Cancer control in Africa: paving the way for Universal Health Coverage - INTERNATIONAL CANCER CONTROL
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Cancer control in Africa:
paving the way for
Universal Health Coverage
IN T E R N AT I O N A L
CANCER CONTROL
PARTNERSHIP
Breast cancer in the African region 32
Table of Contents Nazik Hammad, Queen's University, Canada
Verna Vanderpuye, Consultant Oncologist, AORTIC Secretary Treasurer, Ghana
Beatrice Wiafe Addai, Peace and Love Hospital and Breast Care International, Ghana
Miriam Mutebi, Aga Khan University Hospital, Kenya
Naomi Ohene Oti, National Radiotherapy, Oncology and Nuclear Medicine Centre, Korle Bu Teaching Hospital, Ghana
Foreword AORTIC President 4 Childhood cancer in Africa 34
Foreword UICC President 5 Cristina Stefan, African Organisation for Research and Training in Cancer, South Africa
Fidel Rubagumya, Rwanda Military Hospital &University of Global Health Equity & Rwanda Children’s Cancer Relief, Rwanda
Acknowledgements 6 Biobele J. Brown, Haematology & Oncology Unit, Department of Paediatrics, College of Medicine University of Ibadan /
University College Hospital Ibadan, Nigeria
Abbreviations 6
Prostate cancer 36
Introduction 7 Timothy R. Rebbeck, Dana Farber Cancer Institute and Harvard TH Chan School of Public Health, US
Sonali Johnson, Union for International Cancer Control, Switzerland
Cristina Stefan, African Organisation for Research and Training in Cancer, South Africa Cervical cancer elimination 38
Julie Torode, Union for International Cancer Control, Switzerland
The cancer burden in the African Region 9 Verna Vanderpuye, Consultant Oncologist, AORTIC Secretary Treasurer, Ghana
D. Maxwell Parkin, African Cancer Registry Network & University of Oxford, UK Alex Mutombo, Gynaecologic Oncologist, Kinshasa University Hospital, Democratic Republic of the Congo
Cesaltina Lorenzoni, Ministry of Health, Mozambique & Hospital Central do Maputo, Universidade Eduardo Mondlane, Mozambique
The status of national cancer control plans in the African region 14 Lucy Muchiri, Department of Human Pathology, College of Health Sciences, University of Nairobi, Kenya
Dario Trapani, Department of Oncology and Haematology, University of Milan, Italy
Sonali Johnson, Union for International Cancer Control, Switzerland
Rosie Tasker, Union for International Cancer Control, Switzerland
Verna Vanderpuye, Consultant Oncologist, AORTIC Secretary Treasurer, Ghana
Moving forwards through partnerships 42
Zuzanna Tittenbrun, Union for International Cancer Control, Switzerland
Yannick Romero, Union for International Cancer Control, Switzerland
Women in global oncology forum: expanding the oncology workforce 42
Miriam Mutebi, Aga Khan University Hospital, Kenya
Cancer control spotlights 17 Supporting AORTIC’s young generation 44
Fidel Rubagumya, Rwanda Military Hospital &University of Global Health Equity & Rwanda Children’s Cancer Relief, Rwanda
Cristina Stefan, African Organisation for Research and Training in Cancer, South Africa
Policy and legislation for the prevention and control of NCDs in Africa 17 Kwanele Asante, University of Witwatersrand, South Africa
David Makumi, Kenya Network of Cancer Organizations, Kenya
Preethi Mistri, Cancer Association of South Africa, South Africa African Cancer Registry Network: Accomplishments, activities and plans for the future 45
D. Maxwell Parkin, African Organisation for Research and Training in Cancer & University of Oxford, UK
FCTC implementation in the African region 19 J. Olufemi Ogunbiyi, University of Ibadan/ University College Hospital, Nigeria
Tih Ntiabang, Framework Convention Alliance, Cameroon Eric Chokunonga, Zimbabwe National Cancer Registry, Zimbabwe
Biying Liu, African Organisation for Research and Training in Cancer, UK
Early detection 21
Ophira Ginsburg, Department of Population Health, New York University School of Medicine, US Capacity Building for Civil Society in the African Region: 47
Ashley Newcomb, Department of Population Health, New York University School of Medicine, US Key UICC Programmes and Opportunities
Mélanie Samson, Union for International Cancer Control, Switzerland
Pathology in Africa 24 Kirstie Graham, Union for International Cancer Control, Switzerland
J. Olufemi Ogunbiyi, University of Ibadan/ University College Hospital, Nigeria
Sally Donaldson, Union for International Cancer Control, Switzerland
Cesaltina Lorenzoni, Ministry of Health, Mozambique & Maputo Central Hospital,
Alessandro Di Capua, Union for International Cancer Control, Switzerland
Universidade Eduardo Mondlane, Mozambique
Domenico Iaia, Union for International Cancer Control, Switzerland
WHO Model List of Essential Medicines and access to medicines across 26 Sabrina Zucchello, Union for International Cancer Control, Switzerland
the African region The Africa Cancer Research and Control ECHO: Utilising technology-enabled 51
Shalini Jayasekar Zürn, Union for International Cancer Control, Switzerland
collaborative learning to advance national cancer control plan implementation
Yehoda M. Martei, Hematology-Oncology Division, University of Pennsylvania, US
Kalina Duncan, Center for Global Health, U.S. National Cancer Institute, US
Radiotherapy 28 Mishka K. Cira, Clinical Monitoring Research Program Directorate, Frederick National Laboratory for Cancer Research, US
Hannah Simonds, Division of Radiation Oncology, Stellenbosch University, Tygerberg Academic Hospital, South Africa Anne Ng’ang’a, Ministry of Health, Kenya
Wilfred Ngwa, Brigham and Women’s Hospital, Dana-Farber Cancer Institute, Harvard Medical School, US
Civil society organisations and integrating cancer in Universal Health Coverage 53
Surbhi Grover, Department of Radiation Oncology, University of Pennsylvania, US
Rosie Tasker, Union for International Cancer Control, Switzerland
Improving surgical oncology in Africa 29
Miriam Mutebi, Aga Khan University Hospital, Kenya
Recommendations for AORTIC members 55
Palliative care and psycho-oncology in the African region 30
Christian R. Ntizimira, City Cancer Challenge, Rwanda
Chioma C. Asuzu, Psycho-Oncology Unit, Department of Radiation Oncology, College of Medicine, University of Ibadan, Nigeria
References 56
Foreword Foreword
In 2015, I became the first woman from the African The chapters concisely address a diverse selection UICC is honoured to publish this booklet with the The African region has enormous resources at its
continent to be elected President of AORTIC. I felt of topics, including cervical cancer, childhood African Organisation for Research and Training disposal, with a young population and a growing
honoured but also humbled when contemplating cancer, surgery and cancer surveillance and in Cancer (AORTIC) on Cancer control in Africa: and vibrant economy. The region has dynamic
the task ahead, with numerous far-reaching feature important collaborations, projects and paving the way for Universal Health Coverage. and committed scientists, health providers and
changes needed for greater progress in cancer partnerships underway to strengthen cancer The goal of cancer control to reduce the burden advocates, who come together through AORTIC
control in the region. I was determined to do all control in Africa, such as programmes for young of cancer and improve the quality of life of and its conferences to plan a better future for
I could to significantly increase the contribution African leaders and many others. It also contains cancer patients and the general population is cancer patients and to take steps to reduce the
of our organisation to improving cancer care in reflections and proposals meant to reduce cancer complementary to achieving the vision of UHC, incidence of cancer on the continent. As this
Africa and achieve our vision of transforming related morbidity and mortality, to improve where all people have access to quality health booklet will show, there are many steps that can be
cancer control through collaboration in education, prevention, early diagnosis and treatment, with the services without suffering the financial hardship taken from now to reduce the cancer burden that
research and delivery of equitable and timely aim to promote the best care and a better life for all associated with paying for care. The impact of are cost effective and feasible to implement across
interventions to minimise the impact of cancer. people living on the continent. cancer can be catastrophic not just on the physical health systems.
