Colchicine dans le traitement du coronarien
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Colchicine dans le traitement du
coronarien
Aucun conflit d’intérêt en la matière

La maladie coronaire est aussi une maladie inflammatoire des artères coronaires

Les arguments pour la théorie
inflammatoire
de l’athéro-thrombose coronaire
Arguments pour théorie inflammatoire de l’athéro-thrombose
1) Augmentation de l’incidence des infarctus du
myocarde après certaines épidémies virales
The n e w e ng l a n d j o u r na l of m e dic i n e
Original Article
Acute Myocardial Infarction after
Laboratory-Confirmed Influenza Infection
Jeffrey C. Kwong, M.D., Kevin L. Schwartz, M.D., Michael A. Campitelli, M.P.H.,
Hannah Chung, M.P.H., Natasha S. Crowcroft, M.D., Timothy Karnauchow, Ph.D.,
Kevin Katz, M.D., Dennis T. Ko, M.D., Allison J. McGeer, M.D.,
Dayre McNally, M.D., Ph.D., David C. Richardson, M.D.,
Laura C. Rosella, Ph.D., M.H.Sc., Andrew Simor, M.D.,
Marek Smieja, M.D., Ph.D., George Zahariadis, M.D.,
and Jonathan B. Gubbay, M.B., B.S., M.Med.Sc. Ontario/Canada
A BS T R AC T
BACKGROUND Acute MI after Influenza. NEJM 2018
Acute myocardial infarction can be triggered by acute respiratory infections. Previ- From
Original Article
Acute Myocardial Infarction after
Laboratory-Confirmed Influenza Infection
Jeffrey C. Kwong, M.D., Kevin L. Schwartz, M.D., Michael A. Campitelli, M.P.H.,
Hannah Chung, M.P.H., Natasha S. Crowcroft, M.D., Timothy Karnauchow, Ph.D.,
Kevin Katz, M.D., Dennis T. Ko, M.D., Allison J. McGeer, M.D.,
Dayre McNally, M.D., Ph.D., David C. Richardson, M.D.,
Laura C. Rosella, Ph.D., M.H.Sc., Andrew Simor, M.D.,
Marek Smieja, M.D., Ph.D., George Zahariadis, M.D.,
rction after Influenza and Jonathan B. Gubbay, M.B., B.S., M.Med.Sc.
A BS T R AC T
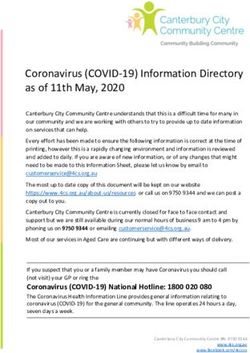
Table 2. Incidence Ratios for Acute Myocardial Infarction after Laboratory-
BACKGROUND
Confirmed Influenza Infection.* Acute myocardial infarction can be triggered by acute respiratory infections. Previ- From the Institute for Clinical Evaluative
ous studies have suggested an association between influenza and acute myocar- Sciences (J.C.K., K.L.S., M.A.C., H.C.,
D.T.K., L.C.R.), Public Health Ontario
dial infarction, but those studies used nonspecific measures of influenza infection (J.C.K., K.L.S., N.S.C., L.C.R., J.B.G.),
or study designs that Incidence Ratio
were susceptible to bias. We evaluated the association be- Dalla Lana School of Public Health
Variable tween laboratory-confirmed (95% CI) infection and acute myocardial infarction.
influenza (J.C.K., K.L.S., N.S.C., A.J.M., L.C.R.),
and the Departments of Family and Com-
munity Medicine (J.C.K.) and Laboratory
METHODS
Primary analysis: risk interval, days 1–7 6.05 case-series
We used the self-controlled (3.86–9.50)design to evaluate the association between
Medicine and Pathobiology (N.S.C., K.K.,
A.J.M., A.S., J.B.G.), University of Toronto,
laboratory-confirmed influenza infection and hospitalization for acute myocardial University Health Network (J.C.K.), North
Days 1–3 6.30 high-specificity
infarction. We used various (3.25–12.22)laboratory methods to confirm influ- York General Hospital (K.K.), Sunnybrook
Health Sciences Centre (D.T.K., A.S.), Sinai
enza infection in respiratory specimens, and we ascertained hospitalization for Health System (A.J.M.), and the Hospital
Days 4–7 5.78 from
acute myocardial infarction (3.17–10.53)
administrative data. We defined the “risk inter- for Sick Children (J.B.G.), Toronto, Chil-
dren’s Hospital of Eastern Ontario (T.K.,
val” as the first 7 days after respiratory specimen collection and the “control in-
Days 8–14 0.60
terval” as 1 year before and 1(0.15–2.41)
year after the risk interval.
