COVID-19 Testing Framework Implementation Plan - October 2021 Version 1.2 - COVID-19 Testing Framework Implementation Plan - October 2021
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Version 1.2
COVID-19
COVID-19 Testing
Framework
Implementation Plan
October 2021
COVID-19 Testing Framework Implementation Plan - October 2021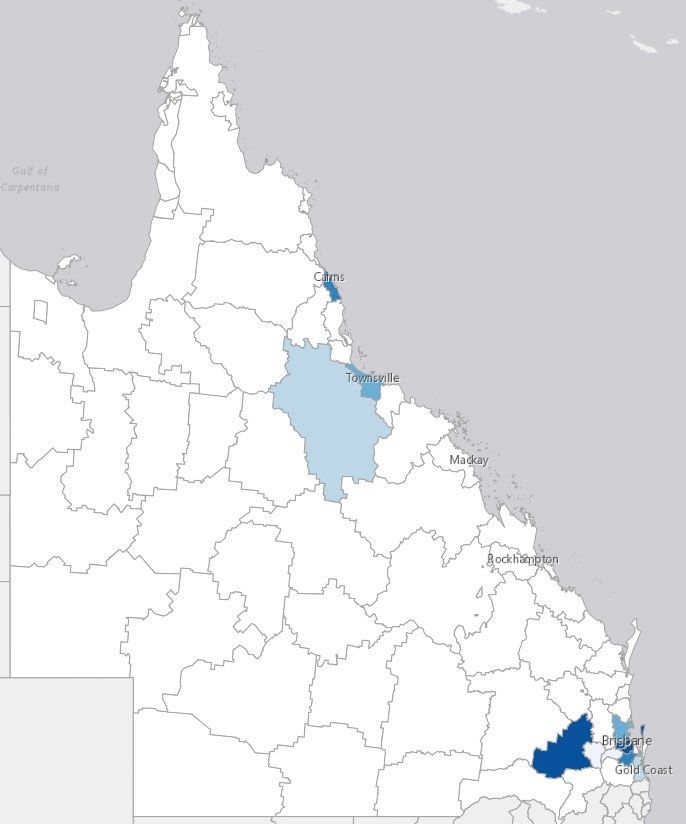
Document COVID-19 Testing Framework Implementation Plan
Purpose To provide best practice guidance to health professionals involved in the testing for
COVID-19. This document should be read in conjunction with:
Supporting National CDNA and • CDNA National Guidelines for Public Health Units
Documents PHLN
• Public Health Laboratory Network guidance on laboratory
testing for SARS-CoV-1 (the virus that causes COVID-19)
Queensland Health • Personal protective equipment (PPE) | COVID-19 |
COVID advice Queensland Health
• Queensland Health Infection Control Guidelines
• Guide to informed decision-making in healthcare
Consumer healthcare • The Australian Charter of Healthcare Rights
rights
Aeromedical retrievals • COVID-19 information for aeromedical retrieval of patients
Aboriginal and Torres • Queensland Public Health Guidelines for Managing a
Strait Islander people COVID-19 outbreak in First Nations communities
• Testing Checklist for Aboriginal and Torres Strait Islander
people
• Aboriginal and Torres Strait Islander COVID-19 POC Testing
Program Guidelines
• Aboriginal Community Controlled Health Services
Pandemic Response Toolkit
Culturally and • Queensland Health CALD COVID-19 Policy and Action Plan
Linguistically Diverse
• Australian Red Cross Communicating in Recovery (best
practice principles around engagement with people from
culturally and linguistically diverse backgrounds)
• COVID-19 Translated Resources
Disability • Responding to a suspected case of COVID-19 in disability
accommodation and residential services
• Information for disability support workers and carers on
coronavirus (COVID-19) testing for people with a disability
COVID-19 Testing Framework Implementation Plan - October 2021 Page 2
Document COVID-19 Testing Framework Implementation Plan
Supporting Residential aged care • CDNA National Guidelines for the prevention, control and
documents public health management of COVID-19 outbreaks in
residential care facilities in Australia
• Pandemic Response Guidance Personal Protective
Equipment in Residential Aged Care and Disability
Accommodation Services
• Infection Control Expert Group (ICEG) Coronavirus (COVID-
19) Guidelines for infection Prevention and Control in
Residential Aged Care Facilities
Correctional facility • CDNA National Guidelines for the Prevention, Control and
residents Public Health Management of COVID-19 Outbreaks in
Correctional and Detention Facilities in Australia
Meat and poultry • Managing the risk of coronavirus (COVID-19) exposure:
processing workers Meat and poultry processing
• Meat & Poultry Processing Facility Assessment Toolkit
COVID-19 Testing Framework Implementation Plan - October 2021 Page 3Background
The Testing framework for COVID-19 in Queensland (testing framework) is intended to outline the
full suite of testing options for SARS-CoV-2 (the virus that causes COVID-19) for clinicians and
decision-makers in Queensland to optimise case ascertainment and surveillance and inform the
public health response.
The framework outlines the priority settings in which testing is currently being conducted or
proposed to be conducted for COVID-19 and emphasises that the highest priority group for
testing is people with symptoms of the disease. The needs of rural and remote populations are
integrated into the overall testing strategy.
The testing framework is supported by specific consideration of testing strategies for the
following population groups or settings:
1. quarantine travellers and close contacts of confirmed cases
2. people undergoing aeromedical retrieval
3. Aboriginal and Torres Strait Islander communities
4. people experiencing homelessness
5. people from Culturally and Linguistically Diverse (CALD) communities
6. residential aged care settings
7. people with disability
8. congregate living and working settings.
Purpose
This document provides guidance on the strategies that have been or will be implemented by
Queensland Health to ensure that adequate COVID-19 testing is available to all Queenslanders,
where indicated for clinical or public health reasons.
Note: Knowledge about COVID-19 is evolving and therefore Queensland Health will continue to
review and update this testing strategy as new information becomes available.
COVID-19 Testing Framework Implementation Plan - October 2021 Page 41 Testing Strategy Summary
Objectives
To ensure early detection of COVID-19 in Queensland through a testing strategy that:
1. Ensures that testing is accessible and that the most appropriate type of testing is
used for each individual’s situation
2. Triggers early implementation of appropriate infection control measures
3. Informs a rapid and effective public health response
4. Triggers activation of Queensland Government rapid response plans
and
5. Has regard for the wellbeing, rights and dignity, including a priority focus on
consent, advocacy and support for people being tested for COVID-19.
