City of New Smyrna Beach - Your Benefits Overview
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

City of New Smyrna Beach
Your Benefits Overview
October 1, 2021– September 30, 2022
2 0 2 1
Table of Contents
3 What’s new for October, 2021 18 Life Insurance
4 Enrollment / Eligibility 22 Short Term Disability
5 Medical Insurance 23 Employee Assistance Program
12 Health Savings Account 24 Metlaw and FraudScout
(HSA)
13 Flexible Spending Account 25 Plansource Enrollment Instructions
(FSA)
14 Dental Insurance 28 Important Notices
16 Vision Insurance
What’s Changing in 2021?
For the 2021‐2022 plan year there are some very exci ng changes within your employee
benefits program! Please see the below informa on on what is new this year:
Medical Carriers are remaining the same but we are offering new Medical op ons
this year.
FHCP: TI5/TF5 ‐ HDHP/HSA
FHCP: T32 ‐ HMO
FHCP: T29 ‐ POS
BCBS: Blue Op ons 03769 ‐ PPO (For currently enrolled employees ONLY)
We are introducing a Health Savings Account (HSA) with an annual contribu ons of
$1,250.00. For those enrolling on the TI5/TF5 HDHP medical plan only.
Removing date of hire City contribu ons for medical and dental.
All employees will receive the same City contribu on depending on the plan.
No changes to other plans.
This Benefits‐At‐A‐Glance booklet is designed to provide basic informa on to employees on benefit plans and programs available October 01, 2021– September 30,
2022. It does not detail all of the provisions, restric ons and exclusions of the various benefit programs documented in the carrier contract or the Summary Plan
Descrip on (SPD). This booklet does not cons tute an SPD or Plan Document as defined by the Employee Re rement Income Security Act (ERISA). 3
Your Enrollment
City of New Smyrna Beach offers a comprehensive and compe ve benefit package for you and
your family that includes op ons suitable for all needs. This booklet will provide you a general
Enrollment
summary for each plan to use as a convenient reference when making your enrollment decisions.
Your benefit plan year for all plans is October 1st through September 30th.
Who is eligible?
All ac ve full‐ me employees working a minimum of 30 hours per week will be eligible to enroll
in medical, dental, life, and short term disability plans.
When does my coverage begin?
I am a new hire….
Coverage for these plans will begin the 1st of the month following 30 days of employment.
I am a current employee enrolling during annual open enrollment….
Any elec ons made during annual open enrollment will be effec ve October 1st, 2021 and will
con nue through September 30th, 2022. Remember no changes to your plans will be permi ed
throughout the plan year, unless you experience a qualifying life event (examples: birth/adop on
of a child, divorce or legal separa on, dependent’s loss/gain of coverage, change in dependent
status, death of spouse, child, or other qualified dependent, change in employment status for
employee, spouse, or dependent, change in residence due to an employment transfer, and
eligibility for Medicare or Medicaid).
This Benefits‐At‐A‐Glance booklet is designed to provide basic informa on to employees on benefit plans and programs available October 01, 2021– September 30,
2022. It does not detail all of the provisions, restric ons and exclusions of the various benefit programs documented in the carrier contract or the Summary Plan
Descrip on (SPD). This booklet does not cons tute an SPD or Plan Document as defined by the Employee Re rement Income Security Act (ERISA). 4
FHCP ‐ Member Portal
By being a Florida Health Care Plans member, you automa cally receive services that are free to you
and your covered dependents.
Below are some of these services. For more informa on, log on to your member portal at
www. cp.com.
Find a Provider/Facility
Medical Insurance
Health Care Reform Informa on
Member Portal Login
Member Wellness Programs
Glossary of Health Coverage and Medical Terms
Summary of Benefits Coverage
Case Management
U liza on Management
Florida Health Care Member Portal
Florida Health Care’s Member Portal is available 24 hours a day, 7 days a week, 365 days a year. The
member’s Portal has three main sec ons, Health Portal, Documents Portal and Member Resources.
See below for a descrip on of each portal.
The Health Portal: Here you will find the “Welcome to Wellness” Health Risk assessment and Health
Management Tool. A er you register, you have the opportunity to complete a personalized health
risk assessment that will provide insight on different areas of improvement concerning member’s
health. This also allows access to a database of thousands of ar cles, programs and news related to
health and health condi ons.
If you u lize a FHCP staff physician, you can access the Pa ent Portal which will allow you to
communicate directly with your FHCP staff physician, make an appointment or request prescrip on
refills.
The Documents Portal: Here you will be able to obtain, view and print your Cer ficate of Coverage
(Member Handbook) which describes your rights and obliga ons along with FHCP rights and
obliga ons with respect to the coverage and benefits provided. You will also be able to view and print
your benefit summary and any applicable benefit riders.
Member Resources: Provides access to common FHCP programs, contacts, resources and forms.
Member Wellness Programs
As a FHCP member, you have access to their Wellness Programs which provides informa on on:
Smoking Cessa on
Weight Management
Diabetes
Acute Low Back and Neck Pain
Nutri on Program
Exercise
This Benefits‐At‐A‐Glance booklet is designed to provide basic informa on to employees on benefit plans and programs available October 01, 2021– September 30,
2022. It does not detail all of the provisions, restric ons and exclusions of the various benefit programs documented in the carrier contract or the Summary Plan
Descrip on (SPD). This booklet does not cons tute an SPD or Plan Document as defined by the Employee Re rement Income Security Act (ERISA). 5
FHCP ‐ Extended Hours Care Centers
Medical Insurance
This Benefits‐At‐A‐Glance booklet is designed to provide basic informa on to employees on benefit plans and programs available October 01, 2021– September 30,
2022. It does not detail all of the provisions, restric ons and exclusions of the various benefit programs documented in the carrier contract or the Summary Plan
Descrip on (SPD). This booklet does not cons tute an SPD or Plan Document as defined by the Employee Re rement Income Security Act (ERISA). 6
FHCP ‐ Doctor on Demand
See a board cer fied doctor or a licensed psychologist or psychiatrist through live, face‐to‐face video visits from
anywhere!
Access to our board cer fied physicians 24/7, book an appointment with a psychologist at your convenience.
Physicians can diagnose, treat and write prescrip ons (if needed) for most non‐emergency medical condi ons.*
Connect using your computer, smartphone, or tablet (with a front facing camera). You can download the app from the App
Medical Insurance
Store or Google Play . Your device must have a front facing camera. If you are connec ng on the web, please use a Safari,
Chrome or Firefox browser.
Video Visit with a Doctor from the Comfort of Home
Text “FHCP” to 68398 or download the Doctor On Demand app from
the App Store on your smartphone or tablet today!
1. Tap “Sign Up”
2. When asked for your health insurance, select “Florida Health
Care Plan” from the list.
3. Enter the informa on from your FHCP insurance card on the next
screen.
Affordable, Simple, Convenient
Visits with a medical doctor are $10* and visits with a psychologist and psychiatrist are each $30*. Visit within the comfort
of your own home. Doctor on Demand also connects you with a physician within just 90 seconds.
Great Doctors who Treat Nearly Everything
You'll have access to board‐cer fied and licensed physicians in every state, wai ng to treat nearly any non‐emergency
medical issue or emo onal health issue such as anxiety and depression.
Get a Prescrip on, Too!
Quick and paperless prescrip on fulfillment to your pharmacy**. When prompted to select your pharmacy, click on the
“Search Near Me” bu on. Florida Health Care pharmacies will appear as the white bird logo.
What is the Cost?