AORTIC has taken a number of steps in the right and emotional health of patients, but also has a
direction to achieve this goal. The publication of The aim of the book is to highlight and share huge financial impact in settings where treatment I greatly thank the International Cancer Control
this first book on cancer control and Universal existing information related to cancer in Africa, and care must be paid for out-of-pocket. This can Partnership (ICCP) for reviewing and contributing
Health Coverage (UHC) in Africa, together with as well as to disseminate plans and measures result in catastrophic health spending, resulting in to this booklet, as well as the experts who
our trusted partners, the Union for International to advance cancer care in the context of UHC. greater impoverishment, inequality and, in many developed the chapters. UICC stands ready to
Cancer Control (UICC) and the International The lesson that emerges is not only that a major cases, treatment abandonment. support national cancer control efforts in Africa
Cancer Control Partnership (ICCP) is another difference can be made in reducing the incidence, and around the world and applauds the efforts
key step in laying the groundwork for evidence- improving the management, and increasing But it need not be so. Proven and effective solutions already underway in many countries in the region
informed advocacy and building partnerships to survivorship for many cancers in Africa, but that exist, from the prevention of cancer and other to integrate cancer control into Universal Health
achieve the objective of improved coverage of cervical cancer, a major threat to women’s health NCDs to the early diagnosis and management of Coverage.
quality cancer services from prevention through to on the continent, can be eliminated. These actions cancer, including pain relief and palliative care. As
palliative care. The election of Dr Tedros Adhanom can be done in cost-effective and affordable ways. an advocate who has worked in cancer control for
Ghebreyesus, the first African Director General Understanding the many facets of the disease and eighteen years; as former Director General of the
of the World Health Organization, has brought determination in fighting it are the keys to success. King Hussein Cancer Foundation in Jordan and
increased commitment in the region and globally to now as President of UICC, I know only too well
This is a book for all AORTIC members: scientists, of the challenges that cancer patients and their
fundamental changes in the accessibility of health HRH Princess Dina Mired
health care practitioners, patients, survivors, families face daily in accessing the lifesaving care
care and the promotion of health equity under UHC. President,
experts, advocates and government officials, they need. As the mother of a cancer survivor, I
UICC and AORTIC are proud to join this global Union for International Cancer Control
but also for the general public who will be the also know of the incredible advances in cancer
force to achieve the vision of ‘Health for All’.
beneficiary of stronger cancer prevention and care treatment and care that exist and must be available
This remarkable book tells us not only the story of and whose place of birth will no longer impact to all those who need it, regardless of geography or
the considerable progress made during the last few negatively on their future. ability to pay.
years in battling cancer on the continent, but also
It is a book about current challenges, but with a
the challenges that remain and areas for action.
strong invitation to action.
Written by and for African leaders, health care
specialists, advocates, survivors and many others
working on cancer control, the book critically
analyses the present cancer environment on the
continent, while also looking towards the future in
the context of UHC.
Cristina Stefan
President,
African Organisation for Research
and Training in Cancer
4 Cancer control in Africa: paving the way for Universal Health Coverage Cancer control in Africa: paving the way for Universal Health Coverage 5
Introduction
Acknowledgements Abbreviations
This publication has been coordinated by AFCRN – The African Cancer Registry Universal Health Coverage (UHC) is a concept Cancer is one of the most compelling examples
an editorial group composed of the UICC Network that has been talked about for decades. The of inequity in health outcomes, with survival rates
Knowledge, Advocacy and Policy team: AFRO – WHO Regional Office for Africa concept of ‘Health for All’ is reflected in WHO’s and cancer mortality varying greatly between
Sonali Johnson, Zuzanna Tittenbrun, constitution and was the key driver in the 1978 and within countries particularly for cancers that
Rosie Tasker and Yannick Romero and the AORTIC – African Organisation for
Alma-Ata declaration on primary health care (PHC). are amenable to prevention and early diagnosis.
Research and Training in Cancer
AORTIC Council represented by AORTIC Achieving ‘Health for All’ is a goal of the World These inequities are not just due to the variation in
President Cristina Stefan. CSO – Civil Society Organisation Health Organization and its member states and the occurrence of cancer risk factors and cancer
EML – The WHO Model list of implies the attainment by all the people of the world epidemiology but also inequalities in access to
The editorial group would like to thank
Essential Medicines of a level of health that would permit them to lead prevention, treatment and care interventions.
the experts and organisations who
a socially and economically productive life. (1) It Given the increasing burden of cancer in Africa,
reviewed and provided comments to the FCTC – The WHO Framework
Convention on Tobacco Control depends on continued progress in medical care accounting for an estimated 1,055,172 new cases
draft versions of this booklet:
and public health to the benefit of all populations, in 2018, (2) cancer must be included in the national
HIC – High-income country but also the removal of obstacles in accessing UHC package in all countries in the region.
