COVID-19 vaccination programme: Workforce and training toolkit - Version 7, 21 April 2021
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

OFFICIAL COVID-19 vaccination programme: Workforce and training toolkit Version 7, 21 April 2021

Contents
Section Slide(s)
Workforce & training context 4
This workforce and training toolkit is for Regional Leads and
Regional Workforce Leads to use as a practical guide and:
National supply 5-7
Workforce staffing models 8-11 • provides information on the workforce and training approach
to support the local mobilisation of workforce and training
Unregistered Vaccinators 12-20 activities
Clinical Assessment 21-26 • provides information that can be shared with appropriate
stakeholders and delivery organisations
Legislation 27-30 • explains how delivery organisations can access the national
workforce supply
Regional mobilisation 31-44
Training requirements 45 Please note the information in this pack will be updated, in
particular the training requirements and pathways for each
Workforce Planning Tool 46-50 role.
Volunteer guidance 51-53 Changes are highlighted in yellow.
Appendices:
1. Operational guidance for workforce 54-70
deployment
2. Memorandum of Understanding 70-71
2 |
About this pack
This pack supports to prepare for the workforce and training mobilisation of the COVID-19 vaccination programme. It includes:
• National supply: The mechanisms to draw down from the nationally procured contracts with Lead Employers as this is how
local trusts will access new supply routes.
• Workforce delivery models: Staffing models to support local recruitment and guidance on the employment credentials that
need to be in place for each of the staff groups.
• Unregistered Vaccinator: Guidance on the utilisation of unregistered vaccinators including clear guidelines and case
studies
• Clinical Assessment: Provision of guidance on alternative delivery modes to streamline the clinical assessment
component of the vaccination pathway, by utilising pre-screening of patients; designed for both vaccination centres and
PCNs under the National Protocol
• Mobilisation: The frameworks for Lead Employers, an outline of the interface with local providers and regional workforce
bureaus, to support workforce optimisation. There is also an outline of how rostering works to support the deployment of the
nationally recruited workforce.
• Training: Details of the training journeys for both registered and non-registered staff, including training requirements and
modes of delivery.
• Workforce Planning Tool: The Foundry Workforce Planning tool allows you to enter, view and manage workforce planning
data
• Volunteer Guidance: guidance on the safe deployment of NHSVR steward volunteers and other volunteer stewards
3 |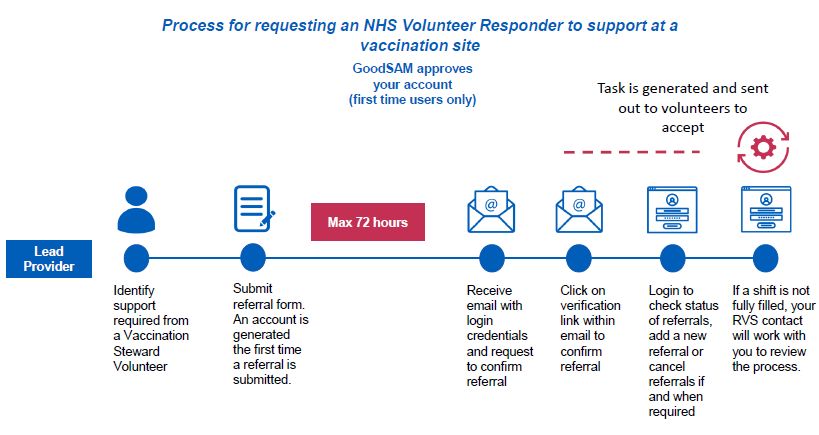
Workforce and training: context • Planning needs to focus on identifying workforce capacity beyond the core vaccinators working in the NHS (by expanding who is able to administer a vaccine through the changes to medicines legislation). Planning will also need to take into consideration business as usual planning within the NHS including elective recovery. • The role of the vaccinator and registered healthcare professional have been developed to be generic roles, filled by people with the relevant skills, so we are less reliant on one staff group. • The model job descriptions have been graded through Agenda for Change for the tasks and competencies required. These can be used to support local recruitment efforts. • Some staff will be newly recruited to the NHS (new vaccinators) while others will be freed up by NHS organisations, where possible. • All staff, regardless of how they are secured, will need to undergo national training and a competency assessment before they can vaccinate patients (except for volunteers from St John Ambulance who will have already been trained). Supervision must be provided. • The recommended staffing pod models can be flexed depending on local requirements. The skill mix must be assured at a local level through safe staffing and clinical supervision arrangements and variations entered into the Workforce Planning Tool to ensure any local variations are reflected in local demand data. • The lead employer model has been established to support NHS Providers and Primary Care (PCN’s and Community Pharmacies). This will also include the services to which primary care supports. • Deployment will prioritise the use of existing staff and local temporary recruitment. Where there is insufficient capacity identified locally, providers can access additional capacity via National Workforce Suppliers (see next two pages). 4 |
National workforce suppliers
Overview of support Roles provided by
Supplier How do I access national supply?
provided supplier
SJA will manage and deploy • Vaccinator Volunteer Lead providers can contact SJA to discuss mobilisation and plans of action by emailing NHS-Vaccinations@sja.org.uk
30,500 volunteers to vaccination • Vaccination Support
centres, including 10,000 Volunteer (post To access the Volunteer Workforce please follow these steps:
observation care)
vaccinators. This will be available 1. Workforce Bureau and/or Lead Provider provides the workforce requirement to the Single Point of Contact via the prescribed online
• Patient Advocate
across all seven regions. form
2. SJA Single Point of Contact uploads the required shifts onto the SJA Global Rostering Service (GRS)
St John 3. SJA Volunteers will then self-roster the shifts in accordance with the Lead Provider requirements.
Ambulance 4. When Volunteer arrives on-site the Lead Provider will be required to conduct the onsite inductions and ensure any face-to-face training
has been completed for Vaccinator Volunteer role. There is no national requirement for volunteers to sign a volunteer agreement but
(SJA)
where local requirements dictate the Lead Provider may request that the volunteer signs a Volunteer Agreement on Lead Employer
headed paper in accordance with its local procedures to ensure areas such as confidentiality and data protection are covered
accordingly. The National Team has provided a template should the Lead Employer wish to use this – see slide 7.