A er inpu ng your informa on from your FHCP insurance card, you will see the following co‐pay amounts*:
Medical Visit: $10 Copay*
Psychology Visit: $30 Copay*
Top Medical Issues/Psychological Issues Treated
Top medical issues treated are: Cold & Flu, Bronchi s & Sinus Infec ons, Allergies, Skin & Eye Issues, Sore Throat,
Urinary Tract Infec on, Pediatric Issues.
Top Psychological Issues Treated are: Anxiety, Stress, Depression, Addic ons, and Rela onship Issues.
*Please check your schedule of benefits to see if a deduc ble applies. If so, medical visits are $42, psychologist visits are
$52.50 for 25 minutes ($95 for 50 minutes), and psychiatry visits are $99.75 for 50 minutes ($225 45‐minute ini al visit)
un l the deduc ble is met.
**No controlled drugs prescribed**
This Benefits‐At‐A‐Glance booklet is designed to provide basic informa on to employees on benefit plans and programs available October 01, 2021– September 30,
2022. It does not detail all of the provisions, restric ons and exclusions of the various benefit programs documented in the carrier contract or the Summary Plan
Descrip on (SPD). This booklet does not cons tute an SPD or Plan Document as defined by the Employee Re rement Income Security Act (ERISA). 7
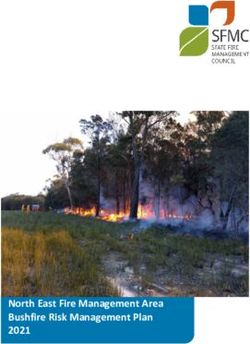
Medical Summary
The summary below provides a high level overview of the FHCP TI5/TF5 and FHCP T32 Plans through Florida Health Care
Plans
Website: www. cp.com
Phone number: 1‐877‐615‐4022
If you choose the Florida Health Care TI5/TF5 or T32 HMO, please be reminded it is a network only plan. You must
receive services from a par cipa ng physician. You must receive a referral to a specialist from your primary care
Medical Insurance
provider. If a service requires a prior authoriza on or pre‐cer fica on and it is not obtained, the service will not be
covered and you will be responsible for 100% of charges.
Plan Name FHCP TI5/TF5 HDHP (HSA) Plan FHCP T32 HMO Plan
Name of Network FHCP FHCP
Calendar Year Deduc ble
Individual/Family $2,500/$5,600($2,800 ind.) $0/$0
Annual Out‐of‐Pocket Maximum (Includes deduc ble, copays, coinsurance)
Individual/Family $5,000/$13,800($6,900 ind.) $2,500/$5,000
Coinsurance (Coins) (Amount paid a er deduc ble is met)
You pay….. 10% 15%
Physician Services
Office Visit Deduc ble + Coinsurance $20 Copay
Specialist Deduc ble + Coinsurance $35 Copay
Chiroprac c Care Deduc ble + Coinsurance $15 Copay
Adult and Child Wellness Exams 100% Covered 100% Covered
Diagnos c Independent Tes ng Outpa ent***
Lab Test & X‐Ray Outpa ent Deduc ble + Coinsurance $0 Copay
Advanced Imaging (MRI, CT, PET) Deduc ble + Coinsurance $25 Copay
Hospital Services
Inpa ent Hospital Per Admission Deduc ble + Coinsurance $250/day (Days 1‐5 days)
Emergency Room Deduc ble + Coinsurance $200 Copay
Urgent Care Deduc ble + Coinsurance $75 Copay
Prescrip on Drugs
Retail (30 day supply)**: CALANDER YEAR DEDUCTIBLE
Preferred Generic $3 Copay/N/A (Walgreens) $3 Copay/$15 Copay (Walgreens)
Non‐Preferred Generic $10 Copay/$15 Copay (Walgreens) $10 Copay/$15 Copay (Walgreens)
Preferred Brand Name $30 Copay/$35 Copay (Walgreens) $30 Copay/$35 Copay (Walgreens)
Non‐Preferred Brand Name $55 Copay/$60 Copay (Walgreens) $55 Copay/$60 Copay (Walgreens)
Specialty Drugs‐Preferred 15% Coinsurance/N/A (Walgreens) 15% Coinsurance/N/A (Walgreens)
Specialty Drugs‐Non‐Preferred 25% Coinsurance/N/A (Walgreens) 25% Coinsurance/N/A (Walgreens)
Mail Order (90 day supply)**: $6/$27/$87/$162 Copay $6/$27/$87/$162 Copay
**Pharmacy Note: If you purchase a preferred or non‐preferred brand product when a generic is available, you will be
responsible for paying the Average Wholesale Price (AWP) for that prescrip on.
*** The diagnos c independent tes ng facility is not the same as an outpa ent hospital se ng. See the summary of
benefits.
This Benefits‐At‐A‐Glance booklet is designed to provide basic informa on to employees on benefit plans and programs available October 01, 2021– September 30,
2022. It does not detail all of the provisions, restric ons and exclusions of the various benefit programs documented in the carrier contract or the Summary Plan
Descrip on (SPD). This booklet does not cons tute an SPD or Plan Document as defined by the Employee Re rement Income Security Act (ERISA). 8
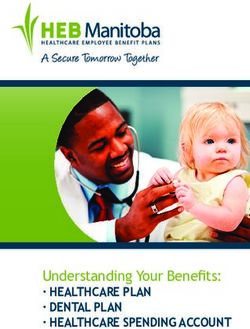
Medical Summary
The summary below provides a high level overview of the FHCP T29 POS and FL Blue, Blue Op ons 03769 PPO Plans.
Website: www. cp.com / www.floridablue.com
Phone number: FHCP: 1‐877‐615‐4022, Fl Blue: 1‐800‐352‐2583
If you choose the Florida Health Care T29 Point of Service Plan, you may also use out of network providers. However, your
out of pocket cost will be lower if you use in network providers. Please see the benefit summary for out of network services.
Medical Insurance
If a service requires a prior authoriza on or pre‐cer fica on and it is not obtained, the service will not be covered and you
will be responsible for 100% of charges.
If you choose the Florida Blue‐Blue Op ons 03769 PPO Plan, you may also use out of network providers. However, your out
of pocket cost will be lower if you use in network providers. Please see the benefit summary for out of network services.
Plan Name FHCP T29 POS Plan FL Blue Blue Options 03769 Plan*
Name of Network FHCP Blue Options
Calendar Year Deduc ble
Individual/Family $0/$0 $500/$1,500
Annual Out‐of‐Pocket Maximum (Includes deduc ble, copays, coinsurance)
Individual/Family $2,500/$5,000 $3,000/$6,000
Coinsurance (Coins) (Amount paid a er deduc ble is met)
You pay….. 15% 20%
Physician Services
Office Visit $20 Copay $25 Copay
Specialist $35 Copay $60 Copay
Chiroprac c Care $15 Copay $60 Copay
Adult and Child Wellness Exams 100% Covered 100% Covered
Diagnos c Independent Tes ng Outpa ent***
Lab Test & X‐Ray Outpa ent $0 Copay $0 (Lab)/$50 Copay (X‐Ray)
Advanced Imaging (MRI, CT, PET) $0 Copay Deduc ble + Coinsurance
Hospital Services
Inpa ent Hospital Per Admission $200 Copay Deduc ble + Coinsurance
Emergency Room $100 Copay $300 Copay
Urgent Care $60 Copay $65 Copay
Prescrip on Drugs
Retail (30 day supply)**:
Preferred Generic $3 Copay/$15 Copay (Walgreens)
Non‐Preferred Generic $10 Copay/$15 Copay (Walgreens) Tier 1: $10 Copay
Preferred Brand Name $30 Copay/$35 Copay (Walgreens) Tier 2: $50 Copay
Non‐Preferred Brand Name $55 Copay/$60 Copay (Walgreens) Tier 3: $80 Copay
Specialty Drugs‐Preferred $125 Copay/N/A (Walgreens)
Mail Order (90 day supply)**: $6/$27/$87/$162 Copay 2.5x’s Copay above
For the FL Blue Plan Only:
*This plan is only for CURRENTLY enrolled employees
For the FHCP T29 POS Plan only:
**Pharmacy Note: If you purchase a preferred or non‐preferred brand product when a generic is available, you will be
responsible for paying the Average Wholesale Price (AWP) for that prescrip on.
