Corporate Presentation - February 2022 - Trevi Therapeutics
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Corporate Presentation
February 2022
Forward Looking Statement Disclaimer
Statements contained in this presentation and oral statements made regarding the subject of this presentation that are not matters of historical facts are
“forward-looking statements” within the meaning of the Private Securities Litigation Reform Act of 1995. Such statements are subject to risks and uncertainties
and actual results may differ materially from those expressed or implied by such forward-looking statements. Such statements include, but are not limited to,
the expected timing of reporting full data from Trevi’s Phase 2 CANAL trial of Haduvio in IPF patients with chronic cough; Trevi’s business plans and objectives,
including future plans or expectations for Trevi’s product candidates; and other statements containing the words “believes,” “anticipates,” “plans,” “expects,”
and similar expressions. Risks that contribute to the uncertain nature of the forward-looking statements include: uncertainties regarding the success, cost and
timing of Trevi’s product candidate development activities and ongoing and planned clinical trials; uncertainties regarding the scope, timing and severity of the
COVID-19 pandemic, the impact of the COVID-19 pandemic on Trevi’s clinical operations and actions taken in response to the pandemic; uncertainties regarding
Trevi’s ability to execute on its strategy; the risk that interim results from a clinical trial may not necessarily be predictive of the results of the completed trial or
other future or ongoing clinical trials; potential regulatory developments in the United States and foreign countries; uncertainties inherent in estimating Trevi’s
cash runway, future expenses and other financial results; including Trevi’s ability to continue as a going concern, comply with its obligations under its loan facility
and fund future operations; as well as other risks and uncertainties set forth in the quarterly report on Form 10-Q for the quarter ended September 30,
2021 filed with the Securities and Exchange Commission and in subsequent filings with the Securities and Exchange Commission. All forward-looking
statements contained in this presentation and oral statements made speak only as of the date on which they were made. Trevi undertakes no obligation to
update such statements to reflect events that occur or circumstances that exist after the date on which they were made.
This presentation includes statistical and other industry and market data that we obtained from industry publications and research, surveys and studies
conducted by third parties as well as our own estimates of potential market opportunities. Industry publications and third-party research, surveys and studies
generally indicate that their information has been obtained from sources believed to be reliable, although they do not guarantee the accuracy or completeness
of such information. We believe that these third-party sources and estimates are reliable but have not independently verified them. Our estimates of the
potential market opportunities for our product candidates include several key assumptions based on our industry knowledge, industry publications, third-party
research and other surveys, which may be based on a small sample size and may fail to accurately reflect market opportunities. While we believe that our
internal assumptions are reasonable, no independent source has verified such assumptions. The industry in which we operate is subject to a high degree of
uncertainty and risk due to a variety of important factors that could cause results to differ materially from those expressed in the estimates made by third
parties and by us.
2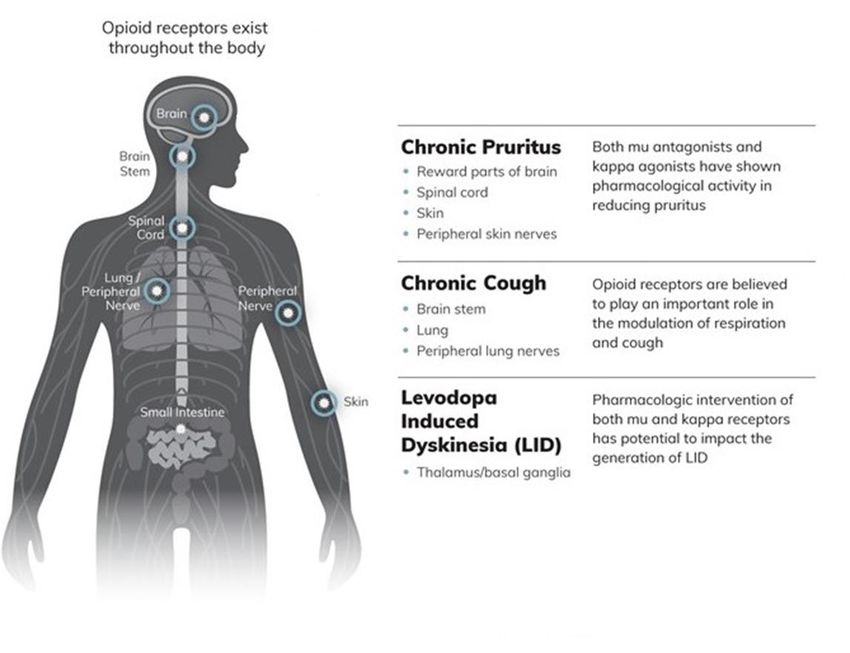
HADUVIO™ (nalbuphine ER) Advancing Two Lead Clinical Programs
Chronic Cough in Idiopathic Pulmonary Fibrosis Pruritus Associated with Prurigo Nodularis1
Phase 1 2 3 Filed Phase 1 2 3 Filed
Chronic Cough in IPF Pruritus in PN
