Constipation: An approach to diagnosis, treatment, referral
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
REVIEW
EDY E. SOFFER M D
Départirent of Gastroenterology-Hepatology,
The Cleveland Clinic
Constipation: An approach
to diagnosis, treatment, referral
ABSTRACT H E N A P A T I E N T reports constipation, a
careful history and physical examina-
When a patient reports constipation, a careful history and tion performed by the primary care physician
physical examination may identify the underlying cause. are usually sufficient to identify any underlying
In many patients, though, no underlying cause is identified. cause, although in most patients no such cause
Empiric treatment with exercise, hydration, fiber can be found.
supplementation, and mild laxatives is often effective. This article outlines an approach to the
If constipation does not resolve with these measures, then diagnosis and treatment of constipation, as
well as what happens when patients with
the physician may refer the patient for further testing for
severe, treatment-resistant constipation are
slow colonic transit, pelvic floor dysfunction, or anatomical
referred for additional testing.
defects, and in difficult and recalcitrant cases for surgical
treatment. • THE PREVALENCE OF CONSTIPATION
KEY POINTS In adults, constipation is more prevalent in the
elderly than in the young, and young to mid-
A detailed history is the most important part of the initial
dle-aged women are much more likely to report
diagnostic evaluation of constipation. it than are men. Nationwide surveys put the
prevalence of constipation in the general pop-
Ask patients about medications they are taking, since ulation at 2% to 12.8%, based on a range of
medications such as anticholinergics, narcotics, and subjective complaints. 1 ' 2 A recent survey based
antidepressants may cause constipation. on definite criteria 3 found a prevalence of 3%.4
A four-step empirical approach to treatment is usually • DEFINING CONSTIPATION
appropriate at first. A N D IDENTIFYING THE CAUSE
A small minority of patients will not be relieved by empiric Constipation is not a disease, but rather a
symptom. As such, it is interpreted subjective-
treatments and should be referred for specialized testing.
ly by the patient. Patients' complaints of con-
stipation vary, and misconceptions about
bowel habits are common and may lead
patients to falsely assume they have constipa-
tion. Patients may also complain of nausea and
abdominal pain associated with less frequent
bowel movements.
Misconceptions about bowel habits
Bowel habits in healthy adults vary widely.
The frequency of bowel movements, for exam-
CLEVELAND CLINIC JOURNAL OF MEDICINE V O L U M E 6 6 • NUMBER 1 JANUARY 1 9 9 9 35
Downloaded from www.ccjm.org on January 29, 2022. For personal use only. All other uses require permission.
CONSTIPATION SOFFER
TABLE 1 Asking the right questions
A detailed history is the most important part
Causes of chronic constipation of the diagnostic evaluation. Asking the right
Mechanical questions helps to identify the extent and the
Neoplasms cause of the constipation:
Rectal intussusception or prolapse • Is the constipation a recent or a chron-
Rectocele
ic problem?
Functional • W h a t is the main complaint: reduced
Irritable bowel disease stool frequency, hard stools, excessive
Pharmacologic straining?
Anticholinergics • How many bowel movements per week
Antidepressants does the patient have?
Antiparkinsonian agents Most patients who complain of constipation
Calcium-channel blockers
Iron supplements have no identifiable underlying cause.
Opiates Nevertheless, the initial history should strive
to exclude a wide variety of potential causes,
Metabolic and endocrine
Diabetes as listed in TABLE 1. These include central and
Hypercalcemia peripheral neurologic diseases, endocrine and
Hypothyroidism metabolic conditions, and colonic obstruc-
Neurogenic tion. Many of these causes are easily
Aganglionosis (Hirschsprung disease) reversible.
Intestinal pseudo-obstruction Ask what medications the patient is tak-
Multiple sclerosis ing. Anticholinergics, narcotics, and antide-
Parkinson disease pressants are among those that can lead to
If history and examination fail to constipation, particularly in the elderly.
identify one of the above causes, In adults, rectal prolapse, an obstructive
then consider: cause of constipation, is far more common in
Slow colonic transit (colonic inertia)
Pelvic floor dysfunction women than in men, especially in elderly
Look for women. Also, if a patient reports the need to
apply pressure on the perineum or on the pos-
concomitant terior wall of the vagina for evacuation, the
use of pie, may vary from several movements a day to physician should suspect a rectocele.
constipating several a week. Yet many people believe that
Laboratory tests
"normal" means at least one bowel movement
drugs, daily and that anything less means constipa- To help identify underlying problems, perform
tion. In addition, many people have miscon- the following laboratory tests routinely in
especially in ceptions about the appearance and consisten- patients who complain of constipation.
older patients cy of stools, which may prompt concern and Thyroid function. Hypothyroid patients
complaints to their physician. often complain of constipation.
