associated with the relationship between the endpoint and health-
related quality of life or survival should be explored and quantified” In addition, instead of criteria about the correlation, it is important to look at
predicted estimates and their uncertainty because the strength (or weakness) of the surrogate relationship will manifest itself in the
width of the predicted interval of the treatment effect on the final outcome.
“Multivariate meta-analytic methods provide such a framework as they, by definition, take into account the correlation between the
NICE (UK)18-19
treatment effects on the surrogate and final outcomes as well as the uncertainty related to all parameters describing the surrogate
relationship.”
© 2021 Blue Matter 13IQWiG has the most specific, if stringent criteria, for surrogate validity
IQWiG considers four levels for surrogate validity 1) proof 2) indication, 3) hint, 4) no proof. This is determined mainly by the reliability of the
validation evidence (i.e. the quality, quantity and suitability of data in the validation study) and by the strength of trial-level association10
Strength of correlation
Considers the degree of trial-level association between the surrogate and true endpoints
Medium (Lower bound of 95% CI of R,
High (Lower bound of 95% CI of R ≥ 0.85) Low (Lower bound of 95% CI of R ≤ 0.7)
0.7 < R < 0.85)
Proof of validity, conclusions on true Proof of lack of validity, no proof of effect
High 1
endpoint possible on true endpoint
Reliability of validation Limited 2
evidence Unclear validity, effect on true endpoint dependent on effect size and STE
Considers certainty of results
(number of studies, Moderate 3
transferability of results)
Low Unclear validity, no proof of effect on true endpoint
If 95% CI of surrogate treatment effect If 80% CI of surrogate treatment effect If 80% CI of surrogate treatment effect not
wholly below STE wholly below STE wholly below STE
Unclear validity, 1 - High reliability Proof of validity Indication of validity No proof of effect on true endpoint
effect on true
endpoint dependent 2 - Limited reliability Indication of validity Hint of validity No proof of effect on true endpoint
on effect size and
STE 3 - Moderate reliability Hint of validity No proof of effect on true endpoint
In addition, the validity of the surrogate endpoint can be downgraded, e.g. high risk of bias, discrepancies in treatment durations between study arms of validation trials
The table assumes that the validation shows a positive correlation
between surrogate and true endpoints (slope of regression not equal to 0).
© 2021 Blue Matter 14Case Studies on Payer Assessment of
Surrogate Endpoints
© 2021 Blue MatterWe chose Germany, France and UK for in-depth review given their high evidence
requirements, international influence and in-depth publications
Publication of
Countries Commercial potential High evidence requirements International influence Selection of analysis
HTA results
US ✓✓✓ ✓ ✓✓ ✓✓
Germany ✓✓ ✓✓✓ ✓✓✓ ✓✓✓ Selected
France ✓✓ ✓✓✓ ✓✓✓ ✓✓✓ Selected
UK ✓ ✓✓✓ ✓✓✓ ✓✓✓ Selected
Canada ✓ ✓✓✓ ✓✓ ✓✓ Some analogs examined
Italy ✓ ✓ ✓✓ ✓
Spain ✓ ✓ ✓✓ ✓
Japan ✓✓ ✓✓ ✓✓ ✓
✓ Low ✓✓✓ High
16
© 2021 Blue MatterValidation of surrogates for payer assessments is highly challenging. Here we
outline a few successful (and not as successful) validations to identify learnings (1/2)
For the case studies, we focus on a few examples that deliver unique learnings. We also focus on 4 markets which publish detailed evaluations.
Disease Drug/classes Surrogate True
Indication G-BA NICE/ SMC HAS CADTH
area examined endpoint endpoint
Surrogate Overall Surrogate Overall Surrogate Overall Surrogate Overall
SVR24,
Sovaldi Chronic
SVR12 HCC,
Infectious (sofosbuvir) Hepatitis C
mortality
disease
virologic Risk of
NNRTI HIV
response AIDS/death
Primary
Cardio- Cardio-
Praluent
hypercholester
vascular LDL-c vascular
(alirocumab)
olemia / mixed
disease events
dyslipidemia*
Perjeta HER2+ eBC
DFS OS
(pertuzumab) adjuvant
Keytruda
Adjuvant
Oncology (pembro- RFS OS
melanoma
lizumab)
Perjeta Neo-adjuvant
pCR OS*
(pertuzumab) HER2+
NOTE: to highlight the impact of surrogate endpoints on assessment outcomes, we reviewed the first payer assessments in the
relevant indications. Additional payer assessments may have since been conducted. * The indication in Canada is heterozygous Favorable Unfavorable
familial hypercholesterolemia or clinical atherosclerotic cardiovascular disease Intermediate Not evaluated by HTA
17
© 2021 Blue MatterValidation of surrogates for payer assessments is highly challenging. Here we
outline a few successful (and not as successful) validations to identify learnings (2/2)
For the hematology case studies, we focus on a few examples that deliver unique learnings. We also focus on 3 markets which publish detailed
evaluations.