5. Volunteer will conduct their shift under the supervision of the Lead Provider.
6. SJA will invoice NHS England and NHS Improvement directly every month for the services delivered in that monthly period. All
invoices will be broken down regionally.
Royal RVS can provide c.50,000 • Steward Volunteer The Lead Employer will be able to access the RVS nation supply chain via the GoodSAM app. To access the Volunteer Workforce please
Voluntary volunteers aligned to the current follow these steps:
NHS Volunteer Responder 1. Workforce Bureau staff and/or Lead Employer staff will be trained via an online webinar on how to upload requests onto the
Services
model. GoodSAM application.
2. Workforce Bureau and/or Lead Provider uploads demand to the GoodSAM application
3. Volunteer will respond to GoodSAM application and sign up to shifts within their geographical areas.
4. When Volunteer arrives on-site the Lead Employer will be required to conduct the onsite inductions. Where required, the Lead
Employer may request that the Volunteer signs a Volunteer Agreement in accordance with its local procedures to ensure areas such
as confidentiality and data protection are covered accordingly. The National Team has provided a template should the Lead
Employer wish to use that.
5. Should there be any issues or queries in relation to the Volunteers, RVS will provide a Regional Relationship Manager who will be
your first escalation point.
6. RVS Volunteer will be inducted and deployed as per the Lead Provider Requirements.
7. RVS will invoice NHS England and NHS Improvement directly every month.
For additional information and PCN and community pharmacy guidance, refer to slide 51-53.
5 |National workforce suppliers
Overview of support to be
Supplier Roles to be provided by supplier How do I access national supply?
provided
Multiple Occupational Health Providers • Registered OH Nurse - Onsite / face-to-face The Occupational Health DPS Framework with 23 suppliers is accessible from the NHS England
can provide additional Registered • OHA (qualified OH nurse; part 3 of register) and NHS Improvement People Directorate. To access the Framework please follow these steps:
Occupational Health Professionals. Onsite / face-to-face 1. Provider/trust to identify specific requirements eg 2 OH nurses to work at X location for 2
months.
2. Provider/trust to identify the required local funding
3. Region accesses full list of accredited suppliers on NHS Health at Work Network
https://www.nhshealthatwork.co.uk/login.asp?origin=covid.asp
Occupational health 4. Once a supplier is identified through the Framework, Lead Employers can contact the
providers supplier directly and enter an agreement with them.
5. OHP employee will be inducted, trained and deployed as per the System Lead Provider
requirements.
6. The Provider/ Trust will be invoiced directly.
The Bring Back Scheme mechanism is • Vaccinator - Pay Band 3 Existing BBS routes should be undertaken by the NHS organisation.
where the System Lead Provider identifies • RHCP - Draw-up & Clinical Assessment* -
a BBS colleague. Pay Band 5 Where routes do not exist, NHS Professionals may be used as a route to contract.
Bringing Back Staff • Registered Healthcare Professional - Pay
Band 6
NHSP has launched a targeted “call for Covid-19 Vaccination Programme Vaccinator- Pay Practices and PCNs will be able to make requests for additional staff via their Lead Provider, but
action” to recruit to specific roles as Band 3 will be required to fund these posts locally, in line with Agenda for Change pay rates and put in
additional workforce. NHSP will be place a collaborative agreement with the Lead Employer.
responsible for the end-to-end process, Specific roles have been developed to be generic
from managing centralised demand, to (not specific to a professional clinical group). To access resource, PCN groupings should follow the drawdown processes for the National
recruitment and virtual training and Workforce Supply Routes.
NHS
confirming employment hosting
Professionals (NHSP) arrangements.
More details are available at: NHS
Professionals - Join the Covid-19 Vaccine
6 | TeamUseful National Workforce Supplier documents
Supplier Title of Document Contents Document Link
Provision of resources to the Covid-19 Provides overview of NHSP resource draw-down https://future.nhs.uk/CovidVaccinations/vie
NHSP Vaccination Programme w?objectId=94215717
Defines the three rostering and deployment models:
1.Lead employer is an NHSP customer
2.Lead employer is not an NHSP customer, and uses Allocate
3.Lead employer is not an NHSP customer, and uses another roster/ bank technology
Outline of roles and responsibilities
St John Information Document • Provides overview of SJA resource draw-down https://future.nhs.uk/CovidVaccinations/vie
Ambulance • Roles & training w?objectId=94215909
• Governance arrangements
• Clinical assurance
• Contact information
St John Information Document • Additional information for requesting SJA volunteer support https://future.nhs.uk/CovidVaccinations/vie
Ambulance w?objectId=96502149
St John Template Volunteer Agreements If required Lead Employers can use the attached template. Please note if you decide to https://future.nhs.uk/CovidVaccinations/vie
Ambulance use your existing Volunteer Agreements for Volunteers, please ensure the provision on w?objectId=94215813
insurance is aligned and/ or incorporated as per the Template. The Template includes:
• The volunteer role
• Induction and training
• Insurance
• Confidentiality
Royal Voluntary Template Volunteer Agreements If required Lead Employers can use the attached template. Please note if you decide to https://future.nhs.uk/CovidVaccinations/vie
Service use your existing Volunteer Agreements for Volunteers, please ensure the provision on wdocument?docid=98691557
insurance is aligned and/ or incorporated as per the Template. The Template includes:
• The volunteer role
• Induction and training
• Insurance
7 | • ConfidentialityWorkforce summary for Pfizer under National Protocol (1)
OFFICIAL
• The tables in this section outline the workforce requirements at each vaccination stage to support the safe and effective delivery of vaccinations across a single vs. a multiple pod site for
Pfizer (Model 1 as per the standard workforce pod model guidance). Updated pod model documents for VCs and HHs can be found on NHS Futures.
• It shows the crude numbers needed at any given time for the models to operate. It does not account for FTE sick leave, breaks, 2 shifts per day.
• The site size dictates the required governance structure, which can vary between a one pod site vs multiple pod site as scaling involves increased management, governance and
accountability. This is a recommended workforce structure and is subject to local flexibility and adjustment.
