Consumption of alcoholic and non-alcoholic beverages: ELSA-Brasil results
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
DOI: 10.1590/1413-81232021269.2.30682019 3825
Consumption of alcoholic and non-alcoholic beverages:
THE BURDEN OF FOOD AND ALCOHOLIC BEVERAGES ON HEALTH
ELSA-Brasil results
Jordana Herzog Siqueira (https://orcid.org/0000-0003-0116-7411) 1
Nathália Miguel Teixeira Santana (https://orcid.org/0000-0003-0160-7659) 2
Taísa Sabrina Silva Pereira (https://orcid.org/0000-0002-5922-7424) 3
Alexandra Dias Moreira (https://orcid.org/0000-0002-4477-5241) 4
Isabela Martins Benseñor (https://orcid.org/0000-0002-6723-5678) 5
Sandhi Maria Barreto (https://orcid.org/0000-0001-7383-7811) 6
Gustavo Velasquez-Melendez (https://orcid.org/0000-0001-8349-5042) 4
Maria del Carmen Bisi Molina (http://orcid.org/0000-0002-8614-988X) 1
Abstract The study aims to describe the con-
sumption of alcoholic and non-alcoholic beve-
rages according to sociodemographic, health and
location variables. Cross-sectional study with
1
Programa de Pós- ELSA-Brasil data (2008-2010). A questionnaire
Graduação em Saúde was used to collect sociodemographic, food, heal-
Coletiva. Universidade
Federal do Espírito Santo. th data and anthropometry. Descriptive analysis
Av. Marechal Campos 1468, and association with variables of interest were
Bonfim. 29047-105 Vitória carried out. In the sample, 8% of the total ca-
ES Brasil. jordana.herzog@
gmail.com loric value comes from non-alcoholic beverages
2
Instituto Federal de (5.6%: sugary drinks), and 4% from alcoholic
Educação, Ciência e beverages (2.7%: beer). Consumers of unsweete-
Tecnologia do Espírito
Santo. Campus Santa Teresa ned and artificially sweetened beverages reported
ES Brasil. moderate/strong physical activity, former smokers
3
Departamento de Ciências and higher education. The opposite was true for
da Saúde, Universidad de
las Américas Puebla. San sugary drinks. Eutrophic people reported higher
Andrés Cholula Cholula consumption of sugary drinks and those obese,
México. artificially sweetened and beer. Alcohol consump-
4
Escola de Enfermagem,
Departamento de tion varied with age (young: beer; elderly: wine/
Enfermagem Materno- spirits) and education (low education: beer/spi-
Infantil e Saúde Pública, rits; higher education: wine). Coffee, natural juice
Universidade Federal
de Minas Gerais. Belo and soda were the most consumed non-alcoholic
Horizonte MG Brasil. beverages and beer was the most prevalent alcoho-
5
Departamento de Clínica lic beverage. Consumption variation was observed
Médica, Faculdade de
Medicina, Universidade de according to geographic location. The consump-
São Paulo. São Paulo SP tion of sugary and alcoholic beverages is high in
Brasil. Brazil and public health strategies are required.
6
Faculdade de Medicina,
Departamento de Medicina Key words Soft Drinks, Fruit Juices, Artificial
Preventiva e Social, Sweeteners, Alcoholic Beverages
Universidade Federal
de Minas Gerais. Belo
Horizonte MG Brasil.3826
Siqueira JH et al.
Introduction this compound is the main factor that can confer
health benefits and cause toxicity, depending on
Changes in dietary patterns, such as increased the pattern of consumption and dosage12,13. The
consumption of unhealthy and highly processed relationship between its excessive consumption
industrialized foods1, represent an important and cardiovascular diseases14 is widely estab-
contribution to adverse health outcomes2. In ad- lished, although the beneficial effects of moder-
dition, increased consumption of beverages with ate consumption remain debated, since results of
high energy density such as sugary drinks, in sev- meta-analyses15,16 and analysis of ten cohorts of
eral countries, have also contributed to the high the English population17 showed no significant
prevalence of chronic non-communicable dis- effects or no protective effect on cardiovascular
eases (NCD)2,3. Excessive alcohol consumption outcomes. A recent meta-analysis showed that, in
unquestionably leads to increased morbidity and men, any amount of alcohol is associated with an
mortality due to NCD, but the effects of moder- elevated risk of hypertension18, but there are still
ate consumption of different alcoholic beverages questions about the differential effect related to a
on the cardiovascular system are still controver- certain type of alcoholic drink14. Although there
sial4. If, on the one hand, there is consolidated is no consensus, a literature review has shown
evidence that the high consumption of sugary that low and moderate wine consumption has a
and alcoholic beverages increases the risk of car- cardioprotective effect, since it is inversely cor-
diovascular diseases, on the other hand, there are related with ischemic heart disease19.