Constipation means different things to Serum calcium levels. Hypercalcemia
different patients: stools too infrequent, due to neoplasms, h y p e r p a r a t h y r o i d i s m ,
stools too hard, stools too difficult to pass, and megadose vitamins can cause constipa-
straining, the feeling of incomplete evacua- tion.
tion after a bowel movement, abdominal dis- Fecal occult blood testing helps exclude
comfort. colon cancer, which can cause constipation.
Defining constipation either as a decrease
in the frequency of bowel movements to fewer Examination of the anus and rectum
than three per week, or as subjective symp- Physical examination may reveal anal fis-
toms of defecatory dysfunction (eg, painful sures or hemorrhoids in patients who com-
defecation, incomplete defecation, excessive plain of painful defecation. Inspection of the
straining) can facilitate the identification of anus during attempted defecation can detect
the underlying cause. 5 prolapse of the rectal mucosa.
42 C L E V E L A N D C L I N I C J O U R N A L OF M E D I C I N E VOLUME 66 • NUMBER 1 JANUARY 1999
Downloaded from www.ccjm.org on January 29, 2022. For personal use only. All other uses require permission.
Digital rectal examination assesses the TABLE 3
presence of fissures, fistulas, and hemorrhoids,
as well as anal sphincter tone. The formation Empirical t r e a t m e n t of constipation:
of a rectocele can be noted during attempted A stepwise approach
defecation, while contraction of the anal Step 1 Nonstrenuous exercise
sphincter suggests pelvic floor dysfunction. Adequate hydration
Digital rectal examination also reveals Dedicated time for bowel movements
fecal impaction, presenting as a hard to rub- Adequate dietary fiber intake
bery mass in the rectum. It is especially impor-
Step 2 Processed or synthetic fiber (polycarbophil, psyllium,
tant to rule out fecal impaction in institution- methylcellulose)
alized patients, as fecal impaction may present Stool softeners with docusate sodium for patients
paradoxically as fecal incontinence. In these with hard stools
patients, constipation often goes unsuspected
and can be aggravated by treatment with con- Step 3 Osmotic laxatives (magnesium citrate, magnesium
hydroxide, sodium phosphates, lactulose); but avoid In
stipating agents.
patients with renal Insufficiency or on sodium-restricted diet
Anoscopy will identify anal fissures, fistu-
las, and hemorrhoids in patients complaining Step 4 Stimulant laxatives, to promote colonic secretion
of painful defecation. and motility
Evaluation of the colon in patients with mmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmmm^m
recent constipation depends on the presenta-
tion. If rectal bleeding or iron deficiency ane- stepwise approach is recommended, as illus-
mia is present, colonoscopy is preferable. trated in TABLE 2.
Otherwise, barium enema radiography is less General measures can be applied at first.
costly and is helpful in establishing the pres- These consist of nonstrenuous exercise (eg,
ence of megarectum or megacolon. walking a few miles a day), adequate hydra-
tion (six to eight glasses of water per day),
• CONSTIPATION OF U N K N O W N CAUSE and 15 to 20 minutes of regular dedicated
time for bowel movements, preferably in the
In most patients, however, no specific under- morning after breakfast, to take advantage of Try exercise,
lying condition can be identified. This is gen- increased colonic motility following food
erally the case in middle-aged and elderly ingestion. A n adequate amount of dietary
dietary fiber,
women. fiber—ie, 20 to 35 g—should be consumed and dedicating
Patients in whom no cause for constipa- daily. Fiber can be obtained from such sources
tion can be identified include those with slow as whole wheat bread, bran cereal, fruits, and
time for bowel
colonic transit and those with pelvic floor dys- vegetables. movements
function (rectopubalis dyssynergia, obstructed Processed or synthetic fiber (polycar-
defecation, pelvic floor dyssynergia). Pelvic bophil, psyllium, methylcellulose) can be
floor dysfunction results from a lack of relax- given if patients fail to take in enough fiber
ation or paradoxical contraction of the pub- from dietary sources. These are available in
orectalis muscle and the anal sphincter in many preparations. Stool softeners containing
response to straining. Clues to the presence of docusate can be given to patients with hard
this condition are complaints of excessive stools.
