CLINICAL PROTOCOL - MUHC - MCH RT
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
CLINICAL PROTOCOL – MUHC
(PROTOCOLE CLINIQUE - CUSM)
Medication included No Medication included
MCH MGH RVH MNH MCI LACHINE
THIS IS NOT A MEDICAL ORDER
Installation and Maintenance of Bubble Nasal Continuous Positive Airway
Title: Pressure (NCPAP) Therapy in the Neonatal Intensive Care Unit (NICU) and
the Resuscitation room in the Birthing Center at the Royal Victoria Hospital.
NICU Oxygen With Love (OWL) Guidelines
Clinical Guideline for Management of Extremely Preterm Infants born less
than 29 weeks and/or less than 1000g in the First 72 hours After Delivery
This document is
attached to: Interprofessional Protocol on Installation and Maintenance of SiPAP®
Clinical Procedure – Protocol for Kangaroo Care in the Pediatric Population
Hand Hygiene Related to patient care – MUHC Policy
1. PURPOSE
Most infants born before 32 weeks gestational age will require some form of respiratory support at
birth. Chronic lung disease secondary to barotrauma and increased oxygen need is a significant
source of long-term morbidity in this population. Bubble nasal continuous positive airway pressure
(bubble NCPAP) is a modality of respiratory support that has been shown to decrease the rates of
chronic lung disease in premature infants that require prolonged respiratory support, in comparison
with other types of NCPAP, non-invasive positive pressure ventilation (NIPPV), or invasive
mechanical ventilation.
Notably, infants born at less than 26 weeks of gestation have high failure rates on bubble NCPAP.
However, results from a large randomized control trial showed a decreased rate of mortality in this
population when given a trial of bubble NCPAP, even if they eventually fail (see Section E. Bubble
NCPAP failure for definitions of failure). Therefore, although many of these infants will require
endotracheal intubation and surfactant administration, an initial trial of bubble NCPAP is always
recommended when possible.
The purpose of the protocol is:
• To assure proper installation and maintenance of bubble NCPAP interface and system
• To harmonize routine care of a patient on bubble NCPAP therapy
2. PROFESSIONALS
• Respiratory Therapists (RRT) from the Montreal Children’s Hospital (MCH) who have
successfully completed an orientation session for installation, routine care, weaning, and
discontinuation of NCPAP.
• Nurses working in the NICU at the MCH who have successfully completed an orientation session
on routine care of a patient receiving NCPAP therapy.
Installation and Maintenance of Bubble NCPAP Therapy in the NICU and the Resuscitation room in the Birthing Center at the RVH
Final September 11th 2018 1
Revision date: September 2022• Physicians and neonatal nurse practitioners (NNP) working in the NICU at the MCH who are
responsible to order the use of any non-invasive respiratory support should be familiar with
indications, monitoring and complications of NCPAP therapy.
3. PATIENT POPULATION
In the Birthing Centre Resuscitation Room at the RVH):
1. Spontaneously breathing premature infants less than 32 weeks gestation
2. Any newborn showing signs of respiratory distress defined as:
• Oxygen needs greater than 21% to maintain appropriate oxygen saturation as per Neonatal
Resuscitation Program(NRP) and OWL Guidelines
• Increased work of breathing defined as the presence of tachypnea, moderate sub-sternal
and/or suprasternal retractions, grunting and / or nasal flaring
• Apnea, bradycardia spells and / or cyanosis
The bubble NCPAP system is recommended as the first choice for newly born infants with the above
criteria unless a pressure of greater than 7 cmH2O is needed.
If NCPAP is provided for 20-30 minutes in the delivery or resuscitation room, admission of the newborn to
the NICU is strongly recommended as to be able to observe the newborn closely.
In the MCH NICU:
1. Spontaneously breathing premature infants less than 32 weeks
2. Immediately post-extubation, in premature infants or in full-term infants based on disease being
treated.
3. Any newborn showing signs of respiratory distress defined as:
• Oxygen needs greater than 21% to maintain appropriate oxygen saturation as per NRP and
OWL Guidelines
• Presence of moderate sub-sternal and/or suprasternal retractions, grunting and / or nasal
flaring
• Apnea, bradycardia spells and / or cyanosis
• Sustained increased in respiratory rate of 20% above normal
4. ELEMENTS OF CLINICAL ACTIVITY
Indications:
Diseases with low Functional Residual Capacity (FRC), such as Respiratory Distress Syndrome
(RDS), Transient Tachypnea of the Newborn (TTN), Pulmonary Edema
Respiratory support post extubation
Atelectasis - prevention or treatment
Apnea of prematurity
Tracheomalacia, or other similar lower airway abnormalities
Neuromuscular weakness with adequate respiratory efforts
Phrenic nerve palsy
Installation and Maintenance of Bubble NCPAP Therapy in the NICU and the Resuscitation room in the Birthing Center at the RVH
Final September 11th 2018 2
Revision date: September 2022Contraindications (includes but not limited to):
Congenital diaphragmatic hernia before surgical repair
Orofacial and upper airway abnormalities, such as bilateral choanal atresia,
Relative contraindications include untreated GI pathologies: obstruction (atresias, malrotation,
volvulus)
Precautions (proceed with caution):
Severe cardiovascular instability (persistent hypotension requiring multiple pressors)
Severe respiratory failure defined by consistent increase in oxygen requirement above 50% (1-
2h), or severe respiratory acidosis defined as PCO2 above 65 with a pH less than 7.20 in two
consecutive blood gases.