still gaps in knowledge in relation to artificially In view of the above, additional caloric con-
sweetened ones5. sumption and alcohol content from these bever-
Four population surveys carried out between ages can play an important role in increasing the
1987-1988 and 2008-09 showed greater acquisi- incidence of cardiometabolic disorders8,14. The
tion of processed foods and beverages at the ex- literature on the consumption of industrialized
pense of fresh and minimally processed foods1. beverages in Brazil is not extensive and the sur-
The household availability of soft drinks in veys carried out use different methodologies. In
Brazilian metropolitan areas increased by 500% Brazil, Household Budget Surveys (POF - Pesqui-
between 1974-1975 and 2002-2003, correspond- sa de Orçamentos Familiares) are being carried
ing to an increase of 0.4% to 2.1% of the total out in metropolitan areas and through them the
calories consumed daily, with this consumption secular trend of household availability of food/
remaining stable in the most recent survey 2008- beverages has been assessed. POF 2002-2003
096,7. The consumption of these beverages has is based on household expenses that probably
been widely studied as a potential risk factor for underestimate general individual consumption,
several health problems. since it excludes food outside the home, an im-
Recent systematic reviews and meta-analyses portant source of industrialized beverages20. The
indicate that the consumption of sugar-sweet- Telephone-based Surveillance of Risk and Pro-
ened drinks is associated with weight gain8, the tective Factors for Chronic Diseases (VIGITEL),
risk of type 2 diabetes9 and coronary heart dis- carried out on probabilistic samples of the adult
ease10. Still, studies involving the consumption population with fixed telephony in Brazilian
of artificially sweetened drinks are controversial capitals and the Federal District, presents a ques-
and inconsistent. Although a positive association tionnaire with questions about food consump-
has already been identified between these bever- tion, however it is not is validated in all Brazilian
ages and cardiometabolic disorders, the current regions21,22.
evidence is still limited, and their consumption Thus, new data on the consumption of bever-
does not seem to be a healthy alternative to sug- ages in large samples of the Brazilian population
ar-sweetened drinks5,9. are needed to assist public food policies. There-
With regard to alcoholic beverages, Brazil ex- fore, this study aims to assess the consumption
ceeds the average annual consumption of pure al- of alcoholic and non-alcoholic beverages in par-
cohol per inhabitant of the American continent11 ticipants of the baseline of the Brazilian Longi-
and the household availability of these beverages, tudinal Study of Adult Health (ELSA-Brasil) ac-
especially beer, has doubled since the 1980s6,7. cording to sociodemographic, health and study
The main active ingredient of any alcoholic bev- location variables.
erage is ethanol, and most evidence indicates that3827
Ciência & Saúde Coletiva, 26(Supl. 2):3825-3837, 2021
Methods and consists of questions related to the frequen-
cy, duration and intensity (AFTL: walking, mod-
Study design and participants erate and vigorous; AFDL: walking, cycling) of
physical activities25. The pattern of physical activ-
This is a cross-sectional study conducted ity, in its different domains, was reported in min-
from the baseline of ELSA-Brasil (2008-2010), utes/week, consisting of multiplying the weekly
composed of 15,105 active or retired employees frequency by the duration of each of the activities
of both sexes, aged between 35 and 74 years, from performed. Physical activity was considered to be
six public institutions of higher education and that done with a minimum duration of 10 min-
national research (USP, UFMG, UFBA, UFRGS, utes/week. The variable was later categorized as
UFES and Fiocruz). Participants with missing low, moderate and strong.
data and those with non-plausible dietary data
(30
General information on the measurement of kg/m²)26.
clinical examinations, as well as on the question-
naire applied in person to collect sociodemo- Assessment of consumption of alcoholic
graphic, health and lifestyle data is available in a and non-alcoholic beverages
previous publication24. All RCs received central-
ized training to maintain quality control in data To assess the consumption of alcoholic bev-
collection. Interviewers and gaugers were also erages (beer, wine, spirits - cachaça, whiskey
certified and recertified every six months. and vodka) and non-alcoholic beverages (soda,
Sociodemographic data, health status and coffee, natural juice, industrialized juice, artifi-
lifestyle, including the consumption of alcohol- cial juice, mate tea, chimarrão and coconut wa-
ic and non-alcoholic beverages, were collected ter), participants used a semi-quantitative Food
during an interview. The race/color variable was Frequency Questionnaire (FFQ), with 114 food
self-reported and categorized as white and non- items, validated by Molina et al.27, with the objec-
white (black, brown, Asian-descendant and in- tive of estimating the usual dietary consumption
digenous); age was categorized into four groups in the last twelve months.
