Body Mass Index Correlates with Body Fat Percentage in Children and Adolescents in the Democratic Republic of the Congo: A cross sectional study
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Body Mass Index Correlates with Body Fat Percentage
in Children and Adolescents in the Democratic
Republic of the Congo: A cross sectional study
Guy Ikambo Wanghi1*, Leslie Lytle2, Augustin Rudahaba Buhendwa3 and Ernest Kiswaya Sumaili1, 4
1. Department of Basic Sciences, Unit of Physiology, Faculty of Medicine, University of
Kinshasa, Kinshasa, RD Congo.
2. Department of Health Behavior, Gillings School of Global Public Health University of
North Carolina at Chapel Hill, Chapel Hill, NC, USA.
3. Department of Physical Medicine and Rehabilitation, Faculty of Medicine, University of
Kinshasa, Kinshasa, RD Congo
4. Renal Unit, Department of Internal Medicine, University of Kinshasa Faculty of Medicine,
Kinshasa, RD Congo
*Corresponding author: Guy Ikambo Wanghi, Department of Basic Sciences, Unit of Physiology,
Faculty of Medicine, University of Kinshasa, Kinshasa, RD Congo. Email: guy.wanghi@unikin.ac.cd.
Summary
INTRODUCTION
Paediatric obesity is a worldwide health challenge and parameters to
evaluate population obesity risk are needed. The purpose of this study is to report
on anthropometric measures for assessing obesity risk for children in sub-
Saharan Africa and to confirm that measuring height and weight to calculate
BMI can be used as a good indicator of obesity risk.
MATERIALS AND METHODS
This was a cross-sectional study of a sample of 1,442 students aged 6 to 18
years enrolled in schools in the city of Kinshasa, the capital of the Democratic
Republic of Congo. These school children were selected using a multistage
sampling method. BMI for-age-sex was calculated using WHO AnthroPlus and
expressed in Z‑scores. Skinfolds were used to calculate percent body fat (%BF).
Data were analyzed using SPSS version 21.
RESULTS
This study showed that the percentage body fat (BF) was higher in girls
than in boys (20.5 ± 9.6 vs 12.4 ± 6.3 p< 0.001). The BMI for girls was higher
compared to boys (18.5 ± 3.7 vs 17.3 ± 3.0 pKeywords: Body Composition, percentage of body fat, Overweight, Obesity, Adolescents, Children
[Afr. J. Health Sci. 2021 34(1):2-11]
associated with level of adiposity but getting
Introduction an accurate measure of fat is very challenging
Childhood and adolescent overweight
[12]. Direct and highly accurate measurement
and obesity is a major public health problem in
of body fat or adiposity requires sophisticated
the developed world [1]. Those conditions
equipment such as a Dexa scan using dual-
have also significantly increased in low and
energy X-ray absorptiometry. Other tools such
middle income countries (LMIc) in the past
as bio-electrical impedance, the use of skin
decades. Overweight and obesity in children
calipers, and body circumference measures are
and adolescents in LMIc now co-exist with
also used to assess adiposity. But these tools
underweight, as a result of nutrition transition
are difficult to use in epidemiological surveys
[2-5].
due to the cost of equipment, the time required,
In sub-Saharan Africa, the prevalence
or the challenging measurement protocols [5,
of overweight and obese children and
13]. To fill this gap, WHO recommends Body
adolescents varies from 5 to 17 % and 1 to 5%,
Mass Index (BMI) as the most useful
respectively [6-7]. Several reports have shown
population level measure of underweight,
that overweight and obesity are now increasing
overweight and obesity. BMI is also the
in low and middle-income populations
surrogate measure for prediction of percentage
(including in Africa), especially in urban areas.
of body fat (% BF) [14].
From 1990 to 2010, the growth rate of
Several studies have shown a
overweight and obesity doubled, indicating
relationship between BMI and percentage body
that Africa has the fastest growth rates of
fat (BF) [15-17] but such studies have rarely
overweight and obesity [8-9] and is expected
been performed in sub-Saharan Africa.
to reach 11% in 2025 [8].
The objective of our study was to
Childhood and adolescence are
report on assessment of body fat and height
important periods of life, as many
and weight for children in the Democratic
physiological and psychological
Republic of the Congo (DRC) and to confirm
transformations take place at these ages.
that measuring height and weight to calculate
Moreover, healthy and unhealthy lifestyles and
BMI can serve as a good indicator of risk for
behaviors are established during these years,
obesity. Comparisons were made between BMI
which can influence the behavior and health
and skinfold thickness, a criterion measure of
status of adults [10-11]. Therefore, it is vitally
adiposity. In addition, percentage body fat was
important to understand the trends in the
compared among boys and girls and by age
development of body weight disorders in
groups. The results of this present work can
young people and their negative effects on
provide a baseline for adiposity in youth in
overall health [5].