Disease Drug/classes Surrogate True
Indication G-BA NICE HAS
area examined endpoint endpoint
Surrogate Overall Surrogate Overall Surrogate Overall
Polivy CR/PFS/
r/r DLBCL OS
(polatuzumab) others
Kymriah
Hemato- (tisagenlec- r/rALL CR/MRD OS
logy leucel)
Gazyva
1L CLL MRD/PFS OS
(obinutuzu-mab)
NOTE: to highlight the impact of surrogate endpoints on assessment outcomes, we reviewed the first payer assessments in the
relevant indications. Additional payer assessments may have since been conducted. Favorable Unfavorable
* CADTH considered EFS Intermediate Not evaluated by HTA
18
© 2021 Blue MatterSovaldi in HCV: sustained virological response (SVR) is accepted as a surrogate
based on precedence and patient-level association
Countries Surrogate validity6 Evaluation Reasons
Treatment-naive/Genotype 2: significant improvement of
Not a validated surrogate per se due to missing validation studies. Depending on
SVR combined with possibility to have interferon-free
However, SVR is considered a sufficiently validated surrogate for subgroup: indication
regimen with reduced AE
Germany occurrence of HCC since a meta-analyses25-28 showed a clearly lower of considerable
Other subpopulations with hint of minor added benefit: only
(July 2014) risk for patients who achieved SVR. The additional benefit is considered added benefit / hint of
single arm studies show SVR and AEs, but reduced
non-quantifiable since the data comes from observational studies. minor added benefit /
treatment duration with less AEs
Insufficient data for assessing surrogacy for other endpoints (e.g., OS). no additional benefit20
No benefit: insufficient data for other subgroups
Validity of SVR for HCC risk or OS not directly addressed. However, TC
ASMR II for all except The clinical data suggest Sovaldi alone or in combination
report states “the aim of treatment is to cure the infection, defined by
for treatment-naive with other molecules can help cure the majority of
France SVR... after the end of treatment”
genotype 3; ASMR III patients with HepC with or without non-liver complications.
(May 2014) Also referenced relationship between SVR12 and SVR24 “agreement
for treatment-naive The product’s place in the therapeutic strategy should be
between SVR12 and SVR24… demonstrates a positive indicative value of
genotype 3 21 reassessed as more therapies are approved.
99% and a negative indicative value of 99%”
Not directly addressed but accepted based on historical precedence
Recommended for
“company submitted a multi-state Markov model… People who had Concerns about the robustness of the clinical
UK certain treatment/
antiviral treatment could move into the non-cirrhotic or SVR cirrhotic effectiveness across different subgroups given that most
(Feb 2015) genotype
health states...” “model was broadly consistent with previous models trials were single-arm and open-label
subgroups22
considered in NICE technology appraisals for hepatitis C24”
SVR at 12 weeks is accepted as a valid surrogate for SVR at 24 weeks
Recommended for
Canada since a meta-analysis of 15 Phase 2 and 3 studies showed a positive and Various single-arm studies and RCTs show high rates of
certain genotype 1-3
(Jan 2018) negative predictive value of >98%; no commentary on validation of SCV in subgroups of patients infected with genotypes 1-3
subpopulations23
SVR against HCC / survival
Please see next slide for a summary of meta-analyses in HCV. Many payers did not even question the relationship between SVR and true endpoints such as HCC / death
Acronyms: HCC hepatocellular carcinoma, SVR sustained virological response Favorable Intermediate Unfavorable
© 2021 Blue Matter 19Sovaldi benefitted from decades of research on HCV, with strong, consistent patient-
level association demonstrated over multiple meta-analyses More studies exist but not
summarized given large body of data
Publication
Cited by Scope Outcome of meta-analysis Conclusions
year
• Incidence rates (per 100 person-years) of HCC, liver-related
• 307 chronic HCV patients with bridging fibrosis or complications, and liver-related death, were 1.24, 0.62, and
cirrhosis were analysed 0.61 among SVR patients, and 5.85, 4.16, and 3.76 among non-
NICE24 2010
• Treatments with peginterferon and ribavirin SVR patients
• Median follow up of 3.5 years post treatment • Non-SVR was an independent predictor of HCC (HR 3.06), liver-
related complications (HR 4.73), and liver-related death (HR 3.71) SVR is durable
and strongly
• 26 observational cohort studies of HCV treatment • Patients with SVR are significantly less likely to develop liver- correlated with
G-BA25 2010 failure patients related mortality (relative risk [RR], 0.23), HCC (RR, 0.21), or patient-level
• Study follow up duration is 2.8-11 years hepatic decompensation (RR, 0.16) outcomes
• SVR was durable (98.4%–100%)
• 6 cohort studies with at least 2 years of follow up
• SVR reduced liver-related mortality among patients with chronic
G-BA16 2011 data (2.1-9.8 years)
HCV (3.3- to 25-fold), the incidence of hepatocellular carcinoma
• Tx: IFN, IFN/RBV, or PEG-IFN/RBV
(1.7- to 4.2-fold), and hepatic decompensation (2.7- to 17.4-fold)
• SVR at 4 and 12 weeks vs SVR at 24 weeks SVR 12 is
• 15 phase 2 and 3 trials, 3 pediatric studies, and 5
• The positive predictive value of SVR12 was 98% and the negative highly
drug development programs
CADTH27 2013 predictive value was 99% for SVR24 correlated with
• Interventions: interferon, pegylated-interferon,
• About 2% of subjects who achieved an SVR12 subsequently SVR 24; SVR12
ribavirin, and direct-acting antivirals
relapsed by week 24 is also durable
As a surrogate endpoint, SVR has clear biological plausibility and strong patient-level association. Payers accepted it despite lack of trial-level association and
heterogeneous data from different MoAs (HCV polymerase inhibitor vs. interferon, nucleoside inhibitor). Of note, G-BA/IQWiG considered the additional benefit
based on surrogate endpoint unquantifiable (data quality issues), but upgraded the benefit in certain subgroups based on reduced AEs
© 2021 Blue Matter 20Similar to HCV, modern antivirals for HIV benefited from decades of research that
demonstrated strong patient-level correlation
“No clear correlation has been found between effects of the intervention on the surrogate and the patient-relevant outcome
that the surrogate is supposed to replace. Nevertheless… the Institute considers the surrogate to have “sufficient
validity” is justified, particularly in view of the dramatic improvements in prognosis for HIV patients in terms of
IQWIG28: survival and progression of the disease… The increased uncertainty is taken account of by the rating assigned to the
extent of the added benefit (rating of any added benefit as “non-quantifiable”)”.