Principles
The following key principles apply to the testing strategy:
1. A risk-based approach is adopted to consider the likelihood of exposure, such as the
characteristics of the setting, the nature and needs of people living in these
environments, the nature of work performed and the mechanisms available for
people to protect themselves from infection in these settings.
2. The testing capacity must be used to best effect.
3. Testing is reliant on effective prevention, screening and surveillance strategies.
4. Testing is universally available i.e. it is not restricted based on factors such
as financial capacity to pay, legal status, residency, cultural background, age or
disability.
5. Testing is encouraged and offered to the benefit of the individual, their family and
friends, and the wider community.
6. Testing is reliant on action being taken on the testing results at an individual,
community and population level. Action includes a comprehensive approach
to treat, isolate and contact trace to suppress transmission.
The testing strategy and its implementation are underpinned by the principles of the
Australian Charter of Healthcare rights (1):
1. Equity of access to testing
2. Safety of individuals (consumers and staff) and community
3. Respect for consumer dignity and culture
4. Partnership including rapid access to results of testing and information about the
test and results
5. Privacy
COVID-19 Testing Framework Implementation Plan - October 2021 Page 5Methods
The testing strategy is intended to be implemented in a manner that supports any broader
strategies and / or benchmarks for COVID-19 in Queensland.
The testing strategy will focus on:
1. Accessibility of testing with a focus on testing in symptomatic people, those with
epidemiological links (stratified by risk) and in high risk and vulnerable groups
2. Positive results are automatically notified to Public Health Units and patients, with
early implementation of appropriate infection control and public health measures
including isolation of all cases and contact tracing
3. Rapid public health response to confirmed cases occurring in high-risk settings,
including aged or disability care settings and congregate living or working settings
4. Identification of new variants of concern or of clusters through whole genome
sequencing in collaboration with epidemiological investigations.
Core elements of the testing strategy are outlined in figure 1.
Figure 1: Core elements of the Queensland Health testing strategy
Specimen
HHS planning and collection & Testing: clinical Testing of specific
Communications Evaluation
logistics laboratory guidance populations
services
Quarantine travellers and
Essential and enhanced close contacts
testing facilities Suspected COVID-19
Accessibility of testing Consumer Accessibility
Aeromedical retrievals
Aboriginal and Torres
Surge testing
Strait Islander
communities
Enhanced testing
Congregate setting
residents
Setting considerations Types of tests Internal communications Safety
Residents of aged care
facilities
Outbreak testing
People with disability
Workforce
People experiencing
homelessness
Specimen collection External communications Escalation
Expanded testing
Consumables (population surveillance) Culturally and
linguistically diverse
communities
COVID-19 Testing Framework Implementation Plan - October 2021 Page 62 HHS planning and logistics
Operational Context
COVID-19 testing programs provided by Hospital and Health Service (HHS) Public Health
Units operate in response to the level of the pandemic (as determined by Health Directives
of Queensland’s Chief Health Officer) as well as any epidemiological intelligence of the level
of virus within local communities.
Each HHS with their Public Health Unit develops strategies and plans to guide their COVID-19
testing programs. These plans should consider the needs of quarantine travellers and close
contacts of confirmed cases, rural and remote populations, Aboriginal and Torres Strait
Islander communities, people experiencing homelessness, culturally and linguistically
diverse communities, healthcare and residential aged care settings, people with disability
and congregate living/working settings.
Each HHS with their Public Health Unit will develop strategies and plans to guide their
COVID-19 testing programs. These plans will need to cover varying contexts:
• Small discrete townships and outstations
• Towns with Queensland Health Multi-Purpose Health Centres (MPHCs) and hospitals
only
• Towns with Queensland Health facilities, GPs and private pathology collection
centres
• Cities with COVID-19 Respiratory clinics
• Discrete Aboriginal and Torres Strait Islander communities
Essential and enhanced testing facilities
All Queensland Health facilities have plans in place for Essential testing due to symptoms
with epidemiological links or epidemiological links alone, and the enhanced testing of
individuals presenting with symptoms of COVID-19, without epidemiological links (2).
Options will include testing via:
• Emergency Departments (EDs), Primary Healthcare Clinics, Aboriginal Community
Controlled Health Services
• Fever clinics including drive through and walk in options
• COVID-19 respiratory clinics, supported by Primary Health Networks (PHNs)
• Private pathology providers via General Practitioner (GP) referral (outside of surge
testing)
• Pop up testing clinics implemented during surge testing periods
COVID-19 Testing Framework Implementation Plan - October 2021 Page 7Surge or outbreak testing Surge testing as part of HHS Rapid Response Plans could encompass all of the above with extended hours for established clinics and the use of pop-up clinics. Surge testing will be of short duration and high intensity. Health and Hospital Services (HHSs) and Public Health Units (PHUs) should have plans in place for surge staffing to support testing in outbreaks in high-risk settings, when directed by Public Health Units, and the people with symptoms in the local community when directed by the Chief Health Officer (CHO). Surge testing planning requirements are outlined in table 1 below. COVID-19 Testing Framework Implementation Plan - October 2021 Page 8
Table 1: HHS surge testing planning requirements
Domain Resources Comments
Planning Need • Number of people and predicted volume of tests required across a range of outbreak scenarios
• High risk populations or populations with specific needs including Aboriginal and Torres Strait Islander communities,
residential aged care facilities, disability accommodation facilities, homeless population and homeless shelters,
Culturally and Linguistically Diverse communities, places of detention (prisons, watch houses, youth detention centres,
immigration detention facilities, community correctional centres), congregate living settings (boarding houses, student
accommodation, women’s refuges, seasonal workers dormitories), high density housing, places of education and
childcare centres, high density work sites (e.g. factories and processing facilities, abattoirs)
Testing capacity • Public and private testing capacity
Environment Location • Consider consumer and staff safety, consumer convenience, and service efficiency
• Optimising accessibility of testing to residents throughout the geographic area of the HHS, across public and private
pathology service providers
• Testing to occur outdoors, where possible – ensure attention to staff safety to prevent risks of dehydration or heat illness
Safety • Capacity to isolate people effectively in the setting
• Pre-existing and current capacity to implement preventative public health measures, including consideration of
environmental, engineering, social and medical factors including vaccination rates of residents / clients and staff
Accessibility • Optimising accessibility of testing sites to persons with disability or frailty – see appendix 1 for details
Staff Staffing • Who collects the tests including their ability to comply with any related public health directions relevant to that setting
considerations in (e.g. Aged Care Direction)
setting-specific
contexts • Education, skill and capacity: Skill, knowledge and capacity of staff working in these settings
Testing staff • HHS staff and / or private pathology laboratory staff, GPs, Aboriginal Community Controlled Health Service staff or
community-based clinicians
COVID-19 Testing Framework Implementation Plan - October 2021Triage staff • Nurses and Aboriginal Health Workers to:
• Triage patients based on:
o Essential versus enhanced testing
o Clinical risks and stability
• Assist in completion of enhanced data surveillance forms
Administrative • Administrative support for registration and generating HBCIS records (and / or episodes of care in relevant digital system
staff depending on type of episode)
Outreach teams • Ability to provide outreach testing teams for instances where surge testing involves persons who experience difficulty in
undertaking travel to hospital e.g. disability accommodation services
Consumables PPE • Ensure access to adequate supplies of PPE aligned to the relevant Queensland Health PPE guidance
Testing • Ensure access to adequate supplies of testing consumables including point-of-care (POC) cartridges where relevant
equipment
Communication Patients • Mechanisms to advise patients of their results in a timely and effective manner – ensure accurate contact details
collected at registration
• Consideration of communication of test results to those who have special communication needs
Transport Transportation of • Ensure transportation of swabs has clear arrangements across a range or geographic and setting scenarios.