ABC Foundation, Ben Anderson, Jean-
Marc Bourque, Nina Caleffi, Cancer IARC – The International Agency quality health services and the development of
for Research on Cancer policies and programmes that promote health. Despite high cure rates for childhood cancer
Association of South Africa (CANSA),
in high-income countries, reaching 80% and
Alison Cox, Alessandro Di Capua, Sally ICCP – International Cancer Control Indeed, inequalities in access to health care and higher for some cancers, survival rates in African
Donaldson, Jacqui Drope, Jeff Dunn, Partnership differential health outcomes globally have defined countries are frequently as low as 20%. (3) While
Allison Dvaladze, Leslie Given, Kirstie
LIC – Low-income country the health agenda in the late 20th and early 21st cervical cancer remains a rare cause of death
Graham, Karin Hohman, Domenico
LMIC – Lower middle-income country centuries. Inequalities in health status reflect, to a among women in Europe and North America, 90%
Iaia, André Ilbawi, International Cancer
large extent, the socio-economic disparities that of cervical cancer deaths globally per year occur in
Control Partnership (ICCP), Shalini NCCP – National Cancer Control Plan exist between low- and high-income countries, low- and middle-income countries, with the highest
Jayasekar Zürn, Rosemary Kennedy,
NCDs – Non-communicable diseases but also those inequalities that are prevalent burden borne by sub-Saharan African countries.
Kenya Network of Cancer Organizations
between or among different socioeconomic, Such stark inequalities in outcomes for preventable
(KENCO), Dan Milner, NCD Alliance NEML – National list of Essential Medicines
ethnic, racial and cultural groups within countries. and treatable cancers are unjust and immoral,
of Kenya, Micaela Neumann, Marta PBCR – Population-based cancer registry The Millennium Development Goals (MDGs) contradicting the right to health as enshrined in
Pazos, Katherine Pettus, Marion Piñeros,
SDGs – Sustainable Development Goals targeted eight key areas with strong inequalities international human rights law.
Belmira Rodrigues, Mélanie Samson,
not only in terms of outcomes, but also in relation
Sinéad Troy, Sabrina Zucchello SSA – Sub-Saharan Africa The recently adopted Political Declaration on
to the availability of and access to services. While
UHC – Universal Health Coverage progress has been made on many of the indicators, Universal Health Coverage at the United Nations
including the health-related goals corresponding General Assembly on 23 September 2019, provides
UICC – Union for International Cancer
to reductions in child mortality, maternal mortality strong global consensus on the urgent need for
Control
and HIV infections, the agenda is still unfinished UHC and sustained political momentum. The
UMIC – Upper middle-income country Political Declaration comprehensively outlines the
and is reflected in the MDGs’ successor, the
WHO – World Health Organization Sustainable Development Goals (SDGs). In addition fundamental actions across the health and related
to including communicable conditions, the SDGs sectors that countries can take both as a global
reflect the changing global epidemiological burden community and in national contexts to achieve
of disease, with a separate target to reduce Non- UHC by 2030. The Political Declaration includes
Communicable Diseases by a third by 2030, the need for countries to strengthen efforts to
where currently, 70% of global deaths are due address NCDs, including cardiovascular diseases,
to NCDs. The health goal of the SDGs also has chronic respiratory diseases, diabetes and cancer.
a target related to Universal Health Coverage, Yet beyond political will, implementing and scaling
which includes financial risk protection, access to up UHC will require the planning and coordination
quality essential health care services, and access of many actors including government, civil society
to safe, effective, quality, and affordable essential and the private sector.
medicines and vaccines for all.
6 Cancer control in Africa: paving the way for Universal Health Coverage Cancer control in Africa: paving the way for Universal Health Coverage 7
It is encouraging that African countries are The following publication has been developed to
already actively pursuing plans for UHC. Indeed,
the African Union agreed to the setting of a more
reflect an advocacy and policy perspective on the
status of national cancer control planning efforts in
The cancer burden
ambitious continental target of 2025 to achieve the African region with a view to including cancer
UHC that would galvanise its Member States to
accelerate action.
in UHC plans across the continent. The focus of
each chapter is to place a ‘spotlight’ on the current
in the African Region
status of a specific aspect of cancer control,
Solutions to prevent and manage cancer exist challenges and gaps in each area as well as policy
and are accessible in all resource settings. recommendations for improvement to achieve the
In African countries with varying levels of
resources, the challenge will be to derive a set
‘Health for All’ vision of Universal Health Coverage. The cancer burden is conventionally measured The Cancer Burden
This publication is by no means exhaustive and as numbers of new cases or deaths from cancer
of recommendations for investments across the (most usefully as rates – the number per 100,000
does not cover the full range of cancer control Incidence
cancer control spectrum. The identification of interventions, nor does it fully describe cancer population per year), or as prevalence – the number
evidence-based and cost-effective interventions Overall 811,200 new cancer cases (4.5% of the
epidemiology in the African continent. Rather, of cancer survivors. More complex indicators such
is an essential starting point in addressing the key world total) and 534,000 cancer deaths (7.3% of
its purpose is to provide members of the African as the number of person-years of life lost due to
question of how do we prioritise interventions as the world total) were estimated to have occurred in
Organisation for Research and Training in Cancer, cancer, or the disability-adjusted life years lost may
part of achieving UHC? This question will need the AFRO countries in 2018 (Table 1). Crude rates
representatives of Ministries of Health, and civil be used, especially where an economic dimension,
to be answered with regard to each country’s of incidence and mortality are much lower than the
society organisations with a resource to assist them and comparisons with other diseases, are being
epidemiological profile, cancer burden and health global average because of the young age of the
in identifying some key areas for advocacy and considered.
system capacities. However, there are a number of African population (the median age in sub-Saharan
policy attention with regard to integrating cancer
cancer policy actions with strong evidence as to Here we discuss only the first three indicators, for Africa in 2015 was 18.2, compared with 29.6 for
within emerging UHC plans. It encourages cancer
their cost effectiveness, that can be implemented in which estimates for 36 cancers are available from the world). (5) In terms of cumulative risk, however,
scientists, researchers, medical practitioners,
African countries within their UHC planning. the GLOBOCAN 2018 database of the International the difference is much less pronounced. Indeed,
patients and advocates to look beyond their
Agency for Research on Cancer (IARC). (4) The cumulative mortality in African women is greater
individual areas of specialty towards broader issues
numbers presented are for the 47 countries of the than the global average.
of cancer control, to engage in coalition-building
African region of WHO (AFRO) in the year 2018.
and create partnerships with other stakeholders
that can identify and implement cancer control
interventions in their national context to help Table 1.
achieve the vision of ‘Health for All’.