Total no of workforce required
Stage Role Description Narrative and comments
One pod site Multiple pod site
• Responsible for patient check-in and pod allocation.
Site registration Front of House (Band 2) 2 2 per pod
• Responsible for patient queries on the day.
Registered healthcare
Clinical assessment • Responsible for the patient clinical assessment pre-
professional as per National 5 5 per pod
and consent vaccination.
Protocol (Band 5)
Experienced registered
• Responsible for diluting and drawing up the vaccine
Vaccine preparation healthcare professional (Band 1 1 per pod
(experienced, trained and competent staff)
5) or vaccinator
• Responsible for the delivery of vaccination.
Vaccine Vaccinator (registered or
• Responsible for the disposal of clinical waste and 2 2 per pod
administration unregistered) For scaling purposes, the numbers show the
change of PPE (when required).
roles needed relative to the pod ratio, but do
• Responsible for patient record keeping. not imply the location of the roles inside the
Vaccine data pod.
Admin Support (Band 3) • Responsible for recording vaccination data (such as 2 2 per pod
recording
batches, numbers).
• Responsible for sanitisation and infection control (eg
Heath Care Assistant (HCA)
Waste management wipe down surfaces). 1 1 per pod
(Band 3)
• Support the vaccination process.
Site Stewarding Marshal • Responsible for patient flow management. 5 5 per pod
• Responsible for answering patient queries and
Patient guidance SJA Patient Advocate 1 1 per pod
addressing any concerns.
Post vaccination • Responsible for managing the post vaccination
SJA Volunteer 2 2 per pod
observation observation area and providing BLS.Workforce summary for Pfizer under National Protocol (2)
OFFICIAL
Total no of workforce required
Stage Role Description Narrative and comments
One pod site Multiple pod site
Registered healthcare • Supervision of the vaccination activity and staff within
1 1 per pod –
professional (Band 6) the pod and observation area.
Within the one pod site, the clinical assessors can
escalate to the senior manager. Scaling up, we
Registered healthcare
• Escalation point for clinical assessment. 0 1 per max 3 pods anticipate the need for a Band 6 as direct
professional (Band 6)
escalation point, one responsible for up to three
Clinical pods.
Supervision & Within the one pod site, a senior manager is able
• Responsible for clinical escalations.
Escalation Nursing Manager to oversee both clinical and operational activity.
• Responsible for overseeing the clinical activity for the 0 1 per max 3 pods
(Band 8a) Scaling up to multiple pods, this role requires
pod and clinical assessment area.
separation of responsibility; therefore, we propose
that instead of a senior manager, a
nursing manager is responsible for the clinical
Senior Manager (Band • Responsible for clinical and operational oversight, oversight of a maximum of 3 pods and there is on-
1 0
8c-d) governance of the site and staff supervision. site presence of an ops director (see below)
responsible for operational oversight.
• Responsible for clinical leadership and governance of 1 per site to cover
At least 1 per Lead We anticipate that a medical director can oversee
the site(s). remote oversight
Medical Director Trust covering multiple sites remotely. This role may be covered
• Responsible for clinical escalations above the nursing of difficult clinical
multiple sites (remote) by the GP in the PCN model.
Overall site manager or senior manager. queries
management • Responsible for non-clinical leadership and operational At least 1 per lead We anticipate that the Ops Director can oversee
delivery of mass vaccination site(s). trust covering multiple one pod sites remotely. For multiple pod
Operations Director 1 per site (on site)
• Responsible for ensuring all workforce, consumables multiple sites sites, this role may be required in-person, dedicated
and equipment are in place. (remote) to that site.
Pharmacy input and oversight must be considered in the mass vaccination sites to maintain product integrity of the Vaccine, ensuring that appropriate cold chain processes are in place
and that the staff carrying out tasks are adequately training to handle the vaccine(s). There will be a mix of new HC Professionals and new recruits hence good pharmaceutical oversight
Pharmacy Team is essential to ensure patient safety. Specifically, management of all aspects of ordering, receipt, storage and onward supply from stock of vaccine and medicines should be provided by
a senior member of the local Pharmacy Team.
SOPs have been developed to support this process and are available on Specialist Pharmacy Services websites.Workforce summary for AstraZeneca under National Protocol (1)
OFFICIAL
• The tables in this section outline the workforce requirements at each vaccination stage to support the safe and effective delivery of vaccinations across a single vs. a multiple pod site for
AstraZeneca (Model 2 as per the standard workforce pod model guidance). Updated pod model documents for VCs and HHs can be found on NHS Futures.
• It shows the crude numbers needed at any given time for the models to operate. It does not account for FTE sick leave, breaks, 2 shifts per day.
• The site size dictates the required governance structure, which can vary between a one pod site vs multiple pod site as scaling involves increased management, governance and
accountability. This is a recommended workforce structure and is subject to local flexibility and adjustment.
Total no of workforce required
Stage Role Description Narrative and comments
One pod site Multiple pod site
• Responsible for patient check-in and pod allocation.
Site registration Front of House (Band 2) 2 2 per pod
• Responsible for patient queries on the day.
Registered healthcare
Clinical assessment • Responsible for the patient clinical assessment pre-
professional as per National 5 5 per pod
and consent vaccination.
Protocol (Band 5)
Registered healthcare
• Responsible for drawing up the vaccine (RHCP or
Vaccine preparation professional (Band 5) or 1 1 per pod
competent non registered staff)
vaccinator
• Responsible for the delivery of vaccination.
Vaccine Vaccinator (registered or
• Responsible for the disposal of clinical waste and 2 2 per pod
administration unregistered) For scaling purposes, the numbers show the
change of PPE (when required).
roles needed relative to the pod ratio, but do
• Responsible for patient record keeping. not imply the location of the roles inside the
Vaccine data pod.
Admin Support (Band 3) • Responsible for recording vaccination data (such as 2 2 per pod
recording
batches, numbers).
• Responsible for sanitisation and infection control (eg
Heath Care Assistant (HCA)
Waste management wipe down surfaces). 1 1 per pod
(Band 3)
• Support the vaccination process.
Site Stewarding Marshal • Responsible for patient flow management. 5 5 per pod
• Responsible for answering patient queries and
Patient guidance SJA Patient Advocate 1 1 per pod
addressing any concerns.