Possible complications (includes but not limited to):
Irritation, bleeding, infection or chronic inflammation of the nasal mucosa
Nasal obstruction from secretions or improper position of nasal prongs
Perinasal skin irritation and pressure necrosis
Abdominal distension (“CPAP belly syndrome”)
Feeding intolerance
Progressive Respiratory Failure – may be caused by natural disease progression or improper
follow up of airway care.
Risk of pneumothorax especially with NCPAP levels above 7 cmH2O in extreme preterm infants
during the acute phase of RDS
Misshaping of the head
Equipment needed:
1. Bubble NCPAP system, set up and ready for use.
2. Accessories for nasal interface including bonnet, chin strap, nasal prongs and adhesive upper lip
protection (Cannulaide®), of all sizes.
3. Suction set-up and accessories
4. Disposable measuring tape
a) PROCEDURE FOR BUBBLE NCPAP INITIATION
1. The physician, NNP, nurse and RT will assess newborn for eligibility criteria as outlined above.
2. The physician/NNP will order the NCPAP level to be initiated. It is recommended to begin at 5
cmH2O. Most infants who respond to NCPAP do so with this pressure level.The nasal interface used
with bubble NCPAP should consist of short bi-nasal prongs in a U-shape, with easy visualization and
access to the face unless:
• It is logistically difficult to keep the bubble NCPAP in place, even after all the appropriate
troubleshooting has been done according to the installation and maintenance procedure
below by both the nurse and RT at bedside.
• There is a concern with nasal septal skin irritation or breakdown.
Installation and Maintenance of Bubble NCPAP Therapy in the NICU and the Resuscitation room in the Birthing Center at the RVH
Final September 11th 2018 3
Revision date: September 2022b) PROCEDURE FOR BUBBLE NCPAP INSTALLATION
ROLES DURING BUBBLE NCPAP INSTALLATION
1. The person at the head will ensure suctioning of the nasopharynx and maintenance of patent
airway.
2. The nurse will:
a. Ensure oxygen saturation probe is on patient,
b. Monitor and document heart rate, skin temperature and oxygen saturation,
c. Suction nasopharynx (as needed),
d. Measure head circumference in order to get the right size bonnet for the NCPAP
kit.(Note: RT may also perform this task.)
3. The RT will:
a. Assist with respiratory support
a. Prepare equipment needed for bubble NCPAP
b. Suction nasopharynx (if not already done)
c. Choose the appropriate available equipment and confirm indications for bubble NCPAP
therapy (see Tables 1, 2 & 3 in Appendix A).
d. Set up the bubble NCPAP device according to the manufacturer’s recommendations.
e. Install the nasal interface for the bubble NCPAP.
f. Document the size of cap and prongs on the appropriate order/flowsheet.
4. Once bubble NCPAP has been started, RT will also:
a. Ensure the nasal interface is properly applied;
b. Ensure that the level of NCPAP ordered is achieved,
c. Document the installation and parameters on the Respiratory Therapy Non-Invasive
Ventilation Order/Flowsheet.DM1229.
5. The team will continuously monitor heart rate, respiratory rate, SpO2, air entry and work of
breathing, and document on respective flow sheets.
6. If initiated in the Birthing Center, once the bubble NCPAP is installed, and newborn is showing
adequate spontaneous breathing, the team will transfer newborn to the NICU. (For infants already
in the NICU, this step does not apply.)
Installation and Maintenance of Bubble NCPAP Therapy in the NICU and the Resuscitation room in the Birthing Center at the RVH
Final September 11th 2018 4
Revision date: September 20221. Set up bubble NCPAP interface and prepare infant:
a. Place the bonnet on the infant by pulling it down over the ears (Figure 1) and positioning
near the infant’s eyebrows (Figure 2). Ensure ears lie flat against head under hat.
Figure 1 Figure 2
b. Use the Nasal Sizing Guide to determine best size of nasal prong for infant (Figure 3).