D.M.) and the Department of Pathology
and Laboratory Medicine, University of
Ottawa (T.K.), Ottawa, William Osler
Days 15–28 RESULTS 0.75 (0.31–1.81) Health System, Brampton, ON (D.C.R.),
We identified 364 hospitalizations for acute myocardial infarction that occurred McMaster University, Hamilton, ON
Sensitivity analyses within 1 year before and 1 year after a positive test result for influenza. Of these,
(M.S.), London Health Sciences Centre,
London, ON (G.Z.), and the Newfound-
20 (20.0 admissions per week) occurred during the risk interval and 344 (3.3 ad- land and Labrador Public Health Labora-
Controlled for calendar month 6.19 (3.88–9.88)
missions per week) occurred during the control interval. The incidence ratio of an tory, St. John’s (G.Z.) — all in Canada.
Address reprint requests to Dr. Kwong at
admission for acute myocardial infarction during the risk interval as compared the Institute for Clinical Evaluative Sci-
Control interval limited to postexposure observation 8.08
with the control interval was(5.04–12.95)
6.05 (95% confidence interval [CI], 3.86 to 9.50). No ences, G1 06, 2075 Bayview Ave., Toronto,
time increased incidence was observed after day 7. Incidence ratios for acute myocar- ON M4N 3M5, Canada, or at jeff.kwong@
utoronto.ca.
dial infarction within 7 days after detection of influenza B, influenza A, respira-
Control interval limited to preexposure observation time virus, and
tory syncytial 4.84 (3.06–7.65)
other viruses were 10.11 (95% CI, 4.37 to 23.38), 5.17 N Engl J Med 2018;378:345-53.
DOI: 10.1056/NEJMoa1702090
(95% CI, 3.02 to 8.84), 3.51 (95% CI, 1.11 to 11.12), and 2.77 (95% CI, 1.23 to 6.24), Copyright © 2018 Massachusetts Medical Society.
Control interval limited to 2 months before and after
respectively. 5.01 (3.04–8.27)
influenza detection CONCLUSIONS
We found a significant association between respiratory infections, especially
Acute
Includes AMI cases with specimen obtainedinfluenza,
during MImyocardial
and acute after
4.45 Influenza.
(2.85–6.97)
infarction. (Funded byNEJM 2018
the Canadian Institutes
admission of Health Research and others.)
Induction interval†
Original Article
Acute Myocardial Infarction after
Laboratory-Confirmed Influenza Infection
Jeffrey C. Kwong, M.D., Kevin L. Schwartz, M.D., Michael A. Campitelli, M.P.H.,
Hannah Chung, M.P.H., Natasha S. Crowcroft, M.D., Timothy Karnauchow, Ph.D.,
Kevin Katz, M.D., Dennis T. Ko, M.D., Allison J. McGeer, M.D.,
Dayre McNally, M.D., Ph.D., David C. Richardson, M.D.,
Laura C. Rosella, Ph.D., M.H.Sc., Andrew Simor, M.D.,
Marek Smieja, M.D., Ph.D., George Zahariadis, M.D.,
rction after Influenza and Jonathan B. Gubbay, M.B., B.S., M.Med.Sc.