“Drug studies aimed at reducing the viral load have led to a dramatic improvement in the prognosis for HIV patients with
regard to survival and onset of the disease in everyday (real-world) treatment.
✔ The biological model is plausible
✔ The correlation between the individual change in viral load and the risk of AIDS-defining diseases / death is very clear
• Data at study level (meta-regressions) also do not contradict this association, even if there is hardly any clear
correlation between the effects on the surrogate and the effects on the patient-relevant endpoint “AIDS-defining
G-BA29: diseases / death”. In these studies, the association is likely to be watered down by the inclusion of many non-inferiority
(close to zero) studies.
For this reason, the extent of the added benefit for the combined outcome “AIDS-defining diseases / death” cannot be
quantified on the basis of the surrogate."
Payers in other countries examined (France, UK, Canada) all accepted the validity of VR for modern antivirals without
HAS, NICE, significant discussions “CD4 cell counts and viral suppression are well-accepted markers of future clinical events.”
CADTH:
© 2021 Blue Matter 21LDL-C in Praluent (primary hypercholesterolemia or mixed dyslipidemia): payers in
different countries reached different conclusions on surrogate validity
Countries Surrogate validity Evaluation Reasons
No commentary on surrogate endpoint by G-BA since it considered LDL-C levels were considered not patient-relevant since
Germany
none of the submitted studies were relevant for the benefit No proof of the significant reduction in LDL-C levels did not translate
(May
assessment; IQWiG considers LDL-c to be a non-validated additional benefit30 into differences in patient-relevant endpoints such as
2016)
surrogate (please see next slide) reduced cardiovascular events.
The efficacy was evaluated only in the reduction of LDL-
C levels and there is no data justifying the efficacy of
TC considered LDL a biological criteria rather than morbidity or
France alirocumab in terms of morbidity and mortality
mortality-related endpoint; no specific comments on validation of Insufficient benefit31
(Apr 2016) (Later obtained ASMR 4 based on reduction in
LDL as a surrogate for CV outcomes or mortality
apheresis frequency in a high unmet need
subpopulation)
The company presented the Navarese meta-analysis data from
UK PCSK9 inhibitor trials which showed decreasing LDL-C levels
Recommended for Treatment was considered cost-effective using either the
(June decreases all-cause/CV mortality. NICE considers the larger and
NHS use32 Navarese or the CTTC validation studies
2016) more well validated CTTC meta-analysis of statins to be the
more appropriate data
LDL‐C is widely accepted as a valid indicator of CV risk, based
Canada on evidence from clinical studies that have shown that changes in
Reimbursement Significant lowering of LDL-C levels and cost-effective (if
(July LDL‐C are correlated with the incidence of CAD‐related clinical
recommended33 discount is granted)
2016) events, and LDL‐C has been used as a surrogate end point in other
studies of PCSK9 inhibitors, including evolocumab
Favorable Intermediate Unfavorable
© 2021 Blue Matter 22IQWiG considers LDL-c as a non-validated surrogate endpoint for mortality, coronary
mortality and non-fatal myocardial infarctions
Assessment Selected analysis outcome / additional
Product Method Conclusion
year comments
Meta-regression across 14
studies; correlation of LDL-c “No statistically significant association was shown between the
reduction to total mortality, degree of the difference of relative LDL cholesterol lowering and
Statins34 2006
coronary mortality, and non- the degree of event reduction, neither for total mortality, nor for
fatal myocardial infarctions coronary mortality, nor for non-fatal myocardial infarctions”
were assessed
If LDL-C was the sole cause of CV events,
then progression rates at the same level of
”Undisputed that LDL is contributing to CV events, but LDL
Review of atorvastatin and LDL-c for atorvastatin and pravastatin
Ezetimibe35 2010 lowering per se has no patient relevant benefit since there is
pravastatin data should be the same, but atorvastatin is
no proof of a causal relationship”
consistently lower. Thus, there must be a
substance specific effect
IQWiG considered that the
”LDL-C is at most a surrogate. The literature provided by the
company presented no valid
Lomitapide36 2015 company [4-20] also did not show that LDL-C is a (sufficiently) No specific meta-analysis provided for HoFH
data to demonstrate
valid surrogate for cardiovascular events in patients with HoFH”
surrogacy
Not explicitly stated why Navarese and CTTC
Not specific validation study “Lowering of LDL-C levels... constituted a non-validated surrogate meta-analyses were not considered, but given
Praluent37 2016
discussed outcome in the present constellation” broader comments, IQWiG may consider the
patient population to be different
© 2021 Blue Matter 23In oncology, payers scrutinize for trial-level association. As a case study, we examined
(i)DFS for Perjeta in adjuvant breast cancer (N+ or HR-)
Company Roche Trial results
FDA / EMA • Adjuvant chemo + trastuzumab +/- pertuzumab
Dec 2017 / May 2018
approvals • Trial included patients which were HER2+ independent of HR-
status with either N+ or high-risk N-
In combination with trastuzumab and chemotherapy as
• Small but significant effect on ITT: iDFS HR of 0.81 (p = 0.045)
Indication an adjuvant treatment of patients with HER2+ early
breast cancer at high risk of recurrence (N+ or HR-) • Larger effect on node-positive (N+): iDFS unstratified
HR of 0.77 (p = 0.02)