Sub-Saharan Africa. In addition, it can help
To evaluate population trends, tools to
encourage health practitioners in clinics to use
assess weight-related risk need to be simple,
the simple measure of BMI to assess the risk of
cost effective and feasible to use across a wide
obesity in their patients and to provide public
variety of settings.
health officials with a good surveillance tool
Overweight and obesity are defined as
for obesity risk in youth.
abnormal or excessive fat accumulation that
may impair health [5]. Chronic disease risk is
African Journal of Health Sciences Volume 34, Issue No. 1, January - February, 2021 3Materials and Methods Anthropometric
Study Sample and Design Measurement
This was a cross-sectional study To measure height, weight and
enrolling 6–18-year-old students living in percentage BF, we used the World Health
Kinshasa, the capital of DRC. The sample was Organization and the International Society for
selected using multistage sampling method the Advancement of Kinanthropometry
from November 15th, 2018 to June 20th, 2019. guidelines [18]. Height was measured in the
A total of 568 eligible primary and secondary sagittal plane with a portable SECA 214
schools were grouped according to their anthropometer (Seca®, Hamburg, Germany) to
location into three strata which correspond to the nearest 0.1 cm. The subjects’ height was
the existing three educational provinces in measured with each subject standing upright,
Kinshasa. The schools in each stratum were the head in Frankfort plane, without shoes,
further stratified into primary and secondary. with both feet flat on the platform and apposed
The name of each school was written at the medial malleoli; the heels, buttocks, and
on a piece of paper, wrapped, and put into the occiput placed against the scale with arms
corresponding ballot bags representing its hanging freely by the sides. The instrument
stratum. A total of 18 schools, one school from was checked before each measurement
each of the 3 strata, were selected by a simple ensuring that both headboard and footboard
random method. Within each selected school, were at 90° to the vertical rule.
classrooms were selected to participate and all Weight was measured in kilograms
students in selected classes were offered the (kg) with an OMRON body composition BF
opportunity to participate. 511 balance (OMRON Healthcare Europe BV,
To be eligible, participant were to Hoofddord, the Netherlands) to the nearest 0.1
meet the following selection criteria: kg. The students stood on the scale without
Congolese citizen, consent of parents or tutors shoes wearing light cotton material. The scale
and age between 6 and 18 years old. School automatically adjusted to zero before each
record of birth certificate of each enrolled child measurement. It was also checked daily using
was used to establish age. Students with an object of known weight as a quality control
disabilities and pregnant girls were excluded. measure to ensure validity and reliability.
Body mass index (BMI) was
Ethical Consideration calculated as weight in kilograms divided by
To conduct this study, ethical approval
height in meters squared (kg/m2) [19].BMI‑for
was obtained from the Ethical Review
Committee of the Ministry of Health (Ref ‑age indices were calculated with WHO
N°.143/CNES/BN/PMMF/2018). Written AnthroPlus® (v1.0.4, World Health
Permission was obtained from Minister of Organization, Geneva 2009) [20] and
Education (the Ministry of primary and expressed in Z‑scores.
secondary schools), as well from each Skinfolds in the biceps, triceps,
participating school and from all classroom suprailiac, subscapularis and abdominal
teachers. Parents or tutors were informed of regions were taken on the right side of the
the study prior to the survey date. The parents body with Harpenden skinfold caliper (Holtain
were consented for this intervention and the Limoted, U.K) with a constant pressure of
youth gave their assent. 10g/mm2 to the nearest 0.2 mm [21].
African Journal of Health Sciences Volume 34, Issue No. 1, January - February, 2021 4Index-for-age-sex was calculated using WHO
Operational Definitions Anthro plus software V.1.0.4. All data
Using BMI, the children were
analyses were performed with Statistical
classified into the following categories:
Package for the Social Sciences (SPSS),
underweight: thin: +2), and “normal weight” (BMI‑for‑age Z‑ body composition variables were computed.
score − 2 to + 1). The values were set from the After the computation of the descriptive
median values of the WHO international analyses, independent t-test was calculated to
growth reference 2007 for 5–19‑year‑old test differences of means with respect to
children [19-20]. statistical significance. The statistical level was
Percentage body fat (% BF) was based set at p-value ≤ 0.05.