A BS T R AC T
Table 2. Incidence Ratios for Acute Myocardial Infarction after Laboratory-
BACKGROUND
Confirmed Influenza Infection.* Acute myocardial infarction can be triggered by acute respiratory infections. Previ- From the Institute for Clinical Evaluative
ous studies have suggested an association between influenza and acute myocar- Sciences (J.C.K., K.L.S., M.A.C., H.C.,
D.T.K., L.C.R.), Public Health Ontario
dial infarction, but those studies used nonspecific measures of influenza infection (J.C.K., K.L.S., N.S.C., L.C.R., J.B.G.),
or study designs that Incidence Ratio
were susceptible to bias. We evaluated the association be- Dalla Lana School of Public Health
Variable tween laboratory-confirmed (95% CI) infection and acute myocardial infarction.
influenza (J.C.K., K.L.S., N.S.C., A.J.M., L.C.R.),
and the Departments of Family and Com-
munity Medicine (J.C.K.) and Laboratory
METHODS
Primary analysis: risk interval, days 1–7 6.05 case-series
We used the self-controlled (3.86–9.50)design to evaluate the association between
Medicine and Pathobiology (N.S.C., K.K.,
A.J.M., A.S., J.B.G.), University of Toronto,
laboratory-confirmed influenza infection and hospitalization for acute myocardial University Health Network (J.C.K.), North
Days 1–3 6.30 high-specificity
infarction. We used various (3.25–12.22)laboratory methods to confirm influ- York General Hospital (K.K.), Sunnybrook
Health Sciences Centre (D.T.K., A.S.), Sinai
enza infection in respiratory specimens, and we ascertained hospitalization for Health System (A.J.M.), and the Hospital
Days 4–7 5.78 from
acute myocardial infarction (3.17–10.53)
administrative data. We defined the “risk inter- for Sick Children (J.B.G.), Toronto, Chil-
dren’s Hospital of Eastern Ontario (T.K.,
val” as the first 7 days after respiratory specimen collection and the “control in-
Days 8–14 0.60
terval” as 1 year before and 1(0.15–2.41)
year after the risk interval.
D.M.) and the Department of Pathology
and Laboratory Medicine, University of
Ottawa (T.K.), Ottawa, William Osler
Days 15–28 RESULTS 0.75 (0.31–1.81) Health System, Brampton, ON (D.C.R.),
We identified 364 hospitalizations for acute myocardial infarction that occurred McMaster University, Hamilton, ON
Sensitivity analyses within 1 year before and 1 year after a positive test result for influenza. Of these,
(M.S.), London Health Sciences Centre,
London, ON (G.Z.), and the Newfound-
20 (20.0 admissions per week) occurred during the risk interval and 344 (3.3 ad- land and Labrador Public Health Labora-
Controlled for calendar month 6.19 (3.88–9.88)
missions per week) occurred during the control interval. The incidence ratio of an tory, St. John’s (G.Z.) — all in Canada.
Address reprint requests to Dr. Kwong at
admission for acute myocardial infarction during the risk interval as compared the Institute for Clinical Evaluative Sci-
Control interval limited to postexposure observation 8.08
with the control interval was(5.04–12.95)
6.05 (95% confidence interval [CI], 3.86 to 9.50). No ences, G1 06, 2075 Bayview Ave., Toronto,
time increased incidence was observed after day 7. Incidence ratios for acute myocar- ON M4N 3M5, Canada, or at jeff.kwong@
6 x plus de risque de presenter un IDM après une grippe
utoronto.ca.
dial infarction within 7 days after detection of influenza B, influenza A, respira-
Control interval limited to preexposure observation time virus, and
tory syncytial 4.84 (3.06–7.65)
other viruses were 10.11 (95% CI, 4.37 to 23.38), 5.17 N Engl J Med 2018;378:345-53.
DOI: 10.1056/NEJMoa1702090
(95% CI, 3.02 to 8.84), 3.51 (95% CI, 1.11 to 11.12), and 2.77 (95% CI, 1.23 to 6.24), Copyright © 2018 Massachusetts Medical Society.
Control interval limited to 2 months before and after
respectively. 5.01 (3.04–8.27)
influenza detection CONCLUSIONS
We found a significant association between respiratory infections, especially
Includes AMI cases with specimen obtainedinfluenza,
during and acute myocardial
4.45 (2.85–6.97)
infarction. (Funded by the Canadian Institutes
admission of Health Research and others.)
Induction interval†
cardiac rehabilitation is effective in reducing total- and CV mortality
and hospital admissions,276 whereas effects on total MI or revascular-
277,278
ization (CABG or PCI) are less clear, especially in the long term.