Study of • OS data immature (HR = 0.89, p = 0.47)
APHINITY (NCT01358877)
interest
Surrogate validity data38,39 Statistical model
• Roche argued that (i)DFS is an appropriate surrogate for OS in this setting, since • Patient-level association: joint distribution of the
mortality is low in early HER2+ breast cancer and trials would therefore require very surrogate endpoint and the true endpoint were
long observation periods for mature OS data estimated with a copula-based model (Clayton’s,
• Roche provided two validation studies (one for iDFS39 and one for DFS38) which both Hougaard’s or Plackett’s) which provided the maximum
include 8 trials with 21,480 patients of HER2-targeted therapies in combination with likelihood value. Strength of association was
chemo with identical treatment duration determined using Spearman’s rank correlation
coefficient
• Subgroup analysis was performed to only include Perjeta target groups (early HER2+,
HR- or N+, treated with HER2-therapy); the R value for the patient-level association • Trial-level association: Proportional hazards model
between OS and DFS was 0.90, and the R2 for the trial-level association between was used to estimate HRs for DFS and OS. Linear
HROS and HRDFS was between 0.75 [95% CI 0.5-1.0] and 0.84 [95% CI 0.67-1.0] regression on log-transformed HRs
• The surrogate threshold effect was estimated to be between 0.56 and 0.81 • In all analysis, the estimation error for estimated HRs
depending on the number of deaths in the trial (since the regression models were was taken into account using a measurement-error
weighted by number of a deaths ) model (or if not possible a weighted regression model)
iDFS: time from randomization until the date of the first occurrence of one of the
following events (hereafter referred to as invasive-disease events): recurrence of
ipsilateral invasive breast tumor, recurrence of ipsilateral locoregional invasive © 2021 Blue Matter 24
disease, a distant disease recurrence, contralateral invasive breast cancer, or
death from any causeWhile methodologically correct, payers were generally unconvinced of the results of
the trial-level association, which fell below STE specified by IQWiG
Countries Surrogate validity Evaluation Reasons
The validation study is adequate to probe the surrogate validity and shows
a medium correlation between DFS and OS (i.e., lower boundary of 95% The significant, albeit moderate reduction in relapse rate
CI of 0.7 < R < 0.85) meaning the validity is unclear and STE has to be and (i)DFS is patient-relevant and outweigh the increased
Germany Hint for minor
considered. While Perjeta’s effect on DFS HR was significant, it did rate of AE. "The endpoint “disease-free survival (DFS)” is
(Jan 2019) not meet the STE criteria (i.e. 95% CI of DFS HR [0.64,0.96] was not additional benefit40
included in the present assessment as an independent,
wholly below STE 0.80-0.82). Hence, no significant effect on OS can be patient-relevant endpoint"
inferred from the size of Perjeta’s treatment effect on DFS
While not specifically assessed as a surrogate, TC did consider iDFS data
France No clinically relevant benefit on iDFS combined with
in its assessment. However, TC concluded that the change in iDFS of Insufficient benefit41
(Jun 2019) increased toxicity
1% too low to be clinically relevant
Acknowledges difficulty in obtaining mature OS data for adjuvant Recommended for N+ patients as cost-effectiveness is
Recommended for
UK treatment. States that in the absence of OS, iDFS is the only available comfortably below £20k/QALY. Incremental treatment
use within NHS for
(Mar 2019) data for decision-making, though the extent to which iDFS translates benefit in ITT is likely to be small but absolute benefit in N+
N+ subgroup42
into OS benefit is not known likely to be greater.
In the final decision, the pERC concludes that (i)DFS is not yet a No clinically meaningful benefit as no proven difference in
validated surrogate for OS in this setting, though the Clinical Guidance OS, and high level of uncertainty around iDFS benefit
Canada Reimbursement not
Panel states that in the absence of an OS benefit, the surrogate iDFS is given the trial was not designed to detect treatment
(Nov 2018) recommended43
likely a reasonable endpoint for decision making and that there is likely a effects within subgroups (N+ vs N- or HR- vs HR+).
small but clinically meaningful clinical benefit in N+. Could not draw conclusions on cost-effectiveness.
Favorable Intermediate Unfavorable
© 2021 Blue Matter 25In contrast, Keytruda validation of RFS produced trial-level association which was
comfortably below the STE in adjuvant node+ melanoma
Company Merck Trial results
FDA / EMA • Adjuvant pembro vs placebo in stage III N+ melanoma
Feb 2019 / October 2018
approvals • Patients stratified by PD-L1 expression (positive vs negative)
Adjuvant treatment of patients with melanoma with • 12 mos RFS: 75.4% with pembro vs 61.0% with placebo
Indication involvement of lymph node(s) following complete (HR = 0.57, pEven then, NICE pERG cautioned against using RFS as a surrogate given concerns
over tx & patients included, statistical assumptions and changing tx paradigms
Countries Surrogate validity Evaluation Reasons
RFS is patient-relevant and results showed a clear, clinically
RFS considered as patient-relevant endpoint in the category of Indication of non-
Germany relevant benefit of pembro which was of unquantifiable
“morbidity” (not a surrogate); no specific discussion on surrogate quantifiable added
(Mar 2019) benefit due to short observation period. In terms of AE,
validation identified benefit46
pembro has a clear disadvantage.