tests to
laboratories for
testing
COVID-19 Testing Framework Implementation Plan - October 2021 Page 10Transport
• Each laboratory option has differing turnaround times depending on their location and
transport times for swabs to the larger laboratories.
• Where patients are close contacts or live or work in high-risk environments, testing
should occur via the closest laboratory with the shortest turn-around time to allow
early identification of cases and early implementation of public health measures.
• Plans for transport of swabs with additional courier runs in the event of reduced
flights need to be considered and for extended or surge testing.3 Specimen collection and laboratory
services
A range of Pathology Services provide specimen collection and laboratory testing services in
Queensland.
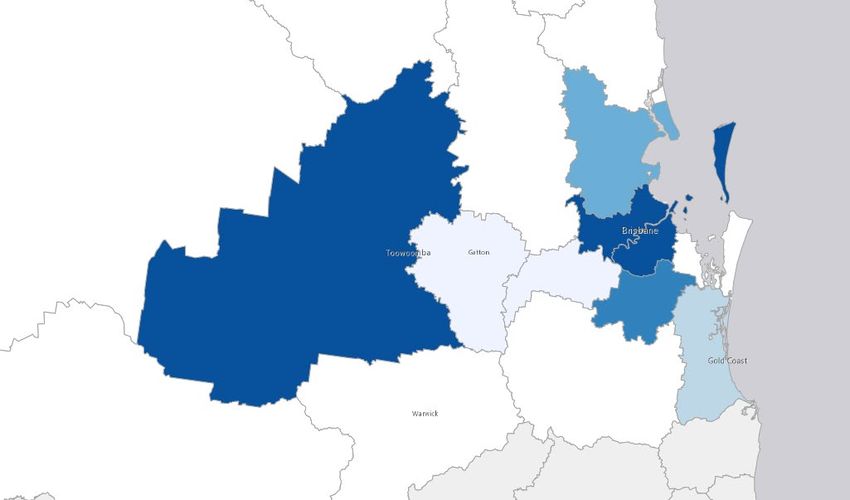
Each HHS will have varying laboratory options that will be used as appropriate for the
pandemic stage and type of testing being implemented. Private pathology companies’
laboratories with COVID testing machines are predominantly located in Brisbane, with some
private providers using interstate laboratories. Queensland Health laboratories have varying
testing capacity spread across the state. The reference laboratories are located at Forensic and
Scientific Services (FSS) at Coopers Plains and Royal Brisbane and Women’s Hospital at
Herston.
Where the Services are undertaken by a public pathology provider, Queensland Health
anticipates that results will be available within 24 - 36 hrs. Results for Services undertaken by
some private pathology providers (e.g. 4CYTE and Medlab) that utilise interstate laboratories
may take longer to receive. During times of high demand (i.e. increase in community
DRAFT
transmission) Queensland Health cannot guarantee any timeframe, whether for public or
private pathology providers.
Test results are uploaded from all pathology providers into the Notifiable Conditions System
(NOCs), the State-wide Public Health Unit Database.
For Services undertaken at private pathology providers, a GP referral is generally required, as
per Commonwealth Medicare requirements. During periods of surge testing, Queensland
Health may waive the need for a GP referral – notification of this , when enacted, will be made
to private providers at the daily State Health Emergency Coordination Centre (SHECC)
meetings and to the public on the Queensland Health testing and fever clinics website.
Accessibility of testing
All Queensland COVID-19 testing clinic locations can be found on the Queensland Health
testing and fever clinics website including information on testing for children. Drive-through
clinics are available in a number of locations throughout the state, and these can be found by
searching the clinic list. Private providers of collection and laboratory services advertise their
COVID testing centres on their private websites.
COVID-19 Booking and Triage Solution
The COVID-19 Testing – Booking and Triage Solution (the solution) was developed by Clinical
Excellence Queensland in partnership with eHealth, clinicians and consumers. The solution
prioritises those most in need of a test based on their epidemiological and clinical criteria.
For more information, please visit COVID-19 Testing – Booking and Triage Solution Queensland
Health
COVID-19 Testing Framework Implementation Plan - October 2021 Page 12Testing and fever clinics — coronavirus (COVID-19)
• Fever clinics - Fever clinics are specialist clinics managed by Hospital and Health
Services that assess people who may be infected with COVID-19. These clinics help to
keep people who may be contagious away from other areas of hospitals and health
centres. This helps to reduce the potential spread of the virus and keeps the
emergency department available for emergencies.
• Respiratory Clinics - Respiratory clinics are doctor (GP)-led clinics that provide face-to-
face assessments, testing and treatment for people experiencing mild to moderate
respiratory symptoms. This includes testing for COVID-19.
