Building the Case for Quality Improvement in the Health Care Industry: A Focus on Goals and Training
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Q Manage Health Care
Vol. 23, No. 3, pp. 138–154
C 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins
Building the Case for Quality Improvement
in the Health Care Industry: A Focus
on Goals and Training
Joy M. Field, PhD; Janelle Heineke, DBA; James R. Langabeer, PhD;
Jami L. DelliFraine, PhD
T
Health care organizations are under intense here is unquestionably a need for a system-
pressure to improve the efficiency and effectiveness atic approach to improving health care de-
of care delivery and, increasingly, they are using livery processes. The 2000 Committee on
quality improvement teams to identify and target Quality of Health Care in America Institute
projects to improve performance outcomes. This of Medicine (IOM) Report, To Err is Human, reports
raises the question of what factors actually drive the that “as many as 98,000 Americans die in hospitals
performance of these projects in a health care each year as a result of medical errors.”1 It further
asserts that “the problem is not bad people; the prob-
environment. Using data from a survey of health
lem is that the system needs to be made safer.”1 Even
care professionals acting as informants for 244
more than a decade after the Institute of Medicine re-
patient care, clinical-administrative, and
port, the consensus among people who study health
nonclinical administrative quality improvement
care is that clinical and patient processes have not
project types in 93 health care organizations, we improved enough and that increasing demands on
focus on 2 factors—goal setting and quality the health care system (eg, an aging population, the
training—as potential drivers of quality passage of the 2010 Affordable Care Act) require re-
improvement project performance. We find that doubled efforts to improve quality, reduce costs, in-
project-level goals and quality training have positive crease access to health care services, and more effi-
associations with process quality, while ciently and effectively use health care resources.2
organizational-level goals have no impact. In The National Institutes of Health, the Institute of
addition, the relationship between project-level Medicine, and the Centers for Medicare & Medi-
goals and process quality is stronger for patient care caid Services recognize that quality improvement ef-
projects than for administrative projects. This forts are necessary to improve health care processes
indicates that the motivational and cognitive effects
of goal setting are greater for projects that involve Author Affiliations: Carroll School of Management,
Boston College, Chestnut Hill, Massachusetts (Dr Field);
interactions with clinicians than for ones that Boston University School of Management, Boston Uni-
involve interactions with other staff. Although versity, Boston, Massachusetts (Dr Heineke); University
project-level goal setting is beneficial for improving of Texas School of Public Health, University of Texas-
process quality overall, our findings suggest the Houston, Houston (Dr Langabeer II); and Department of
Health Administration, Virginia Commonwealth Univer-
importance of being especially attentive to goal sity, Richmond, Virginia (Dr DelliFraine).
setting for projects that impact direct patient care.
Correspondence: Jami L. DelliFraine, PhD, Department of
Health Administration, Virginia Commonwealth Univer-
sity, Grant House, 1008 East Clay St, PO Box 980203, Rich-
mond, VA 23298 (dellifrainj@vcu.edu).
Key words: goals, health care, performance, quality The authors declare that they have no conflict of interest.
improvement DOI: 10.1097/QMH.0000000000000036
138
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.Building the Case for Quality Improvement in the Health Care Industry 139
and reduce costs. As a result, health care reform training with process quality, our measure of project
policies reward hospitals that have better quality and performance, along with the development of the as-
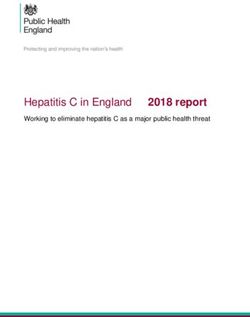
lower costs with higher reimbursement, while hospi- sociated hypotheses. The Figure illustrates the con-
tals with poorer quality, such as preventable readmis- ceptual model for this study and the hypothesized
sions or iatrogenic infections, are reimbursed less.3 relationships.
These changes should motivate providers and orga-
nizations to monitor and improve their processes and
Goals and performance
performance.
The problems of cost and quality are far from People’s conscious ideas affect and regulate their
unique to the United States. In many countries, ac- actions and their performance.6 In particular, Locke
cess to health care is limited or the costs of health care found that people perform at a higher level when
are prohibitive. In countries where health services they have harder rather than easier goals; that spe-
have been accessible, the rising costs of addressing cific goals result in higher levels of performance; and
their populations’ health needs are increasingly chal- that monetary incentives, time limits, and knowledge
lenging. The World Health Organization 2012 report independent of goals and intentions do not affect
estimated that 20% to 40% of expenditure on health performance.6
care is wasted through inefficiency.4 Others, however, warn of some pitfalls of goal
Health care organizations are increasingly using setting. Ordóñez et al7 caution that when goals are
quality improvement teams to identify and imple- overly narrow, people can be too focused and unable
ment projects targeted at improving performance out- to see important aspects of a problem; when individ-
comes. Improvement programs such as Six Sigma uals are not involved in goal setting, it can reduce
and Lean are being applied more frequently in health their commitment; and when focusing on perfor-
care systems, but there has been little study of what mance goals, people may not recognize better alter-
factors make the use of these and other methodolo- natives and fail to learn. Some quality management
gies most effective in the health care environment. leaders, such as W. Edwards Deming,8 have criticized
A theoretical lens that has been used extensively to the use of specific numerical goals as counterproduc-
understand performance outcomes for other types of tive, focusing the workforce more on volume than on
tasks and projects is goal setting.5 We apply this quality.
