Central Karoo District - District Health Plan 2018/19 to 2020/21 - Department of Health
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Central Karoo District
Western Cape
District Health Plan
2018/19 to 2020/21
1. EXECUTIVE SUMMARY BY THE DISTRICT MANAGER
The Central Karoo District Health Service functions in partnership with the other health service
rendering entities in the geographic area. This includes the George Regional Hospital, the
Emergency Medical Services, and the Forensic Pathology Services.
In addition we have close ties to the Environmental Health Team of the Central Karoo District
Municipality, and other key role players in the social cluster: Department of Education and Social
development.
There is also increasingly more interaction with the Local Municipalities (political and officials) and
community participation. The Central Karoo district is committed to collaborate with all
stakeholders to ensure that PSG2 and PSG3 are addressed.
For District Health Services, the focus for the year will be on promoting the development of the
principles of Community Orientated Primary Care. All decision-making will be done to enhance the
progress towards the implementation of this model ensuring that that the focus will be on the needs
of the people served and a shift from illness to wellness. This is a model that starts in the home at the
community level, follows through to PHC facility to District hospital and ultimately to the Regional
Hospital in a seamless way.
As part of this development, it also means that Primary Health Care facilities need special attention
to ensure that they are fully functional.
This means, inter alia:
1. Strengthening clinical support
2. Ensuring Supply Chain Management efficiencies.
3. Interrogating doctor and nurse workload to ensure there is maximum efficiency and
equity between the sub-districts.
4. Improving registry hygiene, by improving patient flow, ensuring electronic appointment
systems, having competent clerical /data staff, and ensuring the registries are
functioning efficiently. This should also decrease waiting times, which will improve the
experience that clients have at our facilities.
5. Improving on the quality of data.
From a service priority point of view, there will be emphasis on the 1000 days approach and
ensuring an integrated approach to the management of chronic diseases (HIV/AIDS/TB/Chronic
Diseases of Lifestyle/Mental Health). For the former the focus is on Family Planning, Termination of
Pregnancy, and Basic Antenatal Care. For the latter the focus is on Tuberculosis outcomes and
maximizing efficiencies for processes for Chronic Disease Management, especially with relation to
the alternate sites for collecting chronic medication.
2
For District Hospitals, the focus will be on the Emergency Centres to ensure that they are functioning
well, have the right staff mix and skills, and have the appropriate functioning equipment. Principles
for the full content of an EC will be developed that will need to be in place for every EC. Other
aspects to focus on are ensuring the completion of the eCCR (discharge note) and ICD-10 coding.
There are also major physical infrastructure projects that will be taking place in hospitals and PHC
facilities.
The above all needs to be done in the bigger context of the province where there is further
significant transformation processes taking place: ‘Management Efficiency and Alignment Project’
and a renewed service design process to take the district towards HC 2030. All this will have to be
done within the context of severe fiscal constraints for the 2018/19 financial year. The Central Karoo
district faces many challenges to ensure that its mandate of moving towards increasing wellness is
attained. It will continue to work with its partners to work towards an integrated approach to health
services and to maximize efficiencies. The systems are in place and with its particular strength, the
resilience of its staff, the implementation of the 2018 plan will be undertaken.
3
2. ACKNOWLEDGEMENTS
The District Health Plan was developed by the Central Karoo District based on the District
Health Planning Guidelines provided by the National Department of Health. In particular, the
District would like to thank the following role-players for their contribution and guidance:
Chief Directorate: Rural District Health Services
Dr R. Crous: Chief Director
Dr D. Pienaar
Ms L. Grebe
District Director: Eden and Central Karoo District
Dr H. Schumann
Central Karoo District Office:
Mrs A. Jooste
Dr S. Janicki
Mrs B. Goliath
Central Karoo District Health Council:
Councillor N. Constable (Executive Mayor, Central Karoo District Municipality)
Councillor D. Slabbert (Deputy Mayor, Beaufort West Municipality)
Councillor G. Lottering (Executive Mayor, Prince Albert Municipality)
Councillor L. Potgieter (Councillor, Laingsburg Municipality)
Eden District Office:
Dr T. Marshall
4
3. OFFICIAL SIGN OFF
It is hereby certified that this District Health Plan:
Was developed by the district management team of Central Karoo District with the
technical support from the Chief Directorate: Rural District Health Services and the Strategic
Planning unit at the provincial head office.
Was prepared in line with the current Strategic Plan and Annual Performance Plan of the
Western Cape Department of Health.
Dr H Schumann
District manager: Central Karoo District SIGNATURE
DATE
Executive Mayor N Constable
Chairperson: Central Karoo District Health Council SIGNATURE
DATE
Dr R Crous
Chief Director: Rural District Health Services SIGNATURE
DATE
Dr K Cloete
Chief of Operations SIGNATURE
DATE
Dr B Engelbrecht
Accounting officer (Head of Department) SIGNATURE
DATE
5
4. TABLE OF CONTENTS
1. EXECUTIVE SUMMARY BY THE DISTRICT MANAGER ............................................................. 2
2. ACKNOWLEDGEMENTS .......................................................................................................... 4
3. OFFICIAL SIGN OFF................................................................................................................. 5
4. TABLE OF CONTENTS ............................................................................................................... 6
5. LIST OF ACRONYMS ................................................................................................................ 7
6. EPIDEMIOLOGICAL PROFILE ................................................................................................ 10
6.1 GEOGRAPHIC OVERVIEW .................................................................................................... 10
6.2 DEMOGRAPHIC OVERVIEW ................................................................................................. 10
6.3 SOCIAL DETERMINANTS OF HEALTH .................................................................................... 13
6.4 CAUSES OF MORTALITY ........................................................................................................ 16
6.5 BURDEN OF DISEASE ............................................................................................................. 18
7. SERVICE DELIVERY PLATFORM AND MANAGEMENT ......................................................... 21
7.1 HEALTH FACILITIES PER SUB-DISTRICT .................................................................................. 21
7.2 HUMAN RESOURCES FOR HEALTH (FILLED POSTS) ............................................................. 24
7.3 BASELINE DATA 2016/17 ...................................................................................................... 25
8. QUALITY OF CARE ................................................................................................................. 32
9. ORGANISATIONAL STRUCTURE OF THE DISTRICT MANAGEMENT TEAM .......................... 34
10. DISTRICT HEALTH EXPENDITURE ............................................................................................ 35
11. DISTRICT PERFORMANCE INDICATORS ............................................................................... 36