For more information, please visit Testing and fever clinics — coronavirus (COVID-19
Mobile Collection
Mobile collections provided by private pathology laboratories include:
• Mater Pathology provide home testing to people with a disability. Depending on
demand, same day testing may be possible. Testing occurs between 10am – 4pm.
• QML Pathology provide home testing to people with disability. It is handled on case-
by-case basis and the referrer (doctor/clinic) needs to organise it with QML. QML need
to know the nature of the disability so they know whether to send one or two people
DRAFT
to collect the sample. There would be a different approach for an outbreak
investigation.
• Sullivan & Nicolaides Pathology (SNP) offers mobile home collections for patients with
a disability and this must be requested by their referring doctor through the SNP
home visit team on 07 3377 8666 (Monday – Friday 6.30am to 5.00pm and Saturdays
7.00am – 12.00pm)
• Medlab and 4Cyte Pathology do not provide mobile or home collections in
Queensland.
For people with disability and/or their carers that are still unable to access testing through the
above mobile collections, consumers or their support person can contact 13 HEALTH and
discuss requirements with the clinician.
Regional Testing capability and laboratories across the state
Appendix 2 lists the sites of the GeneXpert (Rapid Testing) and Panther or COBAS (High
capacity) machines across Queensland and their capacity. Supplies of reagents, swabs, and
POCT cartridges need to be monitored. There are 19 sites in Queensland that are affiliated
with the Kirby Program. These sites include hospitals, Primary Health Care Centres (PHCCs)
and Aboriginal and Islander Community Controlled Health Services (AICCHSs).
Forensic and Scientific Services (FSS)
FSS is the Reference laboratory for Queensland. All positive polymerase chain reaction (PCR)
tests are sent to FSS for genomic sequencing.
COVID-19 Testing Framework Implementation Plan - October 2021 Page 13Laboratory testing: types of tests
Nucleic acid amplification testing (NAAT)
• Reverse transcriptase PCR (RT-PCR) is the routinely performed laboratory test for SARS-
CoV-2. In general, turnaround times are less than 24 – 48 hours when using high-
throughput testing (e.g. when using PANTHER or COBAS machines at larger Queensland
Health laboratories). PCR tests are the most accurate tests for detection of SARS-CoV-2
– however, clinicians need to appreciate that no test has 100% sensitivity and
specificity in all clinical circumstances, with rates of false positives / negatives
influenced by pre-test probability and community prevalence.
• GeneXpert is a low throughput (4-8 swabs simultaneously), fast turn-around (45
minutes per run) test that may be used in select circumstances such as testing in
remote communities or where a rapid result is required for clinical / logistic reasons.
GeneXpert testing is not suitable for enhanced surveillance, surge or mass testing. The
supply of GeneXpert cartridges is limited.
Rapid antigen testing
• Rapid antigen tests can provide results within 15 to 30 minutes – however, they have
less sensitivity than NAAT tests and may be less specific (3-6). In the setting of low
community transmission, use of rapid antigen testing is not supported. As community
transmission increases, there may beDRAFT
a role for rapid antigen testing as directed by
public health units or the Chief Health Officer. For further information refer to the
PHLN – CDNA Joint statement on SARS-CoV-2 Rapid Antigen Tests
Genomics
• Genomic sequencing is performed on positive SARS-CoV-2 PCR results to facilitate
assessment of genomic relatedness of COVID-19 cases to identify emergence of new
variants of concern and inform public health management of clusters
• Where the genomic sequence of the virus can be established, it helps Public Health
and the epidemiologist to determine the source of the COVID infection and focus the
response
Serology
• Detection of antibody response to infection with SARS-CoV-2 occurs within 1 – 3 weeks
following infection, with IgG reliably detected by 21 days post-infection but is
influenced by patient factors
• Is not useful for acute diagnosis of COVID-19 and is not useful in those who have
received COVID-19 vaccination
• The main uses of serology are for:
− Identifying historical cases who remain NAAT positive (e.g. people testing positive
with unclear epidemiological links)
− Providing potential links in transmission chains in defined cluster outbreaks
COVID-19 Testing Framework Implementation Plan - October 2021 Page 14Specimen collection
• There are currently two specimen types validated for use in Queensland:
− Oropharyngeal and bilateral deep nasal swab using a flocked swab remains the
preferred approach – for a detailed description of the approach to swab collection
refer to PHLN guidance (7).
− Saliva testing: generally reserved for testing quarantine staff and healthcare
workers as part of a screening program. Note: saliva testing, when compared to
combined oropharyngeal and bilateral deep nasal swabs, has a lower percentage of
positive results, with this being amplified in settings with low prevalence (8). It
may be considered for use, in consultation with Infectious Diseases specialist or
public health physician, in patients where traditional sampling would otherwise
require sedation e.g. persons with cognitive impairment and severe behavioural
disturbance or in young children.
• In the event of simultaneous mass testing in an accommodation setting, the Public
Health Unit or Outbreak IMT will categorise residents / clients to prioritise the
collection and processing of PCR tests collected according to exposure risk level.
Personal Protective Equipment during testing
PPE should be used in accordance with guidance
DRAFTin Queensland Health’s Infection prevention
and control guidelines for the management of COVID-19 in healthcare settings . Consider
supply and resupply and the relevant logistics.
COVID-19 Testing Framework Implementation Plan - October 2021 Page 154 Testing: clinical guidance
Testing for SARS-CoV-2 may be undertaken in the following contexts, each of which has
associated requirements in relation to quarantine / isolation (see table 2):
1. Essential testing for suspected COVID-19 (symptoms and epidemiological risks)
2. Enhanced testing (symptoms with no epidemiological risks)
3. Testing of asymptomatic people in the context of any of the following:
a. An outbreak in a congregate living setting after a confirmed case in a staff
member, resident, or visitor, or prior to declaring such an outbreak over.
b. Testing in COVID-19 quarantine.
c. Surveillance testing in identified high risk environments and groups at the
discretion of the Incident Management Team (IMT) or Public Health Unit or the
Chief Health Officer – examples include surveillance testing of COVID-19
quarantine and isolation facility workers.