lens to health care improvement projects and ex- Since Locke’s early work, many studies have tested
tend goal theory by exploring how organizational and the relationship between goals and performance.9-11
project goals affect project performance outcomes, The vast majority have supported the basic premises
and whether the effect of goal setting on project per- of goal theory. Some have identified mediating and
formance differs by project type. While goals focus at- moderating variables, including goal choice, learn-
tention and direct action toward desired performance ing goals, framing, affect, and shared vision.10 In
outcomes, teams also require approaches and tools group situations, scholars have generally found a
for enabling task performance. Thus, we simultane- positive relationship between group goals and group
ously examine whether organizational and project- performance.12,13
level goals and quality improvement training impact In this study, quality improvement goals are con-
project performance outcomes. sidered at 2 levels: the organizational (individual
hospital or unit) level and the project level. At the
organizational level, goals are linked to organization-
LITERATURE REVIEW AND
wide strategic issues such as reducing costs or im-
HYPOTHESES
proving patient satisfaction. At the project level,
We next present the rationale for our conceptual management and the project teams can set very
model of the relationships of goal setting and quality specific outcome goals that support the overall
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.140 QUALITY MANAGEMENT IN HEALTH CARE/VOLUME 23, ISSUE 3, JULY–SEPTEMBER 2014
Figure. Conceptual model and hypotheses (construct items are bulleted).
organizational goals. Within health care systems, both Blumenthal and Ferris15 and Reiter et al16 advo-
some goals are also set at the system level. How- cate creating business cases for health care quality
ever, we focus on organizational- and project-level improvement, Blumenthal and Ferris discuss why
goals because system-level goals are often broad and it is difficult to compute return on investments on
not very specific. It tends to be at the organizational quality improvement efforts and what can be done
and departmental levels that broad system goals are to address those difficulties. Lurie et al17 found that
translated into a specific improvement projects and although it is useful to make both the social and
where improvement methodologies are applied. the business cases when undertaking projects to re-
duce disparities in the delivery of health care, it can
Organizational-level goals be particularly challenging to do so as a practical
The vast majority of hospital strategic and/or matter, because it is often nearly impossible to mea-
business plans include quality improvement as a sure the effects of individual interventions in such
priority.14 In particular, organizations that develop a a complex system. Leatherman et al18 found in their
business case or specific justification for why projects comparative study of 7 health care improvement in-
are selected not only provide the rationale for fo- terventions that while the social case for improving
cusing on quality improvement projects and setting quality was clear, the financial benefit to the part of
performance improvement goals but also include ex- the health care system that was implementing the
plicit or inferred task strategies that form the basis of improvement was not always evident—not so much
project-level goal setting. because financial benefit did not occur but because
However, the relationship between organizational- that benefit accrued elsewhere in the system. Song
level goals and outcomes can be complicated. While et al19 found that health care systems that invested in
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.Building the Case for Quality Improvement in the Health Care Industry 141
high-performance work systems did not tend to have This work suggests the importance of both
explicit financial return expectations for investments organizational-level and project-level goals and sup-
but rather viewed the investment as important to the ports the linkages between them.
realization of the organization’s strategic priorities. As previously discussed, setting goals focuses the
Overall, these studies suggest that measurement is- organization and its employees on relevant problems,
sues, rather than the actual efficacy of organizational- regulates efforts to improve performance, and en-
level goals, account for much of the ambiguity in un- courages the development of strategies and action
derstanding their performance impact. plans to improve performance. More than 400 stud-
Boehler et al20 presented a strong argument for col- ies have found a relationship between challenging,
laboration among clinicians and managers to make specific goals with measurable standards and im-
the business case for quality improvement. They proved performance.5 In a study linking goal theory
found that not only were they able to substantially and quality improvement teams, albeit in a manufac-
improve care for their patients but they were also turing context, Linderman24 found that goals were ef-
able to reduce costs—all while developing trust be- fective in driving performance for Six Sigma projects.
tween the financial and clinical professionals. Despite the evidence of the benefits of goal setting
Thus, we propose the following hypothesis, which for project performance, relatively few health care
extends goal theory broadly to the health care envi- organizations specify goals prior to the initiation of
ronment: quality improvement projects, primarily because it
H1: Organizational-level goal setting will be posi- is assumed that team members are doing their best
tively associated with project performance. to deliver results and, therefore, no explicit goal
is required.25 Thus, to test whether the impact of
Project-level goals project-level goal setting on project performance in
Shah et al21 posit that work is coordinated through a health care setting is consistent with the findings
networks of communication and relationships. This in the goal setting body of literature, we hypothesize
relational coordination is based on shared goals be- that the following:
tween the network of participants in the process im- H2: Project-level goal setting will be positively as-
provement efforts, shared knowledge between the in- sociated with project performance.
dividuals and relationships that exist (organizational Goals serve to focus attention and effort on the de-
and interpersonal), and mutual respect for work.22 sired performance outcome and motivate people to
According to Shah et al21 : work toward that outcome. However, setting project-
level goals in health care can be challenging from a
Shared goals motivate participants to act with motivational perspective, because of what can appear
greater regard for the overall work process, to be the tradeoff between patient-centered outcomes
while shared knowledge informs participants and cost. Allen26 notes that physicians and nurses
how their tasks and those of others contribute are not comfortable focusing on cost for its own sake
to the overall work process. Mutual respect for but rather as a byproduct of more patient-focused im-
others’ work further reinforces the inclination provement efforts. Because they view themselves as
to act in line with the goals of the overall work highly trained professionals, physicians and nurses
process. As a set, the three mechanisms rein-
often reject imposed standardization of processes
force frequency, timeliness, and problem solv-
that limit decision-making discretion.27 Physicians,
ing in communication to improve coordination.
Coordination under this theory is defined as in particular, are more likely to embrace clinical
the conscious activity of assembling and syn- process or outcome improvement efforts rather than
chronizing differentiated work efforts so that ones focused on efficiency gains only.25 In addition,
they function harmoniously in attaining orga- Weiner et al28 note clinicians’ lack of involvement
nizational goals.21,23 where “quality” is not the main focus; they suggest
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.142 QUALITY MANAGEMENT IN HEALTH CARE/VOLUME 23, ISSUE 3, JULY–SEPTEMBER 2014
that administrators tend to narrow the projects se- that the necessary focus of health care performance
lected for quality improvement down to only spe- improvement efforts going forward is “optimizing
cific projects “ . . . to avoid the appearance of man- clinical and service outcomes at minimum cost.”
