Build Back Better Act: Health Coverage Provisions Explained
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Build Back Better Act: Health Coverage
Provisions Explained
by Edwin Park, Sabrina Corlette, Anne Dwyer, and Maggie Clark
On November 19, 2021, the House of Representatives passed the Build Back Better Act, the budget
reconciliation bill, with the Senate expected to consider the legislation in coming weeks. The Build Back
Better Act includes numerous provisions that would dramatically strengthen and expand both public
and private health insurance coverage. Some of the new provisions would build on actions Congress
previously took in the American Rescue Plan Act, enacted earlier this year.1
Among its Medicaid and the Children’s Health Insurance Program (CHIP) provisions, the Build Back
Better Act would permanently require states to provide 12 months of postpartum health coverage
and 12 months of continuous coverage for children, make federal funding for CHIP permanent, and
provide a permanent, significant increase in federal Medicaid funding for Puerto Rico and the other
territories. Among its private insurance provisions, the Build Back Better plan would temporarily extend
marketplace subsidies to those in the “coverage gap” in the 12 states that have not yet expanded
Medicaid and also extend the availability of the enhanced marketplace subsidies enacted in the
American Rescue Plan Act.
This issue brief explains the Build Back Better Act’s Medicaid, CHIP and private insurance provisions.
November 2021 CCF.GEORGETOWN.EDU BUILD BACK BETTER 1
Medicaid and CHIP Provisions in the Build Back Better Act
Most notably, the Build Back Better Act would finally provide implement 12 months of continuous eligibility for children
coverage to low-income adults stuck in the Medicaid under age 19 in both Medicaid and CHIP. This requirement
“coverage gap” in states that continue to refuse to adopt would take effect one year from date of enactment.
the Medicaid expansion. (See page 11 for discussion of
This provision would significantly reduce the risk that
how the Build Back Better Act would temporarily extend
children face periods of uninsurance over the course of
marketplace subsidies to this group.) It also includes
a year. Nearly 10 percent of children are uninsured for at
numerous Medicaid and CHIP provisions that would expand
least part of the year. But among children with incomes
coverage and access in the following areas:
below 250 percent of the federal poverty line, 13 percent
z Children’s coverage of children experience a gap in coverage at some point
z Maternal health during a year or are uninsured for the entire year. These
gaps in coverage are even more prevalent among children
z Coverage stability during and after the COVID-19
in communities of color: 14 percent of Latino children and
pandemic
nearly 12 percent of Black children experience uninsurance
z Medicaid in Puerto Rico and the other territories
over the course of a year.3
z Long-term services and supports and home- and
community-based services Mandatory continuous eligibility for children would reduce
the risk of gaps in coverage and limit the impact of churn
z Behavioral health
when children cycle on and off coverage due to temporary
z Criminal justice reform
changes in family income. This, in turn, would improve
z Indian and Native Hawaiian health care health status and well-being as research shows that
z Drug pricing, prescription drug and vaccine coverage individuals with continuous coverage experience fewer
unmet health care needs and are in better health. It would
Some of these provisions would place new federal also promote health equity, mitigate the financial impact of
requirements on states while other provisions would offer income volatility on families, drive more efficient health care
states new or expanded options in their Medicaid and CHIP utilization and spending, reduce administrative burden and
programs. Many provisions would require significant state costs for states, enhance measurement of quality of care
implementation efforts. See Table 1. and increase accountability for managed care.4
Permanent Extension of Federal CHIP Funding,
Children’s Coverage
Other CHIP Provisions
Requirement for Medicaid and CHIP 12-Months CHIP serves a vital role in America’s health care system by
Continuous Eligibility for Children providing comprehensive, affordable health coverage to 6.8
million people (mostly children) each month whose family
While there is a longstanding option for states to provide
incomes are over income eligibility levels for Medicaid but
up to 12 months of continuous eligibility for children in
may otherwise be uninsured.5 First enacted in 1997, CHIP
their Medicaid and CHIP programs, only 24 states do so in
has been a success story in advancing children’s coverage.
both Medicaid and CHIP. (Some additional states provide
However, due to the temporary and capped nature of the
continuous eligibility only for some children or only for
program’s federal funding structure, Congress has had to
children in separate state CHIP programs. 17 states and
repeatedly act to provide additional years of federal funding.
the District of Columbia do not have continuous eligibility
for Medicaid or CHIP for any children. See Appendix Table
1.)2 The Build Back Better bill would require all states to
2 BUILD BACK BETTER CCF.GEORGETOWN.EDU November 2021Table 1. Medicaid and CHIP Provisions
Provision Federal Requirement for New State
States or State Option Implementation Required
Children’s Coverage
Medicaid and CHIP 12-Months Continuous Eligibility for Children Requirement Y*
Extension of Federal CHIP Funding N/A N
Extension of Express Lane Eligibility Option for States Option Y**
Maternal Health
Medicaid and CHIP 12-Months Postpartum Coverage Requirement Y*
Maternal Health Homes Option Y**
Stability of Coverage During and After Pandemic
Transition from Medicaid Continuous Coverage Requirement Requirement*** Y
Temporary New Medicaid Stability Protection Requirement N
Medicaid in the Territories
Federal Medicaid Funding for Puerto Rico and the Other Territories N/A**** N****
Long-Term Services and Supports and Home- and Community-Based Services
Federal Medicaid Support for Home- and Community-Based services Option Y**
(HCBS)
Extension of Spousal Impoverishment Protections for Individuals Requirement N
Receiving Home and Community-Based Services
Extension of the Medicaid Money Follows the Person Demonstration Option Y**
Behavioral Health
Expansion of the Medicaid Certified Community Behavioral Health Option Y**
Clinic Demonstration Program
Extension of State Option to Provide Qualifying Community-Based Option Y**
Mobile Crisis Intervention Services
Criminal Justice Reform
Improved Continuity of Care and Health Care Access for People Requirement Y
Involved in the Criminal Justice System
Indian and Native Hawaiian Health
Extension of Federal Support for Certain Indian Health and Native Requirement N
Hawaiian Health Providers
Drug Pricing, Prescription Drug and Vaccine Coverage
Extension of Medicaid Drug Rebate Program to Separate State CHIP Requirement Y
Programs
Improvements to Accuracy of Medicaid Drug Pricing Survey of Requirement Y
Pharmacies
Permanent Prohibition Against Implementation of Rebate Rule N/A N
Requirement for Medicaid and CHIP to Cover Vaccines for Adults Requirement Y*
* Only if states have not already adopted existing options
** Only if option newly adopted by states
*** As condition of increased federal Medicaid matching rate (FMAP) from April-September 2022
**** Puerto Rico would be required to comply with a physician payment floor but it currently meets that requirement
November 2021 CCF.GEORGETOWN.EDU BUILD BACK BETTER 3During the most recent funding extension, Congress actually funding reauthorization legislation, the stability provision
let annual funding for CHIP lapse entirely from September prohibits states from making their eligibility standards,
30, 2017 until January 22, 2018 — forcing states to rely on methodologies and procedures more restrictive, such
carryover funding and, in some cases, to notify families that as cutting income eligibility or imposing new barriers to
they were planning to close enrollment. While Congress enrollment such as increased premiums.