In order to ensure that the appropriate advice is given to consumers, persons presenting to
health settings for consideration of COVID-19DRAFT
testing, should be screened using a COVID-19
Clinical Screening Assessment process or tool. This assesses the risk factors for and evidence
of severe disease. Where indicated, community testing centres or fever clinics should refer
individuals who are unwell to their GP (via telehealth / telephone initially) or ED as indicated,
for further assessment.
Testing strategies will necessarily change as levels of community transmission change. With
increasing community prevalence of disease, pre-test probability of COVID increases across all
patient groups. It is estimated that 15 to 48% of patients with COVID-19 remain asymptomatic
throughout their infection – therefore, as community prevalence increase, testing strategies
and hospital models of care need to evolve to continue to minimise risk of hospital-based
transmission.
Testing strategies across hospitals in the setting of high levels of community transmission are
outlined in table 3 - this guidance should not replace clinical judgement individualised to the
presentation and local modifying factors. Testing strategies in the setting of escalating
community transmission will only be successful in minimising hospital-based transmission if
supported by:
1. High levels of population and healthcare workers vaccination against COVID-19
2. Utilisation of infection control strategies that span the spectrum of hierarchy of
controls
3. Models of care that:
a. Limit avoidable face-to-face interaction e.g. use of telehealth instead of face-to-
face review for OPD where clinically appropriate
b. Support clinical risk assessment and utilisation of appropriate rapid testing
modalities prior to patient entry to high-risk clinical environments
c. Support rapid streaming of COVID positive patients to dedicated, physically
appropriate environments, by-passing high risk clinical environments such as
emergency departments
COVID-19 Testing Framework Implementation Plan - October 2021 Page 16d. Support use of technologies to limit crowded waiting rooms or avoidable queueing
DRAFT
COVID-19 Testing Framework Implementation Plan - October 2021 Page 17Table 2: COVID testing indications
Indication for COVID-19 testing Inclusion criteria / Type of SARS-CoV-2 test
identification No to low community transmission (elimination Emergence of community transmission (suppression
phase) phase)
Suspected COVID-19 • Symptoms of COVID-19 • RT-PCR (standard) • RT-PCR (standard)
AND • Consider RT-PCR (rapid) if any of: • RT-PCR (rapid) if any of:
• Epidemiological risks 1. Requirement for urgent aerosol generating 1. Urgent AGPs
(see CDNA guidance for procedures (AGPs) 2. Urgent critical care such as operating theatre or
specific clinical and 2. Aeromedical retrieval maternity interventions or labour
epidemiologic criteria) 3. Critical ED flow requirements 3. Acute severe behavioral disturbance unresponsive to
4. Urgent critical care such as emergency verbal de-escalation and where sedation is indicated
operating theatre or emergency maternity 4. Aeromedical retrieval
interventions or labour 5. Hospital admission indicated
5. Acute severe behavioral disturbance 6. Discharge to high-risk setting1
unresponsive to verbal de-escalation and where • All patients should remain appropriately isolated until
sedation is indicated :
Enhanced testing • Symptoms of COVID-19 • RT-PCR (standard) - where RT-PCR positive, release from isolation criteria
Note: in low risk of transmission WITHOUT • Consider RT-PCR (rapid) if no alternate cause of are met, or
community settings (as defined by epidemiological risks symptoms is identified AND any of: - where relevant, until released from quarantine, or
the Chief Health Officer), enhanced 1. Requirement for urgent Aerosol generating - where PCR is negative in patients with low pre-test
testing is indicated where symptoms procedures probability
are not explained by an alternate 2. Aeromedical retrieval • Rapid antigen testing (Rapid Ag) may be used to
cause; 3. Critical ED flow support rapid identification of positive cases where
in very high-risk community settings 4. Discharge to high-risk setting1 where high pre-test probability exists as community
across all levels of community admission until RT-PCR (standard) result is prevalence increases – the role of rapid antigen testing
transmission or in scenarios of high available is not feasible will be defined by the relevant public health direction
community transmission, all patients
are considered to have
epidemiological risk
Outbreak Congregate living • No symptoms of COVID- • RT-PCR (standard) • RT-PCR (standard)
testing settings 19 AND • Where index case is confirmed positive, consider Rapid
• lives in a congregate Ag testing to support rapid identification of positive
living setting with a cases as a supplement to RT-PCR at discretion of local
current outbreak of public health unit where consistent with relevant
COVID-19 public health directionClose contact, • No symptoms of COVID- • RT-PCR on day 0, (day 5) and day 12-14 of • Test high-risk close contacts at entry and exit from
secondary contacts or 19 AND quarantine quarantine (typically at day 12 if 14 day quarantine but
persons in quarantine • Identified as a close drop routine day 5 testing unless there is sufficient
(including if admitted contact of a confirmed testing capacity to continue); test all others in
to hospital) COVID-19 case quarantine if symptomatic and at exit from quarantine
Surveillance Identified high risk At the discretion of the • Defined by Chief Health Officer in public health • Approved tailored testing program involving regular
testing environments Incident Management Team, direction Rapid Ag testing in combination with reduced RT-PCR
Public Health Unit and the over a 7 to 14-day period for essential or critical
Chief Health Officer e.g. workers where consistent with relevant public health
quarantine, COVID ward & direction
ICU staff
1
High risk settings include settings with an inability to isolate or where disease amplification is likely – such high-risk discharge destinations include residential aged care facilities (RACFs), crowded
or high-density housing, Aboriginal and Torres Strait Islander communities, correctional and detention facilities, homeless shelters and residential or crisis hostels.Table 3: Application of testing in hospitals during periods of high community transmission: emergency presentations 1,2,3,4
Clinical stability Indication for Home Additional considerations Test Test Disposition destination
admission environment result
risk
assessment6
Unstable10 with N/A N/A N/A RT-PCR (rapid) All Outcome of resuscitation, goals of care,
urgent interventions 5
RT-PCR result and home risk assessment where relevant,
indicated (e.g. determine disposition destination
intubation /
surgical/endoscopic
/ maternity) or
labour
Stable Emergency N/A N/A SARS-CoV-2 Positive Rapidly move to inpatient confirmed COVID ward
admission to diagnostic Negative Patient moved to:
hospital test9 - low-risk for COVID zone if asymptomatic and vaccinated;
indicated8 - at-risk for COVID zone if symptomatic or unvaccinated
All patients should remain appropriately isolated until : -
- where relevant, until released from quarantine, or
- RT-PCR is negative in patients with low pre-test probability
Emergency Low risk6 home Clinical and / or RT-PCR N/A • Home isolation until :
admission to environment epidemiologic risks for (standard) - where RT-PCR positive, release from isolation criteria are met,
hospital not COVID present or
indicated8 - where relevant, until released from quarantine, or
- where RT-PCR is negative and patients are symptom free
• Positive RT-PCR and / or close or secondary contacts followed
up by PHU
Clinical and / or No test7 N/A N/A
epidemiologic risks for
COVID absent
High risk6 home All RT-PCR (rapid) Positive Admit hospital or medi-hotel
environment 5
Negative Determined with public health / ID input based on risk
assessment
1