agement encroachment on physician autonomy in In this study, we focus on process-level perfor-
clinical decision making.” Thus, for quality improve- mance outcomes linked to quality management
ment teams in health care settings, goals related to practices such as quality improvement teams.30
patient-centered projects and outcomes may be more More specifically, we define “process quality” as
motivating to team members. attributes related to the execution and perceptions
Furthermore, while we expect project-level goals of the process.38 Based on the key process-level per-
to be beneficial overall for improving performance formance dimensions just identified from the health
(as in H2), the actual opportunities to impact perfor- care quality improvement literature, this includes
mance outcomes are not equal across project types.25 decreased errors, improved patient flows, improved
For example, projects vary in terms of length and process or labor efficiency, and enhanced patient sat-
scope as well as the amount of effort required. In this isfaction. We also include improved clinician satis-
study, we look at 3 types of improvement projects: faction as a process quality dimension to capture the
patient care (such as improving operating room flow benefits for team participants. This definition of pro-
or reducing medication errors), clinical administra- cess quality is consistent with a focus on improving
tive (such as admissions or managing clinical sup- clinical and service outcomes through better process
plies), and nonclinical administrative (such as billing quality, with decreased cost as a separate perfor-
or accounts payable). Overall, because goals drive mance outcome.2 Thus, project performance, defined
both motivation and effort to improve, and these as process quality, consists of 5 dimensions in total.
factors can vary by project type, we further explore To further explore alignment between project type
whether and how the effect of project-level goal set- and performance outcomes in the context of project-
ting on performance improvement differs by project level goal setting, we draw on insights from the cus-
type. tomer contact model.39-42 According to the customer
In previous studies of health care quality im- contact model, the predominant orientation of back
provement programs, performance outcomes have office processes is on cost and efficiency, while the
been divided into clinical and process-level orientation of front office processes is on enhanc-
performance.27,29 Clinical performance refers to the ing the customer (or more broadly, the stakeholder)
patient medical outcomes, such as mortality, read- experience. In the continuum from front office to
mission rates, and receipt of recommended treatment back office, direct patient care processes are primar-
protocols.14,27,29-31 Process-level performance relates ily front office processes; clinical administrative pro-
to how health care services are delivered and in- cesses are a mix of back office (e.g., managing clinical
cludes, for example, the level and quality of patient- supplies, determining test results, using electronic
provider interaction, waiting times and total process medical records) and front office (e.g., admissions)
flow time, the efficiency of check-in, and the accu- processes; and nonclinical administrative processes
racy of hospital bills.29,32-35 Quality improvement ef- are primarily back office processes.
forts frequently emphasize reducing errors.32,33,36 Er- We contend that the conceptual alignment of the
ror reduction affects not only clinical performance, process quality construct dimensions is greater for
especially for patient care projects, but also process- front office than for back office processes. This is
level outcomes in both patient-facing and back office because 4 of the 5 dimensions of process quality
activities. In addition, health care providers are in- (i.e., decreased errors, improved patient flows, en-
creasingly focusing on patient satisfaction as a key hanced patient satisfaction, and improved clinician
performance metric that captures perceptions of the satisfaction) are closely tied to managing and evalu-
patient experience.14,29,33,35,37 Overall, Green2 states ating the patient-provider interactions in front office
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.Building the Case for Quality Improvement in the Health Care Industry 143
processes, where “providers” include both clinicians because the connection between the project type and
and staff with direct patient contact. the improvement in the performance dimension is
However, while a focus on efficiency is typically less evident.
associated with back office processes, process or la- In summary, we expect the effect of project-level
bor efficiency, clinical, and other process outcomes goal setting on process quality to be greater for front
can be mutually supportive if team members recog- office (i.e., involving the interactions between pa-
nize that pursuing goals to improve efficiency may tients and providers) than for back office project types
help not only eliminate wasted administrative time for the following reasons. First, providers, especially
and effort for both patients and providers but also clinicians, are primarily focused on improving the
translate into more clinician time for meaningful patient experience and only secondarily on issues
patient care and indirectly lead to better patient such as cost. Second, front office projects are more
outcomes.43 In particular, many quality improve- conceptually aligned with our process quality di-
ment projects are now focusing on shortening treat- mensions and, therefore, afford greater opportunities
ment times and are evolving from clinical needs. to improve along these dimensions. Taken together,
For example, some quality improvement efforts that this suggests that because the theoretical basis for
focus on reducing systemic delays (such as reduc- setting goals is to motivate and encourage quality im-
ing door-to-balloon times) may increase efficiency, provement efforts, project outcomes that are priority
but the primary objective is clinical improvement.44 for providers (i.e., improved patient experience) and
These time-to-treat projects should also have cost goals that are directly aligned with these types of
savings, but rarely do quality improvement teams projects will enhance the motivational and cognitive
consider cost or describe the project in terms of effects of goal setting. While we expect goal setting to
efficiency. Thus, when setting efficiency goals for be associated with improved performance regardless
patient care projects, quality improvement teams of the project type, front office project types should
demonstrate an understanding that increased effi- see an even greater positive effect of goal setting on
ciency is important for improving quality of care. In process quality because of the more compelling link
effect, setting efficiency goals for patient care projects between patient-centered projects and desired out-
is done not only to improve efficiency (or even pri- comes from the perspective of the quality improve-
marily to improve efficiency) but because of the clear ment team members. Thus, based on the front office
implications for quality of care. to back office ordering of patient care, clinical admin-
While much of the goal setting literature has fo- istrative, and nonclinical administrative projects, we
cused on the motivational effects of goals, some re- hypothesize the following:
searchers have argued that goal setting has cogni- H3: Project type moderates the relationship be-
tive benefits as well.5 Campbell et al45 suggest that tween project-level goal setting and process quality.
goals will help employees recognize what tasks to Specifically:
perform if the goals give employees clear information H3a: The relationship between project-level goal
about where to direct their efforts. We argue that this setting and process quality will be stronger for patient
cognitive benefit is more manifest when the project care projects than for administrative project types.
type is conceptually aligned with its performance H3b: The relationship between project-level goal
goals. This alignment makes it easier to identify setting and process quality will be stronger for
opportunities to improve, because employees better clinical-administrative projects than for nonclinical
understand where to direct their efforts and what administrative projects.