ultimately acted to provide federal CHIP funding for ten
Finally, the Build Back Better Act includes a technical
years, no additional funding is available after fiscal year
provision that would allow certain states to increase
2027.
children’s income eligibility through a state plan amendment,
The Build Back Better Act would permanently extend federal rather than through a waiver. This would make it easier for
funding for CHIP, thereby removing financial uncertainty some states to expand their CHIP programs and cover more
and ensuring stability for states and families that depend on children who would otherwise be uninsured. It would also
the CHIP program. The Build Back Better Act would also ensure that territories that take up this new state plan option
permanently extend a number of related CHIP financing would be able to have their CHIP allotments increased to
provisions including redistribution (which transfers unspent account for any expansion as is the case for states. (States
funds after two years to states facing federal funding have their allotments “rebased” every two years to account
shortfalls), the Child Enrollment Contingency Fund (which for their actual spending but prior to the Build Back Better
provides additional federal CHIP funds to states that have Act, states, but not territories, could have their allotments
higher-than-expected enrollment and have exhausted their adjusted between rebasing years if they expand their CHIP
available CHIP funding) and the qualifying state option programs.)
(which allows states that expanded children’s coverage in
Medicaid prior to enactment of CHIP to fund a portion of Permanent Extension of Express Lane Eligibility
such Medicaid child expansions).
Option for States
The Build Back Better Act would also extend other related Express Lane Eligibility (ELE) is a state option that allows
child health provisions including the Pediatric Quality states to use the eligibility findings from other public
Measures Program (PQMP) and grants for child-specific programs like the Supplemental Nutrition Assistance
outreach and enrollment. Federal funding for the PQMP, Program (SNAP) to streamline enrollment and/or renewal for
which supports the advancement and reporting of evidence- children in Medicaid and CHIP. Seven states currently use
based, consensus-driven pediatric quality measures, would ELE in their Medicaid programs or in both their Medicaid and
be made permanent. The PQMP would receive $15 million CHIP programs.6 The ELE state option is currently set to
in fiscal year 2028, with annual adjustments for general expire at the end of fiscal year 2027. The temporary nature
inflation thereafter. In addition, federal funding for outreach of the option has been a factor in discouraging states from
and enrollment grants would be made permanent. $60 implementing it, due to the need for an upfront investment
million would be appropriated over a three-year period of time, spending and technology to maximize its efficiency
(fiscal years 2028-2030) and then subsequently adjusted for and effectiveness. The Build Back Better Act would
general inflation for additional three-year periods. These permanently extend the ELE state option, which would not
grants serve an important role in helping to ensure eligible only allow existing use of ELE to continue over the long run
children can access and maintain Medicaid and CHIP but also could spur adoption of ELE by additional states.
coverage.
The Build Back Better Act would also permanently extend Maternal Health
the existing Medicaid and CHIP stability provision for
children, which prohibits states from cutting eligibility or Requirement for Medicaid and CHIP 12-Months
making it harder for eligible children to enroll. Originally Postpartum Coverage
included in the ACA and subsequently extended in CHIP The Build Back Better bill would permanently require all
4 BUILD BACK BETTER CCF.GEORGETOWN.EDU November 2021states to extend full-benefit postpartum Medicaid and include doulas, community health workers, behavioral health
CHIP coverage from 60 days after the end of pregnancy specialists, social workers, interpreters, and many other
to one year postpartum, starting in the first fiscal year partners who can support the medical and social needs of
quarter beginning one year after date of enactment (which pregnant and postpartum people.
could be as early as January 1, 2023). This permanent and
Maternal health homes would also be required to collect and
mandatory extension of coverage to one year postpartum
report quality metrics, including measures in the Centers for
would thus establish a new national standard for Medicaid
Medicare and Medicaid Services’ Child Core Set and Adult
and CHIP coverage, which covers about 43 percent of
Core Set, and conduct risk assessments and create care
births each year. This is a critical step in responding to
plans for patients. Services provided by maternal health
the alarming maternal mortality crisis in the U.S., which
homes that meet these and other criteria would be eligible
disproportionately affects women of color.7 When Medicaid
to receive a 15 percentage point increase in the federal
and CHIP coverage currently ends at 60 days postpartum,
Medicaid matching rate (FMAP) for the first two years after
many women are at risk of becoming uninsured and missing
the state plan amendment takes effect, not to exceed 90
out on critical access to care that can prevent pregnancy-
percent. The Build Back Better bill would also appropriate
related deaths. The Congressional Budget Office (CBO), for
$5 million for planning grants to interested states, available
example, has previously estimated that about 45 percent of
one year after date of enactment.
women covered by Medicaid on the basis of pregnancy now
become uninsured after the end of the 60-day postpartum The provision includes early intervention providers and
coverage period.8 pediatricians as potential connections for patients, which
would help encourage two-generation care that supports
In the interim, until the requirement to implement 12 months
the healthy development of mothers and infants together.
of postpartum coverage takes effect as early as January 1,
It also would create an opportunity to bring peer support
2023, states can continue to take up the American Rescue
providers, such as doulas and community health workers,
Plan’s state plan option to provide 12 months of postpartum
into Medicaid care models.