*** The diagnos c independent tes ng facility is not the same as an outpa ent hospital se ng. See the summary of benefits.
This Benefits‐At‐A‐Glance booklet is designed to provide basic informa on to employees on benefit plans and programs available October 01, 2021– September 30,
2022. It does not detail all of the provisions, restric ons and exclusions of the various benefit programs documented in the carrier contract or the Summary Plan
Descrip on (SPD). This booklet does not cons tute an SPD or Plan Document as defined by the Employee Re rement Income Security Act (ERISA). 9
Medical Plan Costs Per Paycheck
City contributes 100% of the employee cost and 50%
of the dependents cost.
Medical Insurance
FHCP TI5/TF5
Who is Covered Who is Covered FHCP T32
HDHP
Employee $0.00 Employee $0.00
Employee + Spouse $92.56 Employee + Spouse $127.69
Employee + Child(ren) $92.56 Employee + Child(ren) 127.69
Family $146.52 Family $202.12
BlueOp ons
Who is Covered FHCP T29 Who is Covered
03769*
Employee $0.00 Employee $0.00
Employee + Spouse $146.50 Employee + Spouse $353.45
Employee + Child(ren) 146.50 Employee + Child(ren) $235.63
Family $231.90 Family $563.46
For the FL Blue Plan Only:
*This plan is only for CURRENTLY enrolled employees
This Benefits‐At‐A‐Glance booklet is designed to provide basic informa on to employees on benefit plans and programs available October 01, 2021– September 30,
2022. It does not detail all of the provisions, restric ons and exclusions of the various benefit programs documented in the carrier contract or the Summary Plan
Descrip on (SPD). This booklet does not cons tute an SPD or Plan Document as defined by the Employee Re rement Income Security Act (ERISA). 10Cost Savings Tools
Prescription Drug cost comparison:
Medical Insurance
Use GoodRx's drug price search to compare prices (just like you do for travel or
electronics on other sites) for your prescrip on at pharmacies near you. GoodRx
does not sell the medica ons, the free website and mobile app tells you where
you can get the best deal on them. If you have insurance, your co‐pay might not
be the best price. Hundreds of generic medica ons are available for $4 or even
free without insurance. Every week GoodRx collects millions of prices and discounts from pharmacies, drug manufacturers
and other sources. GoodRx will show you prices, coupons, discounts and savings ps for your prescrip on at pharmacies
near you. Please visit the website at www.goodrx.com or download the app on your smartphone.
Please note: amounts paid for prescrip ons using GoodRx’s discount card do not apply toward your medical plan’s
deduc ble or annual out of pocket maximum.
Pharmacy Discount Programs:
Before you pay for your next prescrip on, check to see if they are available for free or at a lower cost than tradi onal
copays. Pharmacies such as Wal‐Mart, CVS/Target, and Costco offer prescrip on discount programs that allow you to
purchase medica ons for as low as $4 for a 30 day supply. Publix pharmacies also provide a list of free maintenance
medica ons as well as an bio cs that they offer for free (with a prescrip on from your physician). If your local pharmacy
is not listed please check with them to see if they offer any discounts.
Urgent Care/Walk-In-Clinics Vs. Emergency:
Do not pay more than you have to for medical care. The Emergency room is meant for
true emergencies such as life threa ng illnesses and injuries. Walk‐in‐clinics are
designed to treat common ailments and provide basic primary health care and are
typically staffed by nurse prac oners and some mes a physician’s assistant. They are
used for common ailments such as: flu/strep throat, allergies, cold and cough. Urgent
care facili es are designed to serve pa ents who are suffering from acute illnesses
and injuries which are beyond the capaci es of a regular walk‐in‐clinic, are typically
open for extended hours, and are used to treat non‐life threa ng injuries and
illnesses. To maximize savings use in‐network facili es.
Above are poten al ways to save money on the cost of medical care and prescrip ons. Actual results may vary.
This Benefits‐At‐A‐Glance booklet is designed to provide basic informa on to employees on benefit plans and programs available October 01, 2021– September 30,
2022. It does not detail all of the provisions, restric ons and exclusions of the various benefit programs documented in the carrier contract or the Summary Plan
Descrip on (SPD). This booklet does not cons tute an SPD or Plan Document as defined by the Employee Re rement Income Security Act (ERISA). 11Health Savings Account (HSA) ‐ TI5/TF5 HDHP Only
EBC (Employee Benefits Corpora on)
Website: www. Ebcflex.com
Phone number: 1‐800‐346‐2126
Health Saving Account (HSA)
A health savings account (HSA) combines high deduc ble health insurance with a tax‐favored savings account. Money in the
savings account can help pay the costs of qualified medical expenses not covered by medical insurance for you and your
dependents. Money le in the savings account earns interest and is yours to keep.
City of New Smyrna Beach will contribute $1,250.00 annually to an HSA for employees who enroll in the Florida
Healthcare TI5/TF5 HDHPPlan:
MAXIMUM ANNUAL CONTRIBUTIONS 2021 2022
Self ‐ Only Contribu on Limit $3,600 $3,650
Family Contribu on Limit $7,200 $7,300
Catch‐up Contribu on (Age 55 & Older) $1,000 $1,000
EMPLOYEE OWNED ACCOUNT
Pre‐tax contribu ons
Pay for any qualified medical, dental & vision expenses for yourself, spouse or dependents even if they are
enrolled under another medical plan. (See IRS Publica on 502 for a complete list of qualified medical expenses–
sample list below).
Acupuncture Blood pressure monitor Crutches/Wheelchair Lasik/Vision Correc on Surgery Psychologist fees
Alcohol or Drug addic on Breast Pumps and Supplies/ Dental Services Long‐Term Care Smoking Cessa on
treatment Accessories
Ambulance Chiropractor Care Diabe c monitors, test kits, Medicines (prescrip on & Speech Therapy
strips & supplies over‐the‐counter)
Bandages Coinsurance & Copayments Fer lity Treatment Oxygen Sunscreen
Birth Control Contact Lenses & Glasses Hearing aids & ba eries Psychiatric Care Vasectomy
To be HSA‐eligible for a month, an individual must:
Be covered by an HDHP on the first day of the month;
Not be covered by other health coverage that is not an HDHP (with certain excep ons);
Not be enrolled in Medicare; and
Not be eligible to be claimed as a dependent on another person’s tax return.
Why might an HSA be the right choice for you?
It saves you money. For individuals with few regular health expenses, paying a tradi onal health plan premium can feel
like throwing money out the window. HDHPs come with much lower premiums than tradi onal health plans, meaning
less money is deducted from your paychecks. Plus, HSAs are basically “cash” accounts, so you may be able to nego ate
pricing on many medical services.
It’s portable. Even if you change jobs, you get to keep your HSA.
It’s a tax saver. Contribu ons to your HSA are made with pre‐tax dollars. Since your taxable income is decreased by your
contribu ons, you pay less in taxes.
It allows for an improved re rement account. Funds roll over at the end of each year and accumulate tax‐free, as does
the interest on the account. Also, once you reach the age of 55, you are allowed to make addi onal “catch‐up”
contribu ons to your HSA un l age 65.