While RFS validity as a surrogate was not directly assessed, RFS data Moderate
Evaluation takes into consideration superiority of RFS vs
France was key to the positive TC evaluation; in effect, TC considered RFS to improvement in
placebo, significant medical need given high recurrence
(Jun 2019) be an appropriate endpoint in measuring clinical benefit in the actual benefit
rate, AE profile and immature OS data
adjuvant setting (ASMR III)47
While the meta-analysis suggests the HR achieved by pembro should be
sufficient to predict a treatment benefit on OS, the evidence review group
cautioned against using it as a surrogate given i) data comes from Recommendation based on high unmet need in stage III
UK interferon treatment which is not used in NHS, ii) statistical assumptions, iii) Recommendation for melanoma with lymph node involvement and complete
(Dec 2018) different patient characteristics in meta-analysis vs pembro study, iv) data use in CDF48 resection. Long-term RFS benefit uncertain as clinical trial
included older studies which do not represent progress made in treatment. was ongoing at the decision time
Based on the promising effects on RFS, pembro may improve overall
survival compared to surveillance but will have to be confirmed with OS data
The pERC considers RFS as an appropriate surrogate endpoint if Recommendation based on statistically significant and
RFS HRFailure of a curative intent is considered patient-relevant by G-BA;
NICE accepted inclusion of iDFS and RFS endpoints in the economic models
Countries Evaluation RFS - pembrolizumab in adjuvant melanoma
Company referenced the pertuzumab decision:
“In this patient group, a relapse is a patient-relevant event. The occurrence of a relapse means
that the attempt to cure using the curative therapeutic approach was unsuccessful [although it is
Indication of
unclear whether the therapy actually leads to a cure]. When considering an event time analysis of the
non-
G-BA relapse, it is possible that with similar proportions of events in the study arms, an advantage of the
quantifiable
therapy is derived solely from the different time periods until the occurrence of a relapse. However, it
added benefit46
remains unclear what significance - for the course of the disease - a shift in the time of diagnosis of a
relapse has.” Therefore, the proportion of patients with relapse and the associated failure of the
curative therapeutic approach is more important than RFS.46
NICE accepts the company’s economic model which uses data from the RFS and OS
Recommend-
NICE endpoints. However, NICE comments that distant RFS and OS data are incomplete and that this
ation for use in
results in the included estimates to be unreliable and implausible. NICE recommends collecting more
CDF48
data to resolve this uncertainty.48
© 2021 Blue Matter 28It was discussed earlier that regulators accepted pCR as a surrogate despite a lack
of trial-level association
Company Roche Trial results52
FDA / EMA • (NeoSphere trial) The benefit of adding pertuzumab to the
Sept 201350,51 / Mar 201552
approvals D+T combination was assessed using pCR (defined as
ypT0/isypN0 OR ypT0/is). Results showed a significant
Combination with trastuzumab & chemo for neoadjuvant increase in pCR when pertuzumab was added to the
Indication Tx of pts with HER2+, locally advanced, inflammatory, combination, irrespective of the definition used:
or early stage BC at high risk of recurrence.
• ypT0/isypN0: 17.8% increase (p=0.0063); ypT0/is: 16.8%
Study of increase (p=0.0141)
NEOSPHERE
interest
Surrogate validity data11 Statistical model11
• A meta-analysis of 12 trials including 11955 • HRs or EFS and OS (calculated with Cox proportional
patients investigated the correlation between hazards models) were compared with and the odds
different definitions of pCR (ypT0 ypN0, ypT0/is ratios of pCR (calculated with logistic regression
ypN0, and ypT0/is) and EFS/OS in various models).
subgroups • The coefficient of determination (R²) and the associated
• Tumor eradication from both breast and lymph 95% CI to measure the correlation between pathological
nodes (ypT0 ypN0 or ypT0/is ypN0) was better complete response and EFS and OS by treatment effect
associated with EFS and OS (HR 0,44 and HR were calculated using a two-stage model to adjust for
0.36) than tumor eradication from breast only (HR the estimation error of treatment effect size estimates
0.60, HR 0.51)
• Despite this, a trial-level analysis assessing
the suitability of pCR as a surrogate for EFS
or OFS found little association (R2 = 0.03 for
EFS, and R2= 0.24 for OS)
pCR: absence of invasive neoplastic cells at microscopic
examination of the primary tumor at surgery. Remaining in-situ ypT0/isypN0 = Absence of invasive cancer in the breast and axillary nodes;
lesions were allowed. Pathologists at participating centres followed DCIS allowed,
guidelines for the assessment of pCR on serial sections of the © 2021 Blue Matter ypT0/is = Absence of invasive cancer in the breast and DCIS allowed; 29
cervical specimen. Blinded pathology data were reviewed by a regardless of nodal involvement; D= Docetaxel; T = Trastuzumab
consultant pathologist at regular intervals to ensure consistency.However, payers considered validation to be insufficient, and gave mostly negative
evaluations; unlike DFS/RFS, pCR itself was also not considered patient-relevant
Countries Surrogate validity Evaluation Reasons
The surrogacy of pCR was deemed of unclear validity since the
validation studies only show a correlation between pCR and OS on a Due to unclear surrogacy for OS [pCR] could not be taken