coverage in both Medicaid and CHIP and receive federal
matching funds starting on April 1, 2022. A number of states
have already implemented waivers to provide extended Other Investments in Maternal Health
postpartum coverage or plan to implement the American The bill also includes significant investments in training
Rescue Plan state plan option next year, although these and diversification of the perinatal workforce, including
postpartum expansions may be limited.9 See Appendix developing providers of color who treat maternal mental
Table 2. health conditions and substance use disorders. Based
on the bills from the Black Maternal Health Momnibus
New Medicaid Option for Maternal Health Homes package, the Build Back Better bill includes new funding
for maternal health quality improvement, better data
The Build Back Better bill would establish a new permanent
systems to track and identify causes of maternal mortality,
Medicaid state plan option for maternal health homes,
investments in historically Black colleges and universities to
which provide team-based care to pregnant and postpartum
conduct research into maternal health disparities and grants
people. This maternal health home option would take effect
to support implicit bias training for frontline health care
two years (24 months) after the date of enactment.
professionals. Every eligible provision from the 12 bills that
The maternal health home option builds on the requirement made up the Black Maternal Health Momnibus package is
for 12 months of postpartum coverage to provide included in the Build Back Better Act.
coordinated, culturally competent and linguistically
appropriate team-based care to pregnant and postpartum
people and provide linkages to care for medical and social
needs. In addition to medical providers, the team can
November 2021 CCF.GEORGETOWN.EDU BUILD BACK BETTER 5Stability of Coverage During and After existing federal guidance from August 2021 allowing states
to take up to a full year to catch up on delayed renewals
the Pandemic
and pending actions, states will be limited to initiating
renewals or processing changes in circumstances for no
Transition from Medicaid Continuous Coverage
more than 1/12th of enrollees in each month between
Requirement
April and September 2022. States will also be required
Under current law, as enacted by the Families First to make a good faith effort to update contact information
Coronavirus Response Act, states are receiving a 6.2 including mailing addresses, phone numbers or email
percentage point increase in their federal Medicaid addresses, including by coordinating with managed care
matching rates for the duration of the COVID-19 public plans and other state programs. States would be barred
health emergency. As a condition of the increase, states from disenrolling anyone on the basis of returned mail until
cannot cut eligibility or make it harder for eligible families they make at least two attempts to contact the beneficiary
to enroll. They must also provide continuous coverage: through at least 2 modalities and provide at least a 30-day
they cannot involuntarily disenroll any Medicaid beneficiary notice, through at least 2 modalities, before terminating
who was already enrolled or has newly enrolled during the coverage. States will also be required to collect key data
public health emergency. The bill would begin phasing monitoring the impact on enrollees and make reports to
out the matching rate increase starting April 1, 2022, the Secretary of Health and Human Services, including call
with the increase fully eliminated after September 30, center statistics and disenrollment data.10 States would not
2022. Specifically, the FMAP increase would decline to 3 need to meet these new procedural requirements if they
percentage points for April-June 2022 and then decline to refused the increased federal matching rates from April to
1.5 percentage points for July-September 2022. (This would September 2022.
also have the effect of reducing the Families First increase
in the CHIP matching rate from 4.34 percentage points
Temporary New Medicaid Stability Protection
to 2.1 percentage points for April-June 2022 and to 1.05
percentage points for July-September 2022.) See Table 2. While the Build Back Better bill would end the continuous
coverage requirement, health coverage is likely to remain
Table 2. Phase-Down of Families First FMAP volatile for a considerable period of time. The COVID-19
Increases pandemic demonstrated the importance of Medicaid as
a critical source of coverage. The bill therefore would
Medicaid Matching CHIP Matching continue to encourage states to maintain their current
Rate Increase Rate Increase Medicaid eligibility standards, methodologies and
(Percentage (Percentage
Points) Points) procedures between October 1, 2022 and December 31,
Present - 6.2 4.34
2025. States that cut Medicaid eligibility or make it harder
March 31, 2022 for eligible individuals to enroll — compared to the eligibility
April 1, 2022 - 3.0 2.1 standards, methodologies and procedures in effect as of
June 30, 2022
October 1, 2021 — would be subject to a 3.1 percentage
July 1, 2022 – 1.5 1.05
September 30, 2022
point reduction in their regular FMAP. States, however,
could seek an exemption from this requirement for non-
pregnant, non-disabled adults with incomes above 138
In addition, the continuous coverage protection would be percent of the federal poverty line if the state certifies to the
effectively ended April 1, 2022 but as a condition of receiving Secretary of Health and Human Services that the state has a
the phased-down FMAP increase, states would have to budget deficit or is projected to have a budget deficit in the
satisfy a number of procedural requirements before they can upcoming state fiscal year.
terminate Medicaid beneficiaries who have been enrolled
for at least 12 consecutive months (during the period
between April 1 and September 30, 2022). In addition
6 BUILD BACK BETTER CCF.GEORGETOWN.EDU November 2021Medicaid in Puerto Rico and the Other by 0.5 percentage points in the first quarter it is out of
compliance and then by an additional 0.25 percentage
Territories
points in subsequent quarters, but not to exceed a total of 5
percentage points.
Permanent, Significant Increase in Federal Medicaid
Funding for Puerto Rico and the Other Territories Based on spending projections from the territories, the Build
Federal Medicaid funding for Puerto Rico and the other Back Better provision should ensure that Puerto Rico and
territories — American Samoa, Guam, the Northern Mariana the other territories have sufficient federal financial support
Islands and the U.S. Virgin Islands — is capped, with the to sustain their existing Medicaid programs and make further
block grant amounts set at highly inadequate levels that improvements to expand coverage and access over time.
have forced the territories to operate Medicaid programs In the case of Puerto Rico, this would disproportionately
that are far less generous than those in the states.11 In benefit children: more than 60 percent of Puerto Rico’s
addition, the regular matching rate for the territories is children are enrolled in Medicaid or CHIP-funded Medicaid.
officially 55 percent, even though the FMAPs for the The territories, however, will not be able to come into fuller
territories would equal 83 percent if they were calculated in compliance with federal eligibility and benefit requirements
the same way the matching rate for states is determined, without elimination of their block grant structure and a
due to the territories lower per-capita income. Over the last switch to permanent state-like financial treatment under
decade, Congress has provided additional federal Medicaid which the federal government picks up a fixed percentage of
funding and FMAP increases over the last decade in order the territories’ Medicaid costs.
to avoid draconian cuts, respond to recent natural disasters,
and to institute modest eligibility, benefit and provider rate Long-Term Services and Supports and
improvements. But those increases have always been
Home- and Community-Based Services
temporary.