The nasal prongs should completely fill the nares to avoid leak of the NCPAP pressure.
Figure 3
c. Connect short blue inspiratory circuit to one side of the Cannula Body (Figure 4).
Connect short clear expiratory circuit to the other side of the Cannula Body.
Figure 4
d. Place prongs curved side DOWN.
e. Check for termination of pressure monitoring line at the NP, adjust accordingly.
f. Connect the dual - heated circuit, including temperature probes and heated wire
connectors to the ends of the prongs circuit by using an adaptor.
g. Connect the blue inspiratory circuit to the NP blue inspiratory circuit.
h. Connect the clear color expiratory circuit to the clear color NP circuit limb.
i. Connect the water bag to the heating chamber.
j. Add water to the heating chamber. Turn the heater ON and verify that is operating
correctly as per manufacturer’s instructions.
k. Initiate at a flow rate between 5 to 8 liters/minute. Do not exceed 12 liters/minute or
provide less than 5 liters/minute. NOTE: Increasing the flow in an attempt to compensate
for leaks actually increases resistance and is not advised. Flow rates less than 5
liters/minute are not enough to wash out CO2 in the circuit.
l. Set the NCPAP pressure to the prescribed pressure.
Installation and Maintenance of Bubble NCPAP Therapy in the NICU and the Resuscitation room in the Birthing Center at the RVH
Final September 11th 2018 5
Revision date: September 2022m. Set FiO2 as per OWL Guideline.
n. Occlude the prongs to ensure that bubbles are created in the bubble water system,
confirming no leaks in the delivery system.
2. Attach nose bumper and circuit bumpers for secure placement of NP and attachment of
circuit to bonnet.
a. Remove nose bumper pads from package and place them flat on clean surface with hook
side of Velcro in upright position.
b. Align the holes with the nasal prongs. Thread prongs through nose bumper pad and
bring the base of the nose bumper pad up.
c. Tightly wrap around the prong body and secure with the hook that is part of nose bumper
pad (Figure 5 and 6). Change nose bumper pad when soiled or as needed.
Figure 5 Figure 6
d. Place the circuit bumper pad flat on clean surface with hook part in upright position
(Figure 7).
e. Bring base of the circuit bumper pad up (Figure 8) and tightly wrap around inspiratory and
expiratory limbs of circuit.
f. Secure with hook part of circuit bumper pad.
Figure 7 Figure 8
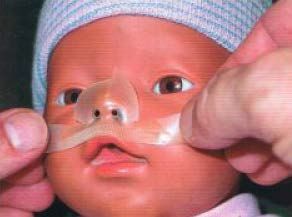
3. Apply Cannulaide® to baby’s face
The Cannulaide® is a nasal seal used during bubble NCPAP therapy. As an adjunct, the
Cannulaide® can improve sealing of the system and may help reduce nasal irritation. It is sized to
fit all nasal cannulas and helps maintain the prongs straight and well positioned in the nares, i.e.
not touching the nasal mucosa. It is best to use the Cannulaide® instead of the RespiraGel
Mustache found in the package as it has better adherence.
Attention:
• Do not use Cannulaide® to reduce the prong size. Remember that babies are nose
breathers and therefore, it is very important that the adequate prong size be used since
small prongs with small Cannulaide® will prevent leak but significantly increase
resistance.
• The Cannulaide® does NOT prevent septum injury. The ONLY way to protect the
septum from injury is by preventing the prongs from touching it.
Installation and Maintenance of Bubble NCPAP Therapy in the NICU and the Resuscitation room in the Birthing Center at the RVH
Final September 11th 2018 6
Revision date: September 2022NOTE: In babies less than 29 weeks gestation, the Cannulaide® will only be placed once in the
NICU, at the first full assessment after admission (at 4-6 hours of life). This is done to optimize the
PEEP received in the birthing center and immediately after birth and to prevent removal of the
NCPAP system as much as possible. Refer to MCH Clinical Guideline for Management of Extremely
Preterm Infants born less than 29 weeks and/or less than 1000g in the First 72 hours After Delivery
a. Clean and dry the patient skin around the application area by using 2X2 gauzes and sterile water
(the Cannulaid ® will adhere best to a warm, clean and oil free surface). Be sure all skin oils,
moisture and secretions are removed and the area is clean and dry. (Additionally, if infant is
placed on NCPAP right after birth, be careful when applying ocular antibiotics, as the ointment
can spread on the cheeks making adherence of Cannulaide ® very difficult. )
b. Remove the Cannulaide® from the package. Warm faceplate between your hands prior to
application. Remove release layer from Cannulaide® faceplate.
c. Center the faceplate on the upper lip below nasal septum and smooth it along upper lip area
(Figure 9). Ensure that the Cannulaide® is placed in such a way that the Velcro portion of the
mustache is not in contact with the nasal septum.
d. Apply gentle pressure with warm hands to upper lip and cheeks to initiate adhesion. Hold in place
until tape adheres well. This may take up to thirty (30) seconds.