patient-level basis, but did not demonstrate this on a trial-level. In into account for consideration of benefit. In addition, it is
Germany No proof of
addition, the validation studies did not take into account the difference unclear whether the magnitude of the benefit observed in
(Feb 2016) additional benefit53
in association among molecular subtypes (e.g., luminal B-like, pCR is relevant since there was no significant difference in
HER2+ like) which have been shown to benefit to differing degrees from OS or recurrence/relapse rate/DFS
pCR on a patient-level
There is insufficient evidence of clinical benefit given the
France statistical shortcomings: The Phase 2 study performed a
Not specifically discussed Not recommended54
(July 2016) three non-hierarchical analysis on the primary endpoint
which cannot be considered a confirmatory study
The committee concluded that there was evidence that
Given the validation study was unable to validate pCR as a surrogate,
pertuzumab could improve pCR rates when added to
UK the committee expressed concerns about the reliability of pCR as a Recommended for
trastuzumab and docetaxel, and that that pCR was more
(Dec 2016) surrogate for OS and it notes that the trial was not powered for long-term use in NHS55
likely than not to have an association with longer-term
outcomes
survival
No clear net clinical benefit compared to trastuzumab and
Canada pERC indicated that pCR has not been validated as a surrogate for docetaxel. These treatment options already key outcomes
Not recommended56
(July 2015) either event-free survival or overall survival valued by patients: prolongation of survival and prevention
of disease recurrence
Favorable Intermediate Unfavorable
© 2021 Blue Matter 30Polivy in r/r DLBCL launched with a small (n=40) study with CR as primary endpoint
and PFS, OS as secondary; it is also an orphan drug
Orphan Drug
POLIVY in combination with bendamustine and rituximab is indicated for the treatment of r/r DLBCL
1o endpoint CR57 2o endpoint PFS58 2o endpoint OS58
© 2021 Blue Matter 31Kymriah in r/r ALL launched with a single-arm study with CR as primary endpoint
and ORR, MRD, PFS and OS as secondary endpoints
Orphan Drug
r/r ALL
Primary 60%) had complete remission, and 16 (21%) had 2o
endpoint complete remission with incomplete endpoint
CR59 hematologic recovery RFS60
2o
2o
endpoint
endpoint
ORR /
OS60
MRD60
RFS was defined as time since onset of CR or CRi to relapse or death due to underlying cancer, whichever is earlier, censoring for new cancer therapy including SCT
© 2021 Blue Matter 32Germany has a high bar for acceptance of surrogates; CR, DoR, MRD, PFS, EFS are
often not accepted (see exceptions earlier)
Country Surrogate validity Evaluation Reasons
CR not a valid surrogate of a patient-relevant
endpoint. Partial remission not relevant since hint for non-
Polivy Statistically significant OS benefit in
disease persists. PFS, DoR, EFS not patient-
quantifiable favor of Polivy. However, imbalances in
r/rDLBCL relevant which the company agrees with, since it's
additional patient populations, small trial, and
(Aug 2020)61 based on imaging and cytology and not on
benefit comparator not widely used; orphan drug
symptoms, and the mortality component is already
included in OS
DoR, EFS (time from infusion to
non- occurrence of relapse or death) not
Kymriah patient-relevant, RFS (time from CR to
CR/CRi not a validated surrogate for patient- quantifiable
r/rALL relapse* or death) unclear patient-
relevant endpoint, MRD not a validated surrogate additional
(Dec 2019)62 relevance (because unclear at the time
benefit whether CAR-T is potentially curative)
so additionally considered; orphan drug
*relapse is defined as recurrence of >=1% blast cells in blood, >5% in bone marrow or recurrence or first occurrence of extramedullary disease
**Additional comments: The mortality component of PFS is valid but already covered in OS, and the other components are of unclear patient-relevance, and overall, there are different views within G-BA on PFS (extent of
additional benefit not influenced by this), Absence of symptoms is patient-relevant if patients perceive symptoms, and all other components of CR are of unclear patient-relevance. Favorable Intermediate Unfavorable
© 2021 Blue Matter 33UK – clinical opinion is considered but evidence thresholds are high; modelling
based on PFS and OS are often decision drivers
Country Surrogate validity Evaluation Reasons
Company submitted cure-mixture model, but NICE
ERG rejected the model citing lack of plateau in
PFS KM curve, only 2-years of data from a small Clinical trial evidence shows increased
Polivy patient sample, and “PFS may not be appropriate progression-free survival and overall
Recommended
r/rDLBCL for estimating long-term remission”; although clinical survival. The cost-effectiveness
experts stated that at least in 1L, 24M CR is for use in NHS
(Sep 2020)63 estimates are within range of acceptable
associated with prolonged OS and there is some for NHS resources
evidence in r/r, NICE concluded that there is
insufficient evidence to justify a cured proportion
CR/CRi not a validated surrogate for patient-
relevant endpoint, MRD not a validated surrogate May extend survival or time to relapse,
Kymriah
but uncertain. No robust data that
r/rALL Cost-effectiveness was mainly based on CDF
Kymriah has curative effect though it has
(Dec 2018)64 modelling/extrapolation of overall survival, which is a curative intent
a secondary endpoint in a single-arm study
Additional note: PFS is technically a surrogate endpoint, but unlike the G-BA, NICE does accept modeling based on PFS; PFS and OS data