• Phase 2 proof-of-concept trial • Completed enrollment January 31, 2022
• Announced positive result from planned interim • Data expected in 2Q 2022
analysis (p
Attractive Categories for Lead Indications
Chronic Cough in Idiopathic Pruritus Associated with Prurigo
Pulmonary Fibrosis Nodularis
✓
• No approved therapies
✓•• No approved therapies
✓
• No oral option available
✓ No oral option available
✓
• High unmet need
✓• High unmet need
✓
• IPF is a life-threatening, debilitating
disease 4
✓• PN is a serious, potentially
debilitating, chronic skin condition 2,3
Dermatologist View on PN Impact on QoL4
Most Bothersome Daily IPF Symptom1 (N=126)
% of patients that experience
symptom on a daily basis
60%
% of Respondents
60% 60% 67%
40% 50% 50%
40%
33%
20% 20%
1%
0% 0%
Shortness Cough Fatigue 1-2 3-5 6-7
of Breath 1=no impact at all, 7=very significant impact
1Voice of the Patient – IPF Patient-focused Drug Development Initiative, 2015 2Iking A JEADV 2013 3Vaidya DC & Schwartz RA Acta Derm Croat 2008 4Trevi data on file 4
Broad Applications for Mechanism of Action of HADUVIO™
Haduvio™ (nalbuphine ER) is an investigational drug 5
Chronic Cough in
Idiopathic Pulmonary
Fibrosis (IPF)
Nalbuphine ER Demonstrated Highly Statistically Significant Reduction of Chronic
Cough In Idiopathic Pulmonary Fibrosis (IPF) From Ph2 Interim Analysis
Nalbuphine ER demonstrated a highly significant and consistent reduction in chronic
cough associated with IPF in an interim analysis
• 52% placebo-adjusted reduction in the geometric mean percent change from study baseline for
nalbuphine ER in daytime cough frequency to day 22 of treatment (p
Opportunity to be First in Class for Chronic Cough in Idiopathic Pulmonary
Fibrosis
Current IPF Prevalence
U.S. 130k1,2 ≥75%
of IPF patients report cough as being one
WW 1M+3 of their most significant symptoms5
~85% 4
of IPF patients suffer from chronic cough
There are no approved therapies for IPF chronic cough
Current IPF therapies (anti-fibrotics), which have not been
shown to reverse disease progression, are not labeled to
reduce cough frequency/severity
1Raghu G et al. Eur Resp J 2016 2Raghu G et al. Am J Resp Care Med 2006 3Nalsnyk L et al. Eur Resp Rev 2012 4Ryerson CJ et al. Respirology 2011 5Voice of the Patient – IPF Patient-focused Drug Development
Initiative, 2015
8
The Significant Role of Chronic Cough in IPF
226-520
Median coughs per day of an IPF patient.1,2
Marker of Disease
Cough may be an early clinical marker of disease activity, identify patients at high risk of progression,
The urge to cough cannot be relieved by
and may predict time to death or lung transplantation.4
coughing.3
Refractory Profibrotic Social
Frequently refractory to antitussive therapy.5
One could hypothesize that cough is not only a symptom but
may also contribute to enhanced activation of profibrotic
mechanisms and disease worsening in IPF.6
Interruption
The social impact of chronic cough in IPF further compounds
limited exercise ability, reduced walking distance and the need
to use supplemental oxygen.3,7
Impacts Daily Function
Coughing can increase feelings of anxiety as it induces breathlessness. Coughing spells or episodes
lead to significant fatigue, air hunger, peripheral oxygen desaturation and some patients also experience
cough-related urinary incontinence8,9,10
1KeyAL et al. Cough 2010 2VanManen M et al. Am J Respir Crit Care Med 2015 3Swigris JJ et al. Health Qual Life Outcomes 2005 4Ryerson CJ et al. Resp 2011 5Hope-Gill BDM et al. Am J Respir Crit Care Med
2003 6VanManen M et al. ERS 2016 7Key AL et al. Cough 2010 8vanManen M et al. Ther Adv Respir Dis 2017 9Wakwaya Y et al. Chest 2021 10Bradia F et al. Rev Mal Respir 2009
9
How Patients and Caregivers Describe Cough’s Impact on Daily Life
Laughing, and that's a [My cough] comes with
very serious thing, because if you exertion … walking up a flight of
On my worst days, coughing will
have two boys who are very stairs … putting your clothes on,
wipe you out for an entire day …
funny, you can't laugh, because bending over and tying your
Physically, you're exhausted.