The Build Back Better bill provides a permanent, significant Additional, Permanent Federal Medicaid Support for
increase in the territories’ block grant amounts. In fiscal year Home- and Community-Based services (HCBS)
2022, for example, Puerto Rico’s base block grant amount Medicaid is the largest payer of long-term services and
would be set at $3.6 billion, well above the $2.8 billion supports (LTSS) in the United States, providing coverage
level for 2021 that was provided under the latest temporary for LTSS for millions of individuals including children with
increase enacted by Congress two years ago. These higher special health care needs.13 However, due to a longstanding
block grant amounts would then be adjusted annually by structural bias towards institutional care settings under
the percentage increase in national Medicaid spending in Medicaid, many states have limits on access to home- and
the preceding year (as determined using the most recent community-based services (HCBS). For example, as of
National Health Expenditure data). In addition, the FMAP 2018, 41 states reported having a HCBS waiting list.14
for the territories would be permanently increased to 83
percent. The most recent federal funding increase for the The Build Back Better Act would provide states the option
territories temporarily raised the FMAP for Puerto Rico to 76 of permanently receiving a six-percentage point increase
percent and the FMAP for the other territories to 83 percent. in their Medicaid matching rate for home- and community-
Unlike for the other territories, for which the 83 percent based services furnished to Medicaid beneficiaries with
FMAP would take effect in fiscal year 2022, Puerto Rico’s LTSS needs if they improve and expand HCBS services and
matching rate would remain at 76 percent for one year and access. (This provision builds on an American Rescue Plan
then rise to 83 percent in 2023. Act provision offering states a one-year FMAP increase of 10
percentage points for HCBS improvements and expansions.)
The Build Back Better Act would also require Puerto Rico to The federal funding caps for the territories would not apply
maintain physician reimbursement rates at certain minimum to this HCBS matching rate increase.
levels.12 Otherwise Puerto Rico would see its FMAP reduced
November 2021 CCF.GEORGETOWN.EDU BUILD BACK BETTER 7HCBS services eligible for the matching rate increase new mandatory HCBS quality measures (which would be
include home health, private duty nursing, personal care, added to the Medicaid child and adult core sets of quality
HCBS services provided through several types of Medicaid measures). The bill would thus significantly improve HCBS
waivers, case management, rehabilitative services (including services over time, including for children with special health
behavioral health), services provided through PACE care needs.
programs (Programs of All-Inclusive Care for the Elderly),
and other services specified by the Secretary of Health Permanent Extension of Spousal Impoverishment
and Human Services. States would be required to use the
Protections for Individuals Receiving Home and
increased federal funding to supplement, not supplant their
Community-Based Services
current level of HCBS spending and maintain their existing
HCBS eligibility, benefits and provider reimbursement rates Under Medicaid’s spousal impoverishment rules, a portion of
so they are not more restrictive than what was in place as a married couple’s combined resources is protected for the
of the date when states received planning grants (which is spouse living in the community when determining financial
discussed below). They must also implement a federally eligibility for an individual seeking long term care. Section
approved plan to expand access including reducing wait 2404 of the Affordable Care Act (ACA) expanded these
lists, expanding eligibility, lowering disparities in using protections beyond institutional care to also require states to
HCBS and newly covering personal care; strengthen the apply the protections to community spouses of individuals
HCBS workforce including adopting processes to ensure receiving Medicaid home and community-based services.
that HCBS payment rates are sufficient and updating However, due to the temporary nature of the provision,
qualification standards’ and increase HCBS payment rates Congress has had to act multiple times to extend spousal
to support recruitment and retention of the direct care impoverishment protections for individuals receiving home
workforce and raise payment rates to direct care workers. and community-based services including most recently in
States would no longer be eligible for the FMAP increase if 2021, which extended the protections through September
they are out-of-compliance with these requirements or, after 30, 2023. The Build Back Better Act would finally extend the
7 years, they fail to demonstrate that they have increased ACA spousal impoverishment protections on a permanent
HCBS availability and that at least half of their total LTSS basis.
spending is for HCBS (or if the percentage was higher before
the improvement plan was approved, no less than such Permanent Extension of the Medicaid Money Follows
percentage). the Person Demonstration
States would also receive $130 million in federal funding for The Medicaid Money Follows the Person (MFP)
planning grants to develop their HCBS improvement plans. demonstration is a federal grant program that provides
States would not be able to receive the FMAP increase for states with enhanced federal matching funds to help
HCBS (discussed above) until they have been awarded transition individuals receiving long term services and
a planning grant and their improvement plan has been supports from institutional settings to community-based
approved by the federal government. They would also be settings. The program was first authorized 2005 under
eligible to receive an additional two percentage point FMAP the Deficit Reduction Act and has subsequently been
increase for six fiscal year quarters if they facilitate the use amended and extended a number of times. As of 2019, 44
of self-directed care by Medicaid beneficiaries with LTSS states participated in the MFP demonstration.15 Funding
needs. States would also receive a higher administrative for the program currently extends through September
matching rate of 80 percent (instead of the regular 50 30, 2023. The Build Back Better bill would permanently
percent administrative matching rate) for costs related to extend funding for the Medicaid Money Follows the Person
implementing HCBS improvements for the next 10 years. demonstration at current funding levels of $450 million per
Finally, state would also receive a permanent administrative year. It would also modify program rules to require a state
matching rate of 80 percent for costs related to reporting to use demonstration grant funds within four years of receipt
8 BUILD BACK BETTER CCF.GEORGETOWN.EDU November 2021or have any unused portion of the funds rescinded by the law, the new state plan option is available starting April 1,
Secretary. Any such rescissions would then be added to the 2022 but is only available for a five-year period. The Build
mandatory program appropriation for the following year. Back Better Act would permanently extend the state option,
removing the five-year sunset. The 85 percent enhanced
matching rate would continue to remain available for the first
Behavioral Health
three years that a state takes up the option.