on the sum of triceps and calf skinfolds derived
from skinfolds using the equation developed
Results
A total of 1,442 pupils (668 females
by Slaughter et al. (1988) [5] which is
and 774 males) participated in the study. Table
internationally accepted for use in children and
1 shows the descriptive statistics of the sample.
adolescents from different ethnic groups. All
There were slightly more boys represented in
anthropometric measurements were taken
the total sample than girls and the sample of
twice by Level 2 ISAK-certified
boys was significantly older than the sample of
anthropometrics’ and the average scores of the
girls. Girls were shorter than boys and girls
two measurements. The values were set from
were significantly heavier, had significantly
the median values of the WHO international
higher mean BMI and had higher body fat as
growth reference 2007 for 5–19‑year‑old
measured by skinfold thickness as compared to
children [19-20]. boys. In the group of younger children, the
Percentage body fat was compared differences between girls and boys were only
with BMI according to Lohman et al. (2000) statistically significant for the percentage of
[5] across six categories, as the following: very body fat and skin folds with girls having
low 7 - 11, low 12 - 14, optimal range 15 - 18, significantly higher values than boys (p <
moderate high 19 - 25, high 26 - 32, and very 0.001).
high 32 and above. When comparing older children by
Statistical Analysis gender, weight, BMI, percentage of body fat
Underweight, overweight and obesity and skin folds were higher in girls than in boys
were defined based on the Body Mass Index (p < 0.001). Boys were, on average, taller than
(BMI) for age-sex of the children. Body Mass girls (p < 0.05).
African Journal of Health Sciences Volume 34, Issue No. 1, January - February, 2021 5Table 1: Characteristics of Study Population by Age Groups
All Age 6-9 years Age 10-18 years
Variables Girl Boy P- Girl Boy P- Girl Boy p-
(n=668 (n=774) value (n=21 (n=196) value (n=451) (n=578) Value
) 7)
Age 11.8±3. 12.2±3. 0.012 7.6 7.7 ±1.0 0.481 13.7 13.7 0.978
(years) 5 4 ±1.1 ±2.5 ±2.4
Height 1.47±0. 1.51±0.Table 2: Categories of Percentage BF by Sex and Age Group
All Age 6-9 years Age 10-18 years
Category Girl Boy P Girl Boy P Girl Boy p-
of body (n=668) (n=774) (n=217) (n=196) (n=451) (n=578) Value
fat
Very low 83 (12.4) 45560
50
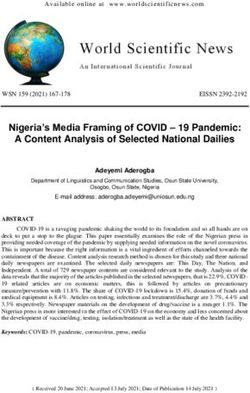
Body Fat (%) 40
30
20
10
0
10 15 20 25 30 35
BMI (Kg/m2)
boy girl
Figure 1: Scatter Plot of the Relationship between Body Mass Index (BMI) and Percentage of
Body Fat (%BF) of School-Aged Girls and Boys in Kinshasa.
Figure 1 shows the positive communicable diseases is roughly equivalent
relationships between percentage BF and BMI to measuring percentage body fat through skin
by sex. In addition, this relationship appears to folds. These results are consistent with those
be linear in nature. This relationship between reported in other studies outside of Africa [15-
BMI and percentage BF was independent at 17]. However, while the technique for
age and increased with BMI. In this sample of measuring skin folds is inexpensive, easy, and
youth from DRC, BMI appears to be a good reproducible for an experienced technician, it
proxy for adiposity. is not very accurate and is subject to inter
observer error [13].
Discussion The results of this study also showed
Our study sample composed of school-
that in the younger age group (6 - 9 years),
aged children and adolescents (6-18 years) in
BMI was non-significantly different between
the city province of Kinshasa tested the
the two sexes, while percentage BF was
hypothesis that body mass index correlates
significantly different between girls and boys.
with body fat percentage in children and
However, for the oldest age group (10-18
adolescents in Sub-Saharan Africa. The results
years), the differences between BMI and the
of this work, shown in figure 1 proved this
percentage BF were statistically significant
hypothesis. Indeed, in the figure 1, BMI places
between the two sexes.
youth in the same category of being at risk for
These large differences in body fat
fatness as does the data that more directly
were also observed in table 2 specifically in the
measure fatness.
younger and older age groups where optimal
The age and sex risk models for
and moderately high body fat was higher in
obesity-related diseases are similar when we
girls than in boys. Some authors explain that
use a body fat assessment which is a more
for the same body mass index (BMI), women
difficult assessment task and requires large
have ~10% more body fat than men [21, 23].
