COVID-19-related smell and taste disorders: A guide for nurses
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

ZAY NYI NYI /SHUTTERSTOCK
COVID-19-related smell and
taste disorders:
A guide for nurses
BY LEASHA LINDSAY, MSN, RN, ANP
Abstract: Olfactory impairment is COVID-19 is a potentially deadly Diminished smell sensitivity sig-
recognized as a hallmark of COVID-19. This respiratory disorder caused by the nificantly compromises a patient’s
article highlights dysfunction of smell and SARS-CoV-2 virus. Among many safety because it makes detecting toxic
taste associated with COVID-19 and other clinical manifestations, agents, smoke, and spoiled food more
discusses implications for nursing practice.
COVID-19 can cause sensory challenging. Losing the ability to smell
dysfunction such as loss of smell and taste can also directly influence
Keywords: ageusia, anosmia, COVID-19,
dysgeusia, olfactory disorders, smell
(anosmia) and taste abnormali- a person’s ability to select and enjoy
disorders, taste disorders ties (dysgeusia).1-6 These can be food, which may impact nutritional
challenging to recognize and intake and social interactions.6
manage because they may mimic Olfactory impairment is recognized
other olfactory and gustatory as a hallmark of COVID-19 and may
disorders. be a predictor of clinical outcome.5
50 l Nursing2021 l Volume 51, Number 4 www.Nursing2021.com
Copyright © 2021 Wolters Kluwer Health, Inc. All rights reserved.
home-quarantined participants, such used standardized questionnaires
A glossary of terms13,14 as younger people and females.7,8 and telephone follow-up to measure
Smell disorders Non-Hispanic Black Americans mood and anxiety levels at enroll-
• anosmia: inability to smell with a history of cardiovascular dis- ment and for the participants’ base-
• dysosmia: altered smell perception ease and those who consumed more line, pre-COVID-19 state. Along
• hyposmia: decreased ability to smell than four alcoholic drinks per day had with mood and anxiety levels, they
• normosmia: normal ability to smell. a higher prevalence of taste impair- assessed severity of smell loss, loss of
Taste disorders ment in another study.7 Only ethnicity, taste, nasal obstruction, rhinorrhea/
• ageusia: complete loss of taste heavy alcohol consumption, and his- mucus production, fever, cough, and
• dysageusia: distorted taste tory of cardiovascular disease were shortness of breath (SOB). They
perception associated with a higher prevalence of found that despite the presence of
• hypogeusia: reduced ability to taste. taste dysfunction among patients in such signs and symptoms as SOB,
this study. Factors significantly associ- only the loss of smell and taste were
This article highlights olfactory and ated with smell dysfunction were age, associated with depressed mood and
gustatory dysfunction associated with gender, ethnicity, educational attain- anxiety. They hypothesize that emo-
COVID-19 and discusses implica- ment, family income, light-to-moderate tional disturbance may be a central
tions for nursing practice. To review alcohol consumption, and history of nervous system manifestation of
terminology associated with these asthma or cancer. Other researchers COVID-19 related to trans-olfactory
disorders, see A glossary of terms. have found that ageusia and anosmia tract penetration of the central ner-
in patients diagnosed with COVID-19 vous system by coronaviruses.3
Incidence and prevalence are not related to rhinitis or nasal ob- Currently, the relationship be-
Emerging evidence shows that olfac- struction symptoms.4 tween COVID-19 and the develop-
tory impairment is highly prevalent A prospective, cross-sectional ment of taste disorders is not well
among patients with COVID-19.5 A study was conducted to investigate understood.4 However, alterations to
study that surveyed 355 patients depressed mood, anxiety, and associ- the sense of smell are believed to be
with lab-confirmed COVID-19 found ated disease characteristics in pa- associated with direct injury to tis-
that the overall population preva- tients with COVID-19.3 Researchers sue in the olfactory system, such as
lence of both smell/taste loss or one
of the two disorders was 70%. Most
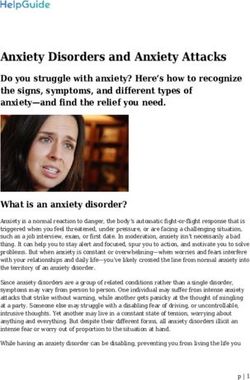
patients who reported a complete On the nose16
loss fully recovered after 14 days
Superior nasal concha
(median recovery time, 10 days).1
In a retrospective review of patients Middle nasal
with lab-confirmed COVID-19 pre- concha
senting to a San Diego hospital, re-
searchers analyzed olfactory and gusta-
tory data available for 128 patients.5 Inferior nasal
They found that hospital admission for Internal concha
COVID-19 was associated with intact nares
sense of smell and taste, increased age,
diabetes, and parameters associated
with respiratory failure. In contrast,
anosmia was strongly and indepen- Eustachian
dently associated with outpatient care. tube opening
The authors concluded that anosmia External
may be associated with a milder nares
course of disease and that normosmia
(subjectively perceived normal olfac-
tory function) is an independent pre-
dictor of hospital admission in patients
with COVID-19. Other research has Esophagus Soft palate Hard palate
found that both olfactory and gusta-
tory dysfunction are more prevalent in
www.Nursing2021.com April l Nursing2021 l 51