Expansion of the Medicaid Certified Community
Behavioral Health Clinic Demonstration Program Criminal Justice Reform
The Protecting Access to Medicare Act (PAMA) of 2014
Improved Continuity of Care and Health Care Access
created the Medicaid Certified Community Behavioral Health
Clinic (CCBHC) demonstration program (also referred to
for People Involved in the Criminal Justice System
as the Community Mental Health Services Demonstration The Build Back Better Act would permanently require
Program) under which the Secretary of Health and Human state Medicaid and CHIP programs to cover incarcerated
Services was authorized to award planning grants to individuals, who are otherwise eligible, 30 days before
states and provide states selected to participate in the their release from jail or prison. (In Medicaid, it would do
demonstration with enhanced federal matching funds so by modifying an existing limitation that generally bars
(equal to the CHIP matching rate) for services provided federal Medicaid funding for incarcerated individuals,
to Medicaid beneficiaries at certified behavioral health although federal Medicaid matching funds are already
clinics. The demonstration was initially limited to 8 states available for certain outside hospital inpatient services.) This
for a length of two years but Congress has subsequently would ensure better care transitions and improved health
expanded and extended the CCBHC demonstration. outcomes, including for those with behavioral health issues,
Today, the demonstration is limited to 10 participating substance use disorders and complex, chronic conditions,
states with the states able to receive the enhanced FMAP as they reenter their communities.16 The provision would
for CCBHC services through September 30, 2023. The take effect on the first day of the first fiscal year calendar
Build Back Better Act would expand access to the CCBHC quarter that begins two years after date of enactment, which
demonstration to all states by authorizing the Secretary would be as soon as January 1, 2024.
to award additional planning grants to interested states,
and allowing any state that meets the requirements of the
Indian and Native Hawaiian Health
demonstration program to participate for a two year period.
The territories would also be allowed to participate if they
Increased Federal Support for Certain Indian Health
meet the demonstration requirements and any amounts
and Native Hawaiian Health Providers
attributable to the increased matching rate under the
demonstration would not be subject to their block grants. The American Rescue Plan Act temporarily applied for two
years the 100 percent FMAP available to Indian Health
Service (IHS) providers for furnishing care to Medicaid
Permanent Extension of State Option to Provide
beneficiaries to services furnished by Urban Indian Health
Qualifying Community-Based Mobile Crisis
Programs. Such providers are grantees of the IHS and
Intervention Services
serve IHS-eligible patients on Medicaid, but they are not
Under the American Rescue Plan Act, Congress created formally part of the IHS and as a result, payments to these
a new option for states to provide qualifying community- providers do not otherwise receive the 100 percent FMAP
based mobile crisis intervention services to individuals that other IHS providers do. The American Rescue Plan Act
experiencing mental health or substance use disorder crises also provided for two years 100 percent FMAP for services
and receive an enhanced 85 percent federal matching rate furnished by Native Hawaiian Health Centers and other
for such services for the first three years. Under current qualified entities. The American Rescue Plan Act provision
November 2021 CCF.GEORGETOWN.EDU BUILD BACK BETTER 9became effective April 1, 2021. The Build Back Better Act Improvements to Accuracy of Medicaid Drug Pricing
would further extend this enhanced funding for both groups Survey of Pharmacies
of providers an additional two years through March 31, 2025.
State Medicaid programs are required to base their
pharmacy reimbursement rates on the actual acquisition
Medicaid and CHIP Drug Pricing, costs of pharmacies in obtaining the drugs they dispense
Prescription Drug and Vaccine Coverage to Medicaid beneficiaries. In order to determine actual
acquisition costs, states are permitted to rely on the
Extension of Medicaid Drug Rebate Program to National Average Drug Acquisition Cost (NADAC) survey
Separate State CHIP Programs of pharmacies conducted by CMS. But pharmacies are
not required to respond to this monthly survey. The Build
Under the highly effective Medicaid Drug Rebate Program,
Back Better bill would require pharmacies to respond to
drug manufacturers are required to pay substantial
the survey (as well as make improvements to the survey
rebates to state Medicaid programs.17 According to the
itself), which should improve the accuracy of the survey and
Congressional Budget Office, because of the success of
better ensure that states’ pharmacy reimbursement rates
the Medicaid rebate program, Medicaid obtains the lowest
are more in line with pharmacies’ actual costs. That, in turn,
prices, net of rebates and discounts, compared to other
should produce both federal and state savings over time.
federal programs and agencies including the Department of
This provision is effective the start of the first calendar year
Veterans Affairs.18
quarter that begins 18 months after the date of enactment.
The Medicaid Drug Rebate Program, however, does not
apply to separate state CHIP programs. (Under CHIP, states Permanent Prohibition Against Implementation of
can use federal CHIP funds to expand Medicaid, establish a Rebate Rule
separate program, or use a combination of the two. CHIP-
The Build Back Better would permanently block
funded Medicaid expansions are subject to the Medicaid
implementation of the rule, finalized by the Trump
rebate program.) It is likely that separate state CHIP
Administration in November 2020, to eliminate the
programs obtain far smaller rebates from manufacturers than
safe harbor in the federal anti-kickback law for rebates
what manufacturers now pay under the Medicaid rebate
negotiated by pharmacy benefit managers (PBMs) on
program, largely due to their small size.
behalf of Medicare Part D plans. (Court orders blocked
Starting January 1, 2024, the Build Back Better bill would implementation until January 2023 and the bipartisan
apply the Medicaid rebate program to all separate state infrastructure law — H.R. 3684 — further blocks
CHIP programs. This would likely result in state CHIP implementation for another three years.)
programs receiving much larger rebates than they (or
While much of the attention on the rebate rule has
their CHIP managed care plans) receive today, with the
focused on how it would significantly increase federal
federal government and states sharing in these savings.
Medicare spending and Medicare beneficiary premiums,
Importantly, this provision would also apply the rebate
the rule would also increase federal and state Medicaid
program’s open formulary requirement to separate state
costs. Based on an earlier Congressional Budget Office
CHIP programs, under which Medicaid must cover nearly
analysis, the rule, if implemented, would likely increase
all FDA-approved drugs. While all separate state CHIP
federal Medicaid spending by $6 billion over 10 years and
programs cover prescription drugs, most have more
state spending by nearly $3 billion. That is because if
restrictive drug formularies than what is provided in
implemented, the rule would effectively replace the current
Medicaid. As a result, this provision would likely increase
rebates that drug manufacturers provide in Medicare Part D
CHIP beneficiary access — both for children and pregnant
plans with so-called “chargeback” discounts. That would
women who are enrolled in CHIP — to needed prescription
reduce the mandatory rebates that drug manufacturers must
drugs.