11.1 DISTRICT HEALTH SERVICES .................................................................................................. 37
11.2 DISTRICT HOSPITALS .............................................................................................................. 40
11.3 HIV AND AIDS, STIs AND TB CONTROL (HAST) ................................................................... 43
11.4 MATERNAL, CHILD AND WOMEN’S HEALTH (MCWH) AND NUTRITION............................ 50
11.5 DISEASE PREVENTION AND CONTROL ................................................................................ 63
12. DISTRICT FOCUS FOR THE YEAR ........................................................................................... 65
13. ORAL HEALTH PLAN .............................................................................................................. 67
ANNEXURE A: CENTRAL KAROO DISTRICT POPULATION ESTIMATES BY AGE ............................. 70
ANNEXURE B: TARGETS FOR SDG 3 – “GOOD HEALTH AND WELL-BEING” ................................. 71
ANNEXURE C: FACILITY LIST ............................................................................................................. 72
ANNEXURE D: TECHNICAL INDICATOR DESCRIPTIONS ................................................................. 73
ANNEXURE E: COMMUNICATION PLAN FOR DISTRICT HEALTH PLAN.......................................... 89
6
5. LIST OF ACRONYMS
AIDS Acquired immune deficiency syndrome
ALOS Average length of stay
APL Approved post list
APP Annual Performance Plan
ART Anti-retroviral treatment
BANC Basic antenatal care
BUR Bed utilisation rate
CBS Community-based services
CDC Community day centre
CDU Chronic dispensing unit
CHC Community health centre
CHW Community health worker
COPC Community oriented primary care
COPD Chronic obstructive pulmonary disease
DHC District Health Council
DHER District Health Expenditure Review
DHP District Health Plan
DHS District Health Services/Systems
DR TB Drug resistant TB
EC Emergency centre
EDR Electronic drug-resistant TB register
EMS Emergency medical services
EPWP Expanded Public Works Programme
ETR.net Electronic TB register
GSA Geographic service area
HAST HIV and AIDS, STIs and TB control
HCBC Home and community based care
HCT HIV counselling and testing
HIV Human immunodeficiency virus
HPV Human papillomavirus
HR Human resource
ICD-10 International classification of disease coding
ICT Information and communication technology
ID Infectious diseases
JAC Electronic Pharmacy Management Inventory System
LG Local government
M&E Monitoring and evaluation
MDG Millennium development goal
7
MDR-TB Multi-drug resistant tuberculosis
MHS Municipal Health Services
MMC Medical male circumcision
MOU Midwife obstetric unit
MTEF Medium-term expenditure framework
MTSF Medium-term strategic framework
NCS National core standards
NDP National Development Plan
NHLS National Health Laboratory Services
NIMART Nurse Initiated Management of Anti-retroviral Therapy
NPO Non-profit organisation
OPD Outpatient department
OSD Occupational specific dispensation
PACK Practical Approach to Care Kit
PCE Patient centred experience
PCR Polymerase chain reaction
PCV Pneumococcal conjugate vaccine
PDE Patient day equivalent
PHC Primary health care
PHCIS Primary Health Care Information Systems
PMTCT Prevention of mother-to-child transmission
PPIP Perinatal problem identification programme
PTB Pulmonary tuberculosis
QIP Quality improvement plan
RCS Rural clinical school
RDHS Rural District Health Services
RIC Retention in care
SAM Severe acute malnutrition
SCM Supply chain management
SD Sub-district
SDG Sustainable development goal
STI Sexually transmitted infection
TB Tuberculosis
TIER.net HIV electronic register
VPUU Violence Prevention through Urban Upgrading
WCG Western Cape Government
WCGH Western Cape Government Health
WCCN Western Cape College of Nursing
WHO World Health Organisation
8
WoW Western Cape on wellness
XDR-TB Extreme drug resistant tuberculosis
YTD Year to date
96. EPIDEMIOLOGICAL PROFILE
6.1 GEOGRAPHIC OVERVIEW
The Central Karoo is one of five rural district municipalities in the Western Cape Province and
is the largest district in the province, making up a third of its geographical area.
The district consists of three local municipalities, namely: Beaufort West, Laingsburg and
Prince Albert. The Central Karoo District Management Area (DMA) was incorporated in the
Beaufort West Sub-district from 1 April 2013.
The district office for Western Cape Government: Health (WCG: Health) is situated in
Beaufort West. There are 18 primary health care (PHC) facilities in the district of which 9 are
fixed facilities. There are four district hospitals and one intermediate care hospital, Nelspoort,
which is located in the Beaufort West Sub-district.
Figure 1: Map of Central Karoo District
[Source: https://municipalities.co.za/map/144/central-karoo-district-municipality]
6.2 DEMOGRAPHIC OVERVIEW
The National Department of Health distributed revised population estimates during 2017,
based on the mid-year population estimates received from Stats SA for 2002 to 2016 and the
short term projections for 2017 to 2021.
10The revised population estimates reflect financial years rather than calendar years as was
previously the case. These estimates will be implemented from 2018/19 going forward and is
reflected in the tables below.
Table 1: Sub-district population size and density 2016/17
Sub-district Town(s) Total Geographic area Population
population(A) (per km²)(B) density
Beaufort West - Beaufort West
- Merweville
51 904 21 917 2
- Murraysburg
- Nelspoort
Laingsburg - Laingsburg
9 043 8 784 1
- Matjiesfontein
Prince Albert - Klaarstroom
- Leeu Gamka 14 391 8 153 2
- Prince Albert
District total 75 338 38 854 2
[Source A: Circular H11/2018: Population data]
[Source B: https://municipalities.co.za/overview/144/central-karoo-district-municipality ]
Central Karoo District is the rural district with the smallest population and the lowest
population density. The sub-districts consist of several towns that are spread out over a large
surface area. Although the number of people who live in this district is small, the vast
geographic area leads to service delivery challenges that are not necessarily experienced
in the other districts.
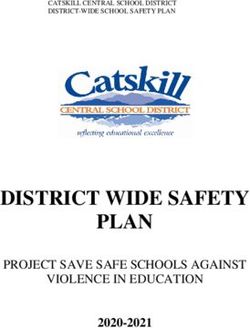
11Figure 2: Sub-district population distribution in Central Karoo District 2016/17
Prince Albert
19.1%
Laingsburg
12.0% Beaufort West
68.9%
[Source: Circular H11/2018: Population data]
Although there is only a 1.5% increase between the total population estimates for 2018/19
(i.e. all age groups) that were release in 2014 and 2017 respectively, there is a 16.7%
increase in the population under 1 year. This will have a significant impact on the district’s
performance for indicators that use the population under 1 year as denominator, e.g. the
immunisation coverage.
For more detailed information on the population breakdown per age group for the district,
refer to Annexure A (page 70).
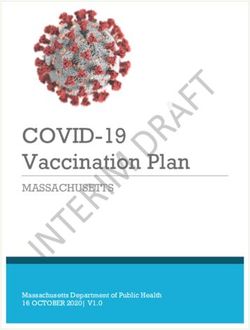
12Figure 3: Central Karoo District population pyramid for 2016/17
80 years and older
75 - 79 years
70 - 74 years
65 - 69 years
60 - 64 years
55 - 59 years
50 - 54 years
45 - 49 years
40 - 44 years
35 - 39 years
30 - 34 years
25 - 29 years
20 - 24 years
15 - 19 years
10 - 14 years
5 - 9 years
Under 5 years
-4 000 -3 000 -2 000 -1 000 0 1 000 2 000 3 000 4 000
Male Female
[Source: Circular H11/2018: Population data]
6.3 SOCIAL DETERMINANTS OF HEALTH
Social determinants may have an impact on the health status outcomes of the district
population.
Table 3: Household dynamics in the Central Karoo District 2016
Age groups Beaufort West Laingsburg Prince Albert District
Households 14 935 2 862 4 183 21 980
Average household size 3.4 3.1 3.4 3.4
Female headed households 39.8% 31.8% 50.3% 40.8%
Formal dwellings 99.6% 97.5% 91.8% 97.8%
Housing owned 66.4% 61.0% 78.9% 68.1%
[Source: https://municipalities.co.za/overview/144/central-karoo-district-municipality ]
Note: The highest and lowest value for each item is coloured orange and green respectively.