Numbers of new cancer cases and deaths, crude and cumulative rates of incidence and mortality (2018)
R Ferlay J, Ervik M, Lam F, Colombet M, Mery L, Piñeros M, Znaor A, Soerjomataram I, Bray F (2018). Global Cancer Observatory: Cancer Today.
Lyon, France: International Agency for Research on Cancer. Available from: https://gco.iarc.fr/today, accessed 22/08/2019
Incidence Mortality
Crude Crude
Cases % Cum risk Deaths % Cum risk
rate (per rate (per
(000's) of world % (0-74) (000's) of world % (0-74)
100,000) 100,000)
Both Sexes
World 18079 236.9 20.2 9555 125.2 10.6
Africa 1055 5.8% 81.9 13.4 694 7.3% 53.8 9.4
AFRO 811 4.5% 75.5 13.0 534 5.6% 49.7 9.2
Male
World 9456 254.6 22.4 5386 139.9 12.7
Africa 447 4.7% 69.4 12.7 317 5.9% 49.2 9.2
AFRO 330 3.5% 52.4 12.0 232 4.3% 43.2 8.6
Female
World 8623 228.0 18.3 4169 110.2 8.7
Africa 609 7.1% 94.4 14.1 377 9.0% 58.5 9.8
AFRO 481 5.6% 89.3 14.1 302 7.2% 56.2 9.6
8 Cancer control in Africa: paving the way for Universal Health Coverage Cancer control in Africa: paving the way for Universal Health Coverage 9
Since very few countries in Africa have statistics Figure 2 shows the numbers of deaths for the 10
Table 2. on mortality from death registration, the numbers major cancers in the AFRO region. The ratio of
Estimation of cancer incidence for 47 countries of the WHO (AFRO) region of deaths are estimated from incidence rates and deaths to cases provides an approximate measure
Ferlay J, Colombet M, Soerjomataram I, Mathers C, Parkin DM, Piñeros M, Znaor A, Bray F (2019). Estimating the global cancer incidence survival appropriate to the level of development of case fatality (the inverse of survival probability).
and mortality in 2018: GLOBOCAN sources and methods. Int J Cancer. 144(8):1941–1953.
of the country (as described below). Ratios of As can be deduced from Figure 2, the mortality to
incidence to mortality of the different cancers are incidence ratio (M:I) for individual cancers is 45%
therefore somewhat similar in the various countries, for breast cancer, 68% for cervix, 53% for prostate,
Region and geographic patterns of mortality follow closely 55% for Kaposi sarcoma, 66% for colorectal
Source of data and method East Middle North South West Africa
those of incidence. cancers, and 98% for liver and oesophagus cancer.
1 Rates from a national registry 1 1 1 3
2a Rates from a single registry 3 2 2 5 12
Figure 2.
2b Weighted/simple average of two or more registries 5 1 1 7 The most frequent cancer in the countries of Africa in Males (LEFT) and Females (RIGHT)
R Ferlay J, Ervik M, Lam F, Colombet M, Mery L, Piñeros M, Znaor A, Soerjomataram I, Bray F (2018). Global Cancer Observatory: Cancer Today.
3b Estimated from national mortality 1 2 3 Lyon, France: International Agency for Research on Cancer. Available from: https://gco.iarc.fr/today, accessed 22/08/2019
4 "All sites" estimates partitioned using frequency data 1 1 3 5
9 No data: the rates of neighbouring countries or registries 6 5 1 5 17
16 8 1 5 17 47
Males Females
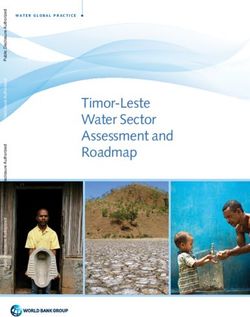
Figure 1 shows the contribution of different cancers Within Africa there are, however, quite marked
to the total burden of incidence and mortality in the geographic variations in these and other cancers.
AFRO countries. In females, cancer of the breast This is due, presumably, to different risk factor
(124,000 or 27% of cases) and cervix (112,000- exposures and potentially the susceptibility of
24.4% of cases) are by far the most burdensome. populations to them. Figure 2 shows the most
numerous cancers in each country, for males
In males, cancer of the prostate dominates in terms (left) and females (right).
of number of cases, (71,000 cases, 22.7% of the
total), followed by liver cancer (24,000; 7.6%) and
colorectal cancers (23,000; 7.5%).
Figure 1.
The most common cancers in the WHO/AFRO region (numbers of cases and deaths, in thousands)
R Ferlay J, Ervik M, Lam F, Colombet M, Mery L, Piñeros M, Znaor A, Soerjomataram I, Bray F (2018). Global Cancer Observatory: Cancer Today.
Lyon, France: International Agency for Research on Cancer. Available from: https://gco.iarc.fr/today, accessed 22/08/2019
Females Males
124
56 Breast Prostate
112 Lung
77
Cervix uteri
71 Liver
Prostate 38
24 23
Kaposi sarcoma
Colorectum
16 16 Non-Hodgkin lymphoma Breast
13 24
13 Liver 23 Leukemia Cervix uteri
15 19
9 NHL 14
12 20
6 Kaposi sarcoma 11
12 14
11 Stomach 13
11 14
11 Oesophagus 14 Cases
8
Lung
15 Deaths
7 15
140 120 100 80 60 40 20 0 0 20 40 60 80 NUMBER (000’s)
10 Cancer control in Africa: paving the way for Universal Health Coverage Cancer control in Africa: paving the way for Universal Health Coverage 11
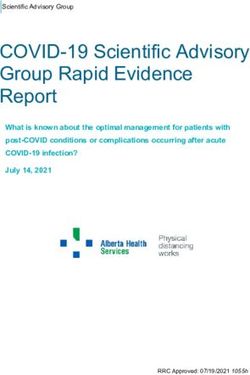
Prevalence The sources of data on cancer incidence are
summarised in Table 2. Of the 47 countries of Figure 3.