Figure 9
4. Apply Circuit and Interface to infant
a. Place the NP in the infant’s nose (Figure 10). With infant in a supine position, head elevated
about 30° and neck supported with a small roll, position the prongs gently into the nares so
there is no upward pressure on the septum. Place prongs curved side DOWN, and connect
them to the NCPAP circuit. Adjust the angle at the corners, to curve the prongs slightly,
matching the curved plane across the upper lip. The prongs should fill the nares’ diameter
completely.
b. Secure baby nose bumper pad to Cannulaide® by gently pressing.
Figure 10 Figure 11
c. Attach circuit bumpers to side of bonnet with hook strip provided (Figure 11). Gently press
circuit bumpers to the bonnet.
Installation and Maintenance of Bubble NCPAP Therapy in the NICU and the Resuscitation room in the Birthing Center at the RVH
Final September 11th 2018 7
Revision date: September 2022d. Position infant and tubing system to avoid pressure on the nose. Adjust tubing and
connections as needed.
NOTE: Careful observation of the position of the prongs is essential. Excessive blanching may
injure the skin and internal structures of the nose. When the appropriate size is selected,
blanching of the nares is not uncommon. When it occurs, wait 30 seconds and reassess. If it is
still present, consider a smaller size of prong.
5. Ensure Consistent Bubbling.
Consistent bubbling is important for alveoli recruitment, maintenance of functional residual
capacity (FRC) and decreasing on airway resistance and work of breathing. However, it is
important to note that some intermittent bubbling may occur normally. If there is no bubbling at all,
then the infant is not receiving effective bubble NCPAP therapy. A system which is not bubbling
has a pressure leak, which must be resolved.
A. One source of leak may be an open mouth. A chin-strap can be utilized in an attempt to
keep the infant’s mouth closed. It should not be so tight that it prevents the infant from
yawning or crying, but tight enough to prevent an air leak at rest. If chin-strap is
indicated the RT or nurse will apply it according to the following instructions:
a. Place chin strap below base of chin with cut out centered at midline base of chin
(Figure 12).
b. Thread oro-gastric (OG) tube through opening in in chin strap.
c. Press Velcro ends of chin strap onto bonnet
d. Ensure that straps are not too tight (baby should be able to yawn or cry), and do not
restrict the airway (should be place under chin, not back towards neck).
Figure 12
B. Positioning of prongs may also create a leak or even blockage. Prongs should never
sit completely up against the septum of the nares – the bumper should be on upper lip,
with a few millimeters of space between the septum and the bumper. Additionally, the
joints of the NCPAP circuit can be turned slightly to achieve optimum positioning, and
thus ensure bubbling.
Installation and Maintenance of Bubble NCPAP Therapy in the NICU and the Resuscitation room in the Birthing Center at the RVH
Final September 11th 2018 8
Revision date: September 2022c) PROCEDURE FOR CARE DURING BUBBLE NCPAP TREATMENT
Care while on bubble NCPAP is aimed at optimizing respiratory status, decreasing work of breathing,
and minimizing FiO2 required. For this reason, disconnecting infants from bubble NCPAP during
routine care should be avoided as much as possible. All care should be done with the prongs in
place. Babies should be weighed with their NCPAP interface and bonnet in place, and head
massages without the bonnet should be done while maintaining prongs in the nares. If Cannulaide ®
change is necessary, it should be done for as quickly as possible (especially in the first 72 hours of
life in extremely preterm infants, as per Clinical Guideline for Management of Extremely Preterm
Infants born less than 29 weeks and/or less than 1000g in the First 72 hours After Delivery) to
prevent derecruitment.
ROLES FOR CARE DURING BUBBLE NCPAP TREATMENT
The best way to prevent complications is for the NICU team to work together to ensure the interface is
properly placed at all times and that there is consistent bubbling
1. All care should be bundled to prevent unnecessary handling and stimulation of the infant
2. RT will:
a. Check that the flow inflating bag and mask are readily available and working properly.
b. Install, wean, and discontinue the NCPAP as per physician order
c. Increase or decrease flow as per physician order
d. Perform equipment checks and proper documentation on Respiratory Therapy Non-
Invasive Ventilation Order/ Flow sheet every 2 hours.
e. Check the bubbler every 2 hours and remove the water in the container holding the
excess water.
f. Change the dual heated circuit and bubbler every 28 days. The interface should be
changed every 7 days, and bumper and prongs must be changed when dirty.