tasks to perform. For projects and performance goals
Quality improvement in health care
without this conceptual alignment (e.g., patient care
projects and cost), we expect it to be more difficult to More than 2 decades ago, Laffel and Blumenthal46
determine what improvement strategies to employ, made the argument that the application of
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.144 QUALITY MANAGEMENT IN HEALTH CARE/VOLUME 23, ISSUE 3, JULY–SEPTEMBER 2014
“industrial” quality improvement methodologies effective tool for clinicians when specific training
such as Six Sigma and Lean could help move qual- and support were provided.14,33,54-56
ity improvement in health care from a static model In general, for quality programs to be successful,
of conformance to a continuous improvement model. participants require approaches and tools to apply to
Boyer et al47 found that health care–specific quality improvement projects.57-60 Shah et al21 refer to this
practices are associated with process quality as mea- as shared knowledge that not only supports shared
sured by the adherence to the Centers for Medicare goals but enables problem solving. Given that the
& Medicaid Services quality of care measures across teams in our study are all engaging in quality im-
medical conditions including myocardial infarction, provement initiatives such as Six Sigma, Lean or
heart failure, pneumonia, and surgery-related infec- others, we focus on the more fundamental question
tion. Lloyd and Holsenbach described positive re- of the impact of team member quality training and
sults of a Six Sigma application in a radiology process knowledge on the effectiveness of quality improve-
and in medication administration in a hospital set- ment efforts. Because quality improvement training
ting but warned that management commitment must is likely to influence the way team members formu-
be demonstrated through investment in data collec- late and execute task strategies, we hypothesize the
tion, analysis capability, and time away from the following:
clinical environment to collect and analyze data.48 H4: Training on quality methods will be positively
Tsasis and Bruce-Barrett49 described the implemen- associated with project performance.
tation of Lean in a children’s hospital in Toronto,
Canada, and the resulting shift in organizational cul-
ture to be more collaborative and data-driven. METHODOLOGY
The recognition of the simultaneous need for more
Data collection
efficient processes, faster patient flow times, and bet-
ter clinical outcomes has led to the increasing use We designed a survey instrument to explore the
of Six Sigma and Lean approaches to quality im- factors associated with health care quality improve-
provement in health care settings.32,50,51 But while ment project performance comprising 36 questions
Six Sigma, Lean, and other quality improvement ap- organized around these factors and performance out-
proaches are gaining traction in health care systems, comes. The survey used a combination of yes-no, Lik-
there is evidence that such quality improvement pro- ert scales and open-ended formats. Before adminis-
grams are more effective when they are clearly linked tering the survey electronically using Qualtrics, we
to organizational strategy via explicit goals, when assessed face validity by relying on a pilot test group
projects are chosen to align with strategic organiza- of executives at 5 different hospitals, all of whom
tional objectives, and when they incorporate cross- were representative of the sample selected. Minor
functional teams.25 In particular, the quality con- changes were made to the survey on the basis of their
text (i.e., market-based quality pressures, manager’s feedback.
knowledge, top management support, and a strong The target respondents were managers and higher
quality department) provides a necessary framework in health care organizations in the United States
in which hospital quality management efforts affect who had responsibilities over both clinical and non-
performance.52 clinical quality improvement projects. We identified
Previous research has shown that health care a professional society that focuses on quality im-
quality improvement programs have the potential provement in health care, the Healthcare Information
to improve performance, but that the overall im- and Management Systems Society and the Manage-
pact of these programs on patient outcomes re- ment Engineering and Process Improvement (MEPI)
mains questionable.32,50,51,53-55 However, quality im- committee, which is a large Healthcare Information
provement programs were found to be an especially and Management Systems Society committee. The
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.Building the Case for Quality Improvement in the Health Care Industry 145
committee represents a subset of approximately 500 of 7 categories of whom the respondent reports to
professionals involved in quality management and (χ 2 = 5.91; P = .43). When comparing the study
improvement. An e-mail was sent with a link to the sample with the MEPI profile on the type of or-
survey in the first week of March 2010. Ninety of the ganization (hospital/multihospital health system or
e-mails were immediately returned as undeliverable, other type of organization), the study sample has a
yielding an effective sampling frame of 410. We re- higher proportion of hospitals than the MEPI profile
ceived 62 survey responses within the first 3 weeks. (χ 2 = 23.33; P = .00). However, the high propor-
A second reminder e-mail was distributed in early tion of hospitals in the sample is not surprising since
May, which yielded 13 additional responses. hospitals are the front line for health care quality im-
To increase the survey sample size, we identified a provement efforts.
second very similar professional society that focuses
on quality improvement in health care: the Society
Measurement of variables
for Health Systems (a division of the Institute for In-
dustrial Engineering). This organization has approx- Each respondent in the study answered questions
imately 450 members. A second wave of e-mails was about quality improvement projects in their health
distributed in the first week of August 2010 to Soci- care organizations. The questions focused on ei-
ety for Health Systems, from which we received an ther the use of projects at the organizational level
additional 47 responses. or a specific type of project (patient care, clinical-
From the 2 societies together, we received 122 re- administrative, and nonclinical-administrative).
sponses out of 860 members, for a response rate of
Dependent variable
14%. Of the 122 respondents, 18 indicated that their
health care organization had not worked on any qual- To measure process quality, the respondents an-
ity improvement projects in the last year, leaving 104 swered the question, “How would you evaluate
respondents whose organization worked on at least project performance in each category?,” for the 5
1 type of project in the previous year. Each respon- process quality construct items (i.e., decreased er-
dent completed the survey for up to 3 project types rors, improved patient flows, improved process or
(patient care, clinical administrative, nonclinical ad- labor efficiency, enhanced patient satisfaction, and
ministrative), as applicable within their organization, enhanced clinician satisfaction) for each project type
with an average of 2.7 project types per organization. (i.e., patient care, clinical administrative, and non-
The MEPI surveys its members each year to pro- clinical administrative) using a 7-point Likert scale.
file its membership in terms of demographic and or- The possible responses ranged from 1 = no improve-
ganizational characteristics (the Society for Health ment to 7 = very significant improvement.