There were an estimated 1.45 million cancer
AFRO for which estimates are available, relatively Sources of data on cancer
survivors (at 5 years post diagnosis) in the AFRO
recent cancer registry data were used for 30, while incidence
region in 2018. This is just 3.3% of the world total
the absence of any recent data for 17 meant that Data source: GICR , Map production:
– a lower proportion than for new cases (4.5%
estimates were based on data from neighbouring IARC World Health Organization
- Table 1) because of the poorer prognosis for
countries. Figure 3 depicts the data sources and
cancer cases in Africa. This is reflected in the M:I
methods used in map form.
ratio- it is 53% for the world, 66% for AFRO, and is
a consequence of the type of cancers seen (case Prevalence is a point estimate, not a rate – it is
mix), but also of poorer prognosis for individual the number of cases present at a given point in
cancer types, due to late presentation and poorer time. For cancer, the total number of survivors
therapeutic facilities. (i.e. persons who have ever had a cancer at some
time in their life and survived it) would be difficult
to estimate and would be of little practical value. Incidence availability
Methods and limitations Globocan presents prevalence as number of (May 19)
of the data presented survivors (in 2018) 1, 3 and 5 years after diagnosis.
High Quality PBCR (8)
It is estimated from the incidence of cancer and
It should be remembered that the figures for PBCR (23)
survival probabilities at these intervals post
incidence, mortality, and prevalence in Globocan Registration activities (7)
diagnosis.
are estimates based on the best available data from No information (18)
each country. The data sources and methods used Not applicable
to estimate incidence in each country are described
in Ferlay et al. (6)
Discussion Population-based cancer registries provide the
In Africa, few countries have national vital statistics solid basis for the establishment, monitoring,
systems capable of registering all deaths with For Africa, almost all of the estimates of the and evaluation of cancer control programmes.
medical certification of cause of death. Recent cancer burden, derive from data on cancer Synthetic estimates based on modelling cannot
cancer-specific mortality statistics were available incidence produced by population-based cancer fulfil this role, nor develop and sustain institutional
from only two countries (Mauritius and South registries. Although this means that rates for knowledge and skills for data generation, analysis,
Africa), while older data from São Tomé and limited areas in a country have been assumed to interpretation, and translation. (7) Increased
Príncipe and Cape Verde were also used to represent the whole national population, at least demand for country-led monitoring in the context
estimate 2018 mortality rates. However, most the data are real (rather than being based on of the SDGs is called for in the 2030 agenda for
countries have developed cancer registration statistical models using the estimated prevalence sustainable development (8) and reflected in
systems, recording the numbers of new cancer of risk factors or correlates of cancer incidence). the indicators in the Global Action Plan for the
cases occurring in a defined population (of known This provides an incentive to develop cancer Prevention and Control of NCDs. (9)
composition, by sex and age), allowing incidence registries or to improve their coverage. Local
rates to be calculated. For 43 countries, mortality data are obviously essential to assess how cancer
was estimated by combining the estimates patterns are affecting populations and how trends
of cancer incidence with estimated survival in different cancers are evolving.
probabilities. (6)
© Moonshine Agency
Pty Ltd 2012
12 Cancer control in Africa: paving the way for Universal Health Coverage Cancer control in Africa: paving the way for Universal Health Coverage 13
National cancer control
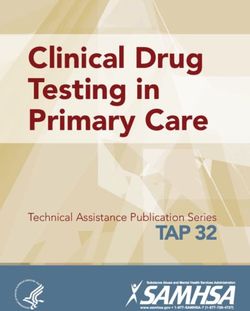
The status of national cancer planning efforts
Figure 4.
Distribution of overall scores of cancer-related
plans reviewed for each region
Nearly 50% (n=18) of the countries surveyed had
control plans in the African Region an NCCP. Of the countries with an NCCP, more
than half are classified as LMICs (n=10). Of those
countries without a cancer- specific plan (n=21) 60%
(i.e. where cancer was addressed through an NCD
plan that encompassed several diseases), two-
National cancer control plans (NCCPs) are Methods thirds (n=14) were LICs. NCCPs across the region 50%
the foundation for cancer control, supporting
were found to be more comprehensive (addressing
countries to identify, prioritise and implement the The data used in this regional analysis comes
key elements of the cancer control continuum
most impactful and cost-effective interventions. from “National Cancer Control Plans: a global 40%
and health system), coherent (linked to other
Politically, they represent a clear, public analysis” (the Global Review), (11) a review of
national health plans) and consistent (aligned with
commitment to action and can also serve as a 527 publicly available cancer-related health
global norms and standards), in comparison to
valuable tool to engage national and international plans including national cancer control plans, 30%
where cancer was addressed through NCD plans
support, through multi-sectoral partnerships noncommunicable disease (NCD) plans which
only. This regional analysis is consistent with the 35% 37% 31% 40% 40% 31%
with civil society and relevant private sector included cancer, and other cancer-related health
findings from the Global Review and underlines 20%
stakeholders in order to reduce the national cancer strategies and policies, as relevant. The Global
the importance of a specific strategy for cancer
South-East Asia
Review analysed documents from 157 countries
Western Pacific
burden and improve patient outcomes.
control. The majority of the plans reviewed had
Middle-East
across all regions and income levels. The Global
The African region has seen a significant increase been produced in the last 5 years (2013 to 2018). 10%
Americas
Review was conducted using a questionnaire
Europe
in the number of countries with a national cancer
Africa
with 121 questions covering 11 domains across The Global Review assessed the quality and
control plan (NCCP) from 46% of countries in 2013 the cancer control continuum, framed through a performance of the plans across the 11 domains, 0%
up to 74% 2017, (10) in line with global trends. health systems approach, namely introduction and and this analysis was used to develop a regional
Cancer-related plans from 39 countries from the overview, prevention, early detection, treatment, score for the African continent. The average score
continent were analysed to provide an overview palliative and supportive care, service delivery, for the region was 35% (Figure 4) and individual
governance, health workforce, health information Figure 5.
of cancer control planning efforts across Africa, country scores ranged from 8%-55%, with a
systems, research and financing. (12) Each of the standard deviation of 11% (Figure 5). This was Individual country scores
discuss strengths and highlight remaining
challenges to tackle this public health issue. 121 questions was investigated and scored. The close to the average score in the global analysis of
Thirty-five countries belong to the World Health overall score represents the proportion of total 36%. We also analysed the distribution of country
Organization (WHO) African region and four to the questions addressed by a plan. For the purpose scores according to the income level within the
Eastern Mediterranean region. of this publication we have analysed an additional region (Figure 6). The results indicate that income
two NCCPs that were not available when the Global level can have an impact on the quality and the
Review was conducted. level of detail of planning for cancer control
activities; however, the scores may also be affected
by countries with weaker health systems that are
facing many competing health demands.