(35-44; 45-54; 55-64; 65-74); the level of educa- The FFQ is structured in: 1. Food/prepara-
tion was categorized as elementary (≤8 years of tions; 2. Measures of consumption portions; 3.
study), medium (9-11 years of study) and high- Frequencies of consumption, with eight response
er/graduate (≥12 years of study); smoking was options, ranging from “More than 3x/day” to
categorized as never, former smoker and current “Never/Almost Never”; 4. Seasonal consump-
smoker; family income per capita was calculated tion for individuals who reported spontaneously
and analyzed in Brazilian reais. Physical activi- consuming the food item only at a certain time
ty was estimated using the International Physi- of the year or in the season. The list of food and
cal Activity Questionnaire (IPAQ) long version, beverages was read by ELSA-Brasil interviewers
in the domains of leisure time physical activi- to the participants, who were asked to respond
ty (AFTL) and displacement physical activity about their usual consumption in the last twelve
(AFDL). The instrument was validated in Brazil months, in daily, weekly and monthly consump-3828
Siqueira JH et al.
tion frequencies. A kit of utensils was used during Results
the administration of the FFQ, to help estimate
the amount of food, preparations and beverages The final sample consisted of 14,224 individuals
consumed. with an average age of 52.1±9.1 years. Significant
Regarding non-alcoholic beverages natural differences were found between genders accord-
juice (fruit or pulp), industrialized juice (box or ing to sociodemographic, health and total calorie
bottle), artificial juice (powder), coffee and mate variables (Table 1). Most of the sample was rep-
tea, the participant had three response options: resented by women (55%), with higher educa-
with sugar, without sugar or with artificial sweet- tion (53.5%), overweight (40.4%), who practice
ener. Regarding soda, the participant had two an- weak physical activity (76.9%) and who never
swer options: with sugar or with sweetener. Final- smoked (57.2%). The average caloric intake was
ly, coconut water and chimarrão were considered 2,291±778 Kcal/day.
in their natural versions, that is, without added The consumption of non-alcoholic bever-
sugar. Regarding alcoholic beverages, it was asked ages differed in relation to sociodemographic
about the consumption of spirits (cachaça, whis- and health variables (Table 2). Higher average
key or vodka), beer and wine (white or red). consumption of non-sweetened and artificially
The beverages were divided into two groups: sweetened beverages was observed in women,
alcoholic and non-alcoholic. Alcoholic beverages older age, white, with higher education/postgrad-
were presented separately (beer, wine and spir- uate education and who reported engaging in
its) and as the sum of all drinks. Non-alcoholic moderate/strong physical activity and being for-
beverages were presented separately (each bever- mer smokers (p3829
Ciência & Saúde Coletiva, 26(Supl. 2):3825-3837, 2021
Table 1. Distribution of sociodemographic, health and total calorie variables according to sex. ELSA-Brasil, 2008-
2010.
Sex
Total
Male Female
Variables (n=14,224) p-value*
(n=6,366) (n=7,858)
n (%) n (%) n (%)
Age
35 to 44 1421 (22.3) 1703 (21.7) 3124 (22)3830
Siqueira JH et al.
Table 2. Consumption of non-alcoholic and alcoholic beverages according to sociodemographic and health
variables. ELSA-Brasil, 2008-2010.
Non-alcoholic beverages Alcoholic beveragesa
With
Unsweetened With sugar Beer Wine Spirits
Variáveis sweetener
(ml/day) (ml/day) (ml/day) (ml/day) (ml/day) (ml/day)
Mean±SD Mean±SD Mean±SD Mean±SD Mean±SD Mean±SD
Sex
Male 171±292 312±367 132±232 214±313 32±52 5.8±13
Female 180±279 243±326 159±242 76±158 25±40 1.2±5
p-value* 0.0503831
Ciência & Saúde Coletiva, 26(Supl. 2):3825-3837, 2021
Table 3. Consumption of alcoholic and non-alcoholic beverages according to Research Center. ELSA-Brasil, 2008-2010.
Centro de Investigação
Espírito Minas Rio de Rio Grande ELSA- p-
Variables Bahia São Paulo
Santo Gerais Janeiro do Sul Brasil value*
Mean±SD Mean±SD Mean±SD Mean±SD Mean±SD Mean±SD Mean±SD
Non-alcoholic (n=1,869) (n=1,011) (n=2,979) (n=1,699) (n=1,986) (n=4,686) (n=14,224)
beverages (ml/day)
Soft drinks with 45±108 50±138 54±137 74±185 68±172 67±174 61±1593832
Siqueira JH et al.