Post vaccination • Responsible for managing the post vaccination
SJA Volunteer 1 1 per pod*
observation observation area and providing BLS.Workforce summary for AstraZeneca under National Protocol (2)
OFFICIAL
Total no of workforce required
Stage Role Description Narrative and comments
One pod site Multiple pod site
Registered healthcare • Supervision of the vaccination activity and staff within
1 1 per pod –
professional (Band 6) the pod and observation area.
Within the one pod site, the clinical assessors can
escalate to the senior manager. Scaling up, we
Registered healthcare
• Escalation point for clinical assessment. 0 1 per max 3 pods anticipate the need for a Band 6 as direct
professional (Band 6)
escalation point, one responsible for up to three
Clinical pods.
Supervision & Within the one pod site, a senior manager is able
• Responsible for clinical escalations.
Escalation Nursing Manager to oversee both clinical and operational activity.
• Responsible for overseeing the clinical activity for the 0 1 per max 3 pods
(Band 8a) Scaling up to multiple pods, this role requires
pod and clinical assessment area.
separation of responsibility; therefore, we propose
that instead of a senior manager, a
nursing manager is responsible for the clinical
Senior Manager (Band • Responsible for clinical and operational oversight, oversight of a maximum of 3 pods and there is on-
1 0
8c-d) governance of the site and staff supervision. site presence of an ops director (see below)
responsible for operational oversight.
• Responsible for clinical leadership and governance of 1 per site to cover
At least 1 per Lead We anticipate that a medical director can oversee
the site(s). remote oversight
Medical Director Trust covering multiple sites remotely. This role may be covered
• Responsible for clinical escalations above the nursing of difficult clinical
multiple sites (remote) by the GP in the PCN model.
Overall site manager or senior manager. queries
management • Responsible for non-clinical leadership and operational At least 1 per lead We anticipate that the Ops Director can oversee
delivery of mass vaccination site(s). trust covering multiple one pod sites remotely. For multiple pod
Operations Director 1 per site (on site)
• Responsible for ensuring all workforce, consumables multiple sites sites, this role may be required in-person, dedicated
and equipment are in place. (remote) to that site.
Pharmacy input and oversight must be considered in the mass vaccination sites to maintain product integrity of the Vaccine, ensuring that appropriate cold chain processes are in place
and that the staff carrying out tasks are adequately training to handle the vaccine(s). There will be a mix of new HC Professionals and new recruits hence good pharmaceutical oversight
Pharmacy Team is essential to ensure patient safety. Specifically, management of all aspects of ordering, receipt, storage and onward supply from stock of vaccine and medicines should be provided by
a senior member of the local Pharmacy Team.
SOPs have been developed to support this process and are available on Specialist Pharmacy Services websites.Workforce summary for Moderna under National Protocol
OFFICIAL (1)
• The tables in this section outline the workforce requirements at each vaccination stage to support the safe and effective delivery of vaccinations across a single vs. a multiple pod site for
Moderna (Model 3 as per the standard workforce pod model guidance). Updated pod model documents for VCs and HHs can be found on NHS Futures.
• It shows the crude numbers needed at any given time for the models to operate. It does not account for FTE sick leave, breaks, 2 shifts per day.
• The site size dictates the required governance structure, which can vary between a one pod site vs multiple pod site as scaling involves increased management, governance and
accountability. This is a recommended workforce structure and is subject to local flexibility and adjustment.
Total no of workforce required
Stage Role Description Narrative and comments
One pod site Multiple pod site
• Responsible for patient check-in and pod allocation.
Site registration Front of House (Band 2) 2 2 per pod
• Responsible for patient queries on the day.
Registered healthcare
Clinical assessment • Responsible for the patient clinical assessment pre-
professional as per National 5 5 per pod
and consent vaccination.
Protocol (Band 5)
Experienced registered
• Responsible for drawing up the vaccine (experienced,
Vaccine preparation healthcare professional (Band 1 1 per pod
trained and competent staff)
5) or vaccinator
• Responsible for the delivery of vaccination.
Vaccine Vaccinator (registered or
• Responsible for the disposal of clinical waste and 2 2 per pod
administration unregistered) For scaling purposes, the numbers show the
change of PPE (when required).
roles needed relative to the pod ratio, but do
• Responsible for patient record keeping. not imply the location of the roles inside the
Vaccine data pod.
Admin Support (Band 3) • Responsible for recording vaccination data (such as 2 2 per pod
recording
batches, numbers).
• Responsible for sanitisation and infection control (eg
Heath Care Assistant (HCA)
Waste management wipe down surfaces). 1 1 per pod
(Band 3)
• Support the vaccination process.
Site Stewarding Marshal • Responsible for patient flow management. 5 5 per pod
• Responsible for answering patient queries and
Patient guidance SJA Patient Advocate 1 1 per pod
addressing any concerns.
Post vaccination • Responsible for managing the post vaccination
SJA Volunteer 2 2 per pod
observation observation area and providing BLS.Workforce summary for Moderna under National Protocol
OFFICIAL (2)
Total no of workforce required
Stage Role Description Narrative and comments
One pod site Multiple pod site
Registered healthcare • Supervision of the vaccination activity and staff within
1 1 per pod –
professional (Band 6) the pod and observation area.
Within the one pod site, the clinical assessors can
escalate to the senior manager. Scaling up, we
Registered healthcare
• Escalation point for clinical assessment. 0 1 per max 3 pods anticipate the need for a Band 6 as direct
professional (Band 6)
escalation point, one responsible for up to three
Clinical pods.
Supervision & Within the one pod site, a senior manager is able
• Responsible for clinical escalations.
Escalation Nursing Manager to oversee both clinical and operational activity.
• Responsible for overseeing the clinical activity for the 0 1 per max 3 pods
(Band 8a) Scaling up to multiple pods, this role requires
pod and clinical assessment area.
separation of responsibility; therefore, we propose
that instead of a senior manager, a
nursing manager is responsible for the clinical
Senior Manager (Band • Responsible for clinical and operational oversight, oversight of a maximum of 3 pods and there is on-
1 0
8c-d) governance of the site and staff supervision. site presence of an ops director (see below)
responsible for operational oversight.