3. RN will:
o Measure and document abdominal girth with each care period
o Aspirate air from OG tube q 2-3 hours prior to feeds and, if possible, leave it vented at
least an hour in between feeds to avoid abdominal distention
4. RN and/or RT will:
A. Perform an hourly visualization of the infant, the interface, and the circuit.
B. Perform and document a full respiratory assessment including auscultation, work of
breathing, SpO2, TcPCO2 (if available), and respiratory rate with each care.
C. Ensure blood gas and chest x-ray be done once after initiation of bubble NCPAP
treatment, and if indicated clinically thereafter, as ordered by physician.
D. Suction infant with each care period (see below), and document intervention
E. Perform skin care with each care (see below), and document intervention
F. Optimize opening of airway by appropriate positioning with each care (see below)
G. Increase or decrease FiO2 as per OWL guidelines
H. Optimize positioning of circuit to ensure infant’s comfort
I. Remove water condensation from the circuit
J. Document in respective flowsheets:
a. RNs: Hourly documentation of heart rate, respiratory rate, SpO2, FiO2,
TcPCO2 (if available) & pressure setting of bCPAP
Installation and Maintenance of Bubble NCPAP Therapy in the NICU and the Resuscitation room in the Birthing Center at the RVH
Final September 11th 2018 9
Revision date: September 2022b. RTs: Q2H documentation of equipment and pressure checks on Respiratory
Therapy Non-Invasive Ventilation Order/ Flow sheet
1. Suctioning
RN and RT may perform nasopharyngeal suction together.
Babies on NCPAP should have their nares suctioned frequently since nasal obstruction due to
secretions is the first cause of bubble NCPAP malfunctioning and therapy failure. Suctioning is
required every 1 to 4 hours, depending on each case. Discuss frequency of suctioning with
the team and establish a plan for each patient every day. Signs of airway obstruction are
increased O2 needs, episodes of apnea/desaturations and increased work of breathing. Follow
the suctioning guidelines below. It is recommended that 2 health care professionals are present
when suctioning for extremely preterm infants, especially in the first 72 hours (see Clinical
Guideline for Management of Extremely Preterm Infants born less than 29 weeks and/or less
than 1000g in the First 72 hours After Delivery).
A. Perform hand hygiene as per MUHC Infection Control guidelines.
B. Ensure suction pressure set to 80-100 mmHg
C. Don clean gloves
D. Cover patients’ eyes with gauze or clean wipe as per infection control guidelines to
prevent conjunctivitis. (The bonnet should NOT be used to cover eyes as it may be
already contaminated with droplets.)
E. Suction oropharynx:
a. Using oral suction device, suction sides of oropharynx.
b. Rinse oral suction device with sterile water or normal saline.
c. Cap oral suction device when done.
F. Suction nasopharynx:
a. Measure distance from same-side tragus of the ear to nare and multiply by 1.5 to
obtain length of catheter required to suction the patient.
b. Attach 8 Fr suction catheter to suction tubing. Use a 6 Fr catheter only if unable
to pass an 8 Fr A 6 Fr may pass or slide more easily, but is less effective at
removing secretions.
c. Lubricate suction catheter with small amount of water soluble lubricant
d. Remove one cannula from one nare only (most easily achieved using tweezers),
and pinch this cannula. (The other cannula should remain in the other nare to
maintain some NCPAP pressure during the procedure.)
e. Insert catheter into that nare, aiming towards occiput. Apply suction.
f. Slowly withdraw. Apply suction during withdrawal. Suction should not exceed 5
seconds per pass.
g. Repeat procedure only if large amount of thick secretions obtained.
h. Replace cannula, and allow infant to recover.
i. Rinse suction catheter with sterile water or normal saline.
j. Repeat the same procedure on the other side.
2. Skin Care
Redness can become skin breakdown / necrosis in a matter of hours and it is generally caused
by inadvertent pressure. The bonnet, prongs, and chin strap can all be sources of pressure.
Installation and Maintenance of Bubble NCPAP Therapy in the NICU and the Resuscitation room in the Birthing Center at the RVH
Final September 11th 2018 10
Revision date: September 2022A. Bonnet & head – once per shift, the RN and/or RT will:
a. Remove infant’s bonnet, while maintaining prongs in nares manually.
b. Inspect the head and ears for skin breakdown. Particular attention should be
brought to the area behind the ears, where wetness, redness, irritation, and skin
breakdown can hide.
c. Perform a gentle head massage to promote blood flow to area.
d. Ensure skin is dry and free of compromise before reapplying bonnet. If skin
breakdown is noted, consult with MD/NNP. If bonnet is creating pressure points,
measure head circumference and choose appropriate size.