then you start to cough, so they shoes, fixing something in the
don't tell jokes anymore. kitchen, moving around.
There's an isolation
I also remember my His cough was often
component to it. He could clear a
cough was really so deep that it debilitating. He would have what
crowd. We were in line to go to
he called coughing fits, and when
felt like I broke my ribs, and my the Red Sox games for the World
he would have such violent
ribs became so cramped that I Series, and the look that people
coughs that he couldn't catch his
couldn't even twist, so it caused a gave him for coughing, that --
breath, then he would have to
problem driving. thinking that he was, you know, a
calm himself afterwards.
contagious person.
Voice of the Patient – IPF Patient-focused Drug Development Initiative, 2015 10CANAL Phase 2 Trial Design
Randomized, Double-Blind, Placebo-Controlled, Two Treatment Period Crossover
Treatment Treatment PRIMARY ENDPOINT
Period 1 Period 2 Geometric mean percent change in
Randomization
nalbuphine ER BID Placebo daytime cough frequency from baseline
(Day 1 – Day 22) 2-week
(Day 1 – Day 22) as measured by a digital cough monitor
washout
period /
2-week
follow-up
(VitaloJAK®) between the nalbuphine ER
treatment
Placebo crossover nalbuphine ER BID and placebo treatments
(Day 1 – Day 22) (Day 1 – Day 22)
SECONDARY ENDPOINTS
Daily Patient Reported Outcomes (eDiary)
Cough severity
Fatigue
VitaloJAK Dyspnea
Readings
Day -1 Day 22 Day -1 Day 22 NALBUPHINE ER
Study Treatment Treatment Treatment Oral tablet dosed BID
Baseline/ Period 1 Period 2 Period 2
Treatment Ends Baseline Ends
Titrated to 162mg over the active
Period 1 treatment period
Baseline
www.clinicaltrials.gov: NCT04030026 11
Nalbuphine ER is an investigational drugCANAL Interim Analysis Patient Disposition
Data Cut-off: 28 JAN 2022
Screened
N=45
(2) Active In Screening (4%)
(11) Screen Failed (24%)
Randomized / Enrolled
N=32
(3) Active In Treatment Period 1 (9%)
(1) Discontinued due to COVID (3%)
(2) Discontinued (6%)
• (1) AE
• (1) Protocol Violation
End of Treatment Period 1
Full Analysis Set
N=26 (2) Active In Treatment Period 2 (8%)
(2) Discontinued due to COVID (8%)
(4) Discontinued (15%)
• (4) AE
Completers
N=18
12CANAL Trial Interim Analysis Baseline Characteristics
Completers
Full Analysis Set (Subjects Completing Both
Treatment Periods)
Number of subjects, n 26 18
Male, n (%) 22 (84.6%) 14 (77.8%)
Age (years), mean 72 71
Daytime cough frequency
(coughs/hour):
Mean 31 31
Median 20.6 22.4
Min-Max 3.18 - 92.35 3.18 - 77.18
Nalbuphine ER is an investigational drug 13Primary Efficacy Endpoint Achieved Statistically Significant Reduction in Cough
Frequency with Nalbuphine ER
Primary Endpoint (N=26)
Statistically significant reduction in primary Geometric Mean Change from Study Baseline in
endpoint (100% conditional power, pBaseline Cough Severity
Nalbuphine ER Effect Consistent Across Baseline Cough Severity
Mean Change from Study Baseline in Daytime Coughs per
Magnitude of nalbuphine ER Hour
treatment effect remains consistent 0%
across a variety of baseline cough
-16%
Percent change in coughs/hr from study baseline
counts based on increasing severity
-20% -24% -24%
Treatment effect with nalbuphine
ER independent of baseline cough -40%
count and supports potential
efficacy across a broad patient -60% -68%
population in IPF -74% -72%
-80%
52% PBO Adj Chg. 50% PBO Adj Chg. 48% PBO Adj Chg.