Copyright © 2021 Wolters Kluwer Health, Inc. All rights reserved.the olfactory epithelium (see On the regions throughout the mouth and Nursing considerations
nose).4 The virus also seems to cause throat. All regions are independently When taking a patient’s health his-
an inflammatory response in the na- tested with each taste solution, and tory, nurses can use OLDCART (onset,
sal cavity that temporarily obstructs the patient is asked to describe taste location, duration, characteristics,
odorants from reaching olfactory quality and intensity. aggravating/associated factors,
receptor neurons. Other factors be- • the flavor discrimination test, which relieving factors, and treatment)
sides COVID-19, such as advancing is used to evaluate the combination to assess loss of smell or taste. For
age and certain medications, may of taste and smell sensation. example, the nurse should ask ques-
contribute to olfactory disorders.9 Although diagnostic testing is not tions such as: When did the patient
recommended for patients with first notice the loss of taste and/or
Assessment and treatment COVID-19 presenting with loss of taste smell? What was the duration of the
The University of Pennsylvania Smell or smell, some tests may be useful loss (days, weeks, months, or years)?
Identification Test (UPSIT) is a well- when ruling out other sensory disorders. What is the patient not able to taste:
validated tool that tests a person’s Additional sensory dysfunction assess- salt, sour, bitter, or sweet? Is the
ability to detect odors.2 Forty differ- ments may include cognitive testing, loss of taste or smell partial or com-
ent odors are released by scratching a nasal endoscopy, brain MRI, and com- plete? What relieves or aggravates
panel of microencapsulated “scratch puted tomography of the sinuses or the presenting signs and symptoms?
and sniff” odorants. For each of the nose. If nasal obstruction is suspected, Does the patient have any other
40 odors, the patient chooses an an- the patient should be referred to a neuro- symptoms?
swer from four possible options; only physiologist for more diagnostic studies. Nurses should also obtain a de-
one answer is correct. Test results are Vaira and colleagues recommend tailed medication history to assess for
scored out of 40, with higher scores that practitioners perform olfactory drugs that can affect smell and taste.14
denoting better olfaction. The valid- function tests in routine workups for Examples include antimicrobial agents
ity and reliability of the UPSIT have patients presenting with COVID-19.4 such as amoxicillin and azithromycin,
been reported in the literature.2 The In addition, the American Academy antipyretic drugs such as aspirin and
test-retest reliability is excellent.10 of Otolaryngology–Head and Neck acetaminophen, and antihistamines.10
In one study, the UPSIT was admin- Surgery encourages clinicians world- Antiallergenic agents such as lorata-
istered to 60 patients with confirmed wide to report COVID-19-related dine or prednisone and antihyperten-
COVID-19 and 60 uninfected control olfactory dysfunction to add to the sive drugs such as amlodipine and
subjects matched by age and gender.2 accumulating body of anecdotal evi- diltiazem may also cause gustatory or
Fifty-nine patients in the test group dence about this complication (see olfactory dysfunction.14
exhibited some degree of smell dys- Reporting COVID-19-related anosmia).12 Nurses need to perform a compre-
function; 35 of them either had severe Research has identified various hensive physical assessment for pa-
dysfunction or had lost the sense of potential treatments for olfactory tients diagnosed with loss of taste and
smell entirely. Deficits were evident for impairments; for example, acu- smell to determine if they have any
all 40 UPSIT odorants tested. puncture, theophylline, minocy- associated unexplained neurologic
Many tools are available to assess cline, vitamins, lipoic acid, and signs and symptoms. A complete
taste disorders, including:11 zinc.13,14 However, evidence sup- neurologic assessment includes test-
• the whole mouth taste test, which porting the effectiveness of these ing cranial nerve (CN) function to
tests the patient’s ability to detect, therapies is lacking. Nurses can in- help identify dysfunction and rule
identify, and rate the intensity of var- form patients that COVID-related out other disorders that can affect the
ious concentrations of sweet, sour, loss of smell and taste often re- patient’s ability to taste and smell. For
salty, and bitter taste solutions. solves spontaneously within 2 example, CN 1 olfactory function can
• spatial testing, used to evaluate the weeks of the initial onset of be tested by occluding one nostril
patient’s ability to taste in taste bud COVID-19 signs and symptoms.1 and placing a common scent, such as
coffee or peppermint, under the other
nostril. CN VII, IX, and X contribute
Reporting COVID-19-related anosmia12 to the patient’s ability to perceive
The American Academy of Otolaryngology–Head and Neck Surgery has created a salty, sweet, sour, and bitter tastes.15
COVID-19 Anosmia Reporting Tool to collect information about COVID-19-related
anosmia and dysgeusia worldwide. Patients and healthcare professionals alike Patient education
are invited to submit data. The confidential questionnaire is available at: www.