It puts money in your pocket. You never lose unused HSA funds. They always roll over to the next year.
This Benefits‐At‐A‐Glance booklet is designed to provide basic informa on to employees on benefit plans and programs available October 01, 2021– September 30,
2022. It does not detail all of the provisions, restric ons and exclusions of the various benefit programs documented in the carrier contract or the Summary Plan
Descrip on (SPD). This booklet does not cons tute an SPD or Plan Document as defined by the Employee Re rement Income Security Act (ERISA). 12Flexible Spending Account (FSA)
Those enrolling on the HDHP are not eligible for the Medical FSA.
EBC (Employee Benefits Corpora on)
Website: www. Ebcflex.com
Phone number: 1‐800‐346‐2126
Requirements of an FSA:
Flexible Spending Account
Only certain medical, dental, and vision expenses can be reimbursed
USE IT OR LOSE IT
Pre‐tax contribu ons
Cannot reimburse for dependent care expenses from medical FSA
Full Health Care FSA:
All benefit eligible employees may contribute pre‐tax dollars to pay for any IRS eligible
expenses not covered by insurance.
Maximum annual contribu on: $2,750
Dependent Care FSA:
Available to all benefit eligible employees regardless of medical plan selec on.
Maximum contribu on: $5,000
Savings Example:
Deposits (Reduc on in Taxable Income) $1,500
Federal Income Tax Savings* $300
FICA Tax Savings** $114
YEARLY TAX SAVINGS
INCREASE IN TAKE‐HOME PAY $414
**Includes Social Security tax rate of 6.2% and Medicare tax
rate of 1.45% and assumes Federal Income Tax Rate of 20%
This Benefits‐At‐A‐Glance booklet is designed to provide basic informa on to employees on benefit plans and programs available October 01, 2021– September 30,
2022. It does not detail all of the provisions, restric ons and exclusions of the various benefit programs documented in the carrier contract or the Summary Plan
Descrip on (SPD). This booklet does not cons tute an SPD or Plan Document as defined by the Employee Re rement Income Security Act (ERISA). 13Dental Insurance
Did you know that poor oral health can lead to many seemingly
unrelated medical condi ons? In fact, oral bacteria and oral disease
have been linked to a variety of serious illnesses, including heart
disease, and diabetes.
City of New Smyrna Beach offers eligible employees a PPO dental plan through
Metlife. This plan offers both in and out of network coverage but you will have
the least out of pocket expenses when using in network providers.
Tip
When using in network den sts you can dras cally lower your out of pocket expenses. Visi ng
in network den sts guarantees you will be charged the contracted rate for the services you
have done. While you do have the flexibility of visi ng either an in or out of network den st
when enrolled in a PPO plan, it will always save you money by using a den st in network. To
find in network den sts, you can visit www.metlife.com.
This Benefits‐At‐A‐Glance booklet is designed to provide basic informa on to employees on benefit plans and programs available October 01, 2021– September 30,
2022. It does not detail all of the provisions, restric ons and exclusions of the various benefit programs documented in the carrier contract or the Summary Plan
Descrip on (SPD). This booklet does not cons tute an SPD or Plan Document as defined by the Employee Re rement Income Security Act (ERISA). 14Dental Summary ‐ PPO
The summary below provides a high level overview of the PPO Dental plan offered to you through Metlife.
Website: www.metlife.com
Telephone number: 800‐942‐0854
To use your MetLife PPO dental plan, just call the dental office and verify that the den st is a par cipa ng den st.
Par cipa ng den sts are general den sts or specialists who have agreed to accept MetLife’s nego ated fees (PDP Fee
Schedule) . PDP is short for Preferred Den st Program . If you need a list of den sts in your area, visit the website at
Dental Insurance
www.metlife.com or by calling 1‐800‐942‐0854.
By u lizing a Preferred Den st, you will usually pay the lowest amount for services, and you are only charged the
pa ent share of cost (if any) at the me of treatment.
You do have the freedom to u lize a non‐par cipa ng den st, but by doing so, it o en costs you more money. You are
responsible for the difference between the amount your dental plan pays and the amount a non‐par cipa ng den st
bills. You may also have to pay the en re amount of the non‐par cipa ng den st’s charges in advance and wait for
reimbursement, and you may have to complete and submit your own claim forms or pay a non‐par cipa ng den st a
service fee to submit them for you.
Dental Services In‐Network Out‐of‐Network
Annual Maximum Benefit $1,750
Policy Year Deduc ble: $50 ($150 Family) $50 ($150 Family)
PREVENTATIVE PROCEDURES: Deduc ble Waived
Rou ne Oral Exams (1 in 6 months)
Prophylaxis [Cleanings] (1 in 6 months)
X‐rays – Bitewing (1 per 12 months)
X‐rays – Full Mouth (1 per 60 months) 100% of PDP Fee Schedule 80% of PDP Fee Schedule
Fluoride Treatment (1 per 12 months – up to age 14)
Sealants (1st and 2nd non restored molars—1 in 60
months , up to age 14)
BASIC PROCEDURES: Deduc ble Applies
Fillings (1 in 24 months)
Endodon cs (Root Canal) ‐ 1 per tooth per life me
Oral Surgery 80% of PDP Fee Schedule 80% of PDP Fee Schedule
General Anesthesia/ IV Seda on
Periodontal Scaling (1 in 24 months)
MAJOR PROCEDURES: Deduc ble Applies
Periodontal Surgery (1 in 36 months)
Crowns ‐ (1 in 10 years)
Bridges ‐ (1– in 10 years) 50% of PDP Fee Schedule 50% of PDP Fee Schedule
Dentures ‐ (1 in 10 years)
Implants‐ (1 in 10 years)
** Please refer to your MetLife Plan Design Summary for
limita ons on these benefits. Some examples of limita ons on Who is covered PPO Dental
services are the number of covered cleanings and oral exams,
Employee $0.00
and me limita ons on filling and crown replacement.
Employee + Spouse $8.49
Dental plan costs Employee + Child(ren) $8.89
per paycheck Family $17.10
City contributes 100% of the employee cost and 50%
of the dependents cost.
This Benefits‐At‐A‐Glance booklet is designed to provide basic informa on to employees on benefit plans and programs available October 01, 2021– September 30,
2022. It does not detail all of the provisions, restric ons and exclusions of the various benefit programs documented in the carrier contract or the Summary Plan
Descrip on (SPD). This booklet does not cons tute an SPD or Plan Document as defined by the Employee Re rement Income Security Act (ERISA). 15Vision Insurance
Tip Driving to work, reading a news ar cle and watching television are
Op ons on your likely ac vi es you perform every day. Your ability to do all of these,
glasses such as UV
however, depends on your vision and eye health. Rou ne eye exams
coa ng,
progressive will help maintain your vision as well as detect various eye problems
lenses, etc., which and concerns about your overall health.
are not covered‐in
‐full, may be
available at a
discount at City of New Smyrna Beach offers vision coverage through MetLife.
par cipa ng Similar to your other benefits, using the vision plan in network offers
providers.
the most coverage. When using the plan out of network, you will pay
the full fee out of pocket and then submit a claim to be reimbursed up
to a certain amount (depending on the service obtained) by MetLife.
This Benefits‐At‐A‐Glance booklet is designed to provide basic informa on to employees on benefit plans and programs available October 01, 2021– September 30,
2022. It does not detail all of the provisions, restric ons and exclusions of the various benefit programs documented in the carrier contract or the Summary Plan
Descrip on (SPD). This booklet does not cons tute an SPD or Plan Document as defined by the Employee Re rement Income Security Act (ERISA). 16Vision Summary
The summary below provides a high level overview of the vision plan offered to you through MetLife.