Systems has a similar profile). On the basis of the
results of the 2010 survey (http://www.himss.org/ Independent variables
content/files/MEPI 2010 Survey.pdf), we compared To measure project-level goal setting, we asked re-
our study sample with the MEPI profile on 3 ques- spondents to assess how often specific, measurable
tions to assess potential sample biases. For the first goals are set for each process quality measure and
question about the respondent’s position held in the project type at the onset of the project49 using a scale
organization, a χ 2 test comparing the observed fre- that ranged from 1 = never to 4 = sometimes to
quency of 9 categories of positions in the study sam- 7 = always.
ple with the expected frequencies from the MEPI To test whether project type moderates the rela-
profile showed no significant differences between tionship between project-level goal setting and pro-
the sample and the MEPI profile (χ 2 = 7.34; P = cess quality, we constructed 2 orthogonal Helmert
.50). Similarly, no differences were found between contrasts for project type.61 If we had instead
the study sample and the MEPI profile in terms included 2 simple indicator variables for the project
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.146 QUALITY MANAGEMENT IN HEALTH CARE/VOLUME 23, ISSUE 3, JULY–SEPTEMBER 2014
type, the omitted project type would have served as title?” The text responses were then coded as hospi-
the baseline intercept for the model. However, with tal/corporate executive, department head/director,
Helmert contrasts, the overall intercept can be inter- and project manager/consultant/team leader within
preted as the performance level for an average project or across departments. The last control variable is
type. In addition, the Helmert contrasts chosen were the number of years of respondent health care expe-
of theoretical interest in this study. Helmert1 is the rience, which was input directly by the respondent
difference between clinical-administrative projects (i.e., no scale was provided) and ranged from 1 to
and nonclinical-administrative projects. Helmert2 is 42 years.
the difference between patient care projects and the
average of the 2 administrative project types. We then
Confirmatory factor analysis
constructed interaction terms between the project
type contrasts and goal setting for quality perfor- We conducted a confirmatory factor analysis (CFA)
mance. The terms Helmert1 × Project-level goal set- in Stata version 13.0 with the latent variables: pro-
ting and Helmert2 × Project-level goal setting are cess quality, project-level goal setting, and quality
used to test H3b and H3a, respectively. training. Respondents acted as informants for their
Organizational-level goal setting was measured by organizations and because they reported on up to
asking respondents how often their organization de- 3 project types within the organization, project types
velops a “business case” or specific justification are nested within organizations. Thus, we used ro-
for why projects are selected.8,61 Responses include bust standard errors clustered by organization in the
1 = never, 2 = very rarely, 3 = sometimes, 4 = fairly CFA.65 With robust standard errors, the only fit statis-
regularly, and 5 = always. Quality training was mea- tic Stata calculates for the measurement model is the
sured with 2 items asking respondents about the ex- standardized root mean square residual (SRMR). The
tent to which team members are provided training SRMR of 0.05 satisfies the Hu and Bentler criteria
on quality tools and programs and training on team of less than 0.08.66 For both the CFA and the subse-
effectiveness.14,33,54,55 quent structural equation model, missing data were
deleted listwise, which resulted in a final sample size
Control variables of 244 project types from 93 organizations (out of the
We included an organizational-level Likert scale original 104 organizations).
control variable—the extent to which quality im- Because respondents answered questions about
provement projects are chosen on the basis of both the independent and dependent variables, com-
alignment with organizational strategy or larger mon method variance (CMV) is a potential concern.
initiatives—because quality improvement activities To test for CMV, we conducted a Wald test during the
that are aligned with the overall goals of the organi- CFA that compares a 1-factor model with the factor
zation tend to be more successful.14,25,57,62 structure used in this study. The use of robust stan-
Prior research on health care performance typi- dard errors required us to conduct a Wald test rather
cally includes control variables for ownership status than the usual CFA likelihood ratio test. The hypoth-
and size of the organization.30,35,63,64 In our study, esis that a single factor accounts for all the variance
respondents indicated the ownership status of their in the data is not supported (χ 2 (21) = 17894.39; P <
organization as for-profit, nonprofit, or government. .001), thus allaying concerns about the single method
In addition, because goal setting can occur at of collecting data. This test is analogous to the Har-
multiple levels of the organization, we controlled man’s single-factor test, but the use of CFA is consid-
for whether the organization is a system member.14 ered to be a more sophisticated test for CMV.67 In ad-
Finally, we included control variables related to the dition, while the base question for the process quality
respondents themselves. Respondent job title was and project-level goal setting questions differed, we
based on responses to the question, “What is your job allowed the responses between pairs of performance
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.Building the Case for Quality Improvement in the Health Care Industry 147
measures in the 2 questions to covary to address unconstrained models indicate that the correlation
CMV associated with the structure of the questions. between each pair of variables is different from 1 and
For each multi-item construct, the values of Cron- support discriminant validity.
bach α and composite reliability (Table 1) all exceed
0.7, which indicates that the constructs are internally
Structural equation model
consistent.68 As evidence of convergent validity, all
items load significantly on their constructs (Table 1), Because of the inclusion of latent variables, we esti-
with most items having a factor loading above 0.70.68 mated a moderated structural equation model (SEM)
To establish discriminant validity, we used a CFA on the basis of the conceptual model in the Figure.
approach for each pair of latent variables in Table 1 The model includes estimates of the structural rela-
by estimating 2 models.69 The first model constrains tionships between process quality and each of the
the correlation between the pair to 1, whereas in the following variables: organizational-level goal setting
second model, the correlation is unconstrained. With (H1), project-level goal setting (H2), the interaction
these nested set of models that each differ by 1 df, between the Helmert2 contrast and project-level goal
we conducted a series of χ 2 (1) tests to determine setting (H3a), the interaction between the Helmert1
whether the unconstrained model is a better fit to contrast and project-level goal setting (H3b), and
the data. For all pairs of variables in Table 1, the quality training (H4). In addition to the control vari-
χ 2 test results are significant at the 0.01 level. The ables, the Helmert contrasts themselves are included
significant differences between the constrained and for completeness. To estimate the moderating effect
Table 1
CONFIRMATORY FACTOR ANALYSIS
Standard Factor
Constructs and Scale Items Loadingsa
Process quality (Cronbach α = .89; CR = 0.90; AVE = 0.63)
How would you evaluate project performance in each category?