provide to Medicaid under the Medicaid rebate program
10 BUILD BACK BETTER CCF.GEORGETOWN.EDU November 2021because such chargebacks in Part D would likely have the Back Better bill would make vaccines for adults, as well as
effect of lowering the Average Manufacturer Price (AMP) their administration, a mandatory Medicaid benefit. Adult
of drugs, which helps determine the amount of mandatory vaccines would also be exempt from cost-sharing for all
Medicaid rebates. That, in turn, would raise the net cost Medicaid beneficiaries in order to ensure parity across the
of prescription drugs for the federal government and the program. (Vaccines are already mandatory and exempt
states.19 As a result, this provision blocking implementation from cost-sharing for children in Medicaid.) It would also
of the safe harbor rebate rule would protect state Medicaid make adult vaccines and their administration, without cost-
programs from higher drug costs over time. sharing, mandatory for CHIP (for anyone who is aged 19 or
older). The effective date would be the start of the first fiscal
Requirement for Medicaid and CHIP to Cover year quarter than begins 1 year after date of enactment,
which would be early as January 1, 2023. However, states
Vaccines for Adults
that provide Medicaid coverage of adult vaccines without
Medicaid requires coverage of vaccines (as recommended cost-sharing as of the date of enactment would receive a
by the Advisory Committee on Immunization Practices) one percentage point FMAP increase related to vaccines
without cost-sharing for some adults, such as those covered and their administration for two years.
under alternative benefit plans, but not others. The Build
Private Health Insurance Provisions in the Build Back
Better Act
The Build Back Better Act includes a number of policies to Marketplace Subsidies to Address the Coverage Gap
build on and improve the Affordable Care Act, including: in Non-Expansion States
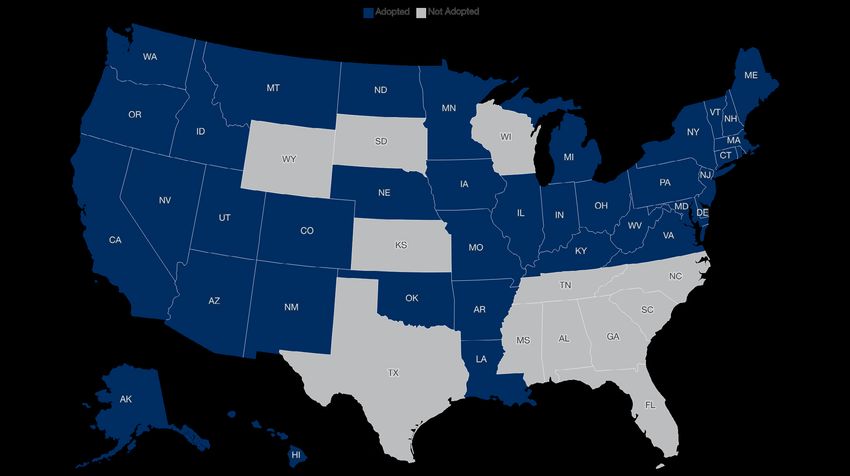
z Closing the Medicaid “coverage gap”: marketplace There are currently 12 states that have still not adopted
subsidies and additional benefits for people with the Affordable Care Act’s Medicaid expansion: Alabama,
incomes under 138 percent of the federal poverty line Florida, Georgia, Kansas, Mississippi, North Carolina, South
in non-expansion states Carolina, South Dakota, Tennessee, Texas, Wisconsin and
Wyoming. See Figure 1. According to the Kaiser Family
z Enhanced premium tax credits at all income levels
Foundation (KFF), if all of these states expanded Medicaid,
z Extra financial assistance for people who experience
about four million uninsured adults would become newly
unemployment
eligible. Of those, 2.2 million low-income people in poverty
z Tax relief for low-income individuals who receive are stuck in the “coverage gap” with incomes too low to be
premium tax credits eligible for marketplace subsidies but who are ineligible for
z Improved access to marketplace subsidies for those Medicaid.20
with unaffordable employer-based insurance
The Build Back Better bill would temporarily enable these
z Expanded consumer assistance
individuals to qualify for premium tax credits to purchase a
z Cost-sharing help for insulin products $0 premium benchmark plan on the marketplaces beginning
z A state-level grant program to improve insurance in 2022 (but only through 2025). These plans would be
affordability required to cover 94 percent of an average person’s health
care costs. In 2023, the plans’ generosity would increase to
These changes are designed to increase access to 99 percent. Beginning in 2024, these plans will be required
affordable private health plans through the Affordable to cover non-emergency transportation and certain family
Care Act’s marketplaces. Most of the changes, however, planning services not typically covered in commercial health
would only be temporary and end in 2025, barring further insurance but covered in Medicaid.
congressional action.
November 2021 CCF.GEORGETOWN.EDU BUILD BACK BETTER 11Figure 1. Status of Medicaid Expansion by State
Individuals with incomes under 138 percent of the federal To further encourage states to take up the Medicaid
poverty line who do not qualify for Medicaid would expansion, the Build Back Better bill would temporarily
have a continuous, year-round opportunity to enroll in a increase the expansion FMAP from 90 percent to 93
marketplace plan, unlike other applicants who generally percent for three years (2023-2025), which would create
must have a qualifying event outside of open enrollment.21 an additional incentive for states to take up the Medicaid
They would also not be disqualified from premium tax credits expansion. This would also have the effect of encouraging
if they have an offer of employer coverage; for most of these states that have already adopted the Medicaid expansion to
individuals, the marketplace plan will be a better value. To maintain it, despite the temporary availability of this fallback
help raise awareness of these new coverage options, the provision extending marketplace subsidies to those with
bill would devote $105 million in funding for culturally and incomes below 138 percent of the federal poverty line not
linguistically appropriate outreach and marketing. And eligible for Medicaid.
the U.S. Health & Human Services Department (HHS)
In addition, the substantial financial incentives for the twelve
would be required to spend at least $10 million in 2022 to
non-expansion states to adopt the Medicaid expansion
support Navigators in these 12 states to assist people with
provided through the American Rescue Plan remains in
enrollment, increasing to $20 million each year for 2023,
effect.22 Under that permanent provision, states that newly
2024, and 2025. Additionally, because participating insurers
expand Medicaid receive an additional five percentage point
were not able to set their 2022 premiums to account for
increase in their regular FMAP for two years, no matter
these new enrollees, the bill would create a temporary
when they newly expand. (This increase does not affect
reinsurance program to provide a financial cushion if they
the expansion itself but applies to the rest of the Medicaid
experience excessive claims costs.
program covering children, some parents, people with
12 BUILD BACK BETTER CCF.GEORGETOWN.EDU November 2021disabilities and seniors.) KFF has previously estimated that Extension of American Rescue Plan Premium Tax
the FMAP increase in the American Rescue Plan is expected Credit Enhancements
to more than offset expansion costs in all of the non-
The Affordable Care Act provides advance premium tax
expansion states in a two-year period, assuming expansions
credits (PTCs) to qualified individuals and families that enroll
are implemented in 2022.23 And as described above, the
in coverage through the health insurance marketplaces.