8
7,2
7
6,4
6 5,8 5,6
5,2 5,0
5 4,8 4,7
4,5 4,5
4,1 4,0 4,0
%
4
3,5 Suggar-sweetened
Alcoholica
3
2
1
0
Bahia Espírito Minas Rio de Rio Grande São Paulo ELSA-Brasil
Santo Gerais Janeiro do Sul
Research center
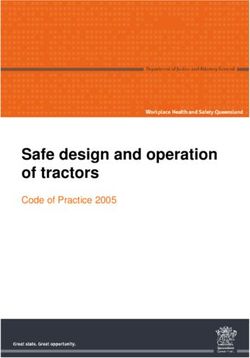
Figure 1. Daily caloric contribution of sugar-sweetened and alcoholic beverages to total energy consumption
according to Research Center. ELSA-Brasil, 2008-2010.
a
n=8,956.
Source: Elaborated by the authors.
beverages, is characterized by the intake of coffee, It is well documented that men have a high-
juices and soft drinks, and two foods are marked- er intake of alcoholic beverages than women and
ly for regional consumption, one being tea in the that habitual consumption is higher in individ-
south of the country28. In addition, greater coffee uals with higher education29. The INA (2008-
intake was observed in the north and northeast 2009) showed a higher prevalence of soft drink
of the country28, corroborating with the data intake in men and in the highest income quar-
from the present study that found higher con- tile28, as did VIGITEL, which also found a high-
sumption averages in the Bahia RC. The lowest er consumption of soft drinks among men with
averages of beer consumption were observed in higher education during the period evaluated
the Rio Grande do Sul RC, while it presents the (2007-2016)30. In our study, the average con-
highest average consumption of wine and chi- sumption of sugary and alcoholic beverages was
marrão, known as more convenient options for higher in men and in individuals with less educa-
the regional climate and culture. tion (except for wine). We observed that in indi-
According to the POF (2008-2009), the av- viduals with higher education, the consumption
erage consumption of soft drinks in Brazilian of non-sweetened drinks, those artificially sweet-
adults was approximately 100 ml/day6, a value ened and wine is higher. Artificial sweeteners are
close to that found in this study. In the United marketed as an alternative for weight loss be-
States and United Kingdom, the average con- cause they do not add calories, although studies
sumption of soft drinks is higher, around 284 have already indicated changes in the microbiota
ml/day and 114 ml/day, respectively9. POF (2008- and glucose homeostasis31. The consumption of
2009) analyses also showed that alcoholic and wine, a drink generally with a higher price, has
non-alcoholic beverages contribute about 17% been associated with a better quality of life and
to total energy consumption3. In this sample, the cardioprotective benefits32.
contribution of these beverages was slightly low- Meta-analysis showed the effect of consum-
er, around 12%. ing sugar-sweetened drinks on weight gain and3833
Ciência & Saúde Coletiva, 26(Supl. 2):3825-3837, 2021
Table 4. Averages and daily caloric contribution of non-alcoholic and alcoholic beverages to total energy consumption.
ELSA-Brasil, 2008-2010.
Sex
Total
Male Female Male Female
Variables p- p- Percentage
Percentage of caloric value* Mean±SD
Mean±SD (Kcal/day) value* of caloric
contribution (Kcal/day)
contribution
Non-alcoholic (n=6,366) (n=7,858) (n=6,366) (n=7,858) (n=14,224) (n=14,224)
beveragesa
Unsweetened 35±68 37±67 0.081 1.4 1.83834
Siqueira JH et al.
natives, such as artificially sweetened beverages the POF and VIGITEL make the comparison of
and fruit juices5. A recent systematic review and data delicate, but they contribute to the discus-
meta-analysis shows that the habitual consump- sion of the topic. There are still no published
tion of sugar-sweetened drinks increases the risk studies that endorse this declining trend as of
of type 2 diabetes regardless of adiposity, and ar- 2007, considering that the last national popula-
tificially sweetened drinks and fruit juice do not tion-based survey was carried out in 2008-2009.
decrease the risk of such injury and, therefore, At the same time, it is important to highlight
cannot be considered healthy options9. These that the growth of the food processing indus-
findings are probably related to the high glycemic try, the inclusion of transnational companies in
index (soft drinks) and moderate one (juices) as- parallel with the expansion of supermarkets has
sociated with type 2 diabetes41; the high fructose been rapidly diversifying the options of drinks
content associated with insulin resistance42; in with high energy density in Brazil47. The con-
addition to the deleterious effects of caffeine43, sumption of these beverages in the country fol-
phosphoric acid and dyes44. lows the trends of increasing excess weight, since
It is worth pointing out that the potential the percentage of Brazilian adults with excess
benefits of consuming non-calorie drinks will weight increased from 24% (1974-1975) to 49%
not be achieved if the intake is accompanied (2008-2009)48. In the present study, overweight
by a compensatory increase in energy intake exceeds 60%. In this context, one of the main tar-
from other food sources5. Thus, we have shown gets for rapidly improving public health has been
in the present study that the consumption of the taxation of processed foods and beverages49.