straining in spite of the frequent urge to defe- Osmotic laxatives can be added next.
cate. These patients should be treated empiri- This group contains mostly various magne-
cally, and those that respond poorly to empir- sium salts (magnesium citrate, magnesium
ic treatment should be referred. hydroxide) or nonabsorbable sugars such as
lactulose or sorbitol. They have a good safety
• STEPWISE APPROACH TO TREATMENT profile but should not be used in patients with
renal insufficiency, because of the risk of mag-
The great majority of patients with constipa- nesium overload, or in patients on a sodium-
tion can be treated empirically, regardless of restricted diet. T h e chronic use of mineral oil
whether an underlying cause is identified. A can result in malabsorption of fat-soluble vit-
C L E V E L A N D C L I N I C J O U R N A L OF M E D I C I N E VOLUME 66 • NUMBER 1 JANUARY 1999 37
Downloaded from www.ccjm.org on January 29, 2022. For personal use only. All other uses require permission.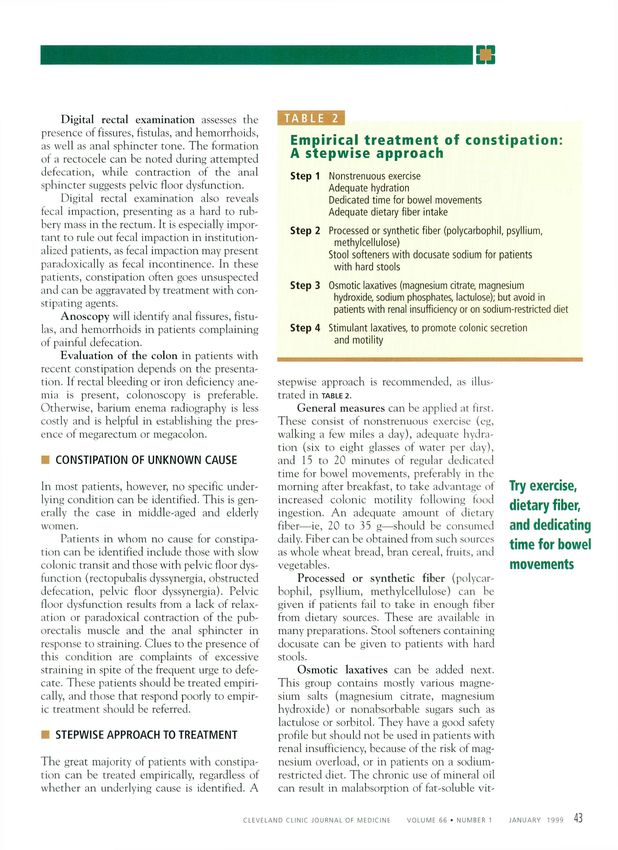
CONSTIPATION SOFFER
amins and should be altogether avoided in who complain of infrequent defecation yet
patients at risk for aspiration, for fear of lipoid have normal colonic transit are more likely to
pneumonia. Cisapride, a prokinetic agent, has have psychological disturbances, as compared
shown some promise in recent studies. Water with those with slow transit. 9
enemas or those containing saline laxatives
are less easy to use. Soapsuds enemas can cause Anorectal manometry
colitis 6 and should be avoided. Anorectal manometry combined with elec-
Stimulant laxatives should be reserved for tromyography of the perianal surface provides
last. They stimulate colonic secretion and pressure profiles of the anal sphincter. Under
motility. Most are diphenylmethane deriva- normal conditions, the intra-abdominal pres-
tives (bisacodyl or phenolphthalein com- sure increases and the anal sphincter relaxes,
pounds) or anthraquinone derivatives (such as with no electromyographic change.
senna). Compounds containing phenolph- However, in patients with obstructed defe-
thalein have been recently withdrawn follow- cation, electromyographic activity and
ing warnings of possible carcinogenic effects. increased anal pressure are observed during
attempted defecation. This pattern of
• REFERRAL FOR ADDITIONAL TESTING increased activity may be seen in the laborato-
ry but may be absent in ambulatory studies, 10
A small minority of patients will not be or may be present in asymptomatic subjects."