13Figure 4: Central Karoo District education levels 2016
Education levels by sub-district
31.8%
35.0%
29.5%
26.3%
30.0%
23.7%
25.0%
20.0%
15.0%
9.2%
10.0%
5.8%
5.4%
4.8%
3.8%
3.2%
2.4%
1.7%
5.0%
0.0%
Beaufort West Laingsburg Prince Albert District
No schooling Matric Higher education
[Source: https://municipalities.co.za/overview/144/central-karoo-district-municipality ]
Figure 5: Central Karoo District household services 2016
Household services by sub-district
120.0%
96.0%
95.9%
95.6%
95.4%
95.3%
95.1%
93.7%
91.7%
90.8%
88.8%
100.0%
82.7%
79.5%
77.9%
73.8%
70.9%
80.0%
56.5%
60.0%
40.0%
20.0%
0.0%
Beaufort West Laingsburg Prince Albert District
Flush toilet connected to sewerage Weekly refuse removal
Piped water inside dwelling Electricity for lighting
[Source: https://municipalities.co.za/overview/144/central-karoo-district-municipality ]
Laingsburg Sub District seems to be worst off in terms of service delivery to households.
According to the IDP document for Laingsburg Municipality the number of households
increased from 2408 (2011) to 2862 (2016). The municipality is dependent on ground water of
which the biggest portion has access to piped water inside the dwelling or within the yard.
The biggest portion of households has access to Eskom electricity utilising it for lighting and
14cooking. Alternative energy is also being used within the municipality. The majority of
households are connected to a sewerage system or chemical toilets but 2.1% of households
make use of other sources of sanitation. Refuse removal are on done on a weekly basis.
Over the next five years, the municipality will be investing in a number of major infrastructure
projects, including upgrade of the electricity Network, provision of new water infrastructure
and upgrading of current water infrastructure.1
Figure 6: Main economic sectors in Central Karoo District
Construction, 7.0% Other,
5.0%
Community services, Agriculture, 47.0%
19.0%
Finance and
business services,
22.0%
[Source: https://municipalities.co.za/overview/144/central-karoo-district-municipality ]
1 Laingsburg Municipality IDP; https://www.laingsburg.gov.za/resource-category/integrated-
development-plan?category=104
156.4 CAUSES OF MORTALITY
Table 4: Leading underlying natural causes of death, Western Cape, 2015
Cape Western
Rank Central Karoo Cape Town Eden Overberg West Coast
Winelands Cape
Chronic lower Ischaemic
Diabetes Diabetes
HIV disease respiratory Tuberculosis heart Tuberculosis
1 mellitus mellitus
(7.2%) diseases (7.0%) diseases (7.9%)
(7.5%) (7.2%)
(9.1%) (7.1%)
Cerebrovasc Cerebrovasc Diabetes
Tuberculosis HIV disease HIV disease HIV disease
2 ular diseases ular diseases mellitus
(6.7%) (6.3%) (6.7%) (6.1%)
(6.9%) (6.6%) (7.4%)
Malignant
Ischaemic Ischaemic
Diabetes Cerebrovasc Cerebrovasc neoplasms of Cerebrovasc
heart heart
3 mellitus ular diseases ular diseases resp & ular diseases
diseases diseases
(6.7%) (6.2%) (6.6%) intrathoracic (7.2%)
(5.7%) (5.8%)
organs (6.5%)
Ischaemic Chronic lower
Cerebrovasc Diabetes Cerebrovasc
Tuberculosis HIV disease heart respiratory
4 ular diseases mellitus ular diseases
(6.6%) (5.2%) diseases diseases
(4.9%) (6.1%) (5.6%)
(6.4%) (6.6%)
Chronic lower Chronic lower Ischaemic
Diabetes Diabetes
respiratory Tuberculosis respiratory heart Tuberculosis
5 mellitus mellitus
diseases (4.5%) diseases diseases (5.3%)
(5.2%) (6.2%)
(6.2%) (5.6%) (5.8%)
Ischaemic Chronic lower Chronic lower Chronic lower
Hypertensive Hypertensive
heart respiratory respiratory Tuberculosis respiratory
6 diseases diseases
diseases diseases diseases (5.0%) diseases
(5.2%) (4.6%)
(5.5%) (4.4%) (5.8%) (5.1%)
Malignant
Malignant Malignant Malignant neoplasms of Malignant Malignant
HIV disease
7 neoplasms neoplasms neoplasms resp & neoplasms neoplasms
(4.6%)
(5.0%) (4.1%) (4.2%) intrathoracic (4.9%) (4.5%)
organs (4.9%)
Malignant Malignant Malignant Malignant
neoplasms of neoplasms of neoplasms of Malignant Hypertensive Malignant neoplasms of
8 resp & resp & resp & neoplasms diseases neoplasms resp &
intrathoracic intrathoracic intrathoracic (4.6%) (4.0%) (4.4%) intrathoracic
organs (5.0%) organs (4.0%) organs (4.2%) organs (4.5%)
Malignant
Ischaemic Other forms Other forms
Hypertensive Hypertensive neoplasms of Hypertensive
heart of heart of heart
9 diseases diseases resp & diseases
diseases disease disease
(3.3%) (4.1%) intrathoracic (4.0%)
(4.0%) (3.7%) (3.3%)
organs (3.7%)
Other forms Other forms Other forms Other forms Other forms
Hypertensive Influenza and
of heart of heart of heart of heart of heart
10 diseases pneumonia
disease disease disease disease disease
(3.4%) (2.8%)
(3.2%) (3.8%) (3.1%) (2.5%) (3.2%)
[Source: Mortality and causes of death in South Africa, 2015: Findings from death notification, Statistical Release
P0309.3]
16A sub-district breakdown of the underlying natural causes of death was not included in the
above publication.
Table 5: Institutional maternal mortality rate (iMMR) in Central Karoo District
2011 2012 2013 2014
Deaths during pregnancy, 0 0 0 3
childbirth and puerperium
iMMR 0 0 0 273.2
[Source: Saving Mothers, 2014]
Note: The source listed above is the latest published Saving Mothers Report.
During the 2014 calendar year, there were 4 maternal deaths in the Central Karoo District. In
2015, 2016 and 2017 there were zero (0) maternal deaths in the district.
The causes for the 2014 maternal deaths were:
Pulmonary embolism
Pulmonary tuberculosis
Preeclampsia
Asthma
Table 6: Infant and child mortality in Central Karoo District
District Infant mortality rate (< 1 year) Child mortality rate (< 5 years)
2011 2012 2013 2011 2012 2013
Central Karoo 33.8 29.6 22.6 41.0 32.7 31.1
[Source: Western Cape Mortality Profile 2013]
Note: The source listed above is the latest published Western Cape Mortality Profile.
The most important point to keep in mind is that the Infant & Child Mortality Rates in rural
districts with small populations must be interpreted with extreme caution. Because of the
small population and the low number of births in the district any infant or child death will
have a significant impact in the calculated rate. The Central Karoo District often shows up
as the ‘best’ or the ‘worst’, but this is because of the very small numbers that are implicated,
in comparison to places with higher numbers. From a purely statistical point of view, the
results show one picture, but the detail needs to be interrogated, and the full context
unpacked.