Build Back Better Act would increase the expansion FMAP
Until enactment of the American Rescue Plan, these PTCs
from 90 percent to 93 percent for three years, which would
were available only to people with modified adjusted gross
further increase the fiscal benefit to states if states take up
income between 100 and 400 percent of the federal poverty
the expansion before the end of calendar year 2025.
line (between $26,200 and $104,800 for a family of four),
Finally, the Build Back Better Act would establish some who are lawfully present in the U.S. and do not qualify for
disincentives for states that continue to refuse the other affordable minimum coverage such as Medicaid,
expansion. This includes, starting in fiscal year 2023, Medicare, or an employer plan. The ACA’s tax credits
scaling back certain Medicaid waivers that provide funding effectively cap an individual or family’s premium contribution
to providers for uncompensated care. States with such at a percentage of their income. That specified percentage
Section 1115 waivers are Florida, Kansas, Tennessee and varies, with lower-income families required to pay the lowest
Texas. Specifically, federal funding under such waivers percent of income towards premiums. The ACA required
would no longer be available for uncompensated care these percentages to be adjusted annually for inflation.
related to individuals who would be otherwise eligible under
The American Rescue Plan Act increased the PTCs available
the Medicaid expansion (if a state had expanded). The
for marketplace enrollees by reducing the percentage of
bill would also reduce the size of states’ federal Medicaid
income that individuals and families contribute towards
Disproportionate Share Hospital (DSH) allotments, starting
premiums for plan years 2021 and 2022. Under the
in fiscal year 2023, if states do not fully cover expansion
enhanced premium schedule, families with incomes between
individuals. Specifically, the DSH allotment a non-expansion
100 and 150 percent of the federal poverty line had their
state would otherwise receive would be reduced by 12.5
premium contribution reduced to $0. Families with incomes
percent.
over 400 percent of the federal poverty line became
eligible for subsidies for the first time, with their premium
contribution capped at 8.5 percent of family income. See
Table 3.
Table 3. Maximum Income Contribution Percentage by Household Income
under the Affordable Care Act and the American Rescue Plan Act
Range of Maximum Income Distribution
(Percent of Income)
Income Range
(Percent of Federal Under Affordable Care Act Under Affordable Care Act Under American Rescue Plan
Poverty Level)
(2014, original schedule) (2021, after annual inflation
adjustments)
100-133 2.0 2.07 0
133-150 3.0-4.0 3.10-4.14 0
150-200 4.0-6.3 4.14.6.52 0-2.0
200-250 6.3-8.05 6.52-8.33 2.0-4.0
250-300 8.05-9.5 8.33-9.83 4.0-6.0
300-400 9.5 9.83 6.0-8.5
400+ – – 8.5
November 2021 CCF.GEORGETOWN.EDU BUILD BACK BETTER 13Under the American Rescue Plan, marketplace enrollment is greater than what they projected, they could owe some
has increased dramatically and enrollees have seen or all of the excess premium tax credits back to the federal
significant reductions in premiums. Over 2.8 million people government, in a process called “reconciliation.”
enrolled in a marketplace health plan during the COVID-19
The Build Back Better Act recognizes that income often
special enrollment period that ended on August 15, 2021,
fluctuates for low-income families, placing them at
bringing total marketplace enrollment to its highest ever, at
heightened risk of owing the IRS excess premium tax credits
12.2 million people. On average, enrollees saved $67 per
at tax time. The bill would cap the amount that individuals
month, with close to half able to find a plan for less than $10
under 200 percent of the federal poverty line would have to
per month. Additionally, because many people were able
pay back during reconciliation at $300 for married couples
to take their additional tax credit and “buy up” to a more
filing jointly and $150 for single individuals. Individuals
generous plan, the average deductible for a marketplace
under 138 percent of the federal poverty line who are not
plan fell by 90 percent this year.24
otherwise required to file a tax return would be exempt from
The Build Back Better Act would extend the American repaying any excess premium tax credits, and they could not
Rescue Plan premium tax credit enhancements through be denied future premium tax credits if they fail to file a tax
plan year 2025 and would eliminate the annual inflation return and reconcile their past year’s premium tax credits.
adjustment through 2026.
Help for People with Expensive Employer-Based
Increased Subsidies for Those Experiencing Insurance
Unemployment Under the ACA, only those individuals who are not
The U.S. economy lost 22 million jobs between February eligible for “minimum essential coverage” may qualify
and April 2020.25 Many individuals lost their employer-based for marketplace premium tax credits. Minimum essential
health insurance at the same time. The American Rescue coverage includes employer-based insurance, so long as
Plan Act increased the amount of premium tax credits and that insurance is “affordable” and “adequate.” The IRS has
cost-sharing help for individuals who received, or were defined “affordable” employer-based insurance in 2021 to
approved to receive, at least one week of unemployment have a premium for a self-only policy that does not exceed
insurance benefits in 2021. These individuals qualify for a 9.83 percent of the family’s income.26 For 2022-2025,
benchmark Silver plan with a $0 premium, with cost-sharing the Build Back Better Act would lower that affordability
subsidies resulting in the plan paying 94 percent of the threshold to 8.5 percent of income, meaning that employees
cost of care for the average enrollee. This provision of the whose premium for their job-based insurance exceeds that
American Rescue Plan Act extends only through 2021; the amount could opt out and obtain a marketplace plan with
Build Back Better Act would provide similarly enhanced subsidies instead.
subsidies and cost-sharing help for these individuals through
the end of 2022. Expanded Consumer Assistance
Several states have established consumer assistance or
Tax Time Reconciliation Relief for Low-Income ombudsmen programs to help consumers with insurance
Families problems or complaints. Staff of these programs assist
Under the ACA, when an individual enrolls in a marketplace consumers with:
plan with a premium tax credit, the marketplace estimates
z Filing complaints and appeals with insurance
the amount of premium tax credit to allocate based on that
companies
individual’s projected income and household size for the
coming year. These premium tax credits are then advanced z Collecting, tracking, and quantifying consumers’
to the enrollee on a monthly basis. If the individual’s actual insurance problems
income for the year (as reported in their annual tax filing) z Educating consumers on their insurance rights and
14 BUILD BACK BETTER CCF.GEORGETOWN.EDU November 2021responsibilities sharing to the lesser of $35 or 25 percent of the negotiated
z Resolving problems with financial assistance price. Any cost-sharing the enrollee faces would have to be
programs.27 applied towards his or her annual out-of-pocket maximum.