Decreased errors 0.72
Improved patient flows 0.84
Improved process or labor efficiency 0.70
Enhanced patient satisfaction 0.90
Improved clinician satisfaction 0.80
Project-level goal setting (Cronbach α = .88; CR = 0.88; AVE = 0.60)
How often do you set specific, measurable goals at the onset of the
project related to the following?
Decreasing errors 0.67
Improving patient flows 0.81
Improving process or labor efficiency 0.77
Enhancing patient satisfaction 0.84
Improving clinician satisfaction 0.77
Quality training (Cronbach α = .84; CR = 0.84; AVE = 0.72)
What preparation/training is provided for quality improvement
team members?
Training on quality tools or programs 0.82
Training on team effectiveness 0.88
Abbreviations: AVE, average variance extracted; CR, composite reliability.
a All factor loadings are significant at P < .01.
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.148 QUALITY MANAGEMENT IN HEALTH CARE/VOLUME 23, ISSUE 3, JULY–SEPTEMBER 2014
of project type on the relationship between project- effect of clinical administrative projects (vs nonclin-
level goal setting and process quality in the SEM, ical administrative projects) on the relationship be-
product indicators of the interaction between project tween project-level goal setting and process quality
type and the latent variable project-level goal setting (H3b) is not supported.
were formed and specified following the procedure Three control variables and the 2 Helmert contrasts
recommended by Marsh et al.70 are significant. The indicator variables for both for-
As with the CFA, we used Stata 13.0 with ro- profit (coefficient = 0.679; P < .05) and nonprofit
bust standard errors clustered by organization to ac- (coefficient = 0.296; P < .10) ownership status (vs
count for the nested structure of our data (i.e., project government ownership) are positive and significantly
types within organizations). Because of this struc- associated with process quality, as is being a mem-
ture, the only fit statistic Stata calculates for the ber of a system (coefficient = 0.197; P < .10). The
SEM is the SRMR. The SRMR = 0.05, which again structural equation estimates for the Helmert con-
satisfies the Hu and Bentler66 criteria of less than trasts are both positive and significant, with Helmert1
0.08. (coefficient = 0.107; P < .05) indicating a higher
level of process quality for clinical administrative
projects (vs nonclinical administrative projects) and
RESULTS Helmert2 (coefficient = 0.096; P < .10) indicating
a higher level of process quality for patient care
Table 2 shows the descriptive statistics for the vari- projects (vs the average of the 2 administrative project
ables (means, standard deviations, and correlations), types).
and Table 3 displays the results for the SEM. The
sample size, n, at the project type level is 244, clus-
tered within 93 organizations. DISCUSSION
In H1, we hypothesized a positive association be-
tween organizational-level goal setting and project In this study, we explored how the setting of
performance. With process quality as the dependent organizational-level and project-level goals and qual-
variable, the estimated coefficient for organizational- ity training affects the performance of health care
level goal setting is not significant (coefficient = quality improvement projects. Our conceptual model
−0.025; P > .10). Therefore, H1 is not supported. in the Figure is based on the following premises: goal
However, the coefficient estimates for project-level setting focuses attention and directs action toward
goal setting (coefficient = 0.677; P < .01) and quality desired performance outcomes, with organizational-
training (coefficient = 0.196; P < .05) are both posi- level goals providing the context in which project-
tive and significant. These provide support for both level goals are set; opportunities for improvement
a positive association between project-level goal set- and motivation for pursuing process quality can dif-
ting and process quality (H2) and a positive associ- fer by project type, with project-level goal setting
ation between quality training and process quality having a greater impact on performance when the
(H4). In addition, the interaction between Helmert1 project type and desired performance outcomes are
and project-level goal setting is not significant (co- aligned with these opportunities and motivations;
efficient = −0.011; P > .10), but the interaction be- in addition to goals, teams also require training to
tween Helmert2 and project-level goal setting is pos- acquire approaches and tools for enabling task per-
itive and significant (coefficient = 0.126; P < .05). formance. Thus, by testing this model, we simul-
Thus, the positive moderating effect of patient care taneously examine the roles of organization-level
projects (vs administrative project types) on the rela- and project-level goals and team quality training for
tionship between project-level goal setting and pro- enhancing health care quality improvement project
cess quality (H3a) is supported, while the moderating performance.
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.Table 2
DESCRIPTIVE STATISTICSa
Variable Mean SD 1 2 3 4 5 6 7 8 9 10 11 12
1. Process quality 4.94 1.28 1
2. Project-level goal setting 5.12 1.28 0.79b 1
3. Quality training 4.47 1.54 0.61b 0.60b 1
4. Organizational-level goal 3.65 0.90 0.46b 0.54b 0.53b 1
setting
5. Strategic alignment 5.51 1.25 0.33b 0.33b 0.53b 0.43b 1
6. Ownership status: 0.09 0.28 − 0.04 − 0.12 − 0.23c − 0.04 − 0.20 1
for-profit
7. Ownership status: not 0.77 0.42 0.08 0.03 0.10 − 0.01 0.20 − 0.56b 1
for-profit
8. System member: yes 0.49 0.50 0.13 0.05 0.03 0.01 − 0.05 − 0.16 0.03 1
9. Respondent job title: 0.27 0.45 0.00 0.04 − 0.02 0.05 0.09 − 0.09 0.00 0.08 1
hospital/corporate
executive
10. Respondent job title: 0.34 0.48 − 0.19 − 0.14 − 0.02 − 0.20 0.08 − 0.07 0.05 − 0.11 − 0.01 1
department head/director
11. Respondent health care 18.43 10.73 0.01 0.03 0.13 0.01 0.21c − 0.09 − 0.04 − 0.08 0.19 0.06 1
experience
12. Full-time employees 4.43 1.16 0.06 − 0.01 0.10 0.00 − 0.06 − 0.41b 0.36b 0.29b − 0.08 − 0.08 − 0.05 1
an = 244 project types from 93 organizations (respondents).
bP < .01.
c P < .05.