screening and intervention efforts compared to
Striking gender differences appear during
a BMI assessment which is much easier to
puberty: the increase in body weight in boys is
measure height and weight in large screening
mainly due to increases in lean body mass
and intervention efforts. It is clear that these
while in girls due to increased fat mass; typical
results have shown that measuring BMI to
android and gynoid fat distributions also
change obesity and the risk of chronic non-
African Journal of Health Sciences Volume 34, Issue No. 1, January - February, 2021 8appear for the first time during this period [23 to be a simple and easy measure that clinicians
– 26]. Two studies in black Africa, mainly in can use to analyze the risk of obesity and
Zimbabwe and Kenya, have shown that girls chronic non-communicable diseases in
have high percentage BF values compared to children and adolescents in sub-Saharan Africa
boys. Michelin et al in their study found that and particularly in DR Congo.
there are typical gender differences in body fat
composition for both younger and older
Conflict of Interest
All authors declared no competing
adolescents [27-28].
interests.
We also found large differences in
very low body fat in boys, especially in the Author Contributions
older age group (58 % boys vs. 6 % girls). This GIW and ESK were involved in the
could be due to a combination of adverse conception, design, data analysis and
environmental constraints to good growth interpretation of the study. GIW collected in
amplified in boys such as under-nutrition, high addition data. LL contributed to interpretation.
burden of infectious or parasitic diseases, poor ESK and ARB contributed to data analysis and
living conditions including housing, economic interpretation. All authors were involved in the
insecurity, food crisis and lack of sanitary or writing of the manuscript and provided final
educational facilities [29]. However, the approval.
difference between girls and boys in the very
References
low-fat category for the total sample (12.4 %
1. Ji CY, Cheng TO: Prevalence and
of girls versus 58.8 % of boys) is more
geographic distribution of childhood
explained by differences observed in the older obesity in China in 2005. Int J Cardiol
age group (6.0 % of girls versus 58.0 % of 2008, 131 (1):1-8.
boys). The gender difference is slightly smaller 2. Reddy SP, Resnicow K, James S,
in the younger age group (25.8 % versus 61.2 Kambaran N, Omardien R, Mbewu AD:
%). Underweight, overweight and obesity
Strength and Limitations of among South African adolescents: results
of the 2002 National Youth Risk
Study Behaviour Survey. Public Health Nutr
The strengths of our study are the 2009, 12 (2):203-207.
relatively large sample size, the quality of the 3. Hands B, Larkin D, Parker H, Straker
anthropometric measurements, and the fact that L, Perry M: The relationship among
all social categories were present in the physical activity, motor competence and
sample. The cross-sectional nature of the study health-related fitness in 14-year-old
could be seen as a limitation and skinfold adolescents. Scand J Med Sci Sports 2009,
measures used as the criterion measure of 19 (5):655-663.
adiposity while DEXA or bioelectrical 4. Garcia-Hermoso A, Correa-Bautista JE,
impedance may be the more rigorous measures Olloquequi J, Ramirez-Velez R: Health-
of adiposity. related physical fitness and weight status
in 13- to 15-year-old Latino adolescents. A
Conclusion pooled analysis. J Pediatr (Rio J) 2019, 95
Our study showed a correlation (4):435-442.
between BMI and percentage BF in children 5. Monyeki MA, Neetens R, Moss SJ,
and adolescents in sub-Saharan Africa. Given Twisk J: The relationship between body
the difficulties of measuring skin folds and composition and physical fitness in 14 year
training experienced technicians, BMI appears old adolescents residing within the Tlokwe
African Journal of Health Sciences Volume 34, Issue No. 1, January - February, 2021 9local municipality, South Africa: the Sectional Cohort Study. Diabetes Metab
PAHL study. BMC Public Health 2012, Syndr Obes, 13:1587-1597.
12:374. 13. Mechanick JI, Farkouh ME, Newman
6. Martorell R, Kettel Khan L, Hughes JD, Garvey WT: Cardiometabolic-Based
ML, Grummer-Strawn LM: Overweight Chronic Disease, Adiposity and
and obesity in preschool children from Dysglycemia Drivers. J Am Coll
developing countries. Int J Obes Relat Cardiol,2020, 75 (5):525-538.