The ACA provided grant funding to help support these The “Improve Health Care Affordability Fund”
consumer assistance programs, but the last federal grants The Build Back Better bill would establish a $30 billion fund
were issued in 2014. Many programs were forced to shut ($10 billion per year, for 2023-2025) to provide grants to
down; others continue to operate with only state or private states for either a reinsurance program or to reduce enrollee
support. The Build Back Better Act would provide $100 cost-sharing in marketplace health plans. Although the
million over four years ($25 million each year from 2022- grant funds would be made available in 2023, states would
2025) to support these programs. have just 120 days from the date of enactment to submit
applications to HHS. Once HHS has approved a state’s
Increased Subsidy Eligibility Through “MAGI” proposal, it will be deemed approved for each remaining
Adjustments year of the grant program as well (through 2025). States that
have yet to expand Medicaid would not be eligible to submit
Eligibility for marketplace premium tax credits and cost-
an application. HHS would instead run a default reinsurance
sharing subsidies is based on a household’s “modified
program in their state.
adjusted gross income,” or MAGI. MAGI includes multiple
possible sources of income, including wages, tips, capital
gains, investment income, and more. Lump-sum Social Funding for State Innovation
Security payments have also been considered part of MAGI. The ACA includes a provision enabling states to apply
However, these sometimes unexpected payments (such as to HHS to waive certain provisions of the law in order to
in the case of a death or retirement) can result in individuals implement state-based health reforms. These are often
facing reduced premium tax credits or a repayment to the referred to as “Section 1332 waivers.” Currently 17 states
IRS during reconciliation. have 1332 waivers in place, 15 of which are used to support
state-level reinsurance programs designed to moderate
The Build Back Better bill would exempt these lump sum
individual market premiums.29 The Build Back Better bill
Social Security payments from the MAGI calculation. It
would include $50 million in 2022 for grants to states to
also would allow individuals to discount income from a
develop and submit 1332 waiver applications, applications
dependent under the age of 24, so long as the aggregate
for extensions or amendments and to implement section
amount of dependent income in the household is less than
1332 waivers. Grants for an individual state are not to
$3,500, indexed for inflation. This latter provision, however,
exceed $5 million.
would only be available through 2026.
Pharmacy Benefit Manager Transparency
Reduced Cost-Sharing for Insulin
Starting with plan years beginning on or after January
Over 10 million Americans with diabetes depend on insulin
1, 2023, the Build Back Better bill would require health
to manage their condition. Since 2012, the price of many
insurance issuers, group health plans and pharmacy benefit
newer forms of insulin have risen on average 15 to 17
managers (PBMs) to report certain information to plan
percent per year, well above the rate of inflation. As many
sponsors (such as employers) related to prescription drug
as one in four people report rationing insulin to save money,
benefits and pricing. This would include information related
placing their health — and in some cases their lives — at
to why certain drugs received preferred formulary placement
risk.28 Beginning in 2025, employer plans and individual
and what rebates, fees, discounts or other remuneration
market insurers would be required to cover certain insulin
were paid by drug manufacturers for claims incurred or that
products and would be required to exempt them from
are related to utilization of drugs. In addition, starting with
enrollee deductibles. They would also have to limit cost-
November 2021 CCF.GEORGETOWN.EDU BUILD BACK BETTER 15plan years beginning on or after January 1, 2023, the bill Expansion of Health Coverage Tax Credit for Workers
would prohibit issuers, group health plans, and PBMs from Losing Jobs due to Trade
entering into contracts with manufacturers, distributors,
In 2002, Congress enacted legislation creating a tax credit
wholesalers and other third-party entities that limit the
to subsidize the health insurance premiums of workers
disclosure of the information required to be reported.
who either lost jobs due to international trade (i.e., when
This provision would increase drug benefit and pricing a manufacturer moves its operations overseas) or whose
transparency in group health plans and likely reduce the defined-benefit pension plans were taken over by the
prevalence of troubling practices by PBMs. In recent years, Pension Benefit Guaranty Corporation because of financial
for example, some PBMs have received increasing scrutiny difficulties. Under current law, the Health Coverage Tax
for failing to fully pass through rebates and other savings Credit (HCTC) covers 72.5 percent of the premium for
not only to patients at the pharmacy counter but also to qualifying health insurance (such as COBRA coverage or an
employers and other plan sponsors. And some PBMs have individual market health plan). The HCTC is slated to expire
placed certain drugs on preferred drug lists or formularies, on January 1, 2022. The Build Back Better Act would make
even though there are alternative drugs in the same the HCTC permanent and increase the amount of premium
therapeutic class that are less costly but are equally, or covered by the credit to 80 percent.
more, clinically effective. This was because those preferred
drugs gleaned greater rebates which then accrued, at least
in part, to the PBMs themselves, rather than to patients or
plan sponsors.
About the Authors
This brief was written by Edwin Park, Anne Dwyer, and Maggie Clark of the Georgetown University Center for
Children and Families and Sabrina Corlette of the Georgetown University Center for Health Insurance Reforms. The
authors would like to thank Joan Alker, Tricia Brooks, and Cathy Hope for their contributions to the report. Design
and layout provided by Oyinade Koyi.
The Georgetown University Center for Children and Families (CCF) is a nonpartisan policy and research center
founded in 2005 with a mission to expand and improve high-quality, affordable health coverage for America’s
children and families. The Georgetown University Center on Health Insurance Reforms (CHIR) is a team of nationally
recognized experts on private health insurance and health reform, with a mission to improve access to affordable
and adequate health insurance by providing balanced, evidence-based research, analysis, and strategic advice.
Both are based in the McCourt School of Public Policy’s Health Policy Institute.
16 BUILD BACK BETTER CCF.GEORGETOWN.EDU November 2021You can also read