Vision Services In‐Network Out‐of‐Network Contact Lens and Frame Allowances
Vision Insurance
Copays
Eye Exams $10 copay Reimbursed up $45
Single vision lenses $25 copay Reimbursed up to $30 $130 (a er $25
Bifocal vision lenses $25 copay Reimbursed up to $50
Frames copay) every
24 months
Trifocal vision lenses $25 copay Reimbursed up to $65
Frames $130 Allowance Reimbursed up to $70
Contact Lenses $130 Allowance Reimbursed up to $105
Contact Lenses
Frequencies for Services $130 every 12
Eye Exams months
Contact Lenses 12 months (in lieu of glasses)
Lenses for Glasses
Frames 24 months
*Contacts and eyeglasses cannot be purchased in the same year
Addi onal Informa on
Choose from a large network of ophthalmologists, optometrists and op cians, from private prac ces to retailers
like Costco® Op cal and Visionworks.
Polycarbonate (child up to age 18) and UV Coa ng: Covered in full a er $25 eyewear copay.
Progressive, Polycarbonate (adult), Photochromic, An ‐reflec ve, Scratch‐resistance coa ngs and Tints: Your cost
will be limited to a copay that Metlife has nego ated for you. These copays can be viewed a er enrollment at
metlife.com/mybenefits.
Who is covered Cost
Employee $4.01
Vision plan costs Employee + Spouse $8.04
per paycheck Employee + Child(ren) $6.80
Family $11.22
This Benefits‐At‐A‐Glance booklet is designed to provide basic informa on to employees on benefit plans and programs available October 01, 2021– September 30,
2022. It does not detail all of the provisions, restric ons and exclusions of the various benefit programs documented in the carrier contract or the Summary Plan
Descrip on (SPD). This booklet does not cons tute an SPD or Plan Document as defined by the Employee Re rement Income Security Act (ERISA). 17Life Insurance
Having life insurance is important for people of all ages and the below
ques ons may help you think more clearly about your needs and the
benefits of enrolling in life insurance coverage:
Are you the primary household income?
Tip Do you have a mortgage, college loans or other unpaid loans?
Keeping your Could you (or your family) afford thousands of dollars in medical bills and/or
beneficiary up to funeral costs?
date is very
Who would have the burden of paying any debt or other financial
important. You
responsibili es that you leave behind?
can change your
beneficiary or add
addi onal
Basic Life & Accidental Death & Dismemberment Coverage ‐
beneficiaries at
any point during NO COST BENEFIT
the year. The City of New Smyrna Beach provides group term life insurance and accidental death and
dismemberment coverage through The Standard to all eligible full‐ me employees. The amount of
coverage varies depending on your job classifica on as noted on the below chart. For ac ve full
me employees, the benefit amount is equal to the employee’s salary, rounded up to the next
$1,000 not to exceed $200,000. Employees will be eligible the first of the month following a 30 day
wai ng period, a er date of hire. The cost of this insurance is paid en rely by the City of New
Smyrna Beach.
Classifica on Job Classifica ons Included Coverage Amount Employer Contribu on
Class I All Eligible Employees 1x Salary, up to $200,000 100%
Class II All Commissioners $25,000 100%
This Benefits‐At‐A‐Glance booklet is designed to provide basic informa on to employees on benefit plans and programs available October 01, 2021– September 30,
2022. It does not detail all of the provisions, restric ons and exclusions of the various benefit programs documented in the carrier contract or the Summary Plan
Descrip on (SPD). This booklet does not cons tute an SPD or Plan Document as defined by the Employee Re rement Income Security Act (ERISA). 18Voluntary Employee Paid Life
Website: www.standard.com; Telephone number: 800‐628‐8600
Voluntary Life & AD&D
Guaranteed Issue $150,000
Con nuing employee guaranteed coverage annual in‐ May increase up to 2 increments, up to GI (Employees not
crease amount during Open Enrollment currently enrolled may enroll in amounts of $10,000 or
$20,000)
Minimum Benefit Amount/Maximum Benefit Amount $10,000/$500,000 or 5x salary (lesser of)
Life Insurance
Increments of…. $10,000
Voluntary Spouse Life & AD&D
Spouse Guaranteed Issue $50,000
Con nuing employee guaranteed coverage annual in‐ May increase up to 2 increments, up to GI (Employees not
crease amount during Open Enrollment currently enrolled may enroll in amounts of $5,000 or $10,000)
Maximum Benefit Amount $250,000 (not to exceed 50% of EE’s amount)
Increments of…. $5,000
Voluntary Child(ren) Life & AD&D
Birth to 25 years $10,000
Addi onal Informa on
The total amount of life insurance you have (combining your Basic Life and Voluntary Life Insurance amounts) cannot
exceed eight (8) mes your annual salary
Age‐bracketed premiums: rate increase per 5 year increment
You must purchase Voluntary Life Insurance for yourself in order to purchase Voluntary Life Insurance for your eligible
dependents
Evidence of Insurability form (medical ques onnaire) is required for employees increasing or enrolling in coverage
amounts above the guaranteed issue amounts for employee, spouse, child(ren). Guarantee Issue amounts only apply to
new hires. If you do not apply when first eligible, you will need to complete and Evidence of Insurability Form (medical
ques onnaire)
Portability/Conversion ‐ These features allow you to con nue your life insurance coverage should you leave your
employer for any reason, without having to provide evidence of insurability (informa on about your health). The Basic
Life (paid by the employer) can be converted into an individual life insurance policy by the employee directly through
The Standard. The Voluntary Life (paid by the employee) is portable, meaning the policy can remain in force by the
employee a er employment ends. Call The Standard since applica on and premium must be remi ed to the carrier
within 31 days of your leaving employment.
Accelerated Living Benefit ‐ The Accelerated Living Benefit feature is standard with voluntary term life coverage and is
available to you exclusively. This benefit allows you to apply for a percentage of your life insurance in advance should a
licensed physician diagnose you as having a terminal health condi on. Please see your human resources department for
more informa on.