176.5 BURDEN OF DISEASE
DISTRICT HIV AND AIDS PROFILE
Figure 7: Antenatal Survey HIV prevalence: South Africa vs Western Cape; 1990 - 2015
35.0
30.0
25.0
HIV prevalence (%)
20.0
15.0
10.0
5.0
0.0
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
Western Cape South Africa
[Source: National Antenatal Sentinel HIV & Syphilis Survey Report, 2015]
Figure 8: HIV prevalence among antenatal women, 2010 - 2015
HIV prevalence among antenatal women
35
30
25
HIV prevalence (%)
20
15
10
5
0
2010 2011 2012 2013 2014 2015
South Africa Western Cape Central Karoo
[Source: National Antenatal Sentinel HIV & Syphilis Survey Report, 2015]
HIV prevalence in the Central Karoo district is much lower than that of the Western Cape
and of South Africa.
18DISTRICT TB PROFILE
Management of TB has become complex over the last few years, with HIV that make the
disease more complex to manage. To fulfil this task in managing both diseases, clear
expectations must be set with regards to the specific functions for each level of care, with
clear referral pathways.
Nelspoort Hospital: Ward Garlick: Sensitive TB patients
This is a 12 bed unit for TB sensitive clients.
It is mainly for non-compliant TB clients, as well as TB clients that need extra care due
to social circumstances or illness.
Patients from all the sub-districts in the Central Karoo can be referred.
Clinical Support:
o Medical Officer from Beaufort West visits Ward Garlick on a weekly basis.
o The HAST Coordinator visits Ward Garlick every second week.
o The HAST Coordinator is also responsible for initiation on ART for co-infected
patients.
o The outreach TB specialist from Harry Comay Hospital visits Ward Garlick
every second month.
Nelspoort Hospital Garlick ward: MDR patients:
This is two 4 bed wings at the ends of Ward Garlick for MDR TB patients.
Clinical support is the same as mentioned above.
Additional support includes visits from the audiologist (George) every month.
Nelspoort Hospital Eikenhof ward: XDR patients:
8 Bed Ward used for XDR patients.
XDR patients are referred via the review committees in either Cape Town or George.
If there are no XDR palliative patients, MDR patients are moved to this ward.
The unit is managed by a local NPO.
Patients are voluntary admitted to the Palliative unit.
Patients are also seen if necessary by the clinical team mentioned above.
Priorities:
TB Screening:
Early identification and initiation of treatment is crucial element to eradicate TB. Studies
conducted by Desmond Tutu Foundation showed that patients with infectious TB who
attend health facilities for other reasons are not recognised and treated. Therefore the
Western Cape Department of Health adopted the universal symptom screening for all
19clients entering health facilities. Further to this the department also adopted the 90/90/90
strategy, meaning that 90% of vulnerable people for TB should be identified and treated.
Screening of all contacts exposed to infectious TB has always been one of the priorities of
the TB Control Program and should be maintained. However, monitoring thereof is still
problematic and reporting systems needs to be explored.
Operational managers working in PHC facilities, out-patient and emergency units in
hospitals should ensure that the screening policy is adhered to for all clients entering health
facilities.
TB is a communicable disease which infects contacts in households, work places, schools
and social gatherings. Screening of contacts and high risk groups should be done by
community care workers under the supervision of the CBS coordinators and the NPO’s
contracted to support the program.
Challenges:
Patients defaulting on treatment
Difficulty in tracking patients that default on treatment. Patients move between
facilities, towns, sub district and districts, making it difficult to follow up.
A system was put in place to address the number of patients defaulting on
treatment. The results will reflect in the 2018/2019 outcomes.
207. SERVICE DELIVERY PLATFORM AND MANAGEMENT
7.1 HEALTH FACILITIES PER SUB-DISTRICT
Table 7: Health facilities per sub-district as at 31 March 2017
Sub-district
Central/tertiary
District hospital
outreach team
Ward based
TB hospital
Regional
hospital
hospital
Satellite
Mobile
Clinic
CDC
CHC
Beaufort West 0 4 1 5 1 0 2 0 0 0
Laingsburg 0 1 1 1 0 0 1 0 0 0
Prince Albert 0 1 1 2 0 0 1 0 0 0
Central Karoo 0 6 3 8 1 0 4 0 0 0
[Source: Sinjani]
Improving the experience of patients in health facilities is one of the departmental goals.
The focus areas for primary health care services are:
Improving patient flow in facilities.
Maximising use of the Primary Health Care Information System (PHCIS).
Management of minor ailments.
Improving the system for the management of chronic diseases including clinical
quality.
The focus areas for home community-based care are:
Screening of the population.
Health promotion.
Defaulter tracing.
In terms of the health facilities in the Central Karoo District:
There are no 24-hour PHC facilities.
Fixed clinics (8) are open five days a week between 07h30 and 16h15. Services are
nurse-led with support from visiting doctors.
The community day centre (CDC) is open five days a week between 07h30 and
16h15 and has a full-time doctor in addition to the package of care provided by the
nurse practitioners.
A Community Day Centre (CDC) renders the same service package as a
community health centre (CHC) but does not have a maternity obstetric unit (MOU).
Furthermore, a CDC is only open during office hours, for a maximum of 8 hours per
day.
Contract general practitioners (GPs) are classified as independent consulting rooms.
21Although Beaufort West, Laingsburg and Prince Albert are separate sub-districts, the primary
health care services are managed as one in terms of financial and human resource
management. The district spans a vast geographical area and mobile clinics are a
necessity. The mobile clinics service the following areas:
Beaufort West Mobile Clinic: One mobile clinic serves two large mobile routes
surrounding Beaufort West. The mobile operates on a daily basis with a turn-around
time of 3 months.
Nelspoort Mobile Clinic: The mobile service at Nelspoort was discontinued in
November 2015. There is a need to restore the service.
Merweville Mobile Clinic: One mobile clinic serves a mobile route surrounding
Merweville. The mobile operates three times a week: Monday, Wednesday and
Friday, with a turn-around time of 3 months.
Murraysburg Mobile Clinic: The mobile service at Murraysburg was discontinued in
October 2014. There is a need to restore the service.
Prince Albert Mobile Clinic: One mobile clinic serves a mobile route surrounding
Prince Albert and Leeu Gamka. The mobile operates twice a week, with a turn-
around time of 2 months.
Laingsburg Mobile Clinic: One mobile clinic serves a mobile route surrounding
Laingsburg and Matjiesfontein. The mobile operates twice a week, with a turnaround
time of 2½ months.
The satellite clinics are open on the following days and times:
Merweville Satellite Clinic: Open 2 days a week (Tuesdays and Thursdays) between
07h30 and 16h15.
Klaarstroom Satellite Clinic: Open on a Wednesday between 09h00 and 15h00.
Matjiesfontein Satellite Clinic: Open on a Wednesday between 09h00 and 15h00.
As mentioned previously, fixed clinics are open five days a week between 07h30 and 16h15.
Services are nurse-led with support from visiting doctors. The CDC is open five days a week
between 07h30 and 16h15, but has a full-time doctor in addition to the package of care
provided by nurse practitioners.
The Western Cape Government assumed responsibility for personal primary health care
services in all five rural districts since 2006. Therefore there are no longer any local
government facilities in the Central Karoo District.
The district has multiple mobile vehicles that attend to rural areas, mostly for those on
farms.
The population is wide-spread throughout the district and it remains a challenge to
provide equal access for all.
22 Laingsburg, Murraysburg and Prince Albert Hospitals are small hospitals with bed
numbers below 30. Murraysburg and Prince Albert also have low bed utilisation rates
and average lengths of stay (ALOS). The local situation and context must be taken
into consideration when the hospitals’ functions and performance are evaluated.