55%
8%
14 Cancer control in Africa: paving the way for Universal Health Coverage Cancer control in Africa: paving the way for Universal Health Coverage 15
Leadership for implementation was more
Figure 6. commonly reported in LICs (90% of plans) and
Representation of overall scores for LMICs (90% of plans) compared to UMICs (50% of
African countries plans).
Civil society organisations (CSOs) are important
stakeholders and often contribute to the
Score development of plans by playing an active role
Category
(%) on planning committees. The role of CSOs is
Global average 36 reinforced in the region’s NCCPs. They were
acknowledged the 85% of plans regionally,
African continent average 35 compared to 72% globally.
African high-income average 42 Monitoring and evaluation were incorporated
in 85% of the plans. However, only one country
African upper middle-income average 42 specified a strategy to implement an accountability
and monitoring framework for progress in the
African lower middle-income average 38
operationalisation phase. Again, this omission
African low-income average 32 mirrors a global trend, as no more than 7% of the
global plans included an implementation strategy
Cancer control spotlights
for monitoring and evaluation.
The main challenges regionally were found in
three domains; namely prevention (35% regional Half of the plans specify financial resources for
average vs 39% global average), early detection implementation, in line with the global average. In
(32% regional average vs 44% global average), and the region, 60% of plans report the costs for further Policy and legislation for Kenya
service delivery (20% regional average vs 23% global planned activities and 20% have an implementation
average). Domains such as palliative care (35% strategy for resource allocation and sustainable the prevention and control Kenya, like many SSA countries, faces a
triple burden from communicable, non-
regional average and globally), health workforce resource mobilisation, compared to 10% globally. of NCDs in Africa communicable diseases, and injuries. The
(21% vs 23%), health information systems (32% vs country has legislation, guidelines and policy
34%) research (22% vs 24%) and treatment (27% vs Governments across many African countries
29%) were all well-defined and equal or very close to
Conclusion are increasingly aware of the heavy burden of
documents that directly impact the prevention
and control of NCDs. These include a National
the global score. Finally, governance (42% vs 36%) NCDs including cancers. This is evidenced by the
The analysis of the cancer-related plans from Africa Cancer Control and Prevention Act, the Non-
and the financial domains’ scores (27% vs 22%) were Brazzaville Declaration on Non-Communicable
is encouraging as many countries have developed Communicable Diseases strategic plan as well
higher in Africa compared to the global average Diseases Prevention and Control in the WHO
new plans since 2013. These cancer plans rely on as policy documents and guidelines on nutrition
score. African Region adopted in 2011, which member
data originating from robust and reliable sources and physical exercise. Kenya also has legislation
countries signed to affirm their political willingness
such as population-based and hospital-based on tobacco and alcohol as well as relatively
Overall, the quality of the plans from Africa to put in place strategies and resources to control
cancer registries. Many plans address core topics high taxes on these products. (14) However,
was similar to the global average, however, we NCDs. (13)
and have a clear accountability framework. These implementation of existing policy and legislation
observed discrepancies between countries. These
can be further strengthened to improve the Civil society and patient groups across Africa play has been slow due to resource constraints.
discrepancies may have resulted from the lack of
comprehensiveness, coherency and consistency of a major role in pressuring governments to develop,
a specific cancer plan in certain countries and the To accelerate progress in combating NCDs in
the plans. fund, and implement NCD control plans.
use of an NCD plan only, which may not necessarily Kenya- civil society, private sector, academics,
cover cancer control planning in as comprehensive a The remaining challenges in cancer control patient groups and the government have now
way as a dedicated cancer control plan. planning such as a developing a comprehensive
Opportunities for change
joined efforts to drive the NCD policy and
strategy in cancer prevention, early detection, Kenya and South Africa are two countries that have legislative agenda forward. This model is much
Readiness for implementation service delivery, as well as identifying financial made strides in addressing the prevention and more effective because the government has
resources and enhancing monitoring and control of NCDs through developing a policy and recognised and leveraged the expertise and skills
The review explored to what extent the plans had evaluation could be addressed through existing legislative framework. that non- state actors have, which are not always
mechanisms for accountability, monitoring and international collaborations, or through available in the public sector. A multistakeholder
evaluation and had identified financial resources partnerships with countries with similar cancer approach can also be replicated in other
required for implementation. Thirty-eight of the burdens and health system capacities. The analysis countries seeking to improve their policy and
thirty-nine plans had the endorsement of the highlights a clear opportunity for countries across legislative environment to tackle NCDs.
Ministry of Health and other relevant governmental the region to share successful experiences and
authorities. Furthermore, 87% of the plans identified best practices to improve the efficiency of cancer
a body responsible for implementation of the plan. control planning.