• Responsible for clinical leadership and governance of 1 per site to cover
At least 1 per Lead We anticipate that a medical director can oversee
the site(s). remote oversight
Medical Director Trust covering multiple sites remotely. This role may be covered
• Responsible for clinical escalations above the nursing of difficult clinical
multiple sites (remote) by the GP in the PCN model.
Overall site manager or senior manager. queries
management • Responsible for non-clinical leadership and operational At least 1 per lead We anticipate that the Ops Director can oversee
delivery of mass vaccination site(s). trust covering multiple one pod sites remotely. For multiple pod
Operations Director 1 per site (on site)
• Responsible for ensuring all workforce, consumables multiple sites sites, this role may be required in-person, dedicated
and equipment are in place. (remote) to that site.
Pharmacy input and oversight must be considered in the mass vaccination sites to maintain product integrity of the Vaccine, ensuring that appropriate cold chain processes are in place
and that the staff carrying out tasks are adequately training to handle the vaccine(s). There will be a mix of new HC Professionals and new recruits hence good pharmaceutical oversight
Pharmacy Team is essential to ensure patient safety. Specifically, management of all aspects of ordering, receipt, storage and onward supply from stock of vaccine and medicines should be provided by
a senior member of the local Pharmacy Team.
SOPs have been developed to support this process and are available on Specialist Pharmacy Services websites.Workforce deployment: workforce by delivery model and supplier pools –
required under National Protocol
Delivery Model Role Pay Band Supplier pool • The expected workforce requirements by role and band are set out in
Vaccination Centre Delivery Vaccinator 3 NHSP, SJA the tables alongside the likely draw-down process from existing
Model staffing pools.
RHCP 5 Staff Sharing, Secondment, NHSP
• A single location, capable Registered HCP – Supervisor 6 Staff Sharing, Secondment, NHSP
of supporting safe provision
HCA 3 Staff Sharing, Secondment, NHSP • Acronyms: SJA (St. John Ambulance), NHSP (NHS Professionals),
of vaccinations over an
extended period to large Vaccination Admin Support 3 Staff Sharing, Secondment, NHSP NHSV (NHS Volunteers), BBS (Bringing Back Scheme), RHCP
numbers of people in a (Registered Healthcare Professional).
Post-vaccination Observation & BLS SJA SJA
predominantly indoor
setting Steward – Volunteer non-clinical support NHSV NHSV
• This table shows the Patient Advocate – Patient Interaction SJA SJA, NHSP
workforce required which Front of House / Reception 2 Existing workforce bank, NHSP
can be scaled up and down
based on local Nursing Manager 8a Staff Sharing & Secondment
requirements Medical Director Med Gr Staff Sharing & Secondment
Operations Director Gr/ESM Staff Sharing & Secondment
Senior Manager 8b-8c Staff Sharing & Secondment
Pharmacy Team - -
Delivery Model Role Pay Band Supplier pool
Hospital Hub Delivery Model Vaccinator 3 NHSP, SJA
RHCP 5 Staff Sharing, Secondment, NHSP
• Delivery of vaccination to
the citizens in hospital hubs Registered HCP – Supervisor 6 Staff Sharing, Secondment, NHSP
HCA 3 Staff Sharing, Secondment, NHSP
• This table shows the total
workforce required which Vaccination Admin Support 3 Staff Sharing, Secondment, NHSP
can be scaled up and down
Front of House / Reception 2 Existing workforce bank, NHSP
based on local
requirements Nursing Manager 8a Staff Sharing & Secondment
Pharmacy Team - -
14 |Job Descriptions under National Protocol
Role Role
Band 3 Vaccinator Band 3 HCA
Band 5 HCP –
Band 3 Admin Support
Dilution required*
Band 5 HCP –
Band 2 Front of House/Reception
Dilution not required*
Band 6 HCP
Band 8a Nursing Manager
Clinical Supervisor**
* The original Band 5 HCP was designed to cover vaccine dilution
responsibilities. In instances where HCPs cannot dilute under the
Band 8b-8c Senior Manager
vaccine specifications guidance, please use the adjusted Band 5
JD.
** The original Band 6 JD has been amended to allow Allied Health
Professionals to be able to apply for this role.
ESM Operations Director
15 |Unregistered vaccinators: context
The unregistered vaccinator role was designed to operate under the National Protocol and enable mass delivery within the vaccination programme without adversely
affecting the registered workforce or impacting business as usual.
Benefits of using unregistered vaccinators:
• The COVID-19 vaccination programme requires a very large staffing pool to be able to deliver at
pace and at scale.
• The vaccination programme runs in parallel, not separate from, the delivery and recovery of business • Provide the volume of workforce required to
Situation
as usual NHS activity in both Primary and Secondary care deliver the vaccination programme
• Reduces the demand on the registered
workforce and is vital to enable business as
• Workforce capacity was identified as a potential constraint to meet the programme’s ambition as the usual to continue
existing NHS workforce alone could not meet the needed supply • Supports the sustainability of the
• As the number of available registered healthcare practitioners dedicated to the vaccination
Challenge programme for both primary care and acute
programme were limited, there was recognition that an expanded workforce was needed
providers
• Splitting the vaccination task into component
• Wide clinical consultation from the Clinical Advisory Group, Chief Nursing Officer’s Team and PHE
School Immunisation programme identified that the vaccination task can be safely split down into parts proved to be the optimal delivery
separate component parts model.
• A Statutory Instrument was laid to amend the Human Medicines Regulations to address the • Positively contributing to a reduced cost of
Solution
programme’s workforce constraints, enabling the expansion of workforce and breaking down
vaccination activity into component parts
the vaccination delivery model.
Solution • The legislative changes allow unregistered staff with appropriate training to administer the vaccine • Mitigating risks of training and
under the National Protocol, meeting the extra demand needed and reducing the pressure on deployment bottlenecks by using an
registrants
• In addition to local recruitment, the national supply chains have recruited and are in the process of
integrated delivery model
deploying more than 10,000 unregistered vaccinators to support the programme • Optimising the volunteer workforce
• St John Ambulance are also providing volunteers who can support (with the relevant pre-requisite
training and competency sign off) as unregistered vaccinators • Providing an essential workforce for the
• This solution addresses both primary and secondary care and should be widely adopted to release future
clinical staff
16 |How can you use unregistered vaccinators?