Building the Case for Quality Improvement in the Health Care Industry
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
149150 QUALITY MANAGEMENT IN HEALTH CARE/VOLUME 23, ISSUE 3, JULY–SEPTEMBER 2014
Table 3 or financial aspects of quality improvement, whereas
they are keenly familiar with how processes of care
STRUCTURAL EQUATION MODEL RESULTS FOR
impact performance outcomes without the need for
PROCESS QUALITY
a business case. This suggests that further research is
needed on if and when organizational-level goal set-
Coefficient
Variable Estimate ting impacts other project performance dimensions.
As expected, we found support for the association
Helmert1a 0.107b between project-level goal setting and project perfor-
Helmert2c 0.096d mance. This finding is consistent with other litera-
Project-level goal setting 0.677e
ture that demonstrates a strong association between
Helmert1 × Project-level goal setting − 0.011
Helmert2 × Project-level goal setting 0.126b setting specific goals and better performance.5 On the
Organizational-level goal setting − 0.025 basis of goal setting theory and the customer contact
Quality training 0.196b model, we expected a stronger relationship between
Strategic alignment 0.005 project-level goal setting and process quality for pa-
Organizational status: For-profit 0.679b tient care projects versus the administrative projects.
Organizational status: Non-profit 0.296d
System member: yes 0.197d
In addition, we expected project-level goal setting
Respondent job title: Hospital/corporate − 0.023 to have a stronger relationship with process quality
executive for clinical administrative projects versus nonclini-
Respondent job title: Department − 0.180 cal administrative projects. However, we found only
head/director a moderating effect for patient care projects. This im-
Respondent health care experience − 0.000
plies that the motivational and cognitive effects of
Full-time employees 0.019
N 244 goal setting are greater for projects that involve in-
Standardized root mean squared residual 0.050 teractions with clinicians than for ones that involve
a Helmert1
interactions with other staff (e.g., registration) and is
is the difference between clinical-administrative and
nonclinical administrative projects. suggestive of the particular benefit of goal setting to
b P < .05. focus patient care projects on improving the actual
c Helmert2 is the difference between patient care projects and the
and perceived quality of the underlying processes
average of the 2 administrative project types.
d P < .10. that impact direct patient care.
e P < .01. As predicted, training on quality tools is positively
and significantly associated with process quality.
The hypothesis that organizational-level goal set- This finding makes sense, since many quality
ting is positively associated with project performance improvement tools focus on defining problems,
was not supported. This is consistent with Goldstein measuring outcomes, and benchmarking perfor-
and Naor71 who found no relationship between hos- mance. Quality improvement tools may also provide
pital goal setting and the quality management prac- a clear “how to” for improvement projects, thereby
tices put in place to improve performance. One expla- clarifying task strategies to implement change and
nation for this finding may be related to how process achieve performance goals.
quality is measured. Process quality includes met-
rics focused on and transparent to patients that are
Academic and managerial implications
the “default” orientation for health care quality im-
provement projects.25,26 Thus, a business case or spe- This study provides an example of the type of rich
cific justification for why projects are selected would research environment that operations management
not necessarily be essential for improving patient- researchers can find in the health care industry, an
centered performance. In addition, quality improve- industry that has been slow to adopt quality improve-
ment teams may feel more removed from the business ment tools and practices. However, the academic
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.Building the Case for Quality Improvement in the Health Care Industry 151
literature in operations management in the health level goals for performance improvement is benefi-
care industry is growing as more health care orga- cial overall, project-level goals for improving pro-
nizations embrace quality improvement approaches cess quality generate an added benefit for patient
and the need to evaluate what is and is not effective care projects. As a result, managers should set spe-
becomes more critical.29,36,72-74 Our study adds to cific, measurable goals for all project types, while
this growing stream of research by focusing on how being especially attentive to goal setting for improv-
goal setting and quality training impact health care ing process quality for patient care projects. Third,
quality improvement project performance. because quality training was significantly associated
In terms of academic contributions, the results of with process quality, managers should make sure that
this study support previous research that shows that quality improvement teams have adequate training
specific, measurable goals increase overall perfor- in quality improvement tools and techniques. These
mance. However, this study also shows that goals tools help teams set clearer task strategies for goal
do not uniformly increase performance. For project- attainment.
level goals that focus attention and efforts on perfor-
mance dimensions that are naturally aligned with the
project type, we found that goal setting can be even LIMITATIONS AND CONCLUSIONS
more important for improving performance, in par-
ticular for patient care projects. Although we also ex- Our findings are subject to certain limitations.
pected this result for clinical administrative projects As with all single respondent survey-based studies,
versus nonclinical administrative projects, our find- CMV is a concern. While CMV can never be ruled out
ings did not support the added importance of goals completely, the Wald test during the CFA provides
for improving process quality. These results indicate evidence suggesting that CMV is not a problem in
that more research is needed on understanding the our study. Furthermore, there are other factors that
role of goal setting in driving performance improve- might also be responsible for the success of quality
ments for different types of patient-provider interac- improvement projects, including trust in leadership,
tions. commitment to leadership, and job autonomy.76
In addition, quality training was associated with Although we did control for the alignment of projects
better performance outcomes in this study. Although with the organization’s strategy and a number of
self-efficacy may influence goal setting, this study organizational and respondent characteristics, future
suggests that goal theory could be expanded to em- research could more explicitly account for these
phasize the importance of task strategies enabled and other factors. In addition, there are a number
through quality training in goal attainment.75 of clinical outcomes in addition to decreased errors,
This research also has several managerial implica- improved patient flows, increased efficiency, and
tions. First, our results suggest that organizational- “satisfaction” on the part of either the physician or
level goal setting may not be critical to project the patient. Although we focused on process quality
performance, especially for patient-centered perfor- as the performance outcome in this study, other
mance metrics that are typically the default orien- outcomes that measure patient health would be of
tation for hospitals. However, setting goals at the interest as well.