relieved with the empiric treatments outlined Anorectal manometry also determines the
above. These patients should be referred to a presence of the recto-anal inhibitory reflex
specialist or a tertiary center for manometric (ie, anal sphincter relaxation in response to
and radiologic tests to determine colonic tran- rectal distension). Absence of this reflex rais-
sit and anorectal function. What information es suspicion of Hirschsprung disease (congeni-
can be gained from these tests and how that tal megacolon), which is usually diagnosed in
information guides treatment are discussed infancy but can be observed in older
below. patients. 12 Patients with megarectum require
large volumes to distend the rectum before the
Osmotic Testing colonic transit reflex can be elicited.
Colonic transit is usually measured by count-
laxatives are ing a fixed number of ingested radiopaque Balloon expulsion
generally safe, markers over several days. Two variations of This is a simple test in which the patient
this test are commonly used. In one, the attempts to expel air-filled or water-filled bal-
but avoid in patient ingests 20 markers and then undergoes loons of specific volumes, while lying on the
patients with abdominal flat-plate radiography 6 days later, left side or sitting on a commode. T h e inabil-
which should show 20% or fewer of the mark- ity to expel a balloon can be seen in associa-
renal ers in the colon. 7 tion with pelvic floor dysfunction or anatomi-
insufficiency or In the other method, markers are ingested cal abnormalities such as a large rectocele or
on 3 consecutive days and radiographs are rectal intussusception or prolapse. 13>14
on a low-salt obtained on days 4 and 7. 8 This allows both
diet total and segmental colonic transit time to be Defecography
quantified. For adults, the upper limit of nor- Defecography involves the instillation of arti-
mal for total colonic transit is approximately ficial stool (eg, barium thickened to approxi-
70 hours. Colonic transit is correlated with mate the consistency of stool) into the rec-
bowel movements recorded by the patient. tum, 15 then recording fluoroscopic images on
Both tests require a high-fiber diet and the videotape during defecation. This is particu-
avoidance of laxatives. T h e test is ordered for larly helpful in documenting a rectocele or
patients whose chief complaint is infrequent rectal intussusception or prolapse. T h e test is
defecation. Documentation of prolonged used particularly in female patients who
colonic transit is mandatory prior to contem- require vaginal digital pressure for evacuation
plating colectomy, which is the ultimate treat- or who are unable to expel rectal balloons.
ment for severe constipation. Also, patients However, rectocele is common in asympto-
42 C L E V E L A N D C L I N I C J O U R N A L OF M E D I C I N E VOLUME 66 • NUMBER 1 JANUARY 1999
Downloaded from www.ccjm.org on January 29, 2022. For personal use only. All other uses require permission.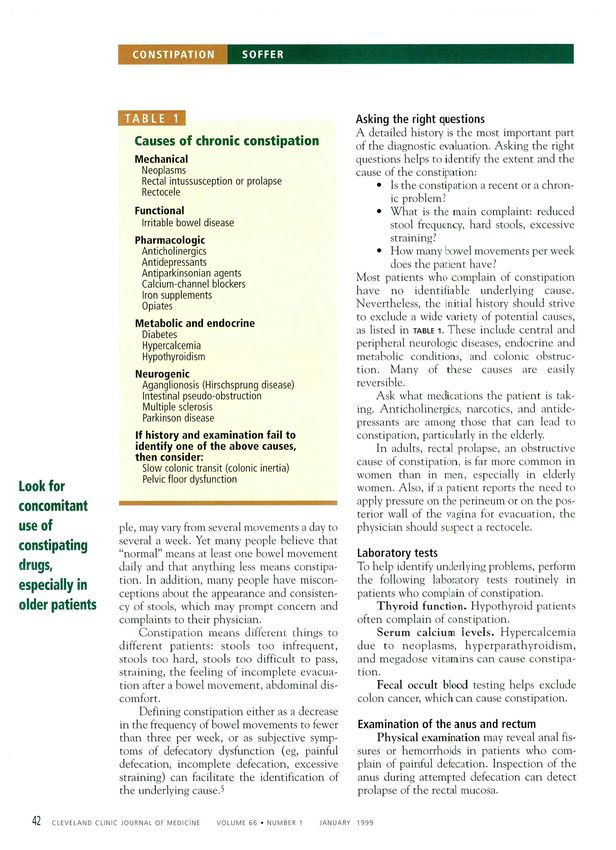
matic subjects, and rectocele does not neces- pation is removal of the colon. The most com-
sarily cause constipation, particularly when it mon approach is subtotal colectomy and ileo-
is less than 2 cm in size. 16,17 rectal anastomosis. While less radical tech-
Changes in the anorectal angle from rest- niques have been used (ileosigmoid anastomo-
ing to squeezing and straining, as well as rec- sis, colorectal anastomosis, left-sided colecto-
tal emptying, may reflect obstructed defeca- my), the more extensive resection provides the
tion. However, the findings may not be specif- best overall results. 23 A notable exception is
ic and are seen in asymptomatic subjects. 1 8 ' 1 9 segmental resection of the sigmoid colon in
Also, normal variation in the anorectal angle cases of megasigmoid 24 or sigmoidocele. 25