B. Prongs & nares/nasal septum – with each care, the RN and/or RT will:
a. During suctioning, perform a thorough visual check of the patient’s nose/septum.
Use penlight to assess inside condition of nares if redness is present.
b. Ensure the nose is dry after suctioning
c. Ensure the nasal prongs/cannula are away from the nasal septum by maintaining
a “cushion” of air (2-3 mm) between the bridge of the prongs and the nasal
septum at all times.
d. Change Cannulaide® only if it no longer adheres to the skin. Assess areas
usually covered by Cannulaide ® for skin breakdown or compromise when
changing.
e. Consult MD/NNP if redness or breakdown is noted. In addition, reposition the
prongs away from the septum and allow the area to recover.
C. Chin strap & chin – with each care, the RN and/or RT will:
a. Remove chin strap and visualize skin under strap
b. Consult MD/NNP if redness or breakdown noted.
c. Ensure skin is dry and free of compromise before reapplying chin strap.
3. Positioning
During each care period, the RN and/or RT will:
• Change the position of the infant. The infant may be placed supine, prone or lateral. It is
recommended to change the position every 2-4 hours. Position changes improve
homogeneity of ventilation.
o When in a supine position, a roll should be placed behind the infant’s neck to keep it
extended in order to keep airway open.
o When prone or lateral, small “pillows” of clean wipes or blankets may be needed to
help keep the head supported without applying pressure on the bubble NCPAP
interface.
NOTE: Repositioning of any extremely preterm infant should always be done by 2 skilled
persons to ensure that the prongs stay in place during procedure, and to ensure smooth position
changes for the baby (see Clinical Guideline for Management of Extremely Preterm Infants born
less than 29 weeks and/or less than1000g in the First 72 hours After Delivery).
4. Holding / Kangaroo Care
An infant on bubble NCPAP therapy may be held or given kangaroo care as long as the baby is
considered stable by the medical team and oxygen requirement is generally less than 50% (see
Clinical Procedure – Protocol for Kangaroo Care in the Pediatric Population).
Installation and Maintenance of Bubble NCPAP Therapy in the NICU and the Resuscitation room in the Birthing Center at the RVH
Final September 11th 2018 11
Revision date: September 2022o It is recommended to have two members of the NICU team to help transfer the infant.
o Be as gentle as possible to avoid undue trauma or irritation of the nostrils/face of
infant.
o Ensure the weight of the circuit is gently supported to reduce tension on the nasal
tubing.
c. BUBBLE NCPAP WEANING AND DISCONTINUATION
The primary determinant to initiate weaning is clinical improvement. Weaning and/or discontinuation may
be considered for the following infants:
1. Preterm infants who are on FiO2 0.21with no evidence of respiratory distress and appropriate
weight gain, and no episodes of apnea and/or bradycardia for the preceding 24 hours. NOTE:
Lower bronchopulmonary dysplasia (BPD)rates have been documented when bubble NCPAP is
left in place until 32 weeks of corrected gestational age even if the patient has been on FiO2 0.21.
2. Term infants who are on FiO2 0.21with no evidence of respiratory distress.
The optimal method of weaning an infant off NCPAP remains uncertain. The following suggestions may
be considered:
• Wean FiO2 to 0.21 prior to weaning pressure (to reduce the risk of oxygen exposure in premature
infants).
• If the pressure is higher than 5 cmH2O, the level should be weaned to 5 cmH2O prior to removal.
It is not necessary to wean pressures below 5 cmH2O.
• In cases of nasal septum breakdown near the weaning period, consider change to a different
mode of non-invasive support such as heated humidified high-flow nasal cannula (HHHFNC)
therapy.
• It is not necessary to cycle on and off NCPAP. The weaned infant should remain off NCPAP as
long as he/she does not develop significant retractions, apnea, bradycardia and increased
oxygen requirements. Bubble NCPAP set-up, circuit, and interface should remain at the bedside
for 24 hours until the wean off support is considered successful.
For preterm infants who have BPD and require bubble NCPAP longer, i.e. until 34 to 36 weeks of
corrected gestational age, an alternative mode of respiratory support is HHHFNC. With HHHFNC, the
infant can be initiated on bottle feeding. NOTE: Bottle or breast feeding while on bubble NCPAP has been
documented in other centers without risk of aspiration.
d. EMERGENCY MEASURES
In case of prolonged drop in SpO2 below 88% or heart rate below 100 bpm the infant should be
stimulated and FiO2 increased. While doing that:
1- Check if the NCPAP system is bubbling. If not, there is a leak in the system. In this case, check if
the prongs are in place or need to be repositioned. Is there is a significant leak from the mouth?