Emergency presentations are defined as presentations to the Emergency Department, unplanned presentations to walk-in services including maternity, mental health, oral health, or sexual health
services; note that where parents, carers or birthing support partners stay with a patient through their hospital admission they will be required to undergo COVID-19 testing, with the type of testdetermined by the pre-test probability, the community prevalence, turn-around time of available tests in the location of presentation and relevant public health directions. 2 Community transmission trigger determined by Chief Health Officer 3 This guidance should not replace clinical judgement individualised to the presentation and local modifying factors 4 Staff and patients in high community prevalence environments will be using PPE in accordance with Queensland Health PPE guidance for high risk levels 5 Rapid RT-PCR testing encompasses GeneXpert or Liat®; if rapid PCR testing modalities are unavailable, expedited standard RT-PCR may need to be substituted 6 High risk home assessment includes inability to isolate or identification of a high-risk discharge destination, where disease amplification is likely – such high-risk discharge destinations include residential aged care facilities (RACFs), crowded or high-density housing, Aboriginal and Torres Strait Islander communities, correctional and detention facilities, homeless shelters and residential or crisis hostels. 7 Assumes the ability to appropriately isolate the person, staff wear appropriate level of PPE consistent with Queensland Health PPE guidance and there is a rapid assessment and disposition – where these conditions are not able to be met consider rapid RT-PCR 8 Senior clinician input is required at point of triage 9 SARS-CoV-2 diagnostic test that is most appropriate will be determined by the pre-test probability, the community prevalence, turn-around time of available tests in the location of presentation and relevant public health directions. 10 Unstable includes unstable vital signs or acute severe behavioral disturbance unresponsive to verbal de-escalation and where sedation is indicated for patient or staff safety
Table 4: Application of testing in hospitals during periods of high community transmission: elective presentations 1,2,3,4
Presentation type Clinical screen Pre-presentation testing Test on day Test result Disposition destination
of
presentation
Elective admission RT-PCR (standard) within Positive Defer surgery where clinically appropriate.
• RT-PCR (rapid)5 if high
the 72 hours prior to Disposition determined by clinical risk
risk procedure or if no
presentation that is assessment:
available RT-PCR
negative – patients are admit to inpatient COVID ward or
(standard) results from
asked to self-isolate at discharge to outpatient COVID model or HITH
within the 72 hours prior
their place of residence Negative Admit and progress with elective procedure
to presentation
after testing and prior to
admission
Stable with no
Outpatient N/A Positive Disposition determined by clinical risk
epidemiological • RT-PCR (rapid)5 if aerosol
presentation6 assessment:
risks and no clinical generating procedure
admit to inpatient COVID ward or
features of COVID8 planned in OPD
discharge to outpatient COVID model or HITH
Negative Proceed with OPD assessment
Regular hospital N/A SARS-CoV-surveillance test 7
Positive Admit to COVID ward and proceed with
attendee more than - frequency individualised intervention / treatment if clinically
weekly for required appropriate
therapy e.g. oncology Negative Proceed with intervention / treatment
day patient or
hemodialysis patient
1
Elective presentations include any planned presentation for admission or outpatient review (medical, surgical, oral health, mental health, sexual health or maternity) or regular attendance
for required (e.g. dialysis / chemotherapy); note that where parents, carers or birthing support partners stay with a patient through their hospital admission they will be required to undergo
COVID-19 testing, with the type of test determined by the pre-test probability, the community prevalence, turn-around time of available tests in the location of presentation and relevant
public health directions.
2
Community transmission trigger determined by Chief Health Officer
3
This guidance should not replace clinical judgement individualised to the presentation and local modifying factors
4
Staff and patients in high community prevalence environments will be using PPE in accordance with Queensland Health PPE guidance for high risk levels
5
Rapid RT-PCR testing encompasses GeneXpert or Liat®; if rapid RT-PCR testing modalities are unavailable, expedited standard RT-PCR may need to be substituted
6
All outpatient episodes of care, where clinically appropriate, should be performed by telehealth
7
SARS-CoV-2 surveillance test refers to any of a standard RT-PCR, rapid RT-PCR or rapid Antigen test (if the latter is approved by relevant Public Health Direction) - where the latter is used, the
minimum recommended frequency of testing is twice weekly.
8
If clinical or epidemiologic features are present then the patient should be referred for urgent COVID RT-PCR testing with a decision on progression of planned treatment based on a clinical
risk assessment and ability to appropriately isolate and ensure safety of patients and staffInterpreting PCR results Positive Results All positive results are reported to Public Health Units by laboratories and through NOCS, the Public Health Notification Database. All persons with a positive result will be interviewed by the Heatlhdirect, with referral to one of three clinical pathways (primary care provider care, virtual care or Hospital in the Home). PHUs will receive information from the Healthdirect initial screening questionnaire and then interviewing will be undertaken by the relevant PHU for the purposes of contact tracing as appropriate. The case will remain in isolation until formally cleared by the Infectious Disease team. Repeating positive tests Any positive test from a GeneXpert require confirmatory NATA-approved RT-PCR testing. If the original test was from a Kirby Institute GeneXpert, the swab will need to be recollected to send to the reference laboratory. False Positives False positives are very rare but possible. All positive cases are assessed by the public health unit for symptoms, potential exposure to COVID virus and the prevalence of virus in the Queensland community and known transmission sites nationally. The Threshold cycle (Ct value) is also considered and if there are doubts about the validity of the test, it will be repeated on-site and then at FSS and further samples collected over the following days for repeat testing. Any positive and repeated tests should be discussed with the local Public Health Unit and pathology/microbiology department. Repeat testing will be supervised by a clinical microbiologist to assist with difficult and borderline results. Full instrument data will be made available to the microbiologist for consideration with escalation to rapid testing in a reference lab within hours. An Expert Advisory Group (MDT) may be held to make a consensus decision on whether the test represents a case or not. Negative Results All persons with symptoms should remain isolated until symptoms resolve. Any persons being tested for COVID-19 who is subject to quarantine must meet formal criteria for release from quarantine described in CDNA Public Health Unit guidelines AND must have received formal notification by the relevant public health unit of their clearance for release from quarantine. False Negatives False negative PCR results for COVID-19 can occur due to suboptimal specimen collection, testing occurring very early post-exposure, inappropriate specimen type, low viral load, low analytic sensitivity or variability in viral shedding (9). The incidence of false negative results may increase with increasing community prevalence. Where pre-test probability of COVID-19 is high (based on epidemiologic and clinical assessment), infectious diseases or public health physicians should be consulted about continued isolation and retesting.