and its measurements limit the usefulness of With careful selection of patients, success
defecographic testing for documenting pelvic rates of 50% to 100% can be a c h i e v e d . ^ - 3 0
floor dysfunction. 16,17,20 T h e main complication is small bowel
obstruction, which can occur in about 10% of
• TREATMENTS FOR PATIENTS patients. Diarrhea and fecal incontinence
WITH SEVERE CONSTIPATION after the operation tend to improve with time.
T h e most appropriate candidates for
Few patients with constipation have anatom- surgery are those with chronic disabling symp-
ical defects such as rectocele or prolapse, con- toms related to constipation refractory to
ditions treated surgically in adults. Most often, medical therapy, who have documented slow
after the above tests, patients are categorized colonic transit in the absence of dysmotility
as having slow-transit constipation, pelvic involving other segments of the gut and, in
floor dysfunction with or without slow-transit particular, intestinal pseudo-obstruction.
constipation, or functional constipation and While patients with slow-transit constipation
irritable bowel syndrome. have a very good outcome after colectomy,
improvement is limited in those with evi-
Slow-transit constipation dence of proximal gut dysmotility. 31 Thus,
T h e typical patient with slow-transit consti- evaluation of gastric motility or small-bowel
pation has no urge for a bowel movement for motility are advised as part of the preoperative
more than 3 days, followed by bloating, dis- evaluation, particularly if symptoms suggest For pelvic floor
upper gut dysmotility (early satiety, nausea,
comfort, and difficult defecation of hard
stools. Approximately 30% of patients with vomiting, abdominal distension).
dysfunction
such symptoms prove to have normal colonic Patients with slow-transit constipation the treatment
transit and have evidence of psychosocial dis-
turbances (eg, anxiety, depression, obsessive-
who also have pelvic floor dysfunction should
of choice is
undergo biofeedback training prior to surgery.
compulsive disorder) on tests such as the However, the presence of pelvic floor dysfunc- retraining with
Minnesota Multiphasic Personality Inventory
(MMPI). 2 1 It is important to review the types
tion may not preclude good results after the
biofeedback
operation. 27 ' 32
of laxatives taken and how they are used. Not Finally, the psychological profile of the
infrequently, patients avoid the use of laxa- patient has an important bearing on the success
tives for a week or more for fear of being of surgery. Constipated patients with anxiety or
habituated. depression may fair poorly after surgery.33
Treatment. Patients should be instructed
on the use of proper amounts of laxatives and Pelvic f l o o r d y s f u n c t i o n
when to take them. It is not necessary to have T h e typical patient with pelvic floor dysfunc-
a bowel movement every day, and an adequate tion is a woman who reports unsuccessful
amount of laxative taken every 2 to 3 days attempts at defecation in spite of a normal
may be sufficient for most patients. urge. Each of the physiological tests described
Misoprostol (prostaglandin E-l analog) above can suggest the presence of the disorder,
can be helpful in some patients, 22 but should but no single test is diagnostic. Consequently,
be used with care in females of childbearing in making the diagnosis, the physician consid-
potential, because it can cause abortion. ers the history and supports it with a few tests
T h e decisive treatment for severe consti- such as balloon expulsion and electromyogra-
C L E V E L A N D CLINIC J O U R N A L OF M E D I C I N E V O L U M E 66 • NUMBER 1 JANUARY 1 9 9 9 39
Downloaded from www.ccjm.org on January 29, 2022. For personal use only. All other uses require permission.