Beaufort West Hospital, on the other hand, has a high bed utilisation rate and ALOS.
George Regional Hospital provides outreach to Beaufort West Hospital in the following
disciplines:
Obstetrics and Gynaecology
Paediatrics
Family Medicine
Internal Medicine
Surgery
Orthopaedics
Ophthalmology
This has had a very positive result in terms of medical officer and specialist interaction,
clinical governance and patient-centred experience. Significantly fewer patients have to
travel to George from outlying areas to attend the specialist clinics.
Governance
The overall management of District Health Services in the Central Karoo District is done by
the District Manager. The District Manager reports to the Chief Director: Rural District Health
Services.
Overall clinical governance of the district is led by the general specialist of George Regional
Hospital. At sub-district level, depending on resources available, clinical governance is led
by the clinical manager or the medical manager.
A functional mechanism whereby all the provincial health services role-players meet on a
quarterly basis to plan, implement integrated care, and inter alia, review clinical
governance aspects, is also in place. These role-players, members of the Geographic
Service Area (GSA), come from George Hospital, Eden District and the Central Karoo District
and include representatives from Emergency Medical Services (EMS).
Nelspoort Hospital is classified as an intermediate care facility. It has TB and psychiatric
beds.
For a complete list of health facilities in the district, refer to Annexure C (page 72).
237.2 HUMAN RESOURCES FOR HEALTH (FILLED POSTS)
Table 7: Filled posts as at 31 March 2017
Physiotherapist
Enrolled nurse
Occupational
health worker
Professional
Community
Audiologist
Pharmacist
Sub-district
therapist
therapist
assistant
Speech
Nursing
Doctor
Dentist
Admin
nurse
Beaufort West 1642 49 41 25 73 83 144 45 1 1 0 0
Laingsburg 206 10 4 5 10 27 18 0 0 0 0 0
Prince Albert 219 17 9 2 11 210 311 0 0 0 0 0
Central Karoo 205 77 54 32 94 12 18 4 1 1 0 0
[Source: PERSAL]
2 Include all administrative posts, including staff working in the workshop (artisans, handyman, grounds
men, etc.)
3 Includes 3 Community Service Doctors
4 Includes 1 Community Service Pharmacist and 10 pharmacy assistants
5 Includes 1 Dentist (5/8 post) and 2 Dental Assistants
6 Includes 1 Handyman
7 Includes 1 Community Service Doctor
8 Post Basic Pharmacy Assistant
9 Includes 2 Handymen
10 Includes 1 Community Service Doctor
11 Includes 1 Post Basic Pharmacy Assistant
247.3 BASELINE DATA 2016/17
Table 9: Performance indicators for District Health Services
District wide Province wide
Programme performance indicator Data source / Type Beaufort West Laingsburg Prince Albert
Frequency value value
Element ID
2016/17 2016/17 2016/17 2016/17 2016/17
SECTOR SPECIFIC INDICATORS
1. Ideal clinic (IC) status rate Annual % 33.3% 16.7% 100.0% 50.0% 17.2%
Numerator 3 3 1 1 1 47
Denominator 2 9 6 1 2 273
2. PHC utilisation rate (annualised) Quarterly No 2.7 2.8 2.5 2.3 2.3
Numerator 6 199 941 143 590 22 611 33 740 14 413 350
Denominator 7 75 338 51 904 9 043 14 391 6 318 281
3. Complaint resolution within 25 working Quarterly % 84.0% 80.0% 100.0% 80.0% 95.6%
days rate (PHC facilities)
Numerator 10 21 8 5 8 3 175
Denominator 8 25 10 5 10 3 320
25Table 10: Performance indicators for District Hospitals
District wide Province wide
Programme performance indicator Data source / Type Beaufort West Laingsburg Prince Albert
Frequency value value
Element ID
2016/17 2016/17 2016/17 2016/17 2016/17
SECTOR SPECIFIC INDICATORS
1. Hospital achieved 75% and more on Quarterly % 0.0% 0.0% 0.0% 0.0% 69.7%
National Core Standards (NCS) self-
assessment rate (district hospitals)
Numerator 3 0 0 0 0 23
Denominator 4 3 1 1 1 33
2. Average length of stay (district hospitals) Quarterly Days 2.8 2.8 3.5 2.6 3.2
Numerator 7 30 548 19 516 5 396 5 636 909 893
Denominator 8 10 747 7 071 1 546 2 130 280 580
3. Inpatient bed utilisation rate (district Quarterly % 69.7% 75.3% 73.9% 53.2% 84.8%
hospitals)
Numerator 7 30 548 19 516 5 396 5 636 909 893
Denominator 9 43 805 25 918 7 301 10 586 1 072 731
4. Expenditure per PDE (district hospitals) Quarterly R R 2 273 R 2 423 R 1 938 R 1 981 R 2 139
Numerator 10 97 287 724 70 171 591 12 916 458 14 199 675 2 923 677 427
Denominator 16 42 799 28 964 6 665 7 169 1 366 831
5. Complaint resolution within 25 working Quarterly % 79.7% 71.1% 90.0% 100.0% 90.4%
days rate (district hospitals)
Numerator 19 47 27 9 11 1 501
Denominator 17 59 38 10 11 1 661
26Table 11: Performance indicators for HIV and AIDS, STIs and TB control (HAST)
District wide Province wide
Programme performance indicator Data source / Type Beaufort West Laingsburg Prince Albert
Frequency value value
Element ID
2016/17 2016/17 2016/17 2016/17 2016/17
STRATEGIC GOAL: Promote health and wellness.