gathered as secondary endpoints are also accepted, supporting use of other surrogates (e.g., CR / MRD) as primary endpoint for clinical trials
Favorable Intermediate Unfavorable
© 2021 Blue Matter 34France – out of the three countries, France is the most clinically focused; surrogates
are often considered in the overall decision
Country Surrogate validity Evaluation Reasons
Weak methodology (exploratory trial
without non-inferiority or superiority
Polivy CR was discussed as a clinical data point, but hypothesis), infrequently used
Insufficient comparator, uncertainties with CR
r/rDLBCL considered unconvincing given the imbalances results due to unequal patient groups, no
SMR
(July 2020)65 observed between treatment arms robust OS gain data, no QoL data,
uncertainties around lyophilized
formulation
Available data show a high percentage
CR data important in positive evaluation (~40%
of CR in a population with unfavorable
Kymriah maintained in approximately 40% of patients after a
prognosis (but no comparator arm so
r/rALL median follow-up of 9 months); however, HAS ASMR III
uncertainty and short follow-up) and
(Feb 2019)66 considered that maintenance of clinical efficacy in
significant short-term toxicity which
the longer term remains uncertain
influenced the ASMR rating
Favorable Intermediate Unfavorable
© 2021 Blue Matter 35Gazyva in 1L CLL had a large RCT with primary PFS, secondary endpoints included
CR and MRD
Orphan Drug
1L CLL
2o
endpoint
CR68
Primary
endpoint
PFS67
2o
endpoint
MRD68
© 2021 Blue Matter 36G-BA rejected MRD validation, NICE focused on PFS/OS data but HAS considered
MRD data as part of its positive ASMR rating
Country Surrogate validity Evaluation Reasons
Validation of MRD-negativity at the end of treatment in
Böttcher et al. from the CLL8 study is not appropriate
Germany since neither the patient populations nor the treatments non-quantifiable OS immature and not significant but
(May are comparable to the here presented CLL11 study additional indicative, so no quantification of additional
2015)69 (additional reasons: bias due to open-label, MRD was benefit benefit possible; orphan drug
not a prespecified endpoint, not sufficiently powered to
determine the treatment effect on OS)*
PFS shows it is a clinically effective
treatment compared with Clb or R-Clb (but the
UK
meta-analysis to indirectly compare to
(June MRD not specifically assessed as surrogate CDF
bendamustine was not reliable). Significant OS
2015)70
benefit of G-Clb over Clb, but data vs R-Clb
incomplete
Efficacy has been shown in terms of PFS and
rate of residual disease, but increased AEs.
France
MRD data important in positive evaluation; no specific OS shows benefit but immature and not
(July ASMR III
surrogate validation discussed significant (8% vs 12% deaths, p=0.0849,
2016)71
mOS not reached in either group, later cutoff
gives p=0.0632)
*Additional comments: The mortality component of PFS is valid but already covered in OS, and the other components are of unclear patient-relevance, and overall, there are different views within G-BA on PFS (extent of additional
benefit not influenced by this), Absence of symptoms is patient-relevant if patients perceive symptoms, and all other components of CR are of unclear patient-relevance.
© 2021 Blue Matter Favorable Intermediate Unfavorable 37CLL8 examined MRD in patients treated with FC or FCR; G-BA did not accept this as
appropriate validation given different treatments (and population)
Randomized GCLLSG CLL8 Trial72
Patients and Methods MRD in 1,775 blood and bone
marrow samples from 493 patients randomly assigned to
receive fludarabine and cyclophosphamide (FC) or FC
plus rituximab (FCR)
Patients were categorized by MRD into low- (< 10−4),
intermediate- (≥ 10−4 toAs another example in heme, G-BA considered transplant “potentially curative” in
AML, and therefore, relapse/EFS as patient-relevant
FLT3+ 1L AML73
G-BA evaluation of relapse
and DFS as surrogate endpoints74
Although the G-BA had other major concerns with midostaurin study design and
data, it considered transplant as potentially curative, and therefore, prevention of
relapse and EFS as patient-relevant
“Due to the potentially curative therapeutic requirements of the therapy
regimen carried out in the RATIFY study for the treatment of the previously
untreated acute myeloid leukemia, relapses and disease-free survival are
patient-relevant as the endpoint for the failure of the primary therapeutic approach
and thus the potential cure of the disease”
NOTE: RATIFY had OS as primary endpoint; therefore, we will not further discuss
evaluation in other countries
© 2021 Blue Matter
39Challenges and Opportunities
© 2021 Blue MatterIn summary, validating surrogates can be a challenging process, with limited
consistent guidance but high data and modeling requirements
Challenges
• Official guidances are often insufficiently specific
Requirements
• Regulatory and payer requirements differ, with payers having higher evidence thresholds
differ across
• Requirements across payers differ, ranging from formal statistical assessments (e.g.,
stakeholders
G-BA/IQWiG) to clinical interpretation (e.g., HAS); NICE / CADTH falls somewhere in the middle
• While payers have accepted less than perfect analyses (e.g., lack of trial-level association) in certain
Requirements indications (e.g., HCV, HIV), they scrutinize other disease areas in more detail
differ across • Long-history/precedence of prior reimbursement decisions likely played a role in virology, as did the
disease areas clear and dramatic effect on individual patient outcomes (e.g., HCC, death). Whereas in other
disease areas (e.g., oncology), there are higher requirements for trial-level association.