non-sweetened and artificially sweetened bever- The search for strategies to reduce or slow
ages was associated with the practice of more vig- the expansion of consumption of industrialized
orous physical activity and that eutrophic indi- products is essential. It is already proven that the
viduals consumed more sugar-sweetened drinks, taxation of soft drinks in Brazil would lead to re-
while the obese presented greater consumption ductions in consumption50. In 2017, the Minister
of artificially sweetened beverages. Thus, we can of Health in Brazil, in an informal note, reported
see that, under these conditions, sugar-sweet- being in favor of adopting a tax on sugar-sweet-
ened drinks may be being replaced by artificially ened drinks, but no initiative was observed. Thus,
sweetened ones because they have fewer calories in Brazil, there are no advances in the taxation
and, therefore, appear to be healthier options. of sugar-sweetened drinks and there is also no
However, even though studies in this area are progress in the regulation of advertising of food
consolidating in the literature, studies already and beverages, despite the fact that the country
show that the high consumption of artificial has made a commitment to reduce obesity and
sweeteners can contribute to the increased risk the Pan American Health Organization con-
of obesity and negative health effects45, in addi- sumption of sugar-sweetened drinks by 201951.
tion to increasing the risk of stroke46. We also ob- Brazil is one of the signatories to the Glob-
served that individuals who practice low physical al Strategy to Reduce Harmful Use of Alcohol52,
activity and current smokers made greater use of approved by the World Health Assembly, which
sugar-sweetened drinks, adding another compo- brings some aspects and recommendations also
nent to the less healthy lifestyle. present in the National Alcohol Plan53 and in the
Although POF data since the 1980s showed an prohibition on drinking and driving54. However,
increase in household soft drink availability until when analyzing the public policies adopted, with
2002-2003 and stability in 2008-20096,7, a study regard to the reduction of harmful use of alcohol,
by VIGITEL found a significant reduction in reg- it is observed that measures such as the restric-
ular consumption (≥5 days/week) of soft drinks tion of marketing, sponsorship and promotions
and artificial juices from 30.9% to 16.5% during and increase in prices and sales limits55 are not
the years analyzed (2007-2016), although one in being adopted in Brazil.
six adults (16.5%) reported daily consumption30. ELSA-Brasil is not a representative study of
These data, however, need to be interpreted with the Brazilian population, but it portrays a por-
caution, since, despite the downward trend ob- tion of the population, which by the results
served in the period, health risks cannot yet be found, does not differ much from the general
considered to be overcome, since in 2016 al- population. The FFQ is the most suitable instru-
most 26 million Brazilian adults consumed sug- ment for epidemiological studies, but it presents
ar-sweetened drinks almost daily or even every as a limitation the possibility of overestimating
day30. The methodological differences between food consumption. This issue is frequently re-3835
Ciência & Saúde Coletiva, 26(Supl. 2):3825-3837, 2021
ported, but it was possible to minimize it with ple of civil servants from three Brazilian regions
greater quality control in data collection and and used a collection instrument that allows
exclusion of participants who reported implau- greater detail of food consumption, as it reflects
sible intake values. However, the methodological habitual consumption.
aspects of this study reinforce its internal validi- Finally, the consumption of sugary-sweet-
ty, such as the standardization of data collection, ened and alcoholic beverages is high in Brazil
the consolidated procedures for conducting the and there is already evidence that public health
interview, measurement of anthropometric mea- strategies discourage the consumption of these
sures and periodic training in all RCs. Although beverages as part of a healthy lifestyle. Food
the Brazilian surveys that investigated food con- guidelines, inspection policies and taxation of
sumption have strengths (representativeness of processed foods are necessary to reduce and pre-
the Brazilian population), they also have limita- vent diseases related to overweight, in addition to
tions. ELSA-Brasil is carried out with a large sam- improving the population’s food consumption.
Collaborations
JH Siqueira performed the analysis and interpre-
tation of the data and produced the writing of
the article. NMT Santana, AD Moreira and TSS
Pereira assisted in data analysis and critically
reviewed the content. IM Benseñor, SM Barreto
and G Velasquez-Melendez contributed to the
study design and data acquisition. MCB Molina
assisted in the study design, data acquisition, crit-
ical review of the content and final approval of its
version for publication.
Acknowledgments
To ELSA-Brasil employees and participants for
their important contributions. To professor
José Geraldo Mill for contributions in the arti-
cle. JH Siqueira received a scholarship from the
Fundação de Amparo à Pesquisa e Inovação
do Espírito Santo (FAPES)/ Coordenação de
Aperfeiçoamento de Pessoal de Nível Superior
(CAPES). MCB Molina has a Conselho Nacion-
al de Desenvolvimento Científico e Tecnológico
(CNPq) productivity grant.