1.1.1 TB programme success rate Quarterly % 78.2% 75.9% 80.0% 85.7% 80.4%
Numerator 1 467 315 56 96 34 651
Denominator 2 597 415 70 112 43 099
2.1.1 ART retention in care after 12 months Quarterly % 61.2% 58.4% 71.4% 64.4% 72.2%
Numerator 3 229 143 30 56 33 307
Denominator 4 374 245 42 87 46 120
2.1.2 ART retention in care after 48 months Quarterly % 52.1% 50.3% 50.0% 61.1% 60.7%
Numerator 5 113 79 12 22 19 700
Denominator 6 217 157 24 36 32 455
SECTOR SPECIFIC INDICATORS
1. ART client remain on ART end of month - Quarterly No 1 631 1 153 184 294 230 931
total
Element 7
2. TB/HIV co-infected client on ART rate Quarterly % 67.0% 61.4% 89.5% 83.3% 89.6%
Numerator 8 126 89 17 20 14 902
Denominator 9 188 145 19 24 16 637
3. HIV test done – total Quarterly No 31 892 26 461 2 377 3 054 1 379 375
Element 10
4. Male condoms distributed Quarterly No 2 355 590 1 763 790 229 800 362 000 113 913 868
Element 12
5. Medical male circumcision – total Quarterly No 214 178 15 21 11 687
Element 16
6. TB client 5 years and older start on Quarterly % 96.6% 96.0% 86.8% 104.6% 92.9%
treatment rate
Numerator 19 367 266 33 68 21 007
Denominator 20 380 277 38 65 22 612
27District wide Province wide
Programme performance indicator Data source / Type Beaufort West Laingsburg Prince Albert
Frequency value value
Element ID
2016/17 2016/17 2016/17 2016/17 2016/17
7. TB client treatment success rate Quarterly % 78.2% 75.9% 80.0% 85.7% 80.4%
Numerator 21 467 315 56 96 34 651
Denominator 22 597 415 70 112 43 099
8. TB client defaulter / lost to follow up rate Quarterly % 15.4% 18.8% 5.7% 8.9% 10.5%
Numerator 23 92 78 4 10 4 514
Denominator 22 597 415 70 112 43 099
9. TB client death rate Annual % 3.7% 2.7% 10.0% 3.6% 3.9%
Numerator 24 22 11 7 4 1 693
Denominator 22 597 415 70 112 43 099
10. TB MDR treatment success rate Annual % 64.3% 65.2% 100.0% 50.0% 44.6%
Numerator 25 18 15 1 2 738
Denominator 26 28 23 1 4 1 653
28Table 12: Performance indicators for MCWH and Nutrition
District wide Province wide
Programme performance indicator Data source / Type Beaufort West Laingsburg Prince Albert
Frequency value value
Element ID
2016/17 2016/17 2016/17 2016/17 2016/17
SECTOR SPECIFIC INDICATORS
1. Antenatal 1st visit before 20 weeks rate Quarterly % 73.3% 71.2% 82.3% 76.3% 69.6%
Numerator 1 891 605 102 184 63 901
Denominator 2 1 215 850 124 241 91 849
2. Mother postnatal visit within 6 days rate Quarterly % 47.1% 39.5% 69.8% 79.4% 60.0%
Numerator 3 447 295 67 85 54 816
Denominator 4 949 746 96 107 91 322
3. Antenatal client start on ART rate Annual % 35.4% 23.5% 50.0% 83.3% 90.8%
Numerator 5 23 12 1 10 7 009
Denominator 6 65 51 2 12 7 715
4. Infant 1st PCR test positive around 10 weeks Quarterly % 1.4% 1.8% 0.0% 0.0% 0.8%
rate
Numerator 7 1 1 0 0 95
Denominator 8 70 57 7 6 12 013
5. Immunisation coverage under 1 year Quarterly % 67.7% 64.1% 74.3% 80.0% 75.1%
Numerator 9 899 623 106 170 78 933
Denominator 10 1 327 971 143 213 105 108
6. Measles 2nd dose coverage Quarterly % 80.4% 74.0% 104.7% 93.4% 86.3%
Numerator 11 1 122 756 157 209 92 898
Denominator 12 1 396 1 022 150 224 107 596
7. Diarrhoea case fatality rate Quarterly % 0.0% 0.0% 0.0% 0.0% 0.2%
Numerator 16 0 0 0 0 17
Denominator 17 162 95 26 41 6 992
8. Pneumonia case fatality rate Quarterly % 0.0% 0.0% 0.0% 0.0% 0.4%
Numerator 18 0 0 0 0 29
Denominator 19 52 22 4 26 7 943
9. Severe acute malnutrition case fatality rate Quarterly % 0.0% 0.0% 0.0% 0.6%
Numerator 20 0 0 0 0 5
Denominator 21 29 12 0 17 841
29District wide Province wide
Programme performance indicator Data source / Type Beaufort West Laingsburg Prince Albert
Frequency value value
Element ID
2016/17 2016/17 2016/17 2016/17 2016/17
10. School Grade 1 - learners screened Quarterly No 978 823 12 143 55 171
Element 22
11. School Grade 8 - learners screened Quarterly No 0 0 0 0 9 364
Element 24
12. Delivery in 10 to 19 years in facility rate Quarterly % Not required to Not required to Not required to Not required to Not required to
report report report report report
Numerator 26 - - - - -
Denominator 4 949 746 96 107 91 322
13. Couple year protection rate (Int) Quarterly % 116.0% 127.1% 95.7% 89.1% 78.8%
Numerator 27 24 113 18 144 2 381 3 588 1 386 357
Denominator 28 20 793 14 276 2 489 4 028 1 760 154
14. Cervical cancer screening coverage 30 Quarterly % 75.7% 4251.5% 3147.6% 2321.8% 55.7%
years and older
Numerator 29 1 304 49 995 7 300 7 320 90 454
Denominator 30 1 723 1 176 232 315 162 460
15. HPV 1st dose Annual No 601 420 51 130 36 182
Element 31
16. HPV 2nd dose Annual No 593 413 51 129 34 941
Element 33
17. Vitamin A 12 - 59 months coverage Quarterly % 48.2% 44.1% 48.0% 67.2% 48.8%
Numerator 34 5 580 3 738 597 1 245 425 757
Denominator 35 11 572 8 474 1 245 1 854 872 332
18. Maternal mortality in facility ratio Annual No per 0 0 0 0 57
100 000
Numerator 37 0 0 0 0 54
Denominator / 100 000 40 0.010 0.008 0.001 0.001 0.954
19. Neonatal death in facility rate Annual No per 1 000 14 10 43 19 9
Numerator 43 13 7 4 2 783
Denominator / 1 000 38 0.931 0.734 0.092 0.105 91.798
30Table 13: Performance Indicators for District Health Services
District wide Province wide
Programme performance indicator Data source / Type Beaufort West Laingsburg Prince Albert
Frequency value value
Element ID
2016/17 2016/17 2016/17 2016/17 2016/17
SECTOR SPECIFIC INDICATORS
1. Cataract surgery rate (in uninsured Quarterly No per million 1 709 2 451 0 0 1 692
population)
Numerator 1 93 93 0 0 8 050
Denominator / 1 000 000 2 0.054 0.038 0.006 0.010 4.759
2. Malaria case fatality rate Quarterly % 0.7%
Numerator 3 0 0 0 0 1
Denominator 4 0 0 0 0 139
318. QUALITY OF CARE
Table 14: Top 20 worst performing Ideal Clinic elements in PHC facilities 2017/18 YTD
Nr Worst performing elements
1. Patient record content adheres to ICSM prescripts
2. Adolescent and youth friendly services are provided
3. Staffing needs have been determined in line with WISN
4. Staffing is in line with WISN
5. The facility has a dedicated budget
6. Disinfectant, cleaning materials and equipment are available
7. There is a standard security guard room OR the facility has an alarm system linked to armed
response
8. Building is compliant with safety regulations
9. There is a functional clinic committee
10. Contact details of clinic committee members are visibly displayed
11. There is an official memorandum of understanding between the district management and
Cooperative Governance and Traditional Affairs (CoGTA)
12. All external signage in place
13. The National Referral Policy is available
14. There is an official memorandum of understanding between the PDOH and the Department of
Social Development
15. The National Clinical Audit guideline is available
16. Clinic space accommodates all services and staff
17. Ante-natal patient initiated on ART rate is at least 96% or has increased by at least 5% from the
previous year
18. Facility refers environmental health related risks to environmental health services
19. All staff has received in-service training on infection control standard precautions that is in-line
with the Standard Operating Procedure in the last two years.