ESC GUIDELINES
European Heart Journal (2013) 34, 2949–3003
Evidence also points towards beneficial effects on health-related
doi:10.1093/eurheartj/eht296
quality of life (QoL). In selected sub-groups, centre-based cardiac re-
2013 ESC
habilitation mayguidelines onfor
be substituted thehome-based
management rehabilitation, which
of stable coronary
is non-inferior. artery disease
Patient participation in cardiac rehabilitation remains
far The
tooTask
low, particularly
Force in women,
on the management thecoronary
of stable elderlyartery
and disease
the socio-
in of the European Society of Cardiology
economically deprived, and could benefit from systematic referral.
be Task Force Members: Gilles Montalescot* (Chairperson) (France), Udo Sechtem*
(Chairperson) (Germany), Stephan Achenbach (Germany), Felicita Andreotti (Italy),
he Chris Arden (UK), Andrzej Budaj (Poland), Raffaele Bugiardini (Italy), Filippo Crea
7.1.2.11 Influenza vaccination
(Italy), Thomas Cuisset (France), Carlo Di Mario (UK), J. Rafael Ferreira (Portugal),
m-
An annual influenza vaccination is recommended for patients with
Bernard J. Gersh (USA), Anselm K. Gitt (Germany), Jean-Sebastien Hulot (France),
Nikolaus Marx (Germany), Lionel H. Opie (South Africa), Matthias Pfisterer
279,280
CAD, especially the elderly.
(Switzerland), Eva Prescott (Denmark), Frank Ruschitzka (Switzerland), Manel Sabaté
(Spain), Roxy Senior (UK), David Paul Taggart (UK), Ernst E. van der Wall
(Netherlands), Christiaan J.M. Vrints (Belgium).
ESC Committee for Practice Guidelines (CPG): Jose Luis Zamorano (Chairperson) (Spain), Stephan Achenbach
7.1.2.12
(Germany),Hormone
Helmut Baumgartnerreplacement therapy
(Germany), Jeroen J. Bax (Netherlands), Héctor Bueno (Spain), Veronica Dean
(France), Christi Deaton (UK), Cetin Erol (Turkey), Robert Fagard (Belgium), Roberto Ferrari (Italy), David Hasdai
For(Israel),
decades,Arno W. Hoesevidence from
(Netherlands), Paulus epidemiological
Kirchhof (Germany/UK), Juhani Knuutiand laboratory
(Finland), studies
Philippe Kolh (Belgium),
Patrizio Lancellotti (Belgium), Ales Linhart (Czech Republic), Petros Nihoyannopoulos (UK), Massimo F. Piepoli (Italy),
ns, led Piotr
usPonikowski
to believe thatWijnscirculating
(Belgium), Stephanoestrogens had a beneficial effect
(Poland), Per Anton Sirnes (Norway), Juan Luis Tamargo (Spain), Michal Tendera (Poland),
Adam Torbicki (Poland), William Windecker (Switzerland).
be on the risk of CVD and that this could be transferred to the benefits
Document Reviewers: Juhani Knuuti (CPG Review Coordinator) (Finland), Marco Valgimigli (Review Coordinator)
(Italy), Héctor Bueno (Spain), Marc J. Claeys (Belgium), Norbert Donner-Banzhoff (Germany), Cetin Erol (Turkey),
in Herbert Frank (Austria), Christian Funck-Brentano (France), Oliver Gaemperli (Switzerland),
of hormone replacement therapy (HRT). However, results from
José R. Gonzalez-Juanatey (Spain), Michalis Hamilos (Greece), David Hasdai (Israel), Steen Husted (Denmark),
% Stefan K. James (Sweden), Kari Kervinen (Finland), Philippe Kolh (Belgium), Steen Dalby Kristensen (Denmark),
La 1 ere étude randomisée sur l’effet de la vaccination
grippale chez des coronariens
SweedenVaccin grippal et MACE post SCA
Vaccin grippal et MACE post SCA
Vaccination grippale chez le coronarien: IB
Plus généralement: toute infection aigue augmente le risque d’évènement cardiovasculaire ..parfois pendant longtemps
Arguments pour théorie inflammatoire de l’athéro-thrombose
Corrélation
CRP US / IL 1 et IL 6 et évènements coronariensLeft, Relationship of baseline plasma levels of high-sensitivity C-reactive protein (hsCRP) to
risks of future myocardial infarction, stroke, and cardiovascular death in the prospective
Physicians’ Health Study among those randomly allocated to aspirin or placebo.