-100%
All coughs/hr >10 cough/hr >20.5 coughs/hr (50% ITT)
Baseline coughs/hr 31 Baseline coughs/hr 37 Baseline coughs/hr 50
N=26 N=21 N=13
Nalbuphine ER Placebo
Endpoint calculated as arithmetic mean percent change in daytime cough frequency from study baseline 15
Nalbuphine ER is an investigational drugAnalysis by Treatment Period Baseline
Treatment Effect Magnitude Remains Consistent
Mean Change from Treatment Period Baseline in Daytime
Use of treatment period baseline Coughs per Hour (N=26)
demonstrates a 78% placebo 40%
adjusted improvement compared to
Percent change in coughs/hr from study baseline
52% for study baseline 20% 12%
4% -1%
0%
Cough improvement is independent
of the baseline used for analysis -20%
(treatment period baseline vs.
study baseline) and independent of -40%
baseline cough count -66%
-60%
-72% -71%
-80%
78% PBO Adj Chg. 76% PBO Adj Chg. 70% PBO Adj Chg.
-100%
All coughs/hr >10 coughs/hr >20.5 coughs/hr (50% ITT)
Baseline coughs/hr 31 Baseline coughs/hr 37 Baseline coughs/hr 50
N=26 N=21 N=13
Nalbuphine ER Placebo
Endpoint calculated as arithmetic mean percent change in daytime cough frequency from treatment baseline 16
Nalbuphine ER is an investigational drugResponder Analyses
Clear Separation Between Nalbuphine ER vs. Placebo at All Levels
Assessed the magnitude of Percent of Responders Achieving Mean Change from
response by defining the Study Baseline Thresholds (N=26)
percentage of reduction achieved 80%
by treatment response categories 70% 65%
ranged from 30% to 75%
improvement
58%
Percent of Responders
60%
50%
Nalbuphine ER outperforms 42%
placebo in each analysis 40%
38%
42% of nalbuphine ER treated
30%
23%
subjects obtained a 75% reduction 20%
in their cough counts compared to
10%
0% of placebo treated patients
0%
0%
-30% -50% -75%
Change from Study Baseline Thresholds
Nalbuphine ER Placebo
Endpoint calculated as arithmetic mean percent change in daytime cough frequency from study baseline 17
Nalbuphine ER is an investigational drugPatient Reported Outcome Measures Corroborate the Daytime Cough
Frequency Results Measured by the Independent Cough Monitor
Objective cough frequency Objective and Patient Reported Outcome Measures
• Measured via digital cough Mean Change vs. Study Baseline (N=26)
monitor (VitaloJAK®) 25 2.5
2.0
EXACT PRO Mean Change vs. Study Baseline
VitaloJAK Mean Change vs. Study Baseline
20 2
Patient Reported Outcome 15
1.4 1.5
Measures 10 1
• EXACT (scale 0-56): measures
5 0.5
cough, breathlessness, 0.0
0 0
dyspnea, and other measures
-5 -0.2 -0.5
• EXACT2 (scale 0-4): measures
-10 -1
cough frequency -8.3
-1.0
• EXACT7-11 (scale 0-20): -15
-1.4
-1.5
measures breathlessness and -20 -2
dyspnea -25 -23.1 -2.5
-30 -3
VitaloJAK EXACT EXACT2 EXACT7-11
Baseline 31 Baseline 17 Baseline 2 Baseline 7
Nalbuphine ER Placebo
Mean change in daytime cough frequency and PRO scales from study baseline 18
Bacci EM et al. Respiratory Medicine 2018, doi.org/10.1016/j.rmed.2017.11.011
Nalbuphine ER is an investigational drugNalbuphine ER Safety Summary
• CANAL Safety:
• DSMB continues to oversee safety in keeping with DSMB Charter
• No safety concerns have been raised by the DSMB overseeing the conduct of the study
• No reported deaths and 1 reported Serious Adverse Event not considered treatment related
• 5 AEs have resulted in discontinuation (16%):
• 1 anorexia, 1 depression, 1 nausea/vomiting, 1 insomnia/fatigue, 1 agitation/anxiety/dyspnea
• No new safety-related issues have arisen in the study and the adverse event profile
of the drug in the IPF subject population is consistent with the safety profile noted in