Anosmia and dysgeusia can directly
entnet.org/content/reporting-tool-patients-anosmia-related-covid-19.
influence a patient’s quality of life,
52 l Nursing2021 l Volume 51, Number 4 www.Nursing2021.com
Copyright © 2021 Wolters Kluwer Health, Inc. All rights reserved.diminishing appetite and interfering 2. Moein ST, Hashemian SM, Mansourafshar B, 10. Holbrook EH. Disorders of taste and smell.
Khorram-Tousi A, Tabarsi P, Doty RL. Smell Medscape. 2021. https://emedicine.medscape.com/
with eating and drinking. Nutritional dysfunction: a biomarker for COVID-19. Int Forum article/861242-overview#a4.
intake may be inadequate as a result. Allergy Rhinol. 2020;10(8):944-950. 11. Lafreniere D. Evaluation and treatment of
Nurses need to assess patients with 3. Speth MM, Singer-Cornelius T, Oberle M, taste and smell disorders. UpToDate. 2020. www.
Gengler I, Brockmeier SJ, Sedaghat AR. Mood, uptodate.com.
COVID-19 for anosmia and dysgeu- anxiety and olfactory dysfunction in COVID-19:
12. American Academy of Otolaryngology–Head
sia and counsel those at risk for de- evidence of central nervous system involvement?
and Neck Surgery. COVID-19 anosmia reporting
Laryngoscope. 2020;130(11):2520-2525.
veloping taste or smell alterations tool. www.entnet.org/content/reporting-tool-
4. Vaira LA, Salzano G, Fois AG, Piombino P, patients-anosmia-related-covid-19.
about such hazards as exposure to De Riu G. Potential pathogenesis of ageusia and
13. Goncalves S, Goldstein BJ. Pathophysiology of
anosmia in COVID-19 patients. Int Forum Allergy
smoke, natural gas, and spoiled Rhinol. 2020;10(9):1103-1104.
olfactory disorders and potential treatment strategies.
foods. Nurses should also assess pa- Curr Otorhinolaryngol Rep. 2016;4(2):115-121.
5. Yan CH, Faraji F, Prajapati DP, Ostrander BT,
14. Schiffman SS. Influence of medications on taste
tients’ dietary habits, food prefer- DeConde AS. Self-reported olfactory loss associates
and smell. World J Otorhinolaryngol Head Neck Surg.
with outpatient clinical course in COVID-19.
ences, and food choices when man- Int Forum Allergy Rhinol. 2020;10(7):821-831. 2018;4(1):84-91.
aging anosmia and dysgeusia. With 6. Doty RL. Olfactory dysfunction and its measurement 15. Gibbons JR, Sadiq NM. Neuroanatomy, neural
in the clinic. World J Otorhinolaryngol Head Neck Surg. taste pathway. StatPearls [Internet]. 2020. www.
appropriate interventions and patient 2015;1(1):28-33. ncbi.nlm.nih.gov/books/NBK545236.
teaching, nurses can help rule out 7. Liu G, Zong G, Doty RL, Sun Q. Prevalence 16. Anderson MK. Foundations of Athletic Training.
other disorders that may impair the and risk factors of taste and smell impairment 5th ed. Philadelphia, PA: Wolters Kluwer Health/
in a nationwide representative sample of the US Lippincott Williams & Wilkins; 2012.
sense of smell or taste and optimize population: a cross-sectional study. BMJ Open.
patient outcomes. ■ 2016;6(11):e013246.
Leasha Lindsay is an assistant professor at Borough
8. Paderno A, Schreiber A, Grammatica A, et al. of Manhattan Community College in New York, N.Y.
Smell and taste alterations in COVID-19: a cross-
REFERENCES sectional analysis of different cohorts. Int Forum
Allergy Rhinol. 2020;10(8):955-962. The author has disclosed no financial relationships
1. Dell’Era V, Farri F, Garzaro G, Gatto M, Aluffi related to this article.
Valletti P, Garzaro M. Smell and taste disorders 9. Jia C, Hegg CC. Effect of IP3R3 and NPY on age-
during COVID-19 outbreak: cross-sectional study related declines in olfactory stem cell proliferation.
on 355 patients. Head Neck. 2020;42(7):1591-1596. Neurobiol Aging. 2015;36(2):1045-1056. DOI-10.1097/01.NURSE.0000736920.83024.0e
www.Nursing2021.com April l Nursing2021 l 53
Copyright © 2021 Wolters Kluwer Health, Inc. All rights reserved.You can also read