Is the flow on? Is there chest movement? Continue to provide tactile stimulation, readjust the
prongs and/or minimize leaks by closing the mouth. Check again if the system is now bubbling.
2- Check for nasal or upper airway obstruction due to secretions or positioning of the neck/head.
Consider suction of the nares and nasopharyngeal area. If the baby recovers and has good
spontaneous effort, place him/her back on NCPAP.
3- If the infant does not improve, call for help, remove the nasal interface and start bagging using
the mask interface. If apnea persists despite mask/bag, discuss the possibility of changing to
NIPPV or intubation with the medical team.
4- Decompress the stomach after bagging.
Installation and Maintenance of Bubble NCPAP Therapy in the NICU and the Resuscitation room in the Birthing Center at the RVH
Final September 11th 2018 12
Revision date: September 2022e. BUBBLE NCPAP FAILURE
Bubble NCPAP failure is defined as progressive respiratory failure defined by a consistent increase (for
a period between 1 to 2h) in FiO2 greater than 50 % or severe respiratory acidosis - PCO2 greater than 65
mmHg with a pH less than 7.20 in two consecutive arterial/venous blood gases.
Episode of apnea requiring bag/mask ventilation due to failure to resume spontaneous breathing
Frequent episodes of apnea and/or bradycardia (more than 6 episodes in 6 hours). Apnea will be
defined as a respiratory pause longer than 20 seconds, or less than 20 seconds but associated
with desaturation (SpO2 less than 88%) and/or bradycardia. Bradycardia will be defined as a
heart rate less than 100 beats per minute.
Infants who meet these criteria may require escalation of respiratory support,
defined as either initiation of non-invasive positive pressure ventilation NIPPV or
intubation. MD/NNP should be advised immediately if any of the above occur.
NIPPV can be delivered via a ventilator or a SiPAP ®machine. It is recommended to use a nasal mask
rather than prongs for former pre-term patients who have BPD and are now post-term, or in full-term
infants with chronic lung disease
*Note that if the patient is switched to NIPPV with a ventilator for reasons of pressure, the prong interface
should still be used.
Please refer to Respiratory Therapy protocol on installation and maintenance of SiPAP® for further
details on use of this system.
5. MEDICATIONS (IF NECESSARY):
6. MAIN AUTHOR:
Dr. Elizabeth Hailu, Neonatologist
Marisa Leone, Assistant Chief Respiratory Therapy, MCH
Elissa Remmer, MCH NICU NPDE
7. CONSULTANTS:
Dr. Guilherme Sant’Anna, Neonatologist and Respiratory Therapy Medical Consultant
Installation and Maintenance of Bubble NCPAP Therapy in the NICU and the Resuscitation room in the Birthing Center at the RVH
Final September 11th 2018 13
Revision date: September 20228. APPROVAL PROCESS
Institutional and professional approval
Date approved
Committees
[yyyy-mm-dd]
Clinical Practice Review Committee (CPRC) (if applicable) 2018-07-19
Adult Pharmacy and Therapeutics (P&T) (if applicable) NA
Pediatric Medication Administration Policy (PMAP) (if applicable) NA
Pediatric Pharmacy and Therapeutics (Peds P&T) (if applicable) NA
Multidisciplinary Council (MDC) (if applicable)
9. REVIEW DATE
To be updated in maximum of 4 years or sooner if presence of new evidence or need for practice change.
10. REFERENCES
11. Avery ME, Tooly WH et al. Is Chronic lung disease in low birth weight infants preventable? A Survey
of Eight Centers. Pediatrics 1987;79: 26-30.
12. Ali, Hany. Nasal Prongs Continuous Positive Airway Pressure. A simple yet powerful tool. Pediatrics
2001;108(3) 759-761.
13. Sandri F, Ancore G, Lanzoni A et al. Prophylactic nasal continuous positive airway pressure in
newborns of 28-31 weeks gestations. Multicenter randomised controlled clinical trial. Arch Dis Child
Fetal Neonatal Ed 2004;89 (5): F 394-F398.
14. Ammari A. Suri M et al. Variables associated with the early failure of Nasal CPAP in very low birth
weight infants. J Pediatrics 2005;147(3):341-347.
15. Cannulaide®, Beevers Medical Solutions: http://www.beevers.net/our-products/cannulaide
16. Morley CJ, Davis PG, Doyle LW, Brion LP, Hascoet JM, Carlin JB. COIN Trial Investigators.
Intubation at birth for very preterm infants. N Engl J Med 2008;358:700-708.
17. Finer NN, Carlo WA et al: Support Study Group of the Eunice Kennedy Shriver NICHD Neonatal
Research Network. Early CPAP versus Surfactant in extremely Preterm Infants. N Eng J Med.