To Fundação de Amparo à Pesquisa do Esta-
do de Minas Gerais (Fapemig).3836
Siqueira JH et al.
References
1. Martins APB, Levy RB, Claro RM, Moubarac JC, 15. Global Burden of Disease Study 2016 Alcohol Colla-
Monteiro CA. Participação crescente de produtos ul- borators. Alcohol use and burden for 195 countries
traprocessados na dieta brasileira (1987-2009). Rev and territories, 1990–2016: a systematic analysis for
Saude Publica 2013; 47(4):656-665. the Global Burden of Disease Study 2016. Lancet
2. Monteiro CA, Cannon G. The impact of transnational 2018; 392(22):1015-1035.
“big food” companies on the South: a view from Bra- 16. Stockwell T, Zhao J, Panwar S, Roemer A, Naimi T,
zil. PLoS Med 2012; 9(7):e1001252. Chikritzhs T. Do ‘moderate’ drinkers have reduced
3. Pereira RA, Souza AM, Duffey KJ, Sichieri R, Popkin mortality risk? A systematic review and meta-analy-
BM. Beverage consumption in Brazil: Results from sis of alcohol consumption and all-cause mortality. J
the first National Dietary Survey. Public Health Nutr Stud Alcohol Drugs 2016; 77(2):185-198.
2015; 18(7):1164-1172. 17. Knott CS, Coombs N, Stamatakis E, Biddulph JP. All
4. Chiva-Blanch G, Arranz S, Lamuela-Raventos RM, cause mortality and the case for age specific alcohol
Estruch R. Effects of wine, alcohol and polyphenols consumption guidelines: pooled analyses of up to 10
on cardiovascular disease risk factors: evidences from population based cohorts. BMJ 2015; 350:h384.
human studies. Alcohol Alcohol 2013; 48(3):270-277. 18. Roerecke M, Tobe SW, Kaczorowski J, Bacon SL, Va-
5. Johnson RK, Lichtenstein AH, Anderson CAM, Car- faei A, Hasan OSM, Krishnan RJ, Raifu AO, Rehm J.
son JA, Després JP, Hu FB, Kris-Etherton PM, Otten JJ, Sex-Specific Associations Between Alcohol Consump-
Towfighi A, Wylie-Rosett J; American Heart Associa- tion and Incidence of Hypertension: A Systematic Re-
tion Nutrition Committee of the Council on Lifestyle view and Meta-Analysis of Cohort Studies. J Am Heart
and Cardiometabolic Health; Council on Cardiovas- Assoc 2018; 7(13):e008202.
cular and Stroke Nursing; Council on Clinical Car- 19. Haseeb S, Alexander B, Baranchuk A. Wine and Car-
diology; Council on Quality of Care and Outcomes diovascular Health: A Comprehensive Review. Circu-
Research; and Stroke Council. Low-Calorie Sweetened lation 2017; 136(15):1434-1448.
Beverages and Cardiometabolic Health: A Science Ad- 20. Bezerra IN, Souza AM, Pereira RA, Sichieri R. Con-
visory From the American Heart Association. Circula- sumo de alimentos fora de casa no Brasil. Rev Saude
tion 2018; 138:e126-e140. Publica 2013; 47(Supl. 1):200S-211S.
6. Brasil. Ministério do Planejamento, Orçamento e 21. Monteiro CA, Moura EC, Jaime PC, Claro RM. Va-
Gestão. Instituto Brasileiro de Geografia e Estatística lidade de indicadores do consumo de alimentos e
(IBGE). Pesquisa de Orçamentos Familiares 2008–2009 bebidas obtidos por inquérito telefônico. Rev Saude
- Avaliação Nutricional da Disponibilidade Domiciliar Publica 2008; 42:582-589.
de Alimentos no Brasil. IBGE: Rio de Janeiro; 2010. 22. Neves ACM, Gonzaga LAA, Martens IBG, Moura EC.
7. Levy-Costa RB, Sichieri R, Pontes NS, Monteiro CA. Validação de indicadores do consumo de alimentos e
Household food availability in Brazil: distribution bebidas obtidos por inquérito telefônico em Belém,
and trends (1974-2003). Rev Saude Publica 2005; Pará, Brasil. Cad Saude Publica 2010; 26(12):2379-
39(4):530-540. 2388.