Physicians’ Health Study en Prévention primaire
Paul M Ridker Circ Res. 2016;118:145-156
Copyright © American Heart Association, Inc. All rights reserved.Left, Relationship of baseline plasma levels of high-sensitivity C-reactive protein (hsCRP) to
risks of future myocardial infarction, stroke, and cardiovascular death in the prospective
Physicians’ Health Study among those randomly allocated to aspirin or placebo.
Plus la CRPus est élevée plus le risqué d’IDM augmente
Paul M Ridker Circ Res. 2016;118:145-156
Copyright © American Heart Association, Inc. All rights reserved.Relationship of plasma levels of interleukin-6 (IL-6) to future risks of cardiovascular disease
in 25 prospective epidemiologic cohorts.
Paul M Ridker Circ Res. 2016;118:145-156Relationship of plasma levels of interleukin-6 (IL-6) to future risks of cardiovascular disease
in 25 prospective epidemiologic cohorts.
Paul M Ridker Circ Res. 2016;118:145-156
Plus l’IL6 est élevée plus le risqué d’IDM augmenteArguments pour théorie inflammatoire de l’athéro-thrombose
La rupture de plaque est souvent le fait
d’une “poussée systémique” d’athéro-thromboseMultiple atherosclerotic plaque rupture in acute coronary syndrome.
A three vessel intravascular ultrasound study.
Rioufol G et al. Circulation 2002;106:804-8.
C
B
ALa rupture de plaque est souvent le fait
d’une “poussée systémique” d’athéro-thrombose
Une seconde plaque rompue
Dans 79% des cas !!
Une 3ème plaque rompue
Dans 12.5% des cas !!Arguments pour théorie inflammatoire de l’athéro-thrombose
Les statines n’agissent pas seulement par l’effet
hypolipémiant (= fibrates)Arguments pour théorie inflammatoire de l’athéro-thrombose
Essai JUPITER
Les patients avec taux de LDL bas mais CRP
élevée bénéficiaient plus de la statineArguments pour théorie inflammatoire de l’athéro-thrombose
Les maladies inflammatoires “chroniques”
présentent un sur-risque de coronaropathieLe risque cardiovasculaire est augmenté au cours des
rhumatismes inflammatoires (PR -SPA)
La PR est un facteur de risque CV aussi important que le diabète
décorto the The results also persisted when con-
er ma- trolling for the major risk factors for MI.
However, it is possible that unknown Risque coronarien du psoriasis sévère
mited
n bias
cribed Figure. Adjusted Relative Risk of Myocardial
is and Infarction in Patients With Psoriasis Based on
Patient Age
d and
efined 10 Severe Psoriasis
Relative Risk (95% Confidence Interval)
ascer- Mild Psoriasis
in the
d con-
lected
practi-
nd the
nsitiv-
more 1.0
ng out
s were 0.5
20 30 40 50 60 70 80
which
Age, y
of their
nsure Adjusted relative risk is shown on a log scale.Concept Inflammatoire de la
coronaropathie
Foyer dentaire à
éradiquerSi vous voulez démontrer un concept
Facteur (l’inflammation) associé à un surisque
cardiaque….
Il faut démontrer que la suppression de ce
facteur à un impact positif sur le suri-risque
cardiaqueArguments pour théorie inflammatoire de l’athéro-thrombose
L’effet présumé de certains traitements anti-
inflammatoiresCantos: la demonstration du concept
Anti-Inflammatory Therapy with Canakinumab for
Atherosclerotic Disease
La plus belle étude en cardiologie
depuis Framingham
Eugène Braunwald
Paul M Ridker, MD, MPH
Eugene Braunwald Professor of Medicine
Brigham and Women’s Hospital,
Harvard Medical School, Boston MA, USA
on behalf of the worldwide investigators and participants in the
Canakinumab Anti-Inflammatory Thrombosis Outcomes Study (CANTOS)
Ridker ACC 2017From CRP to IL-6 to IL-1: Moving Upstream to Identify Novel Targets for Atheroprotection
Canakinumab
Ridker PM. Circ Res 2016;118:145-156.