Interpreting rapid antigen results
Accuracy of rapid antigen tests is variable – Pathology Queensland (PQ) has supported
progression of two rapid antigen tests, both requiring a nasal swab:
1. BD Veritor System for the Rapid Detection of SARS-CoV-2 – digital reader
2. PanBio COVID-19 Rapid Test Device (nasal) – manual read
The performance characteristics of these two tests were evaluated by PQ using 129 patients
who underwent both antigen testing and RT-PCR testing. 23 positive samples were collected,
14 from symptomatic patients (median symptoms duration 4 days) and the remaining being
asymptomatic. Evaluation identified:
• Both tests had high specificity (100%) with no false positives detected
• Comprehensive assessment of clinical sensitivity was limited by the small number of
COVID-19 positive cases in the evaluation. Positive performance agreement between
rapid antigen testing and RT-PCR was:
− 77% (95% CI 46-95%) for BD Veritor System –True Negatives 51, False negatives 3
(2 of 3 False negatives were asymptomatic)
− 80% (95% CI 44-97%) for PanBio – True negatives 54, false negatives 2
(1 of 2 False negatives were asymptomatic)
Caution is required when using rapid antigen tests to screen asymptomatic individuals or
those outside of disease phases associated with higher viral loads. Sensitivity of rapid
antigen tests may be improved by restricting use to high pre-test probability symptomatic
patients (10) and by use of serial testing every 3 days (11).
Implementation of point of care COVID testing
Implementation of point of care COVID testing needs to consider:
1. Allocation of appropriate resources at the point of testing to allow safe performance of
testing and ensure adequate observation and documentation of results
2. Performance of a risk assessment and appropriate planning of workflow for specimen
collection and testing to minimise infection control risks
3. Digital integration of results into existing data management systems to ensure accurate
data and appropriate patient follow-up
Isolation requirement
The SoNG: Coronavirus Disease 2019 (COVID-19). CDNA National guidelines for public health
units describes the recommendations for isolation requirements for testing strategies. The
following terms are used:
• the term ‘isolation’ is used to separate from the rest of the population, people who are
unwell with confirmed or suspected COVID-19 and restrict their movements until they
are no longer considered infectious to others
• the term quarantine is used to separate from the rest of the population, people who
are well but have been exposed (or potentially exposed) to COVID-19 and restrict their
movements during the disease’s incubation period (i.e. 14 days)All symptomatic persons should isolate whilst awaiting test results and remain isolated until: • they are well AND • their COVID test result is negative. The need for quarantine and testing during quarantine will be guided by the SoNG: Coronavirus Disease 2019 (COVID-19). CDNA National guidelines for public health units, public health and movement directions, and current State operational guidance instituted by the COVID Incident Management Team and public health units. Each case and cluster will be assessed, and advice provided on quarantine and testing to minimise ongoing COVID transmission. Communication of results All people tested will be advised about the result of their test and how they will be contacted. In low-case scenarios, people testing positive will be contacted by Healthdirect. As positive cases increase, SMS texts may be implemented for early notification of positive results including actions required by the patient. All people testing negative will be informed of their result. There are a number of options for how this might be delivered. Some HHSs have set up call centres, some fever clinics and pathology companies use SMS messages, GPs may deliver some results. Consideration should be given regarding how post-testing messaging is provided back to priority populations – e.g. checking whether the person has access to a phone or whether, with the person’s consent, the information can also be provided to a nominated person or support service. It is also important to ensure that those being tested are clear on what actions are required where the person tests negative – clear communication of need for ongoing isolation or quarantine is imperative for successful management of public health risks. Population Surveillance Sewerage testing Queensland Health has partnered with researchers from the University of Queensland and the CSIRO to deliver a wastewater surveillance program for SARS-CoV-2. The results from this program add to the information obtained through clinical testing. The test detects SARS-CoV- 2 genetic material. Detections may be related to a recovered case who is still shedding but is no longer infectious or may indicate that there is an infectious person living or visiting the area who has not yet been identified. A detection of SARS-CoV-2 in wastewater will be considered carefully alongside other information available to Queensland Health, such as recent known cases of COVID-19 in that area. Typically, an expert panel will be convened by the public health unit to evaluate the circumstances surrounding each detection of SARS-CoV-2 and advise on further measures if necessary. Updated wastewater test results can be located here.
Data collection
Irrespective of where swabs are tested (public or private laboratories), all test results will be
captured by the State-wide Public Health Database NOCS. COVID testing data from NOCS is
used by the COVID Incident Management Team (IMT) to assess testing rates across the
pandemic stages and across the HHS regions.
The Queensland Health State-wide COVID-19 Clinical Screening Assessment tool was developed
with the intent to enable Hospital and Health Services (HHSs) to appropriately assess people
presenting for COVID-19 screening in fever clinics. HHSs may be using this data to inform
ongoing service provision.
For expanded testing in outbreaks in high-risk settings, the Public Health Units will collect
data to monitor the progress of testing and further guide the management of the outbreak
response. Particularly for discrete Aboriginal communities and towns in surge testing this
intelligence can further inform ongoing testing to ensure good coverage of the community.
Ethical and Important considerations in COVID-19 testing
Under the Human Rights Act 2019 the Queensland Government recognises that all
Queenslanders have a right to health services and human rights must be considered in all
decision-making and action and only limit human rights in certain circumstances and after
careful consideration.