2010;362(21):1970-1979.
18. Dunn MS, Kaempf J, De Klerk A et al. Vermont Oxford Network DRM Study Group. Randomized trial
comparing approaches to the initial respiratory management of preterm neonates. Pediatrics
2011;128 (5).
19. Todd, David. Methods of weaning preterm babies23. Roberts CT, Owen LS, Manley BJ, Frøisland DH, Donath SM, Dalziel KM, Pritchard MA, Cartwright
DW, Collins CL, Malhotra A, Davis PG; HIPSTER Trial Investigators.Nasal High-Flow Therapy for
Primary Respiratory Support in Preterm Infants. N Engl J Med. 2016 Sep 22;375(12):1142-51.
24. Dargaville PA, Gerber A, Johansson S, De Paoli AG, Kamlin CO, Orsini F, Davis PG; Australian and
New Zealand Neonatal Network. Incidence and Outcome of CPAP Failure in Preterm Infants.
Pediatrics. 2016 Jul;138(1):e 20153985.
25. Subramaniam P, Ho JJ, Davis PG. Prophylactic nasal continuous positive airway pressure for
preventing morbidity and mortality in very preterm infants. Cochrane Database Syst Rev. 2016 Jun
14;(6):CD001243.
26. Bamat N, Jensen EA, Kirpalani H. Duration of continuous positive airway pressure in premature
infants. Semin Fetal Neonatal Med. 2016 Jun;21(3):189-95.
27. Sahni R, Schiaratura M, Polin RA. Strategies for the prevention of continuous positive airway
pressure failure. Semin Fetal Neonatal Med. 2016 Jun;21(3):196-203.
28. Shetty S, Hunt K, Douthwaite A, Athanasiou M, Hickey A, Greenough A. High-flow nasal cannula
oxygen and nasal continuous positive airway pressure and full oral feeding in infants with
bronchopulmonary dysplasia. Arch Dis Child Fetal Neonatal Ed. 2016 Sep;101(5):F408-11.
29. Continuous Positive Airway Pressure to Prevent Neonatal Lung Injury: How Did We Get Here, and
How Do We Improve? Wright CJ, Polin RA, Kirpalani H. J Pediatr. 2016 Jun;173:17-24.
30. Benign gaseous distension of the bowel in premature infants treated with nasal continuous airway
pressure: A study of contributing factors. Jaile JC, Levin T. Wung JT., Abramson SJ., Ruzal-Shapiro
C. Berdon WE. AJR AM J Roentgenol 1992 Jan;158 (1): 125-7
Version History
(for Administrative use only)
Version Description Author/responsable Date
Marisa Leone, Assistant Chief 2018-09-11
No 1 Development and Approval
Respiratory Therapy, MCH
Description (Création, Adoption,
No Révision avec modification, Révision Acronyme direction, Nom fonction
sans modifications, etc.)
Description (Création, Adoption,
No Révision avec modification, Révision Acronyme direction, Nom fonction
sans modifications, etc.)
Description (Création, Adoption,
No Révision avec modification, Révision Acronyme direction, Nom fonction
sans modifications, etc.)
Installation and Maintenance of Bubble NCPAP Therapy in the NICU and the Resuscitation room in the Birthing Center at the RVH
Final September 11th 2018 15
Revision date: September 2022Appendix: A equipment sizing
Table 1. Size bonnet from the Babi Plus NCPAP kit
Part Number Bonnet Size Weight Head Circumference
30301 1 Up to 750 grams 12 – 18 cm
30302 2 650 to 900 grams 15 – 21 cm
30303 3 800 to 1600 grams 18 – 23 cm
30304 4 1500 to 2500 22– 28 cm
grams
Table 2. Nasal Prongs (NP) Kit for the infant based upon approximate body weight
Kit NP Size Approximate Body Weight Kit NP Size Approximate Body Weight
Small 0 less than 700 grams Large 4 2000 to 3000 grams
Small 1 less than 700 grams Large 5 greater than 3000 grams
Small 2 700 to 1250 grams Large 6 greater than 3000 grams
Small 3 1250 to 2000 grams Large 7 greater than 3000 grams
Table 3. Cannulaide ® for the infant based on approximate weight
Size of Cannulaide® Weight
0 less than 700 g
1 700g- 1250 g
2 1250g-2000 g
3 2000g- 3000g
4 greater than 3000g
Installation and Maintenance of Bubble NCPAP Therapy in the NICU and the Resuscitation room in the Birthing Center at the RVH
Final September 11th 2018 16
Revision date: September 2022You can also read

















