16 Cancer control in Africa: paving the way for Universal Health Coverage Cancer control in Africa: paving the way for Universal Health Coverage 17
South Africa Submissions were made in support of sodium FCTC implementation Opportunities for change
reduction, the sugar sweetened beverage tax, the
In South Africa (SA), NCDs accounted for 39% of
Draft Liquor Amendment Bill seeking to further in the African region Though many countries in the region are yet to
deaths in 2010 with cancer being the second most fully establish essential infrastructure for tobacco
regulate alcohol marketing and sales, and the
common cause following cardiovascular disease. Challenges across the region control, such as a functional national coordinating
Draft Tobacco Products and Electronic Delivery
(15) In recognition of the growing burden of NCDs mechanism, development and implementation
Systems Bill to further enforce legislation aligning In February 2005, when the World Health
in SA, the country’s commitment to the Political of comprehensive, multisectoral tobacco-control
with the Framework Convention on Tobacco Organization’s Framework Convention on Tobacco
Declaration on NCDs was made at the United strategies, some countries have been able to make
Control. Contributions were also made to the Control (WHO FCTC) entered into force, 40
Nations General Assembly in 2011 for the first remarkable progress to transpose their treaty
National Cancer Control Strategic Framework, countries around the world had ratified the treaty
UN High Level Meeting on NCDs. (16) The 2011 obligations into national action. For example, in
breast and cervical cancer policies, and the draft with Ghana, Kenya, Madagascar, Mauritius and
National Department of Health NCD Declaration February 2019, the Ethiopian Parliament approved
prostate cancer policy which also highlight the Seychelles being amongst these. (27) To date, 44
followed, paving the way for strategies and policies a historic public health legislation that will become
aforementioned risk factors. Other advocacy work of the 181 parties to the FCTC are WHO AFRO
promoting a multisectoral approach to NCD one of the strongest laws in Africa on reducing
included promoting universal health coverage; member states and only three countries from the
control and addressing modifiable risk factors tobacco use. (33) In 2016, Uganda became one of
submissions on the proposed National Health region, Malawi, Mozambique and South Sudan,
such as diet, physical activity, obesity, tobacco few sub-Saharan African countries to implement
Insurance Bill which seeks equality in access to are not Parties. (28) Similarly, in June 2018 when
and alcohol. (17) These included the Strategic comprehensive national smoke-free legislation. In
healthcare, the Medical Schemes Bill and activism the Protocol to Eliminate Illicit Trade in Tobacco
Plan for the Prevention and Control of NCDs, (16) March 2014, Senegal’s parliament adopted a law
on drug patent laws to make cancer medications Products entered into force, 16 of the required 40
National Health Promotion Strategy, (18) Strategy on the manufacturing, packaging and labelling,
more accessible. Parties were African. (29) This was particularly
to Prevent and Control Obesity (promoting healthy sale and use of tobacco. Senegal’s law prohibits,
diets, food environments and physical activity), (19) important as the Protocol was the first legally
amongst other things, any interference by the
National Food and Nutrition Security Policy, (20) binding instrument adopted under the WHO FCTC.
tobacco industry in national health policy. This
regulations requiring salt reduction in foodstuffs, A look at these numbers confirms that countries
is worth mentioning because tobacco industry
(21) marketing of breastfeed milk substitutes in the African region have rapidly embraced the
Call to action interference has been noted to be one of the
(22) and the sugar sweetened beverage tax. (17) FCTC and are doing the same with respect to this
reasons why FCTC implementation is lagging in
(23) Amendments to tobacco legislation have With the rising health and economic Protocol. However, FCTC implementation has failed
Africa.
contributed to reduced tobacco use as shown burden of NCDs in Africa, cost-effective to be identified in many countries as a national
empirically. (17) Civil society organisations have interventions are particularly pertinent. priority. Tobacco control initiatives are frequently As the use of tobacco has declined in high-income
advocated and continue to campaign for policy The World Health Organization’s “Best placed exclusively under the responsibility of countries, the tobacco industry has increasingly
change including the aforementioned statutes and Buys” offer cost-effective approaches on Ministries of Health with little support from turned to low- and middle-income countries,
strategies. interventions to reduce modifiable risk international development partners or from other particularly in Africa, Asia, and Eastern Europe,
factors for NCDs and these are beginning government ministries and departments. to recruit new users. Transnational Tobacco
to be reflected in different national policy Companies are expanding into African countries
Prevalence of tobacco smoking among adults
and regulatory efforts (24) with some early where, excluding South Africa, the tobacco market
in the African region is estimated to be 21% for
reductions in, for example, tobacco use. grew by almost 70% through the 1990s and into the
males (94 million people) and 3% for females (13
(17) (25) Strong and continued advocacy first decade of the 21st century. (34) The industry’s
million people), although some countries have a
efforts are required for policy change, influence is conspicuous within the political and
prevalence of up to 48% for males and 20% for
implementation and enforcement of economic spheres. Internal industry documents,
females. (30) Despite the relatively low tobacco
these programmes in African countries. such as those of British American Tobacco, reveal
prevalence in Africa compared to other regions, a
Additionally, ongoing evaluation of these that tobacco companies have strategically planned
combination of rising incomes, young population
interventions in LMICs is essential to their expansion across Africa for over two decades,
and the tobacco industry’s vigorous marketing
ascertain their efficacy. (26) seeking to “aggressively and consistently” exploit
accounts for a rapid increase in tobacco use in
these “profitable opportunities”. (34)
the region. (31) Therefore, without comprehensive
tobacco prevention and control policies, smoking
prevalence in Africa is expected to rise by nearly
39% by 2030, from 15.8% in 2010 to 21.9% – the
largest expected regional increase globally. (32)
18 Cancer control in Africa: paving the way for Universal Health Coverage Cancer control in Africa: paving the way for Universal Health Coverage 19However, world leaders have always recognised Early detection Opportunities for change
the power of the FCTC in achieving the health
Two Strategies for Early Detection
target of the SDGs. For example, in 2015, at Challenges across the region
the end of the third international conference on Call to action Early detection comprises two distinct public
financing for development in Addis Ababa, world In cancer care, time is of the essence. When health strategies recognised by the World Health
To ensure the sustainability of tobacco
leaders endorsed increasing tobacco taxes as cancer is detected early and effective treatment Organization: early diagnosis and screening. Early
control, African countries need to
a key strategy to reduce tobacco consumption is provided in a timely manner, the probability of diagnosis is defined as the early identification of
continuously increase taxes on tobacco
and the global burden of NCDs and help finance survival increases, while the cost and complexity cancer in patients who already show symptoms of
products to reduce the affordability of all
sustainable development. (35) Also, while SDG 3 of treatment decreases. (38) In the AFRO region in disease, whereas screening is a process that aims to
tobacco products and reduce consumption.
focuses on health, accelerated implementation of 2018, an estimated 811,228 people were diagnosed identify pre-clinical disease in an otherwise healthy
For this to be effective, there is need for a
the FCTC is recognised as one of the “means of with cancer, including almost 300,000 (36%) with and asymptomatic population (Figure 7). (38)
whole of government approach to tobacco
implementation” to reach this goal and the target either breast, cervical, colorectal, or oral cavity
control. (37) It is important that African Early diagnosis focuses on identifying the disease
on NCDs. cancer. (39) When detected and treated at an early
countries raise awareness of the risks of at the earliest possible opportunity and ensuring
stage, patients with these common cancers are
We have seen many African countries prioritising tobacco use particularly among youth timely and coordinated access to diagnosis and
more likely to survive. (40) Despite the increase in
UHC within their national health strategies. To populations and to take actions to monitor treatment. The WHO outlines three steps to effective
global efforts to prevent and control NCDs, (9) there
make UHC feasible, African countries need both and limit the interference of the tobacco early diagnosis: “1) awareness of cancer symptoms
are still vast global disparities in cancer survival,
political will and sufficient funding. Strengthening industry in health-related policy. and accessing care; 2) clinical evaluation, diagnosis
with the lowest survival rates in LMICs. (41) In many
tobacco taxation programs, which are a win-win settings, health systems are fragile, fragmented, and staging, and; 3) access to treatment and
for both public health and domestic revenue and otherwise inadequately prepared to address palliative care.” (38)
generation, is a solution that is being implemented effectively and equitably, the growing burden of
in some countries. (36) Madagascar, for example, Screening involves the use of tests or examinations
NCDs, including cancer.