Ridker ESC 2017Canakinumab Anti-Inflammatory Thrombosis Outcomes Study (CANTOS)
Stable CAD (post MI) N = 10,061
On Statin, ACE/ARB, BB, ASA 39 Countries
Persistent Elevation April 2011 - June 2017
of hsCRP (> 2 mg/L) 1490 Primary Events
Randomized Randomized Randomized Randomized
Canakinumab 50 mg Canakinumab 150 mg Canakinumab 300 mg Placebo
SC q 3 months SC q 3 months SC q 3 months* SC q 3 months
Primary CV Endpoint: Nonfatal MI, Nonfatal Stroke, Cardiovascular Death (MACE)
Key Secondary CV Endpoint: MACE + Unstable Angina Requiring Unplanned Revascularization (MACE+)
Critical Non-Cardiovascular Safety Endpoints: Cancer and Cancer Mortality, Infection and Infection Mortality
Ridker ESC 2017Cantos: la demonstration du concept
CANTOS: Canakinumab et MACE
Paul M Ridker Circ Res. 2016;118:145-156
Copyright © American Heart Association, Inc. All rights reserved.Paul M Ridker Circ Res. 2016;118:145-156
Copyright © American Heart Association, Inc. All rights reserved.Morphologie de la plaque avant et
12 mois de colchicine
Nette diminution du « noyau actif »Colchicine /coronaires > 12 000 pts randomisés loDoCO Colcot
Colchicine /coronaires > 12 000 pts randomisés
n Situation clinique
COLCOT 4745 SCA
LODOCO2 5522 Coronaropathie stable22% reduction risk for MI
p=0.00546% reduction risk for stroke p=0.009
23% reduction risk for coronary revascularisation p
18% reduction risk for CV
death p=0.3420 cp: 2.8 Euro 0.07 Euro par jour
Figure 2 Colchicine anti-inflammatory actions start with the
interference with microtubule assembly and function and ...
Eur Heart J, Volume 42, Issue 28, 21 July 2021, Pages 2745–2760, https://doi.org/10.1093/eurheartj/ehab221
The content of this slide may be subject to copyright: please see the slide notes for details.The central mechanism of the anti-inflammatory action of colchicine
is the inhibition of microtubule function ...
Eur Heart J, Volume 42, Issue 28, 21 July 2021, Pages 2745–2760, https://doi.org/10.1093/eurheartj/ehab221
The content of this slide may be subject to copyright: please see the slide notes for details.Pourquoi en avez-vous peu (ou pas) entendu parler ?
Pourquoi en avez-vous peu (ou pas) entendu parler ?
20 cp: 2.8 Euro
0.07 Euro par jourLes reco
Priorisation des effets thérapeutiques chez le
coronarien stable à l’ère moderne
• AAP • AOD (Riva 2.5 dans
• Statine Compass)
• BB
• IEC/ARA 2 • Colchicine
• Fibrates • Statine
• Omega 3
• PCSK9 • AAP
• Ca(-)
• AOD
• ….Colchicine in coronary disease Eur Heart J, Volume 42, Issue 28, 21 July 2021, Pages 2765–2775, https://doi.org/10.1093/eurheartj/ehab115 The content of this slide may be subject to copyright: please see the slide notes for details.
Figure 5 Risk of pericarditis in patients treated with or without
colchicine in different settings (acute, recurrent ...
Eur Heart J, Volume 42, Issue 28, 21 July 2021, Pages 2745–2760, https://doi.org/10.1093/eurheartj/ehab221
The content of this slide may be subject to copyright: please see the slide notes for details.Figure 3 Colchicine uptake occurs in the ileum and jejunum. The
drug is metabolized by the liver through cytochrome ...
Eur Heart J, Volume 42, Issue 28, 21 July 2021, Pages 2745–2760, https://doi.org/10.1093/eurheartj/ehab221
The content of this slide may be subject to copyright: please see the slide notes for details.You can also read