20. Annual awareness day on hand hygiene is held
[Source: Ideal Clinic Quality Improvement Plan 2017/18]
Table 15: Top 20 worst performing National Core Standards in district hospitals 2017/18 YTD
Nr Worst performing elements
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
32Nr Worst performing elements
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
[Source: WebDHIS National Core Standards]
Table 16: Top 5 challenges reported by patients in patient surveys and patient complaints
2017/18 YTD
Nr Challenges reported in patient surveys Patient complaints (category)
1. The hospital did not assist me to get a lift home Waiting times
2. I had to wait a long time to get my folder Staff Attitudes
3. It takes longer than 30 minutes to get to the hospital Care and Professional Treatment
4. It costs more than R20 to get to the hospital Other
5. I was very bored at the hospital Safety and Security
[Source: Sinjani]
339. ORGANISATIONAL STRUCTURE OF THE DISTRICT MANAGEMENT TEAM
Figure 9: Organogram for Central Karoo as at 31 March 2017
3410. DISTRICT HEALTH EXPENDITURE
Table 17: Summary of district health expenditure 2016/17
TOTAL
Budget: Adjusted
Sub-programme Expenditure % Overspent
Appropriation Budget Expenditures
(Underspent)
2.1 District Management R 7 914 000.00 R 8 126 524.09 R 7 914 000.00 R 8 126 524.09 6.51%
2.2 Clinics R 45 451 000.00 R 46 036 550.81 R 45 451 000.00 R 46 036 550.81 7.48%
Community Health
2.3 R 2 164 000.00 R 2 061 317.85 R 2 164 000.00 R 2 061 317.85 20.94%
Centres
Community Services
2.4 R 19 708 000.00 R 19 152 748.99 R 19 708 000.00 R 19 152 748.99 1.59%
(incl. PAH)
Other Community
2.5
Services
7.33%
2.6 HIV/AIDS R 30 520 000.00 R 29 026 155.42 R 30 520 000.00 R 29 026 155.42
2.7 Nutrition R 2 767 000.00 R 2 397 348.21 R 2 767 000.00 R 2 397 348.21 -1.27%
2.9 District Hospitals R 92 978 000.00 R 97 287 723.58 R 92 978 000.00 R 97 287 723.58 6.54%
2.12 Other Donor Funding
TOTAL DISTRICT R 201 502 000.00 R 204 088 368.95 R 201 502 000.00 R 204 088 368.95 6.45%
[Source: District Health Expenditure Review (2016/17) or BAS]
3511. DISTRICT PERFORMANCE INDICATORS
The service delivery component is the core business of District Health Services. It covers the
delivery of the full district health package of services, the management and supervision of
these services, how well the service performs in terms of health outcomes, and quality
assurance.
The District has six main focus areas in the context of service delivery:
Primary health care (PHC) services.
Home community based care.
Acute services in the district hospitals especially with regard to the functioning of the
emergency centres.
Infectious diseases (especially HIV, AIDS, tuberculosis (TB) and sexually transmitted
infections (STIs)).
Women’s health and child health.
Improving the experience of patients at health facilities (which is fundamental in the
process).
The following are priorities in terms of actions to address the service delivery challenges:
Addressing the burden of disease by managing patients in an integrated way on all
platforms of care, e.g. community-based, primary health care and district hospitals.
Particular emphasis on the management of chronic diseases. This includes
implementation of the Practical Approach to Care Kit (PACK) programme, an
algorithm-based diagnosis and medication methodology of managing chronic
diseases.
Optimal financial management to maximise health outcomes.
Ensure equity in distribution of all new posts.
Maximise recruitment and retention activities to keep personnel with scarce skills.
Maximise opportunities to improve the capital infrastructure of facilities.
Ensure all vacant posts are filled as soon as possible.
Ensure emergency centres are capacitated to be fully functional.
Consolidate outreach and support services from George Regional Hospital.
Integration of the anti-retroviral treatment (ART) programme into the mainstream
chronic disease management programme.
Ensuring full implementation of the basic antenatal care (BANC) protocols.
On-going training for staff working in labour wards.
Maintain improved coverage of fertility planning services.
Focus on immunisation of children to ensure adequate coverage.
Improving the experience of clients utilising health services.
3611.1 DISTRICT HEALTH SERVICES
Table 18: Performance indicators for District Health Services
Provincial
Data Estimated
Programme performance indicator Type Audited / Actual performance Medium term targets actual
Frequency source / performance
performance
Element ID
2014/15 2015/16 2016/17 2017/18 2018/19 2019/20 2020/21 2016/17
SECTOR SPECIFIC INDICATORS
1. Ideal clinic (IC) status rate Annual % 0.0% 0.0% 33.3% 77.8% 88.9% 100.0% 100.0% 17.2%
Numerator 3 0 0 3 7 8 9 9 47
Denominator 2 9 9 9 9 9 9 9 273
2. PHC utilisation rate (annualised) Quarterly No 2.6 2.6 2.7 2.7 2.7 2.7 2.7 2.3
Numerator 6 191 490 190 933 199 941 205 337 207 363 209 431 211 527 14 413 350
Denominator 7 73 981 74 660 75 338 76 061 76 828 77 610 78 402 6 318 281
3. Complaint resolution within 25 Quarterly % 95.7% 81.8% 84.0% 84.8% 86.7% 92.6% 96.0% 95.6%
working days rate (PHC
facilities)
Numerator 10 22 18 21 28 26 25 24 3 175
Denominator 8 23 22 25 33 30 27 25 3 320
37Table 19: Quarterly targets for District Health Services
Programme performance indicator Data source Frequency Annual target Quarterly targets
/ Element ID 2018/19 Quarter 1 Quarter 2 Quarter 3 Quarter 4
SECTOR SPECIFIC INDICATORS
1. Ideal clinic (IC) status rate Annual 88.9% - - - 88.9%
Numerator 3 8 - - - 8
Denominator 2 9 - - - 9
2. PHC utilisation rate (annualised) Quarterly 2.7 2.7 2.7 2.6 2.8
Numerator 6 207 363 51 263 52 740 49 292 54 068
Denominator 7 76 828 19 207 19 207 19 207 19 207
3. Complaint resolution within 25 working days rate Quarterly 86.7% 85.7% 87.5% 85.7% 87.5%
(PHC facilities)
Numerator 10 26 6 7 6 7
Denominator 8 30 7 8 7 8
Aspects to take into consideration for the Central Karoo include:
The PHC programme is managed centrally from Beaufort West.
Strategic challenges:
Equity in distribution of any new posts established.
Recruitment and retention of professionals with scarce skills.
Achieve Ideal Clinic Status:
Four out of the four (4) identified facilities achieved Ideal Clinic status during 2017/18. Three facilities obtained Ideal Clinic status during
2016/17 and all three facilities maintained their Ideal Clinic status in 2017/18. The two remaining facilities, Kwa Mandlenkosi and Murraysburg
Clinics will be targeted to obtain Ideal Clinic Status in 2018/19.
Key Interventions to achieve Ideal Clinic status includes:
o Operational Managers to complete status determination early in first quarter, or as soon as the template is finalized and available.
o PPTICRM team must complete first audit in July 2018.
o If necessary, the PPTICRM audit team must repeat the PPTICRM review at any Ideal Clinic facilities that does not achieve ideal clinic
status during the first PPTICRM audit. The PPTICRM team and PHC manager must render continuous support to all facilities.
38o PPTICRM team must do at least 2 audit reviews at Kwa Mandlenkosi and Murraysburg Clinics in preparation for peer review audits during
the third quarter.
o Dedicated and specific attention and support for the operational managers at Kwa Mandlenkosi and Murraysburg Clinics.