organizational-level conveys an organizational em- Health care managers are not always flush with
phasis on improving performance metrics that may data on performance, nor are they always certain
be important for organizational success even if they on which data to focus. Since goal setting requires
are not transparent to the patients. Thus, business some degree of knowledge of current performance
cases may still be important for focusing attention levels, the health care industry has been slower
and driving improvement on these other perfor- than other industries to adopt quality improvement
mance dimensions. Second, while setting project- initiatives. However, health care managers are now
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.152 QUALITY MANAGEMENT IN HEALTH CARE/VOLUME 23, ISSUE 3, JULY–SEPTEMBER 2014
getting key information systems in place—such as 12. Locke EA, Durham CC, Poon JML, Weldon E. Goal setting,
electronic medical records, physician order entry, planning, and performance on work tasks for individuals and
groups. In: Friedman SL, Scholnick EK, eds. The Developmen-
monitoring and tracking systems—to extract per- tal Psychology of Planning: Why, How, and When Do We
formance and outcome data and better understand Plan? Mahwah, NJ: Lawrence Erlbaum Associates Publishers;
baseline trends and patterns. This new focus on 1997:239-262.
13. O’Leary-Kelly AM, Martocchio JJ, Frink DD. A review of the
benchmarking and quality improvement in health influence of group goals on group performance. Acad Manag
care suggests that health care managers have in- J. 1994;37(5):1285-1301.
creasing opportunities to set actionable goals on the 14. Cohen AB, Restuccia JD, Shwartz M, et al. A survey of
basis of relevant data to improve clinical outcomes, hospital quality improvement activities. Med Care Res Rev.
2008;65(5):571-595.
project performance, and, ultimately, organizational 15. Blumenthal D, Ferris T. The business case for quality:
performance. In addition, many are also investing in ending business as usual in American health care Web
human resources to drive such improvement, which site. www.commonwealthfund.org/usr doc/715 Blumenthal
business case.pdf Published 2004. Accessed July 1, 2011.
is important in promoting the collaboration between 16. Reiter K, Kilpatrick K, Green S, Lohr K, Leatherman S. How to
clinicians and managers. Our study contributes to develop a business case for quality in health care. Int J Qual
furthering this agenda by moving toward a better Health. 2007;19(1):50-55.
17. Lurie N, Somers SA, Fremont A, Angeles J, Murphy EK. PER-
understanding of health care quality improvement SPECTIVE: Challenges to using a business case for addressing
project performance and, in particular, the roles of health disparities. Health Aff. 2008;27(2):334-338.
goal setting, at both organizational and project levels, 18. Leatherman S, Berwick D, Iles D, et al. The business
and quality training for improving process quality. case for quality: case studies and an analysis. Health Aff.
2003;22(2):17-30.
19. Song PH, Robbins J, Garman AN, McAlearney AS. High-
performance work systems in health care, part 3: the role of
the business case. Health Care Manag Rev. 2012;37(2):110-
121.
REFERENCES 20. Boehler R, Hardesty D, Gonzales E, Kasnetz K. The business
case for quality. Health Financ Manag. 2009;63(10):62-66.
1. Kohn LT, Corrigan J, Donaldson MS. To Err Is Human: Build- 21. Shah R, Goldstein SM, Unger BT, Henry TD. Explaining
ing a Safer Health System. Washington, DC: The National anomalous high performance in a health care supply chain.
Academies Press; 2000. Decis Sci. 2008;39(4):759-789.
2. Green LV. The vital role of operations analysis in im- 22. Gittell JH. Relationships between service providers and their
proving healthcare delivery. Manuf Serv Oper Manag. impact on customers. J Serv Res. 2002;4(4):299-311.
2012;14(4):488-494. 23. Longest B, Klingersmith J. Coordination and communications.
3. Rosenthal M. Nonpayment for performance? Medicare’s new In: Shortell S, Kaluzny A, eds. Health Care Management: Or-
reimbursement rule. N Engl J Med. 2007;357(16):1573-1575. ganizational Design and Behavior. New York, NY: Delmar;
4. WHO, The World Health Report. Health System Financing: 1994:182-211.
The Path to Universal Coverage. Geneva, Switzerland: WHO 24. Linderman K, Schroeder RG, Choo A. Six Sigma: the role of
Press; 2010. goals in improvement teams. J Oper Manag. 2006;24(6):779-
5. Locke EA, Latham GP. A Theory of Goal Setting and Task 790.
Performance. Englewood Cliffs, NJ: Prentice Hall; 1990. 25. Langabeer JR, DelliFraine JL, Heinek J, Abbass I. Implementa-
6. Locke EA. Toward a theory of task motivation and incentives. tion of Lean and Six Sigma quality initiatives in hospitals: A
Organ Behav Hum Perform. 1968;3(2):157-189. goal theoretic perspective. Oper Manag Res. 2009;2(1-4):13-
7. Ordóñez LD, Schweitzer ME, Galinsky AD, Bazerman MH. 27.
Goals gone wild: the systematic side effects of overprescribing 26. Allen S. No waiting: a simple prescription that could dra-
goal setting. Acad Manag Perspect. 2009;23(1):6-16. matically improve hospitals—and American health care.
8. Deming WE. Out of the Crisis. Cambridge, MA: The MIT Press; The Boston Globe. Available at: http://www.boston.com/
2000. bostonglobe/ideas/articles/2009/08/30/a_simple_change_
9. Latham GP, Yukl GA. A review of research on the ap- could_dramatically_improve_hospitals_ndash_and_american
plication of goal setting in organizations. Acad Manag J. _health_care/. Published August 30, 2009. Accessed June 12,
1975;18(4):824-845. 2014.
10. Locke EA, Latham GP. New directions in goal-setting theory. 27. Chandrasekaran A, Senot C, Boyer KK. Process management
Curr Dir Psychol Sci. 2006;15(5):265-268. impact on clinical and experiential quality: managing tensions
11. Tubbs ME. Goal setting: a meta-analytic examination of the between safe and patient-centered healthcare. Manuf Serv
empirical evidence. J Appl Psychol. 1986;71(3):474-483. Oper Manag. 2012;14(4):548-566.
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.You can also read