all other past studies where Nalbuphine ER has been investigated in a variety of
medical conditions
• Nalbuphine ER has been dosed in > 1,000 subjects
19Potential Market Opportunity Across a Broad Array of Chronic Cough
Conditions
Prosecuting patent applications that, if issued,
would provide protection through at least 2039
~$10B
Total
Potential
Refractory Chronic Addressable
Cough / Unexplained COPD Market
Emphysema 20271
Chronic Cough
Refractory Chronic
Chronic Bronchitis
Cough
GERD Heart Failure
Interstitial Lung Diseases
Idiopathic Non-specific Hyper-sensitivity
Bronchiectasis Asthma Lung Cancer
Interstitial Pneumonia Pneumonitis
Idiopathic Pulmonary Unclassified Idiopathic Autoimmune Interstitial Other ILDs (i.e. Post-Nasal Tobacco Smoke /
Fibrosis Interstitial Pneumonia Lung Disease sarcoidosis) Drip Usage
Therapeutic Areas Underlying Chronic Cough
Current Development Potential Future Development
20
12027 est. The Insight Partners Jun 2020 22028 est. VPA Research Idiopathic Pulmonary Fibrosis Report Feb 2021Clinical Development Next Steps—IPF Chronic Cough
• Complete the dosing of additional subjects randomized post interim data cut
• Initiate discussions with relevant health authorities on the next study and the
development program
• Finalize and report full study data with all subjects enrolled
• Prepare to initiate Phase 2b study
Nalbuphine ER is an investigational drug 21Chronic Pruritus in Prurigo Nodularis
Opportunity to be the First Oral Therapy Approved in Pruritus Associated with
Prurigo Nodularis
Current PN Prevalence Itch Trigger
1,2,3,4
U.S. 300k
Itchy Skin
5
WW 730k
• Current off-label treatments for itch lack efficacy and/or have an
unfavorable AE profile Nodules
= ITCH-SCRATCH Chronic
• We believe 40-50% of patients are uncontrolled on off-label More Itch CYCLE Scratching
therapies
• Oral therapy enables opportunity to be used in earlier lines of
therapy
• Many underlying etiologies of itch, but initial scratching may
create an itch-scratch cycle resulting from central and/or
peripheral nervous tissue changes6,7,8,9
1Huang
Bumps /
AH JID 2020 2Stander S JAAD 2020 3Iking A JEADV 2013 4Pereira M JEADV 2018 5Prurigo Nodularis - Market Insights,
Epidemiology and Market Forecast 6Eigelshoven CME Derm 2009 7Vaidya DC & Schwartz RA Acta Derm Croat 2008 8Lee MR, Nodules 23
Shumack S Aus J Derm 2005 9Iking A JEADV 2013Results from Ph2a Prurigo Nodularis Trial and Open Label Extension (OLE)
Continued Separation of WI-NRS Over Time Dose Response Supporting 162mg Selection†
1
All Patients (MITT/LOCF): N = 62 Completing Patients : N = 50
WI-NRS Change from Baseline 0.0
Score from Baseline
-0.5
Mean Δ in WI-NRS
8
-1.0
Placebo
7
WI-NRS
-1.5
-2.0 -1.75
6 -1.85
HADUVIO -2.5 -2.14
5 162mg BID -3.0 -2.51 -2.52
* * p=0.083
-3.5
4 -3.43
-4.0
0 1 2 3 4 5 6 7 8 9 10 p=0.025
Placebo Haduvio™ 81 mg BID Haduvio™ 162 mg BID
Weeks from Baseline *p≤0.025
Drug Separation vs. PBO (OLE) HADUVIOTM Showed Disease Improvements
PN Ph2a 50% Responder Analysis (N=63) Percent of Patients Achieving Outcomes on ≥6
WI-NRS (Blinded 10 weeks)
months of HADUVIOTM
p=0.028 100%
Months of HADUVIOTM
50% Responder Analysis
% Patients on ≥6
n=12
(Equiv. to a 4-point
60% p=0.083 50%
80%
n=18 60% 80%
analysis)
40% 33% 68%
n=22 n=20
40% 58%
18% 20%
20% 20%
0%
0%
MITT COMPLETERS
1 Improved Improved Improved
Placebo Haduvio™ 162 mg BID Lesions Excoriations/crusts ItchyQoL
†All
p-values compare treatment group to placebo. Only the primary endpoint [30% responder analysis] was powered for statistical significance.