Life benefits automa cally reduce beginning at age 65 and con nue to reduce at the following intervals:
Age 65 ‐ 35% reduc on of original amount; Age 70 ‐ 50% reduc on of original amount
Spouse coverage terminates at employee’s age 70
Your voluntary life policy terminates at re rement, however you have the op on of purchasing employer paid life
insurance upon re rement in the amount of half your annual salary rounded up to the next one thousand with a
maximum volume of $50,000
This Benefits‐At‐A‐Glance booklet is designed to provide basic informa on to employees on benefit plans and programs available October 01, 2021– September 30,
2022. It does not detail all of the provisions, restric ons and exclusions of the various benefit programs documented in the carrier contract or the Summary Plan
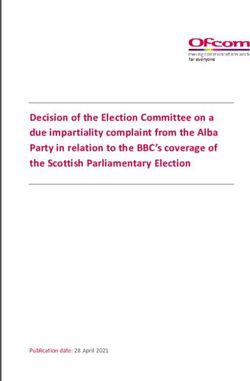
Descrip on (SPD). This booklet does not cons tute an SPD or Plan Document as defined by the Employee Re rement Income Security Act (ERISA). 19Voluntary Life Insurance ‐ Bi‐Weekly Premium Chart
(24 Insurance deduc ons)
Exact amounts to be determined by The Standard
Voluntary Employee Life Rates
AgeVoluntary Life Insurance ‐ Bi‐Weekly Premium Chart
(24 Insurance deduc ons)
Exact amounts to be determined by The Standard
Voluntary Spouse Life Rates
(use the employee’s age and not spouse’s age)
Age < 30 30—34 35—39 40—44 45—49 50—54 55—59 60—64 65—69
Rate 0.06 0.06 0.11 0.17 0.28 0.45 0.7 0.98 1.61
Life Insurance
$5,000 $0.15 $0.15 $0.28 $0.43 $0.70 $1.13 $1.75 $2.45 $4.03
$10,000 $0.30 $0.30 $0.55 $0.85 $1.40 $2.25 $3.50 $4.90 $8.05
$15,000 $0.45 $0.45 $0.83 $1.28 $2.10 $3.38 $5.25 $7.35 $12.08
$20,000 $0.60 $0.60 $1.10 $1.70 $2.80 $4.50 $7.00 $9.80 $16.10
$25,000 $0.75 $0.75 $1.38 $2.13 $3.50 $5.63 $8.75 $12.25 $20.13
$30,000 $0.90 $0.90 $1.65 $2.55 $4.20 $6.75 $10.50 $14.70 $24.15
$35,000 $1.05 $1.05 $1.93 $2.98 $4.90 $7.88 $12.25 $17.15 $28.18
$40,000 $1.20 $1.20 $2.20 $3.40 $5.60 $9.00 $14.00 $19.60 $32.20
$45,000 $1.35 $1.35 $2.48 $3.83 $6.30 $10.13 $15.75 $22.05 $36.23
$50,000 $1.50 $1.50 $2.75 $4.25 $7.00 $11.25 $17.50 $24.50 $40.25
$55,000 $1.65 $1.65 $3.03 $4.68 $7.70 $12.38 $19.25 $26.95 $44.28
$60,000 $1.80 $1.80 $3.30 $5.10 $8.40 $13.50 $21.00 $29.40 $48.30
$65,000 $1.95 $1.95 $3.58 $5.53 $9.10 $14.63 $22.75 $31.85 $52.33
$70,000 $2.10 $2.10 $3.85 $5.95 $9.80 $15.75 $24.50 $34.30 $56.35
$75,000 $2.25 $2.25 $4.13 $6.38 $10.50 $16.88 $26.25 $36.75 $60.38
$80,000 $2.40 $2.40 $4.40 $6.80 $11.20 $18.00 $28.00 $39.20 $64.40
$85,000 $2.55 $2.55 $4.68 $7.23 $11.90 $19.13 $29.75 $41.65 $68.43
$90,000 $2.70 $2.70 $4.95 $7.65 $12.60 $20.25 $31.50 $44.10 $72.45
$95,000 $2.85 $2.85 $5.23 $8.08 $13.30 $21.38 $33.25 $46.55 $76.48
$100,000 $3.00 $3.00 $5.50 $8.50 $14.00 $22.50 $35.00 $49.00 $80.50
Age Reduc on Schedule applies to the shaded columns above and on previous page.
Child coverage for age 6 months to 19 years is $2 per month for $10,000 in coverage.
(Full me Student up to age 30)
(Newborns age 14 days to 6 months coverage is $250 )
This Benefits‐At‐A‐Glance booklet is designed to provide basic informa on to employees on benefit plans and programs available October 01, 2021– September 30,
2022. It does not detail all of the provisions, restric ons and exclusions of the various benefit programs documented in the carrier contract or the Summary Plan
Descrip on (SPD). This booklet does not cons tute an SPD or Plan Document as defined by the Employee Re rement Income Security Act (ERISA). 21Short Term Disability Insurance and Employee Assistance Program Employer Paid Short Term Disability Website: www.standard.com Telephone number: 800‐368‐2859 City of New Smyrna Beach provides short term disability coverage through The Standard. The cost of the short‐term disability benefit is paid en rely by the City of New Smyrna Beach. This income protec on is provided in the event you become injured or disabled and cannot work for a period of me. Your short‐term disability insurance will pay you for periods of me you are unable to work due to sickness or non‐work related accidents. Your income replacement benefit would equal 66.67% of your basic weekly earnings. The maximum weekly benefit you can receive is $1,500. Benefits will begin on the 15th day following a disabling illness or injury and will con nue while you are disabled for up to 13 weeks. This Benefits‐At‐A‐Glance booklet is designed to provide basic informa on to employees on benefit plans and programs available October 01, 2021– September 30, 2022. It does not detail all of the provisions, restric ons and exclusions of the various benefit programs documented in the carrier contract or the Summary Plan Descrip on (SPD). This booklet does not cons tute an SPD or Plan Document as defined by the Employee Re rement Income Security Act (ERISA). 22
Employee Assistance Program (EAP)
Website: www.resourcesforliving.com
Telephone number: 1‐800‐272‐7252
We all experience mes when we need a li le help with life’s challenges. Your employer understands
Addi onal Benefits
this and is providing Aetna’s Resources for Living, an employee assistance program (EAP) to offer
support, guidance and resources to help you and your family resolve personal issues. This service is
paid for en rely by the City of New Smyrna Beach and is provided at no cost to the employee.
Resources for Living can help with the following issues, among others:
• Child Care and Elder Care • Depression
• Alcohol and drug abuse • Personal achievement
• Life Improvement • Emo onal well‐being
• Difficul es in rela onships • Financial and legal concerns
• Stress and anxiety with work or family • Grief and loss
When is it available?
Telephone consulta on and online access to EAP services are always available. Simply call the toll‐
free number or logon to www.resourcesforliving.com and enter the login ID and password. This
program also includes up to six (6) face‐to‐face assessment and counseling sessions. Resources for
Living will work with you to schedule appointments according to your needs.
Is it confiden al?
Your calls and all counseling services are completely confiden al. Informa on will be released only
with your permission or as required by law. Please see your human resources department for
addi onal informa on regarding your EAP program.
Call 1‐800‐272‐7252 or visit www.resourcesforliving.com.
Your username is: CNSB and your password is: CNSB.
This Benefits‐At‐A‐Glance booklet is designed to provide basic informa on to employees on benefit plans and programs available October 01, 2021 – September 30,
2022. It does not detail all of the provisions, restric ons and exclusions of the various benefit programs documented in the carrier contract or the Summary Plan
Descrip on (SPD). This booklet does not cons tute an SPD or Plan Document as defined by the Employee Re rement Income Security Act (ERISA). 23MetLaw and FraudScout
Website: www.info.legalplans.com
Telephone number: 800‐821‐6400 (Hya Legal Plans)
$21.75 per month (includes both MetLaw and FraudScout).
MetLaw and FraudScout
When life calls for legal help, MetLaw is there for you.
MetLaw covers you, your spouse and dependents. Telephone and office consulta ons are available for an
unlimited number of personal legal ma ers with an a orney of your choice.
MetLaw consulta ons include money ma ers, home and real estate issues, estate planning, family ma ers, civil
lawsuit assistance, elder care issues and many other items.
To learn more, visit info.legalplans.com and enter access code: 9560010 or call the Client Service Center at
1.800.821.6400 Monday‐Friday, 8am‐8pm (EST Time).
FraudScout® is there for you in the fight against iden ty fraud.
Early detec on is the best protec on and is the first line of defense in the fight against iden ty fraud.
FraudScout is an integrated pla orm that goes beyond simple credit monitoring to provide comprehensive
fraught and credit monitoring services coupled with 24/7 dedicated support. FraudScout’s comprehensive
coverage scours records and all three major credit bureaus to help uncover and minimize fraud. Iden ty
monitoring and protec on services are only available to the member and spouse.