3911.2 DISTRICT HOSPITALS
Table 20: Performance indicators for District Hospitals
Provincial
Data Estimated
Programme performance indicator Type Audited / Actual performance Medium term targets actual
Frequency source / performance
performance
Element ID
2014/15 2015/16 2016/17 2017/18 2018/19 2019/20 2020/21 2016/17
SECTOR SPECIFIC INDICATORS
1. Hospital achieved 75% and more Quarterly % 0.0% 0.0% 0.0% 25.0% 25.0% 75.0% 100.0% 69.7%
on National Core Standards
(NCS) self-assessment rate
(district hospitals)
Numerator 3 0 0 0 1 1 3 4 23
Denominator 4 3 4 3 4 4 4 4 33
2. Average length of stay (district Quarterly Days 2.9 3.3 2.8 2.8 2.8 2.8 2.8 3.2
hospitals)
Numerator 7 30 905 32 227 30 548 30 395 30 716 31 042 31 373 909 893
Denominator 8 10 507 9 824 10 747 10 769 10 879 10 992 11 107 280 580
3. Inpatient bed utilisation rate Quarterly % 70.6% 73.6% 69.7% 69.4% 70.1% 70.9% 71.6% 84.8%
(district hospitals)
Numerator 7 30 905 32 227 30 548 30 395 30 716 31 042 31 373 909 893
Denominator 9 43 805 43 805 43 805 43 805 43 805 43 805 43 805 1 072 731
4. Expenditure per PDE (district Quarterly R R 1 814 R 2 007 R 2 273 R 2 532 R 2 616 R 2 711 R 2 840 R 2 139
hospitals)
Numerator 10 81 724 110 90 921 997 97 287 724 108 279 000 113 015 000 118 361 000 125 250 000 2 923 677 427
Denominator 16 45 043 45 312 42 799 42 770 43 207 43 652 44 104 1 366 831
5. Complaint resolution within 25 Quarterly % 57.1% 77.8% 79.7% 81.3% 83.7% 85.7% 89.8% 90.4%
working days rate (district
hospitals)
Numerator 19 16 42 47 39 41 42 44 1 501
Denominator 17 28 54 59 48 49 49 49 1 661
40Table 21: Quarterly targets for District Hospitals
Programme performance indicator Data source Frequency Annual target Quarterly targets
/ Element ID 2018/19 Quarter 1 Quarter 2 Quarter 3 Quarter 4
SECTOR SPECIFIC INDICATORS
1. Hospital achieved 75% and more on National Quarterly 25.0% - - - 25.0%
Core Standards (NCS) self-assessment rate (district
hospitals)
Numerator 3 1 - - - 1
Denominator 4 4 - - - 4
2. Average length of stay (district hospitals) Quarterly 2.8 3.0 2.8 2.8 2.7
Numerator 7 30 716 7 980 7 639 7 600 7 497
Denominator 8 10 879 2 655 2 725 2 728 2 771
3. Inpatient bed utilisation rate (district hospitals) Quarterly 70.1% 72.9% 69.8% 69.4% 68.5%
Numerator 7 30 716 7 980 7 639 7 600 7 497
Denominator 9 43 805 10 951 10 951 10 951 10 952
4. Expenditure per PDE (district hospitals) Quarterly R 2 616 R 2 375 R 2 722 R 2 602 R 2 770
Numerator 10 113 015 000 26 111 805 29 104 876 28 033 101 29 765 218
Denominator 16 43 207 10 996 10 693 10 772 10 746
5. Complaint resolution within 25 working days rate Quarterly 83.7% 84.6% 83.3% 83.3% 83.3%
(district hospitals)
Numerator 19 41 11 10 10 10
Denominator 17 49 13 12 12 12
Infection control
Improve/implement infection control principles at district hospitals:
o Wearing of masks.
o Open windows.
o Hand washing with anti-bacterial soap and promoting hand washing practices amongst staff through on-going training and annual
hand washing campaigns.
Annual TB screening of all health care workers.
41Mental Health Services
Improve mental health information systems by increasing the percentage of mental health patients who are discharged from the emergency
centre and the hospital with an ICD-10 code.
Hospital achieved 75% and more on National Core Standards (NCS) self-assessment rate (district hospitals)
All district hospitals to do a self-assessment during the third quarter of 2018/19.
Set up a district team to conduct NCS assessments at all district hospitals during the third quarter of 2018/19.
Ensure all staff understands the criteria for national core standards (NCS).
Learn from gaps identified during mock assessments conducted by the Office of Health Standards Compliance.
Monitor progress and maintain extreme and vital measures within the NCS via monthly supervisory visit tool.
All district hospitals must write and submit a QIP after the NCS assessment was conducted. The report must be submitted before the end of
the third quarter.
Progress on the QIP must be monitored and discussed at management meetings.
Complaint resolution rate
Re-visit system to ensure that all complaints are documented.
Make sure all sub-districts are using the standardised SOP (Circular H64/2015).
Discuss complaints and compliments on the monthly nursing managers’ forum.
Average length of stay:
Improve on ICD-10 coding.
Conduct triage/waiting time audits twice a year at Beaufort West Hospital and once a year at the other district hospitals.
Reduce waiting times at all facilities - implement/improve appointment system.
Mortality and morbidity reviews:
Monthly morbidity and mortality (M & M) meetings. Each district hospital must identify a person who will take responsibility for this e.g. a
medical officer or the nursing manager.
Follow up areas of concern or any trends identified during M & M discussions.
Discuss M & M findings at quarterly extended management meetings.
Feedback to all staff to improve on previous challenges and skills.
4211.3 HIV AND AIDS, STIs AND TB CONTROL (HAST)
Table 22: Performance indicators for HIV and AIDS, STIs and TB control (HAST)
Provincial
Data Estimated
Programme performance indicator Type Audited / Actual performance Medium term targets actual
Frequency source / performance
performance
Element ID
2014/15 2015/16 2016/17 2017/18 2018/19 2019/20 2020/21 2016/17
STRATEGIC GOAL: Promote health and wellness.
1.1.1 TB programme success rate Quarterly % 79.2% 79.3% 78.2% 76.5% 83.5% 83.5% 83.6% 80.4%
Numerator 1 462 490 467 455 500 502 503 34 651
Denominator 2 583 618 597 595 599 601 602 43 099
2.1.1 ART retention in care after 12 Quarterly % 67.9% 57.2% 61.2% 59.5% 59.6% 59.8% 59.9% 72.2%
months
Numerator 3 184 186 229 223 226 229 232 33 307
Denominator 4 271 325 374 375 379 383 387 46 120
2.1.2 ART retention in care after 48 Quarterly % 60.6% 51.3% 52.1% 53.7% 53.1% 52.6% 52.0% 60.7%
months
Numerator 5 94 99 113 102 102 102 102 19 700
Denominator 6 155 193 217 190 192 194 196 32 455
SECTOR SPECIFIC INDICATORS
1. ART client remain on ART end of Quarterly No 1 418 1 416 1 631 1 710 1 970 1 990 2 010 230 931
month - total
Element 7
2. TB/HIV co-infected client on ART Quarterly % 66.7% 67.0% 67.0% 75.4% 75.5% 75.7% 75.8% 89.6%
rate
Numerator 8 118 126 126 141 142 143 144 14 902
Denominator 9 177 188 188 187 188 189 190 16 637
3. HIV test done – total Quarterly No 17 646 27 543 31 892 35 786 36 098 36 417 36 742 1 379 375
Element 10
4. Male condoms distributed Quarterly No 1 526 194 1 904 270 2 355 590 2 304 200 2 347 418 2 392 075 2 437 864 113 913 868
Element 12
5. Medical male circumcision – Quarterly No 518 117 214 250 252 254 256 11 687
total
Element 16
43You can also read