already has a specific tax levied for the benefit of to identify previously unknown cancers or their
the national tobacco control program which has To significantly reduce global, regional, and precursors in an asymptomatic target population.
helped the country to sustainably enforce tobacco within-country inequities in access to cancer Screening should be viewed as a process, as it
control measures under the FCTC. care, “strategies are needed that link public requires additional resources and coordination
health policies to clinical outcomes.” (42) This is to: inform and invite the target population to
of particular relevance to early detection across participate; administer the screening test and follow
Africa, as patients can face a complex interplay of up with test results; refer as needed for diagnostic
geographic, sociocultural, and financial barriers testing (often requiring imaging and biopsy); and
to accessing effective and affordable cancer ensure that the necessary care pathways are
care services. Even when patients present for accessible without delay. (38)
care soon after noticing a symptom that requires
evaluation for a possible cancer, they are sometimes
misdiagnosed, turned away, or otherwise face Figure 7.
inordinate delays to an accurate diagnosis and Distinguishing screening from early diagnosis
prompt treatment. What is sometimes called according to symptom onset (38)
“patient delay” might in fact reflect inadequate Guide to Cancer Early Diagnosis. Geneva, Switzerland: World
health systems for cancer early detection and care. Health Organization; [2017]. Licence: CC BY-NC-SA 3.0 IGO
Symptom onset
Healthy Abnormal Pre-invasive Invasive Cancer
Death
cells cells Cancer Cancer spread
Screening Early diagnosis
Service provided for a target population Service provided only for people with symptoms
20 Cancer control in Africa: paving the way for Universal Health Coverage Cancer control in Africa: paving the way for Universal Health Coverage 21Health System Considerations At the same time, community-engaged awareness, Screening can be highly effective and cost- Breast cancer highlights the complexity of
adoption of evidence-based screening and effective for certain cancers, in particular cervical selecting the appropriate early detection strategy.
Early detection is a central component of
treatment guidelines, and provider education at and colorectal cancers, where pre-clinical disease Early detection is particularly effective for cancers
comprehensive cancer control. However, it
all levels of the health care system have important (such as cervical pre-cancer and colorectal with self-identifiable symptoms, like a breast
is essential to note that early diagnosis and
roles to play in ensuring any early detection polyps) can be readily detected and treated. mass, where improving awareness of signs and
screening are fundamentally different strategies
strategy is effective to improve cancer outcomes Many countries in Africa have now introduced symptoms can prompt patients to seek timely
in terms of resource and infrastructure
(Figure 8). national cervical cancer screening programmes, evaluation. Screening with mammography, on the
requirements, as well as overall impact and cost.
with varying degrees of success. South Africa’s other hand, can be effective and even cost-effective
(38) To effectively implement early detection
national programme has had little impact to date, in some settings, but is generally resource intensive
programmes, health planners and policy-makers
having reached only 14% of the target population and expensive. (45), (46) According to WHO,
must be equipped with good data on the local/
by 2014. (43) In comparison, Zambia has been population-based breast screening should only be
regional disease burdens (which can be addressed
relatively successful in transitioning to scale, with considered where programmatic infrastructure,
with population-based cancer registries), and
implementation in as many as 75 government-run including quality control, monitoring and evaluation
on sociocultural norms, that can influence
health facilities across 10 provinces. (43) In both are assured. (45) For this reason, screening
acceptability, feasibility and uptake of services.
Zambia and Tanzania, where resources have been mammography is not recommended until a health
appropriately allocated and health systems have system is (at least) able to adequately serve the
been supportive, such programmes have led to needs of all women with palpable breast masses or
Figure 8. sharp declines in both incidence and mortality from other symptoms and signs of breast cancer. (47)
Potential interventions to strengthen early diagnosis (38) invasive cervical cancer over time (see the chapter
on cervical cancer). In the case of colorectal
Guide to Cancer Early Diagnosis. Geneva, Switzerland: World Health Organization; [2017]. Licence: CC BY-NC-SA 3.0 IGO
cancer, population-level screening programmes
have not yet been implemented across the AFRO
region. (44) Careful planning with appropriate Call to action
pre-implementation community and provider The evidence is clear: early detection,
awareness, accompanied by the allocation of
Step 1 Step 2 Step 3 combined with accessible, affordable,
adequate financial and human resources, will be effective, timely treatment, can improve
required to ensure sustainable management and survival and reduce morbidity and mortality
financing of organised programmes. from cancer. As the number of cancer
cases rises annually, and the economic
Awareness Clinical burden of cancer continues to take its toll
and evaluation Access to disproportionately in LMICs, the need
accessing diagnosis and treatment for timely, cost-effective, population-
care staging "The evidence is clear: early level interventions grows urgently. Health
detection, combined with systems across the AFRO region must be
strengthened to meet the growing need
accessible, affordable, effective,
for cancer care and control. Multilateral,
timely treatment, can improve regional and local partnerships to support
survival and reduce morbidity and these efforts can be part of the solution.
Diagnostic
Awareness of symptoms, Accurate clinical Referral for Accessible, high-quality mortality from cancer"
testing and
seeking and accessing care diagnosis treatment treatment
staging
Interventions: Interventions: Interventions: Interventions: Interventions:
• Empower and engage • Improve • Strengthen • Develop • Improve access to treatment
people and communities provider diagnostic referral by reducing financial,
• Improve health literacy and capacity at first and mechanisms geographic, logistical and
reduce cancer stigma contact point pathology and sociocultural barriers
services integrated
• Facilitate access to care
primary care
• provide
supportive
counselling
and peo-
ple-centered
care
© Creative commons
22 Cancer control in Africa: paving the way for Universal Health Coverage Cancer control in Africa: paving the way for Universal Health Coverage 23You can also read