• Payers have high requirements for meta-analyses in terms of relevant patient populations, SoC
Large amounts interventions, consistent treatment paradigm and correct statistical assumptions. This creates
of tailored and challenges for any product, but especially those that are first-in-class or in a fast changing, competitive
consistent data landscape
required • Contradictory evidence (e.g., one or two examples of substance-specific effect for LDL-c) could lead
to conclusion of no proof of surrogacy by some payers
© 2021 Blue Matter 41Pharma should focus on robust long-term data generation in high unmet need
patients, and providing supportive patient-relevant outcomes
Opportunities
• Plan well in advance for long-term data collection, even as secondary endpoints not required for
regulatory approval
• Include some studies that are powered for true endpoint if at all possible
Plan clinical • Focus on high unmet need subpopulations where a clear effect size can be shown
development (e.g., Keytruda in N+ melanoma vs. Perjeta in N+ and N- breast); many payers will consider the clinical
program to context and apply medical judgment in their final decisions
address payer – Downside is that data for meta-analysis in specific subpopulations may be difficult to obtain
requirements • Provide patient-relevant outcomes even if they are not the most preferred endpoints for payers (e.g.,
reduction of AEs for Sovaldi, reduction of LDL apheresis for Praluent)
– Even in oncology, DFS/RFS are considered patient-relevant by the G-BA and other payers,
whereas endpoints such as pCR only have surrogate validation to rely on
Broaden scope of • Collaborate with academia/other pharma to generate data in relevant patients
evidence • Consider effective use of RWE where relevant (e.g., acceptance of observational studies for HCV,
generation potentially greater use of RWE as part of conditional reimbursement going forward)
Collaborate and • Collaborate with academia when possible to conduct the meta-analyses (e.g., NICE preference for
obtain feedback CTTC rather than company submitted analysis)
on statistical • Obtain feedback early on modelling requirements, but multiple models/analyses may need to be
validation developed to provide payers with greater certainty
© 2021 Blue Matter 42Different countries have different requirements; country-specific strategies should be
developed, including demonstrating patient-relevance for Germany
Likelihood of accepting the surrogate Patient-relevance as an alternative
endpoint in the benefit assessment route to market access in Germany
Considers best clinical • If a non-validated surrogate endpoint is considered to be
understanding; may accept surrogate patient relevant, it can be included in the benefit
endpoint in the absence of validation assessment (though in oncology usually under morbidity)
studies
• To be considered patient relevant, a surrogate endpoint
needs to report on patient-perceived outcomes such
as patient-reported symptoms or QoL
Acceptance of some degrees of
uncertainty in cost-effectiveness • Alternatively, a surrogate endpoint based on imaging/lab
modeling parameters may be considered patient relevant if it shows
the failure of a treatment with curative intent
- Example: Disease recurrence (e.g., DFS, RFS) in a
curative context of early tumor settings (e.g., adjuvant
Insistent on bona fide surrogate BC40, 1L AML74)
validation unless decades of data
support transformative patient-level
association (e.g., HCV, HIV)
43
© 2021 Blue MatterThomas Quirk Yan Xue
Partner Principal
tquirk@bluematterconsulting.com yxue@bluematterconsulting.com
© 2021 Blue MatterReferences
1. Schuster Bruce, C., Brhlikova, P., Heath, J., & McGettigan, P. (2019). The use of validated and nonvalidated surrogate endpoints in two European
Medicines Agency expedited approval pathways: A cross-sectional study of products authorised 2011-2018. PLoS medicine, 16(9), e1002873.
https://doi.org/10.1371/journal.pmed.1002873
2. Downing, N., Aminawung, J., Shah, N., Krumholz, H., & Ross, J. (2014). Clinical Trial Evidence Supporting FDA Approval of Novel Therapeutic Agents,
2005-2012. JAMA, 311(4), 368. https://doi.org/10.1001/jama.2013.282034
3. U.S. Food and Drug Administration. (2018). Surrogate Endpoint Resources for Drug and Biologic Development. https://www.fda.gov/drugs/development-
resources/surrogate-endpoint-resources-drug-and-biologic-development
4. U.S. Food and Drug Administration. (2020). Table of Surrogate Endpoints That Were the Basis of Drug Approval or Licensure.
https://www.fda.gov/drugs/development-resources/table-surrogate-endpoints-were-basis-drug-approval-or-licensure
5. Buyse, M., Molenberghs, G., Burzykowski, T., Renard, D., & Geys, H. (2000). The validation of surrogate endpoints in meta-analyses of randomized
experiments. Biostatistics, 1(1), 49–67. https://doi.org/10.1093/biostatistics/1.1.49
6. Taylor, R., & Elston, J. (2009). The use of surrogate outcomes in model-based cost-effectiveness analyses: a survey of UK Health Technology Assessment
reports. Health Technology Assessment, 13(8). https://doi.org/10.3310/hta13080
7. Burzykowski, T., Molenberghs, G., & Buyse, M. (2005). The Evaluation of Surrogate Endpoints. Springer.
8. European Medicines Agency. (1998). ICH: E 9: Statistical principles for clinical trials - Step 5: Note for guidance on statistical principles for clinical trials
(CPMP/ICH/363/96). https://www.ema.europa.eu/en/documents/scientific-guideline/ich-e-9-statistical-principles-clinical-trials-step-5_en.pdf
9. Burzykowski, T., & Buyse, M. (2006). Surrogate threshold effect: an alternative measure for meta-analytic surrogate endpoint validation. Pharmaceutical
statistics, 5(3), 173–186. https://doi.org/10.1002/pst.207
10. Institute for Quality and Efficiency in Health Care. (2011). Validity of surrogate endpoints in oncology (Executive summary of the rapid report A10-05).
https://www.iqwig.de/download/a10-05_executive_summary_v1-1_surrogate_endpoints_in_oncology.pdf
© 2021 Blue Matter 45You can also read