8. Malik VS, Popkin BM, Bray GA, Després JP, Hu FB. 23. Schmidt MI, Duncan BB, Mill JG, Lotufo PA, Chor D,
Sugar-sweetened beverages, obesity, type 2 diabetes Barreto SM, Aquino EM, Passos VM, Matos SM, Mo-
mellitus, and cardiovascular disease risk. Circulation lina MC, Carvalho MS, Bensenor IM. Cohort Profile:
2010; 121(11):1356-1364. Longitudinal Study of Adult Health (ELSA-Brasil). Int
9. Imamura F, O’Connor L, Ye Z, Mursu J, Hayashino Y, J Epidemiol 2015; 44(1):68-75.
Bhupathiraju SN, Forouhi NG. Consumption of sugar 24. Mill JG, Pinto K, Griep RH, Goulart A, Foppa M, Lo-
sweetened beverages, artificially sweetened beverages, tufo PA, Maestri MK, Ribeiro AL, Andreão RV, Dantas
and fruit juice and incidence of type 2 diabetes: sys- EM, Oliveira I, Fuchs SC, Cunha RS, Bensenor IM.
tematic review, meta-analysis, and estimation of po- Medical assessments and measurements in ELSA-Bra-
pulation attributable fraction. BMJ 2015; 351:h3576. sil. Rev Saude Publica 2013; 47(Supl. 2):54-62.
10. Temple NJ. Fat, Sugar, Whole Grains and Heart Disea- 25. Matsudo S, Araujo T, Matsudo V, Andrade D, Andra-
se: 50 Years of Confusion. Nutrients 2018; 10(39):1-9. de E, Oliveira LC, Braggion G. International Physi-
11. World Health Organization (WHO). Global Status cal Activity Questionnaire (IPAQ): Study of validity
Report on Alcohol and Health 2014. Genebra: WHO; and reliability in Brazil. Rev Bras Ativ Fis Saude 2011;
2014. 6(2):5-18.
12. Mukamal KJ, Jensen MK, Grønbaek M, Stampfer MJ, 26. World Health Organization (WHO). Obesity: pre-
Manson JE, Pischon T, Rimm EB. Drinking frequency, venting and managing the global epidemic: report of a
mediating biomarkers, and risk of myocardial infarc- WHO consultation. Genebra: WHO; 2000.
tion in women and men. Circulation 2005; 112:1406- 27. Molina MCB, Benseñor I, Cardoso LO, Velasquez-Me-
1413. lendez G, Drehmer M, Pereira TSS, Faria CP, Melere
13. Krenz M, Korthuis RJ. Moderate ethanol ingestion C, Manato L, Gomes ALC; Fonseca MJM; Sichieri R.
and cardiovascular protection: from epidemiologic Reprodutibilidade e validade relativa do questionário
associations to cellular mechanisms. J Mol Cell Car- de frequência alimentar do ELSA-Brasil. Cad Saude
diol 2012; 52:93-104. Publica 2013; 29(2):379-389.
14. Piano MR. Alcohol’s Effects on the Cardiovascular 28. Souza AM, Pereira RA, Yokoo EM, Levy RB, Sichieri R.
System. Alcohol Res 2017; 38(2):219-241. Alimentos mais consumidos no Brasil: Inquérito Na-
cional de Alimentação 2008-2009. Rev Saude Publica
2013; 47(Supl. 1):190S-199S.3837
Ciência & Saúde Coletiva, 26(Supl. 2):3825-3837, 2021
29. Machado IE, Monteiro MG, Malta DC, Lana FCF. 47. Aguiar DRD. The Case of Brazil. In: Stiegert KW, Kim
Brazilian Health Survey (2013): relation between al- DH, editores. Structural Changes in Food Retailing: Six
cohol use and sociodemographic characteristics by Country Case Studies. Madison: Food System Research
sex in Brazil. Rev Bras Epidemiol 2018; 20(3):408-422. Group; 2009. p. 151.
30. Figueiredo N, Maia EG, Silva LESD, Granado FS, Cla- 48. Brasil. Ministério do Planejamento, Orçamento e
ro RM. Trends in sweetened beverages consumption Gestão. Instituto Brasileiro de Geografia e Estatística
among adults in the Brazilian capitals, 2007–2016. (IBGE). Pesquisa de Orçamentos Familiares 2008–2009
Public Health Nutr 2018; 21(18):3307-3317. -Antropometria e estado nutricional de crianças, ado-
31. Pearlman M, Obert J, Casey L. The Association Betwe- lescentes e adultos no Brasil. Rio de Janeiro: IBGE;
en Artificial Sweeteners and Obesity. Curr Gastroente- 2010.