What can an unregistered vaccinator do? What can’t an unregistered vaccinator do?
Administer a pre-prepared vaccine dose: The Clinical assessment and consent process must be carried out
• To already consented and assessed individuals, under the direct supervision of a registered healthcare by a trained registered healthcare professional and this task cannot
professional (recommended ratio is 1:3 registered to non-registered staff) be carried out by unregistered staff.
• If they completed relevant online and face-to-face training and have been assessed and signed-off as
competent against the PHE COVID-19 Competency Assessment Tool
It is not recommended that an unregistered vaccinator dilute and
draw-up the Pfizer vaccine (unless they are currently working in an
An unregistered vaccinator can only be responsible for both the draw-up and the administration of the Astra- NHS Aseptic unit). This task should be carried out by a registered
Zeneca vaccine if: healthcare professional (usually at least a band 5 RCHP) under the
• The National Protocol for that vaccine legally allows them to do so supervision of a doctor, nurse or pharmacist (if not one themselves).
• They operate under the direct supervision of a doctor, nurse or pharmacist. This is in addition to the Clinical This should also apply to future vaccines that require dilution.
Supervisor overseeing the whole vaccination process as per National Protocol guidance. Oversight and direct
supervision needs to be based on an individual’s experience and competency. For inexperienced staff,
supervision needs to be provided on at least a 1:2 ratio until the member of staff gains more experience and
the supervisor is assured of competency Unregistered vaccinators cannot administer the vaccine under the
• They have experience of and have received specific training on drawing up of multi-dose vials as well as Patient Group Direction (PGD).
aseptic technique and infection prevention and control procedures. This will need to be provided and
competency assessed locally as there is no national provision. This needs to be structured training and not
just a ‘see one, do one’ approach
• They have been signed-off as competent. Competency must be assessed by a RHCP with experience and Unregistered vaccinators cannot vaccinate if they are not under the
knowledge of aseptic technique, usually a pharmacist from an NHS aseptic unit direct supervision of a registered healthcare professional.
The specifications above have been designed to ensure the safe delivery of the two known vaccines and their characteristics to date (Pfizer and AstraZeneca), in line with the legislation
and national clinical guidance and regulations. As and when new vaccines become available, principles will be re-evaluated to ensure that specific vaccine particularities are considered.
Utilisation of unregistered vaccinators should be congruent with the nationally recommended workforce pod models, red lines and principles. Please visit NHS Futures for
17 |
reference.How can you use unregistered vaccinators?
Unregistered
vaccinator pool
1 Unregistered
Can be considered for
vaccinator applicant
alternative roles within
without previous
the programme.
experience in a
clinical setting
2 3 2 3
2 Unregistered Training locally Signed off as
Face-to-face Signed off as provided based on set competent to
vaccinator applicant Deployed as
vaccination competent to training specifications draw up.
with previous vaccinator
training vaccinate for drawing up. Further Further information on
experience in a
information on slide 6&7. slide 6&7
clinical setting
3 Face-to-face vaccination Signed off as competent
St John Ambulance training ensured by SJA to vaccinate by SJA
(SJA) Volunteer Training Lead Clinical Lead
KEY
Vaccinator specific e-learning not completed Competency assessment not passed Vaccinator role not currently available Willing to undertake training in drawing up the
AZ vaccine
Vaccinator specific e-learning* completed Competency assessment passed Vaccinator role currently available
18 |Unregistered vaccinators drawing-up The National Protocol and characteristics of the AstraZeneca vaccine mean unregistered vaccinators can be considered and upskilled to draw-up the vaccine, based on appropriate training being completed and competency being signed off. Principles applied to unregistered vaccinators drawing-up: • Unregistered vaccinators can only draw-up the AstraZeneca vaccine (this will be re-evaluated as and when new non-dilution vaccines with similar characteristics become available) and under the National Protocol • Unregistered vaccinators are eligible to be considered for the draw-up task if they have previous healthcare experience • Unregistered vaccinators can undertake training in the draw-up task only after they complete all other vaccinator training • Unregistered vaccinators must be willing to undergo training and carry out the draw-up task • Training requirements are met before a vaccinator is signed-off as competent, in line with national guidance (see following slide) • Structured training covering all aspects needs to be described and provided locally as there is no national provision or standard • For inexperienced staff, supervision needs to be provided on at least a 1:2 ratio until the member of staff gains more experience and the supervisor is assured of competency • The draw-up task will be completed by an unregistered vaccinator when it is deemed locally as an efficient workforce model (e.g. improves throughput, optimises workforce, reduces the pressure on professional staff) • The employed unregistered vaccinators should be prioritised to be trained so we optimise the recruited workforce before using voluntary or military support • A proof of concept was undertaken with St John Ambulance to have their volunteers trained and signed off as competent to draw up. This was successful and can be used as a blueprint for roll out to other lead employers, refer to slide 8. • The unregistered vaccinator would operate under the National Protocol guidance using the national workforce model • Overall the decision to deploy unregistered vaccinators for drawing-up needs to take into consideration adherence to the clinical red lines and any legal requirements 19 |
Training specification for unregistered vaccinators drawing-up
Specific face-to-face training is required for unregistered vaccinators before being able to draw up vaccines. The training specification outlined below should be completed in addition
to all other vaccinator training (i.e. national e-learning modules and local face-to-face training in Immunisation, COVID-19 Vaccination, Anaphylaxis, Basic Life Support, IM injections
and Statutory/Mandatory training).
Training and competency sign-off for drawing-up will need to be provided locally as there is no national provision. Local consideration should be made on the approach to deliver the
training and assessing capacity to provide the training, how to ensure the right level of supervision for observation and sign-off, and how to create a safe simulated environment to
conduct the training sessions and assessment outside of an active pod.
Training standards and competencies to be assessed for drawing-up Competency sign-off process for drawing-up
The following training standards are required in addition to all other vaccinator training and competency
• The individual would need to be signed off as competent
assessment.
against the training standards usually by an experienced
The individual would need to undertake training and be competency assessed by an experienced aseptic unit aseptic unit pharmacist but could also be an experienced
pharmacist for the following: doctor or nurse.