• All human life is equal, and all people should be able to access healthcare and live
with dignity, regardless of their age, disability, expected longevity or where they live.
• Decisions made about prioritising testing, should the system reach capacity, must be
based on a triage process that minimises possible bias.
• The rights of individuals must be balanced with consideration of the welfare and
wellbeing of others, particularly at a time when there can be severe consequences to
life if adequate infection control measures are unable to be fully realised.
• All testing is voluntary. Staff undertaking the testing must provide enough information
to enable people to give properly informed consent and balance their responsibility to
themselves, society and the healthcare teams.
• People in hotel or home quarantine and close or secondary contacts in quarantine
who refuse exit testing (typically conducted at day 10-12) will have their quarantine
period extended by 10 days.
• All people tested should be advised about the result of their test and how they will be
contacted. All people testing positive will be contacted by Healthdirect (and
potentially additionally their nearest Public Health Unit). All people testing negative
will be informed of their result. There are several options for how this might
be delivered. Some HHSs have set up call centres, some fever clinics and pathology
companies use SMS messages, GPs may order some results.5 Communications
All clinicians and members of the public or patients are advised to:
1. Regularly check contact tracing (exposure sites) for coronavirus and COVID-19 Public Health
Alerts
2. Regularly check the Chief Health Officer public health directions
3. Ensure that there is a shared understanding between the person being tested and the
clinician ordering the test of the actions a person is to take when they receive the test
result, with specific reference to need for ongoing isolation or quarantine (and how this
result will be communicated).
4. Ensure that the patient’s contact details are correct and that the proposed mechanism for
notification of test results is feasible for the individual patient’s circumstances.
The Chief Health Officer with advice from the State-wide COVID-19 Incident Management team will
lead communication on moving between community-risk levels and testing categories. Both the
Commonwealth and State Departments of Health have communication packages. Each HHS will
have communications plans in place. In the rural, remote regions and First Nations communities
using Councils, Mayors and Primary Health Networks, and well-known Indigenous Health leaders
may be useful.
A key priority is to ensure that those that are directly affected by an outbreak, i.e. those that are
living or working in a congregate setting are informed as early as possible and preferable before
or at least at the same time as the wider community. Caution also needs to be exercised so as not
to inadvertently blame or victimise any group or reinforce pre-existing stereotypes particularly for
those that are living in congregate settings many of whom may already socially and economically
disadvantaged.
It is also important to ensure that the messages and the communication method is tailored to
those living in congregate settings as there may be a large variation in age, educational status,
cognitive ability. There should be consideration of working with people who have experienced
trauma and appropriate communication strategies in place to assist staff to support people living
in these congregate settings.
Figure 2 outlines key internal stakeholder communication pathways during outbreaks. Outbreaks
in specific population groups or residential settings have additional reporting requirements that
are addressed in the specific population sections.
The needs of stakeholders for information are outlined in table 5.Figure 2: Overview of communication pathways during surge testing periods* *Note: when case numbers reach a threshold where notification by PHU is no longer feasible, automated NOCS notifications may be implemented
Table 5: Stakeholder communication needs
Stakeholder Information Required Responsible Party and Method
Priority populations Accessible, easy-read resources: Queensland Health developed – Factsheets, videos, transcripts, easy-read
− requirement for testing (if meet case criteria) translations
− reason for testing Test results from pathology to person and/or nominee
− process/procedure for testing – where and how to get tested if experience challenges with access
− requirements re what occurs pending test results (isolation)
− test results
− translated into languages specific to the needs of CALD communities in Queensland
Residents congregate living settings Accessible, easy-read resources: Queensland Health developed – Factsheets, videos, transcripts, easy-read
− requirement for testing (if meet case criteria or if confirmed or suspected case in the accommodation) translations
− reason for testing Congregate living service provider – direct to client
Test results from pathology to person and/or nominee
− process/procedure for testing – where and how to get tested if experience challenges with access Commonwealth Department of Health communications where congregate living
− requirements re what occurs pending test results (isolation) settings are under Commonwealth regulation
− test results
Staff/Volunteers Requirement for testing (if meet case criteria or if confirmed or suspected case in the facility) Operator or Service Provider – direct to staff
Reason for testing Queensland Health – factsheets
Promote understanding of their role in testing Test results from pathology to staff/volunteer
Process/procedure for testing Commonwealth Department of Health communications where congregate living
Requirements re what occurs pending test results (isolation) settings are under Commonwealth regulation
Test Results
Visitors including Requirement for testing (if meet case criteria or if confirmed/suspected case in the facility or close contact) Provider – direct to visitor/contractor/support provider
GPs/Contractors/Support Providers Reason for testing Queensland Health – factsheets
Process/procedure for testing Test results from pathology to visitor/contractor/support provider
When to order tests for residents (GPs only)
Requirements re what occurs pending test results (isolation)
Test Results
Public Health Unit Test request and results in accordance with relevant legislation Pathology to inform – note this may be automated where case numbers are high
PHU will contact case and obtain details of contacts and issue quarantine directions. PHUs may need to contact support services
to identify and speak with contacts.
Public/Media Number of tests Department of Health via media units
Public Health Direction updates
Services where there are active cases
Community leaders / Number of tests Department of Health
Peak Organisations/Advocacy Groups Services where there are active cases
Information for distribution to community / sector
Department of Communities, Housing Liaison re outbreaks and suspected outbreaks in congregate living accommodation Local Public Health Unit/ Department of Health
and Digital Economy
Department of Seniors, Disability Liaison re outbreaks and suspected outbreaks in retirement villages, disability accommodation services, Aboriginal and Torres Department of Health
Services and Aboriginal and Torres Strait Islander communities
Strait Islander partnerships
Queensland Corrective Services Liaison re outbreaks and suspected outbreaks in correctional services Local Public Health Unit/ Department of Health
NDIS Quality and Safeguards Services where there are active cases in disability accommodation Department of Health
Commission
Commonwealth Department of Health Number of tests Department of Health / SHECC
Services / communities where there are active cases
Requirements for activation of Commonwealth response
Public guardian Outbreaks or cases involving persons with impaired decision-making capacity Department of Health for outbreaks / clinicians for individual patientsYou can also read