Credit Report & Monitoring Cyber Monitoring
Review three bureau credit monitoring of credit ac v‐ Protects you by providing a service that con nually
i es, including credit inquires, delinquencies, judge‐ monitors the internet and alerts you of any possible
ments, and more. suspicious ac vity
Credit Score Summary $1 Million Iden ty The Expense Reimbursement
Provides a dashboard view of credit score from all If necessary, the member/spouse shall receive Ex‐
three credit bureaus. You get one free annual credit pense Reimbursement for the following: reasonable
report to keep tabs on ac vity and be on the lookout and necessary costs incurred, lost wages, legal de‐
for new lines of credit. fense fees and expenses, and unauthorized electroni‐
ca fund transfer reimbursement.
FraudScout® Monitoring and Alert:
At‐a‐glace dashboard allows you to see and update personal informa on, and understand any
FraudScout alerts.
This Benefits‐At‐A‐Glance booklet is designed to provide basic informa on to employees on benefit plans and programs available October
January 01, 2018–
2021– December
September31,
30,
2022.
2018. It does not detail all of the provisions, restric ons and exclusions of the various benefit programs documented in the carrier contract or the Summary Plan
Descrip on (SPD). This booklet does not cons tute an SPD or Plan Document as defined by the Employee Re rement Income Security Act (ERISA). 24Enrollment Instructions
To enroll in benefits, go to: h ps://benefits.plansource.com
Plansource Enrollment Instruc ons
Login Page: Enter username & password to get
started.
Username: Your username is the first ini al of
your first name, up to the first six le ers of your
last name, and the last four digits of your SSN.
For example, if your name is Taylor Wil‐
liams, and the last four digits of your SSN
are 1234, your username would be
twillia1234.
Password: Your ini al password is your birthdate
in the YYYYMMDD format.
Homepage
On the Homepage, click
“Get Started” to begin.
This Benefits‐At‐A‐Glance booklet is designed to provide basic informa on to employees on benefit plans and programs available October
January 01, 2018–
2021– December
September31,
30,
2022.
2018. It does not detail all of the provisions, restric ons and exclusions of the various benefit programs documented in the carrier contract or the Summary Plan
Descrip on (SPD). This booklet does not cons tute an SPD or Plan Document as defined by the Employee Re rement Income Security Act (ERISA). 25Enroll in Benefits
Profile
First, you’ll be asked to
review and update your
profile and ensure that all
informa on listed about
yourself and your family
Plansource Enrollment Instruc ons
members is correct.
Shop for Benefits
You can then begin
shopping for benefits!
Educa onal material about
the specific plan type is
available at the top of the
page.
Note: the plans, products
and pricing in the
illustra on on this page do
not reflect the plans or
pricing offered by the City
of New Smyrna Beach and
are only instruc onal on
how to use the Plansource
enrollment pla orm.
This Benefits‐At‐A‐Glance booklet is designed to provide basic informa on to employees on benefit plans and programs available October 01, 2021– September 30,
2022. It does not detail all of the provisions, restric ons and exclusions of the various benefit programs documented in the carrier contract or the Summary Plan
Descrip on (SPD). This booklet does not cons tute an SPD or Plan Document as defined by the Employee Re rement Income Security Act (ERISA). 26Plan Details
The plan detail page will give
you informa on about each
Plansource Enrollment Instruc ons
plan, including deduc ble,
cost per pay period and
projected costs.
Select Plan
To select a plan, indicate
which family members are
covered by clicking “edit
family covered” and select
the card for each family
member you’d like to be on
the plan.
Click “Update Cart” to
choose the plan.
Shopping Cart
The shopping cart displays a
running total of your
combined benefits costs and
shows your progress. You will
need to select or decline a
plan in each benefit type
before you can check out.
Checkout
To finalize your choices, click
“Review and Checkout and
then “Checkout”. You must
complete the checkout
process in order to be
enrolled in benefits.
There is one final
“Checkout” you must click to
finalize your selec ons.
This Benefits‐At‐A‐Glance booklet is designed to provide basic informa on to employees on benefit plans and programs available October
January 01, 2018–
2021– December
September31,
30,
2022.
2018. It does not detail all of the provisions, restric ons and exclusions of the various benefit programs documented in the carrier contract or the Summary Plan
Descrip on (SPD). This booklet does not cons tute an SPD or Plan Document as defined by the Employee Re rement Income Security Act (ERISA). 27Special Enrollment Rights No ce Health Insurance Portability and Accountability Act (HIPAA) No ce
If you are declining enrollment for yourself or your dependents (including Federal law requires that group health plans allow certain employees and
your spouse) because of other health insurance or group health plan dependents special enrollment rights when they previously declined
coverage, you may be able to enroll yourself and your dependents in this coverage and when they have new dependents. This law, the Health
plan if you or your dependents lose eligibility for that other coverage (or if Insurance Portability and Accountability Act (HIPAA) also addresses the
the employer stops contribu ng towards your or your dependents' other circumstances under which treatment for medical condi on may be
coverage). However, you must request enrollment within 30 days a er your excluded from health plan coverage.
or your dependents' other coverage ends (or a er the employer stops This Informa on in this no ce is intended to inform you, in a summary
contribu ng toward the other coverage). fashion, of your rights and obliga ons under these laws. You, your spouse
Important No ces
In addi on, if you have a new dependent as a result of marriage, birth, and any dependents should all take the me to read the en re no ce
adop on, or placement for adop on, you may be able to enroll yourself and carefully.
your dependents. However, you must request enrollment within 30 days Special Enrollments: If you decline enrollment for yourself or your
a er the marriage, birth, adop on, or placement for adop on. dependents (including your spouse) because of having other health
Special enrollment rights also may exist in the following circumstances: insurance coverage at the me of your eligibility to par cipate, you may
enroll yourself or your dependents at a future point, provided that you
If you or your dependents experience a loss of eligibility for
request enrollment within 30 days a er your other coverage ends. In
Medicaid or a state Children’s Health Insurance Program
addi on, if you have a new dependent as a result of a marriage, birth,
(CHIP) coverage and you request enrollment within 60 days
adop on or placement for adop on, you may be able to enroll yourself and
a er that coverage ends; or
your dependents, provided that you request enrollment within 30 days of
If you or your dependents become eligible for a State such an event.
premium assistance subsidy through Medicaid or a state If you or your dependents lose eligibility for coverage under Medicaid or the
CHIP with respect to coverage under this plan and you Children’s Health Insurance Program (CHIP) or become eligible for a
request enrollment within 60 days a er the determina on premium assistance subsidy under Medicaid or CHIP, you may be able to
of eligibility for such assistance. enroll yourself and your dependents. You must request enrollment within 60
If you or your dependents lose eligibility for coverage under days of the loss of Medicaid or CHIP coverage or the determina on of
Medicaid or the Children’s Health Insurance Program (CHIP) eligibility for a premium assistance subsidy.
or become eligible for a premium assistance subsidy under Obtaining Addi onal Informa on: If you need assistance in determining
Medicaid or CHIP, you may be able to enroll yourself and your rights under ERISA or HIPAA, you may contact your Plan Administrator
your dependents. You must request enrollment within 60 or the U.S. Department of Labor by wri ng to the Chicago Regional office at
days of the loss of Medicaid or CHIP coverage or the 200 W. Adams Street, Suite 1600, Chicago, IL 60606, or by calling the
determina on of eligibility for a premium assistance Department at (312)353‐0900.
subsidy. If you have any ques ons about this no ce or the law, please contact your
Note: The 60 day period for reques ng enrollment applied only in these last Plan Administrator at the number or loca on provided in your benefits
two listed circumstances rela ng to Medicaid and state CHIP. As described booklet or Summary Plan Descrip on.
above, a 30‐day period applied to most special enrollments. Also, if you have changed marital status, or if you, your spouse or any other
qualified dependents have changed addresses, please no fy your local
Women’s Health & Cancer Rights Act of 1998 Human Resources Representa ve.