CONSTIPATION SOFFER
phy. Negative results exclude pelvic floor dys- T h e current t r e a t m e n t of choice is
function, whereas a positive test points to an retraining with biofeedback. W i t h the use of
abnormality and is supplemented by a manometric probes, electromyography, or
defecogram to exclude anatomical abnormali- both, patients are taught to improve anorec-
ties as described above. tal function by watching their electromyo-
Treatment. In the past, attempts were graphic or pressure profiles on a monitor.
made to diminish the contractile capacity of Patients may require a few sessions, each last-
the sphincter, either surgically by dividing the ing 30 to 60 minutes. Short-term improve-
puborectalis at different anatomical loca- ment following biofeedback is observed in
t i o n s , , 3 5
5 4 or by myectomy, 36 or medically with approximately two thirds of patients, 3 S but
botulinum A toxin. 37 These interventions pro- data from long-term follow-up is scant.
duce only partial success and result in some Biofeedback is safe and painless, but it is
incontinence and have generally been aban- time-consuming and requires dedicated and
doned. experienced personnel. •
• REFERENCES Dis Sci 1993; 38:353-358.
1. Sonnenberg A, Koch TR. Epidemiology of constipation in the United 21. Wald A, Burgio K, Holeva K, Locher J. Psychological evaluation of
States. Dis Colon Rectum 1989; 32:1-8. patients with severe idiopathic constipation: which Instrument to use.
2. Sandler RS, Jordon MC, Skelton BJ. Demographic and dietary determi- Am J Gastroenterol 1992; 87:977-980.
nants of constipation in the U.S. population. Am J Publ Health 1990; 22. Soffer EE, Launspach J, Metcalf A. The effects of misoprostol on
80(2): 185-189. patients with severe chronic constipation. Dig Dis Sci 1994; 39:929-933.
3. Thompson WG, Creed F, Drossman DA, Heaton KW, Mazzacca G. 23. Pfeifer J, Agachan F, Wexner S. Surgery for constipation: a review. Dis
Functional bowel disease and functional abdominal pain. Colon Rectum 1996; 39:444-460.
Gastroenterology International 1992; 5:75-91. 24. Belliveau P, Goldberg SM, Rothenberger DA, Nivatvongs S. Idiopathic
4. Drossman DA, Li Z, Andruzzi E, et al. US householder survey of func- acquired megacolon: the value of subtotal colectomy. Dis Colon
tional gastrointestinal disorders. Prevalence, soclodemography, and Rectum 1982; 25:118-121.
health impact. Dig Dis Sci 1993;38:1569-1580. 25. Jorge J, Yang Y, Wexner S. Incidence and clinical significance of sig-
5. Falk GW. Constipation. In: Achkar E, Farmer RG, Fleshier B, editors. moidoceles as determined by a new classification system. Dis Colon
Clinical Gastroenterology. Philadelphia: Lea and Febiger, 1992; 70-81. Rectum 1994; 37:1112-1117.
6. Orchard JL, Lawson R. Severe colitis induced by soap enemas. South 26. Leon S, Krishnamurthy S, Shuffler M. Subtotal colectomy for severe
Med J 1986; 79:1459-1460. idiopathic constipation. Dig Dis Sci 1987; 32:1249-1254.
7. Hinton JM, Lennard-Jones JE, Young AC. A new method for studying 27. Kamm M, Hawley P, Lennard-Jones J. Outcome of colectomy for
gut transit times using radioopaque markers. Gut 1969; 10:842-847. severe idiopathic constipation. Gut 1998; 29:969-973.
8. Metcalf AM, Phillips SF, Zinsmeister AR, et al. Simplified assessment of 28. Beck D, Fazio V, Jagelman D, Lavery IC. Surgical management of
segmental colonic transit. Gastroenterology 1987; 92:40-47. colonic inertia. South Med J 1989; 82:305-309.
9. Caruana BJ, Hinds JP, Freimanis M, et al. Psychological and physiologi- 29. Yoshioka K, Keighley M. Clinical results of colectomy for severe consti-
cal characteristics of patients with severe idiopathic constipation. pation. Br J Surg 1989; 76:600-604.