• Aseptic technique specific to the needs of this role • Competency sign-off requires a suitable period of observed
• Understanding the correct syringe to use and being able to recognise it (i.e. dose sparing syringes provided practice until both the vaccinator and the registered
by the programme) pharmacist are confident that the vaccinator is competent in
• Drawing up of multi-dose vials: accurately drawing up correct dose (0.5mls) without wastage, expelling air the competencies outlined previously. The number of
to ensure air bubbles minimised, ensuring the vial is not shaken, avoiding multiple entries to the vial with observed practices or length of observation time required
the same needle should be locally evaluated (e.g. 1:1 direct supervision on 1-
• Ability to identify what the correct appearance of the vaccine should be and what abnormal looks like (i.e. 2-3h sessions).
white spots/black spots)
• Infection prevention and control procedures (as the vials are unpreserved) • Those unregistered vaccinators who pass their competency
• Safe management/disposal of sharps assessment can passport between sites/employers using
• Cold chain management (in instances where vaccinators withdraw vials from the fridge) their signed-off competency assessment.
If a non-registered vaccinator has a significant gap between shifts, it would be for local judgement to determine if they need to be retrained / re-assessed for competency. SJA
volunteers
20 | commit to 2 shifts a month and this has been assessed as being a minimum level to maintain their competency.Upskilling St John Ambulance volunteers and unregistered vaccinators
St John Ambulance (SJA) Volunteers and unregistered vaccinators successfully upskilled in drawing-up the AstraZeneca
Vaccine
A proof of concept was developed at two London Trusts, Barts Heath NHS Trust and Chelsea & Westminster
Hospital, to demonstrate the feasibility of upskilling St John Volunteers to both draw up and vaccinate the ✓ All trainees found training
AstraZeneca vaccine. clear and easy to follow,
and were confident to
undertake the draw up
• Chelsea & Westminster ran a small scale proof of concept made up of 2 volunteers and 4 NHS unregistered
activity.
vaccinators, involving trainees in both the draw-up and vaccine administration.
• On a larger scale, Barts adopted a different pod model training 30 SJA volunteers and practiced only the ✓ Supervisors considered
draw-up activity then passing the doses to the vaccinators. that the level of
individuals following
To select potential candidates, both Trusts worked with SJA to select candidates based training was appropriate
on a criteria looking at willingness to be upskilled, previous vaccination experience and to start in the pod
100% performance to date on the programme. Training was provided locally in line with
Competency national guidance on principles and training specifications with the Trusts defining the
assessment pass training environment, personnel and materials and providing a mix of e-learning
rate (module on the aseptic non-touch technique) and practical sessions on site. All “Trainees were keen to
trainees were then competency assessed and signed-off to practice in an active pod. learn, enthusiastic and
grateful for the opportunity.”
The proof of concept has yielded very positive results and has so far received good feedback from trainers,
- Trainer, Chelsea &
volunteers and supervisors. Wider rollout is now underway which will allow further opportunities for the Westminster
programme to optimise the workforce as well to strengthen relationships with the national suppliers.
21 |St Helens and Knowsley Teaching Hospitals NHS Trust
Delivering the vaccine programme alongside the Merseyside Fire & Rescue Service
Merseyside Fire and Rescue Service (MFRS) are proud of the relationships they have developed
over many years with their partners including those in Health and Social Care. When Covid-19
first arrived, the Service started to think differently. They offered support with many Covid related
activities and in December 2020, the Service was asked if it would be able to help deliver
the vaccination programme.
St Helens and Knowsley Teaching Hospitals NHS Trust arranged NHS educators to train a large number of MFRS workforce to vaccinate,
enabling them to support those delivering the programme in Merseyside. They now have 130 trained vaccinators and a further 50 individuals
providing admin support and patient care. The ‘volunteer workforce’ includes firefighters, control staff, trainers, workshops staff, Officers, HR,
Finance and other support staff, with even the Chief Fire Officer trained as a vaccinator. Since 8 Feb the MFRS team has administered over
10,000 vaccinations, drawn up thousands and supported over 30,000 vaccinations through their 3,000 or so hours of support.
They have integrated seamlessly with those from St Helens and Knowsley Teaching Hospitals NHS Trust and have offered their support in
varying roles and shift hours with minimal issues. Feedback from patients has been very positive, and among the volunteer workforce
themselves they describe the experience as ‘heart-warming’ and ‘an honour’ as they have been able to reunite families and deliver a
programme that impacts not just the region, but the entire country.
“We feel privileged to be in such a position where we are able to help to end the pandemic. Our staff from right across the Service have stepped forward in their
numbers to contribute towards vaccinating the nation. Alongside the British Army, Royal Navy, St John Ambulance, Hospital Volunteers, Site staff and of course our
amazing NHS colleagues, we are extremely proud that they are able to make such an enormous difference. The team really is incredible.”
Mark Thomas, Group Manager for Prevention, Merseyside Fire and Rescue Service and Lead Officer for the Covid-19 Vaccination Programme
22 |Hampshire and Isle of Wight Workforce Bureau
Recruiting for a blended workforce across Hampshire and Isle of Wight (HIOW)
It was identified early in the programme that relying solely on registrants to deliver vaccines would be difficult for the system
and so, the teams at HIOW Workforce Bureau and Solent NHS Trust (lead Provider) partnered with University
Hospital Southampton NHS Foundation Trust (lead Employer) and NHS Professionals (NHSP) for their recruitment efforts.
This led to the creation of a blended workforce made up of unregistered vaccinators working under the national protocol
with existing mutual aid healthcare professionals across four vaccination centres.
Developing the unregistered vaccinator workforce
Recruiting for the workforce was conducted in a varied manner with candidates coming forward from the national
NHSP campaign, local social media campaigns, NHS Jobs and Indeed with over 6000 applications for unregistered
vaccinator positions. A comprehensive workforce development pack was developed to support training for both the
registered and unregistered workforce. Face to face training was delivered with support from local universities,
in house trainers, and private providers, accompanied by the e-learning for health (eLFH) modules. Licences were acquired
for additional specific online training with statutory and mandatory training requirements streamlined. Currently there are
over 450 unregistered vaccinators available across HIOW, with almost all vaccinator shifts in the vaccine centres filled
until the end of May. Some Primary Care Networks and Community Pharmacies are also starting to book shifts for unregistered vaccinators.