rol Rep 2017; 19(12):64. 49. Rivera JA, Muñoz-Hernández O, Rosas-Peralta M,
32. Fernandes I, Pérez-Gregorio R, Soares S, Mateus N, Aguilar-Salinas CA, Popkin BM, Willett WC. Consu-
Freitas V. Wine Flavonoids in Health and Disease Pre- mo de bebidas para una vida saludable: recomenda-
vention. Molecules 2017; 22:292. ciones para la población mexicana. Salud Publica Mex
33. DiMeglio DP, Mattes RD. Liquid versus solid carbohy- 2008; 50(2):173-195.
drate: effects on food intake and body weight. Int J 50. Claro RM, Levy RB, Popkin BM, Monteiro CA. Su-
Obes Relat Metab Disord 2000; 24(6):794-800. gar-Sweetened Beverage Taxes in Brazil. Am J Public
34. Willett W, Manson J, Liu S. Glycemic index, glycemic Health 2012; 102(1):178-183.
load, and risk of type 2 diabetes. Am J Clin Nutr 2002; 51. Interministerial Food and Nutrition Security Cham-
76(1):274S-280S. ber. Brazil’s Commitments to the United Nations Deca-
35. Pereira RA, Duffey KJ, Sichieri R, Popkin BM. Sour- de of Action on Nutrition (2016–2025). Brasília: CAI-
ces of excessive saturated fat, trans fat and sugar con- SAN; 2015.
sumption in Brazil: an analysis of the first Brazilian 52. World Health Organization (WHO). Global strategy
nationwide individual dietary survey. Public Health to reduce the harmful use of alcohol. Genebra: WHO;
Nutr 2014; 17(1):113-121. 2010.
36. Institute for Health Metrics and Evaluation. Global 53. Brasil. Decreto nº 6.117, de 22 de maio de 2007. Apro-
Burden of Disease. Country Profiles. Brazil. Seattle: va a Política Nacional sobre o Álcool, dispõe sobre as
IHME; 2013. medidas para redução do uso indevido de álcool e
37. Brasil. Economia Brasileira em perspectiva. Brasília: sua associação com a violência e criminalidade, e dá
Ministério da Fazenda; 2010. outras providências. Diário Oficial da União 2007; 23
38. World Health Organization (WHO). International mai.
Guide for Monitoring Alcohol Consumption and Rela- 54. Brasil. Lei nº 11.705, de 19 de junho de 2008. Altera a
ted Harm. Genebra: WHO; 2000. Lei nº 9.503, de 23 de setembro de 1997, que ‘institui
39. Muhlack E, Carter D, Braunack-Mayer A, Morfidis o Código de Trânsito Brasileiro’, e a Lei nº 9.294, de 15
N, Eliott J. Constructions of alcohol consumption de julho de 1996, que dispõe sobre as restrições ao uso
by non-problematised middle-aged drinkers: a qua- e à propaganda de produtos fumígeros, bebidas alco-
litative systematic review. BMC Public Health 2018; ólicas, medicamentos, terapias e defensivos agrícolas,
18(1):1016. nos termos do § 4o do art. 220 da Constituição Fe-
40. Traversy D, Chaput JP. Alcohol Consumption and deral, para inibir o consumo de bebida alcoólica por
Obesity: An Update. Curr Obes Rep 2015; 4(1):122- condutor de veículo automotor, e dá outras providên-
130. cias. Diário Oficial da União 2008; 20 jun.
41. Livesey G, Taylor R, Livesey H, Liu S. Is there a dose 55. Pan American Health Organization (PAHO). Regional
-response relation of dietary glycemic load to risk of Status Report on Alcohol and Health in the Americas.
type 2 diabetes? Meta-analysis of prospective cohort Washington, D.C.: PAHO; 2015.
studies. Am J Clin Nutr 2013; 97:584-596.
42. Stanhope KL. Role of fructose-containing sugars in
the epidemics of obesity and metabolic syndrome.
Annu Rev Med 2012; 63:329-343.
43. Bhupathiraju SN, Pan A, Malik VS, Manson JE, Willett
WC, van Dam RM, Hu FB. Caffeinated and caffeine-
free beverages and risk of type 2 diabetes. Am J Clin
Nutr 2013; 97:155-166.
44. Fitzpatrick L, Heaney RP. Got soda? J Bone Miner Me-
tab 2003; 18(9):1570-1572.
45. Shearer J, Swithers SE. Artificial sweeteners and meta-
bolic dysregulation: Lessons learned from agriculture
and the laboratory. Rev Endocr Metab Disord 2016;
17(2):179-186. Article submitted 30/03/2019
46. Mossavar-Rahmani Y, Kamensky V, Manson JE, Silver Approved 07/02/2020
B, Rapp SR, Haring B, Beresford SAA, Snetselaar L, Final version submitted 09/02/2020
Wassertheil-Smoller S. Artificially Sweetened Bevera-
ges and Stroke, Coronary Heart Disease, and All-Cau-
se Mortality in the Women’s Health Initiative. Stroke Chief editors: Romeu Gomes, Antônio Augusto Moura da
2019; 50(3):555-562. Silva
CC BY This is an Open Access article distributed under the terms of the Creative Commons Attribution LicenseYou can also read