Gastroenterology 1989; 97:932-937. 30. Piccirillo M, Reissman P, Carnavos R, Wexner S. Colectomy as treat-
10. Duthie GS, Bartolo DCC. Anismus: the cause of constipation? Results ment for constipation in selected patients. Br J Surg 1995; 82:898-901.
of investigation and treatment. World J Surg 1992; 16:831-835. 31. Redmond J, Smith G, Barofsky I, Ratych R, Goldsborough D, Schuster
11. Voderholzer WA, Neuhaus DA, Klauser AG, Tzavella K, Muller-Lissner M. Physiological tests to predict long-term outcome of total abdcmi
SA, Schindbeck NE. Paradoxical sphincter contraction is rarely indica- nal colectomy for intractable constipation. Am J Gastroenterol 1995;
tive of anismus. Gut 1997; 41:258-262. 90:748-753.
12. Anuras S, Hade JE, Soffer EE, et al. Natural history of adult 32. Pemberton J, Rath D, llstrup D. Evaluation and surgical treatment of
Hirschsprung's disease. J Clin Gastroenterol 1984; 6:205-210. severe chronic constipation. Ann Surg 1991; 214:403-413.
13. Barnes PRH, Lennard-Jones JE. Balloon expulsion from the rectum in 33. Fisher S, Breckan K, Andrews H, Keighley M. Psychiatric screeninç for
constipation of different types. Gut 1985; 26:1049-1052. patients with fecal Incontinence on chronic constipation referred for
14. Fleshman JW, Dreznik Z, Cohen E, Fry RD, Kodner IJ. Balloon expulsion surgical treatment. Br J Surg 1998; 76:352-355.
test facilitates diagnosis of pelvic floor outlet obstruction due to non- 34. Barnes PR, Hawley PR, Preston DM, Lennard-Jones JE. Experience of
relaxing puborectalis muscle. Dis Colon Rectum 1992; 35:1019-1025. posterior division of the puborectalis muscle in the management of
15. Finlay IG, Bartolo DCC, Bartram Cl, et al. Proctography (symposium). chronic constipation. Br J Surg 1985; 72:475-477.
Int J Colorect Dis 1988; 3:67-69. 35. Kamm MA, Hawley PR, Lennard-Jones JE. Lateral division of the pub-
16. Bartram CI, Turnbull GK, Lennard-Jones JE. Evacuation proctography: orectalis muscle in the management of severe constipation. Br J Sjrg
An investigation of rectal expulsion in 20 subjects without defecatory 1988; 75:661-663.
disturbance. Gastrointest Radiol 1988; 13:72-80. 36. Yoshioka K, Keighley MR. Anorectal myectomy for outlet obstruclon.
17. Shorvon PJ, McHugh F, Diamant NE, et al. Defecography in normal Br J Surg 1987; 74:373-376.
volunteers: Results and implications. Gut 1989; 30:1737-1749. 37. Hallan RI, Williams NS, Melling J, et al. Treatment of anismus in
18. Jones PN, Lubowski, DZ, Swash M„ Henry MM. Is paradoxical contrac- intractable constipation with botulinum A toxin. Lancet. 1988;
tion of the puborectalis muscles of functional importance? Dis Colon 2:714-717.
Rectum 1987; 30:667-670. 38. Enck P. Biofeedback training in disordered defecation. Dig Dis Sci
19. Miller R, Duthie GS, Bartolo DCC, et al. Anismus in patients with nor- 1993; 38:1953-1960.
mal and slow transit constipation. Br J Surg 1991; 78:690-692. ADDRESS: Edy E. Soffer MD, Department of Gastroenterology-HepatoJogy,
20. Wald A, Jafri R, Rehder J, Holeva K. Scintigraphic studies of rectal 540, The Cleveland Clinic Foundation, 9500 Euclid Avenue, Cleveland, OH
emptying in patients with constipation and defecatory difficulty. Dig 44195.
42 C L E V E L A N D C L I N I C J O U R N A L OF M E D I C I N E VOLUME 66 • NUMBER 1 JANUARY 1999
Downloaded from www.ccjm.org on January 29, 2022. For personal use only. All other uses require permission.You can also read

















