“Love working here, such a great set up and lovely people….I have such respect for the NHS, but from what I have seen, and also from what I have heard from
patients, this is Britain at its best. So many people that have passed through the centre have said how slick and efficiently the service runs.”
Vaccinator
Relying solely on the registered workforce to deliver across four vaccination centres was recognised as unsustainable from the beginning and so, recruiting and
training the unregistered workforce has been crucial to the success of our vaccine delivery.’
Angela Murphy, Vaccinations Programme Lead, HIOW STP System Workforce Team
23 |Alternative Clinical Assessment: Context
The nationally recommended pod model for vaccination centres was designed to support high-volume and clinically safe vaccination at scale. The pod model was
developed following extensive engagement and using simulation software to create a standardised workforce model, which was then tested in live exercises to
develop the optimal delivery solution. The modelling highlighted that splitting of the tasks within the vaccination pathway was the most efficient clinical model,
and therefore the national protocol has been introduced to enable the optimal clinical model to be achieved.
As we continue to deliver the vaccination programme, we are able to learn and evaluate the pod model activity to identify opportunities to refine, innovate and
optimise. This document provides guidance on alternative delivery models to streamline the clinical assessment component of the vaccination
pathway, by utilising pre-screening of patients, and is designed for both vaccination centres and PCNs under the National Protocol. This will provide
opportunities to improve efficiency, patient experience, release time to care for more complex patients, increase throughput and optimise workforce skill mix.
We are looking at “the world of the possible” to
There are strict legal and clinical requirements The following solutions are
innovate while complying with these
that must to be followed: proposed and detailed in this pack:
requirements:
• Under the National Protocol, clinical assessment and informed consent must be
• Fast-tracking the assessment
undertaken by a registered healthcare professional • There is an opportunity to ensure processes are process – reducing clinical
• Clinical assessment and consent is a mandatory requirement in the process and must optimised to reduce the number of registered assessment time by offering members
be completed for each of the doses delivered healthcare professionals required by the existing of the public the choice to complete a
pod model: screening questionnaire and utilising a
• Consent must be taken on site on the vaccination day irrespective of the dose
✓ For individuals with no complex medical fast-track triage route enabling more
• Consent must be given voluntary by an appropriately informed person who has the situations or those whose medical situation time to be spent with those patients
capacity to make the decision has not changed since first vaccine dose that need it
• Clinical assessment adheres to the minimum standard for the vaccination programme ✓ When individuals can be pre-screened prior to • Virtual clinical assessment –
(i.e. screening questions in the Point of Care system have been addressed) clinical assessment and consent at the same reducing the time spent at the
• Appropriate escalation points must be in place for any issues raised during the clinical standards vaccination site by offering members
assessment process ✓ When relevant information is provided of the public the choice to complete
pre-screening questions and being
• For full guidance on clinical red lines and design principles, please refer to the pod beforehand on anticipated benefits, risks and
likely side effects clinically assessed by a clinician on
model documentation attached in the appendix. Full guidance on consent:
the phone (if required)
https://future.nhs.uk/CovidVaccinations/view?objectId=95245253
24 |Streamlining the clinical assessment and consent stage by fast-tracking eligible
individuals: principles
Under the National Protocol, clinical assessment and consent must happen for each of the vaccination dose and must be carried out by a registered healthcare
professional. There is an opportunity to offer an alternative process for eligible individuals by implementing a screening questionnaire which members of the public can
choose to complete prior to being assessed. A triage stage can be introduced to review the questionnaire and identify those individuals who can be fast-tracked to an
expedited assessment and consent checkpoint. A registered healthcare professional will ensure the patient is suitable and offers informed consent before proceeding to be
vaccinated. As we are moving into younger cohorts and second doses, this approach has several benefits: it maximises throughput, it reduces the number of registrants
required for clinical assessment and it further encourages the vaccine administration to be separate from clinical assessment.
Vaccine
Before clinical assessment Triage Fast-tracked clinical assessment
delivery
✓ An appropriately trained member of staff checks ✓ A registered healthcare professional:
✓ Individual completes a standardised set
the screening questionnaire and directs the • Reviews the screening questionnaire and confirms if the
of screening questions
patient through the appropriate lane patient is clinically suitable to have the vaccine
✓ Questions have a yes or no response
✓ The triage role can be filled by unregistered • Ensures patient has been provided with sufficient
and are matching those in the exclusion
staff, but not by volunteers information (e.g. on side effects or post vaccination care) ✓ Eligible and
and caution checklist in the Point of
✓ Patient can be fast-tracked if: • Obtains informed and voluntary consent consented
Care system (refer to Appendix)
• Questionnaire is fully completed ✓ An administrator: individuals
✓ Stewards will provide and encourage
can proceed
patients to complete the form • They have answered NO to all questions • Searches for the patient in the IT system and confirms
to receive the
• They are clear on the process and have no vaccination history and any potential alerts for previous
✓ Completing the questionnaire is not vaccination
additional questions or concerns Flu or Covid-19 vaccinations
mandatory and will not determine the
• They have the capacity to give consent • Records the screening answers and consent on behalf of
eligibility for receiving the vaccine
themselves the healthcare professional
✓ There is a further opportunity to consider • Can be an unregistered member of staff, but this role is
✓ Patients who do not meet all the above criteria
the implementation of a digital solution not appropriate for volunteers
won’t be fast-tracked and will go through the
to complete the pre-screening process
existing pod model lane. ✓ Patient provides voluntary and informed consent
A larger pool of St John Ambulance Patient Advocates should be utilised to ensure the patients get all the relevant information on risks, benefits and post vaccination
care, to support the pre-consent conversation with the nurse, therefore speeding up the process.
Appropriate
25 | levels of volunteer stewards at the front and back end of the vaccination pathway are required to ensure that patient flow is maintained. Increase in clinical assessment and
vaccination lanes should be proportionate with the increase in steward staffing.You can also read