The Women’s Health and Cancer Act (WHCRA) requires group health plans No ce of Privacy Prac ces: Plan administrators, clearinghouses, business
to provide par cipants with no ces of their rights under WHCRA, to provide associates, and health care providers that transmit health informa on
certain benefits in connec on with a mastectomy, and to provide other electronically or use electronic health records may not redistribute or
protec ons for par cipants undergoing mastectomies. If you have had or are unlawfully use electronic health records without permission from the
going to have a mastectomy , you may be en tled to certain benefits under insured. The insured may request informa on on how their electronic
the Women’s Health and Cancer Rights Act of 1998 (WHCRA). For Individuals records are distributed, how frequently they are distributed, and who they
receiving mastectomy –related benefits, coverage will be provided in a are distributed to by contac ng the U.S. Department of Health and Human
manner determined in consulta on with the a ending physician and the Services.
pa ent, for: Health Insurance Marketplace Coverage No ce
All stages of reconstruc on of the breast on which the The Health Insurance Marketplace is available to assist you as you evaluate
mastectomy was performed; health insurance op ons for you and your family. This no ce provides some
basic informa on about the new Marketplace and employment based health
Surgery and reconstruc on of the other breast to produce a coverage offered by your employer. The Marketplace is designed to help you
symmetrical appearance; find private health insurance and compare private health insurance op ons.
Prostheses; and You may also be eligible for a new kind of tax credit under sec on 36B of
Internal Revenue Code that could poten ally lower your monthly premium.
Treatment of physical complica ons of the mastectomy, If you purchase a qualified health plan through the Marketplace, you may
including lymphedema. lose the employer contribu on (if any) to any health benefit plan offered by
These benefits will be provided subject to the same your employer and all or a por on of that contribu on may be excludable
deduc bles and coinsurance amounts applicable to other from income for federal income tax purposes . More informa on on the
medical and surgical benefits provided under the health health insurance Marketplace may be found at h ps://www.healthcare.gov.
plan offered by your employer.
Please keep this informa on with your other group health
plan documents. If you have any ques ons about the Plan’s
coverage of mastectomies and reconstruc ve surgeries,
please contact the Human Resources Department.No ce of Rescission Mental Health Parity & Addic on Equity Act 2008 (MHPAEA)
(a) Prohibi on on rescissions ‐ (1) A group health plan, or a health Under the MHPAEA, the financial requirements and treatment limits that
insurance issuer offering group or individual health insurance coverage, group health plans and health insurance issuers apply to mental health or
must not rescind coverage under the plan, or under the policy, cer ficate, substance use disorder benefits generally cannot be more restric ve than
or contract of insurance, with respect to an individual (including a group to those applicable to medical and surgical benefits. If a plan covers mental
which the individual belongs or family coverage in which the individual is health and substance use disorder, MHPAEA provides medical and surgical
included) once the individual is covered under the plan or coverage, unless benefits and mental health and substance use disorder benefits. MHPAEA
Important No ces
the individual (or a person seeking coverage on behalf of the individual): it must comply with the federal parity requirements. The MHPAEA
contains the following parity requirements:
I. performs an act, prac ce, or omission that cons tutes fraud
The financial requirements (such as deduc bles, copayments, coinsurance
II. makes an inten onal misrepresenta on of material fact, and out‐of‐pocket limits) applicable to mental health and substance use
as prohibited by the terms of the plan or coverage. A group health plan, disorder benefits cannot be more restric ve than the predominant
or a health insurance issuer offering group or individual health insurance financial requirements applied to substan ally all medical and surgical
coverage, must provide at least 30 days advance wri en no ce to each benefits.
par cipant (in the individual market, primary subscriber) who would be Treatment limita ons (such as frequency of treatment, number of visits,
affected before coverage may be rescinded under this paragraph (a)(1), days of coverage or other similar limits on the scope or dura on of
regardless of, in the case of group coverage, whether the coverage is coverage) must also comply with the MHPAEA’s parity requirements. Non‐
insured or self‐insured, or whether the rescission applies to an en re quan ta ve treatment limita ons (such as medical management
group or only to an individual within the group. (The rules of this standards, formulary design and determina ons of usual, customary or
paragraph (a)(1) apply regardless of any contestability period that may reasonable amounts) are subject to a separate parity requirement.
otherwise apply.) A rescission is a cancella on or discon nuance of
coverage that has retroac ve effect. For example, a cancella on that If medical and surgical benefits are offered on an out‐of‐network basis, a
treats a policy as void from the me of the individual's or group's plan or issuer must also offer mental health and substance use disorder
enrollment is a rescission. As another example, a cancella on that voids benefits on an out‐of‐network basis.
benefits paid up to a year before the cancella on is also a rescission for
this purpose. Newborn’s and Mothers’ Health Protec on Act
A cancella on or discon nuance of coverage is not a rescission if ‐ Group health plans and health insurance issuers generally may not, under
Federal law, restrict benefits for any hospital length of stay in connec on
I. The cancella on or discon nuance of coverage has only a with childbirth for the mother or newborn child to less than 48 hours
prospec ve effect; following a vaginal delivery, or less than 96 hours following a cesarean
sec on. However, Federal law generally does not prohibit the mother's or
II. The cancella on or discon nuance of coverage is effec ve
newborn's a ending provider, a er consul ng with the mother, from
retroac vely, to the extent it is a ributable to a failure to mely pay
discharging the mother or her newborn earlier than 48 hours (or 96 hours
required premiums or contribu ons (including COBRApremiums)
as applicable). In any case, plans and issuers may not, under Federal law,
towards the cost of coverage;
require that a provider obtain authoriza on from the plan or the insurance
III. The cancella on or discon nuance of coverage is ini ated by the issuer for prescribing a length of stay not in excess of 48 hours (or 96
individual (or by the individual's authorized representa ve) and the hours).
sponsor, employer, plan, or issuer does not, directly or indirectly,
take ac on to influence the individual's decision to cancel or COBRA (Consolidated Omnibus Budget Reconcilia on Act)
discon nue coverage retroac vely or otherwise take any adverse Cobra provides eligible individuals and their dependents who would
ac on or retaliate against, interfere with, coerce, in midate, or
otherwise lose group health coverage as a result of a qualifying life event
threaten the individual; or with an opportunity to con nue group health coverage for a limited me
IV. The cancella on or discon nuance of coverage is ini ated by the period under certain circumstances such as:
exchange pursuant (the insured).
Voluntary or involuntary job loss
Michelle’s Law
Reduc on in the hours worked
Michelle’s Law protects a postsecondary student from losing full‐ me
student status under an employer’s medical coverage if the student is (i) a Transi on between jobs
dependent child of a par cipant or beneficiary under the terms of the
plan; and (ii) enrolled in a plan on the basis of being student at a Death
postsecondary educa onal ins tu on immediately before the first day of a
medically necessary leave of absence from school. A dependent covered Divorce
under the law is en tled to the same benefits as if the dependent
And other qualifying life events
con nued to be enrolled as a full‐ me student. The law also recognizes
that changes in coverage (whether due to plan design or a subsequent If you are en tled to elect COBRA coverage, you will have 60 days (star ng
annual enrollment elec on) pass through to the dependent for the on the date you are furnished the elec on no ce or the date you would
remainder of the medically necessary leave of absence. lose coverage) to choose whether or not to elect con nua on coverage.You can also read