1Post-hoc analysis on completers. Consists of the patients who completed the 10-week course of treatment. 24
DOI: 10.1111/jdv.17816
Nalbuphine ER is an investigational drugPhase 2b/3 PRISM Trial Design (N=~360)
Top-Line Data Expected 2Q 2022
Optimizations from Ph2a to Ph2b/3 PRISM Trial
Increased Powering Enriched Population Increased Duration
Focusing on severe population
63 patients (Ph2a) → 360 patients (Ph2b/3) 10 weeks (Ph2a) → 14 weeks (Ph2b/3)
WI-NRS ≥5 (Ph2a) → WI-NRS ≥7 (Ph2b/3)
Blinded
Screening Double-Blind Fixed Dose Comparison Open Label Extension
PRISM Titration Period
Period (2 weeks) (12 weeks) (up to 38 weeks)
Trial
Design HADUVIO HADUVIO 162 mg BID Open-Label HADUVIO
Placebo Placebo BID 162 mg BID
Randomization Primary Endpoint
Trial Status: Primary Efficacy Endpoint (responder analysis): Open Label Extension:
• 60+ Sites • % WI-NRS Responders for NAL-ER versus PBO • ~90% of subjects who reached Wk 14 have
• Completed enrollment January 31, 2022 • Responder = 4-point reduction from baseline at Wk 14 continued into the open label extension
• Long-term safety
Inclusion Criteria: Key Secondary Endpoints • Durability of effect
• Worst-Itch Numerical Rating Scale (WI-NRS) (change from baseline): • Lesion healing
Score ≥7 • QoL (ItchyQoL)
• 10+ pruriginous nodules • Skin lesions
• PN present on at least 2 separate body parts • Sleep disturbances
Nalbuphine ER is an investigational drug 25Potential Market Opportunity Across a Broad Array of Chronic Pruritic
Conditions
~$20B
Total Market
20261
Global Pruritus
Category
$20B1
Multiple Sclerosis
HIV Protease
PN Post Herpetic
Inhibitor Induced
$3.2B2 Pruritus
Pruritus
Chemotherapy Burn Induced
Hepatitis C
Induced Pruritus Pruritus
Cancer Related Brachioradial
Aquagenic Pruritus Chronic Cirrhosis
Pruritus Pruritus
Lichen Simplex Primary Sclerosing Hodgkin's
Atopic Dermatitis Psoriasis Psychiatric Causes
Chronicus Cholangitis Lymphoma
Primary Biliary Neuropathic
Uremic Pruritus Prurigo Nodularis Idiopathic Pruritus Urticaria Polycythemia Vera
Cholangitis Pruritus
Renal/ Pain/
Dermatology Hepatology Oncology
Dialysis Neurology
Therapeutic Areas Underlying Itch
Previous/Current Development Potential Future Development
26
12026 est. OG Analysis Global Pruritus Therapeutics Market 22031 est. DelveInsight Prurigo Nodularis Market Insight, Epidemiology, and Market Forecast May 20202022 Milestones—Key Data Readouts
Date Milestone
Jan 31, 2022 PRISM (Pruritus in PN Phase 2b/3) Completed Enrollment
Feb 24, 2022 CANAL (Cough in IPF Phase 2) Positive Interim Analysis Results
2Q 2022 PRISM Topline Data
Early 3Q 2022 CANAL Full Data
27Trevi Value Proposition
Dual acting MOA in clinical development that works both peripherally and centrally to
Rebalancing the
rebalance the kappa and mu receptors, both of which are important in mediating cough and
Cough/Itch Pathway pruritus
Strong Cough in IPF Chronic cough Ph2 interim analysis showed 52% placebo-adjusted reduction in daytime
Interim Results cough frequency (p≤0.0001)
Statistically significant pruritus reduction in uremic pruritus Ph2b/3 trial
Existing Pruritus Safety
Prurigo nodularis Ph2a WI-NRS reduction vs. placebo
& Efficacy Data Prurigo nodularis Ph2a open-label extension demonstrated disease improvement1
Broad Potential Use
Ability to utilize nalbuphine ER across a variety of therapeutic areas that experience cough
Across Therapeutics and itch
Areas
Near Term Data for Chronic cough in IPF Ph2 full data expected early 3Q 2022
Lead Indications Pruritus in PN Ph2b/3 topline data expected 2Q 2022
1Prurigo nodularis Ph2a open-label extension demonstrated disease improvement in patients on Nalbuphine ER ≥6 months 28You can also read