Metab Disord 2000, 24 (8):959-967. 14. West J, Manchester B, Wright J, Lawlor
7. Kouanda S, Doulougou B, De Coninck DA, Waiblinger D: Reliability of routine
V, Habimana L, Sondo B, Tonglet R, clinical measurements of neonatal
Ketelslegers JM, Robert A: Insulin circumferences and research measurements
Growth Factor-I in Protein-Energy of neonatal skinfold thicknesses: findings
Malnutrition during Rehabilitation in Two from the Born in Bradford study. Paediatr
Nutritional Rehabilitation Centres in Perinat Epidemiol, 2011,25 (2):164-171.
Burkina Faso. J Trop Med 2009, 2009: 15. Kyle UG, Genton L, Slosman DO,
832589 Pichard C: Fat-free and fat mass
8. de Onis M, Blossner M, Borghi E: percentiles in 5225 healthy subjects aged
Global prevalence and trends of 15 to 98 years. Nutrition 2001, 17 (7-
overweight and obesity among preschool 8):534-541.
children. Am J Clin Nutr 2010, 92 16. Deurenberg P, Hautvast JG: Prevalence
(5):1257-1264. of overweight and obesity in The
9. Negash S, Agyemang C, Matsha TE, Netherlands in relation to
Peer N, Erasmus RT, Kengne AP: sociodemographic variables, lifestyle and
Differential prevalence and associations of eating behavior: starting points for the
overweight and obesity by gender and prevention and treatment of obesity. Bibl
population group among school learners in Nutr Dieta 1989; (44):8-21.
South Africa: a cross-sectional study. BMC 17. Rush EC, Chhichhia P, Hinckson E,
Obes 2017, 4:29. Nabiryo C: Dietary patterns and vitamin
10. Galan-Lopez P, Ries F, Gisladottir T, B(12) status of migrant Indian
Dom-nguez R, Sánchez-Oliver AJ: preadolescent girls. Eur J Clin Nutr 2009,
Healthy Lifestyle: Relationship between 63 (4):585-587.
Mediterranean Diet, Body Composition 18. Physical status: the use and interpretation
and Physical Fitness in 13 to 16-Years Old of anthropometry. Report of a WHO
Icelandic Students. Int J Environ Res Expert Committee. World Health Organ
Public Health 2018, 15 (12):2632 Tech Rep Ser 1995, 854:1-452.
11. Twig G, Yaniv G, Levine H, Leiba A, 19. de Onis M, Onyango AW, Borghi E,
Goldberger N, Derazne E, Ben-Ami Siyam A, Nishida C, Siekmann J:
Shor D, Tzur D, Afek A, Shamiss A et Development of a WHO growth reference
al: Body-Mass Index in 2.3 Million for school-aged children and adolescents.
Adolescents and Cardiovascular Death in Bull World Health Organ 2007, 85(9):660-
Adulthood. N Engl J Med 2016, 374 667.
(25):2430-2440. 20. WHO: AnthroPlus for Personal
12. Macek P, Biskup M, Terek-Derszniak Computers Manual: Software for
M, Stachura M, Krol H, Gozdz S, Zak Assessing Growth of the World’s Children
M: Optimal Body Fat Percentage Cut-Off and Adolescents. Bull World Health Organ
Values in Predicting the Obesity-Related 2007, Geneva: WHO; 2009. Available
Cardiovascular Risk Factors: A Cross- from:
African Journal of Health Sciences Volume 34, Issue No. 1, January - February, 2021 10http://www.who.int/growthref/tools/en/ 25. Hattori K, Tahara Y, Moji K, Aoyagi K,
[Last accessed on 2019, January 15th]. Furusawa T: Chart analysis of body
21. Brown N, Scurr J: The need for a composition change among pre- and
standardised anthropometric protocol for postadolescent Japanese subjects assessed
objective assessment of pre- and by underwater weighing method. Int J
postoperative breast surgery. Gland Surg Obes Relat Metab Disord 2004, 28:520–
2012, 1(3):142-145. 524.
22. Eriksson Hogling D, Bäckdahl J, Thorell 26. Wells JC: Sexual dimorphism of body
A, Rydn M, Andersson DP: Metabolic composition. Best Pract Res
Impact of Body Fat Percentage ClinEndocrinol Metab 2007, 21:415–430.
Independent of Body Mass Index in 27. Olivieri F, Semproli S, Pettener D,
Women with Obesity Remission After Toselli S Growth and malnutrition of rural
Gastric Bypass. 2020; Obes Surg, 30 Zimbabean children ( 6 – 17 feaors of age).
(3):1086-1092. Am J Phys Anthrol 2008, 136 : 214 – 222
23. Grundy SM, Williams C, Vega GL: 28. Semproli S, Gualdi-Russo E. Childhood
Upper body fat predicts metabolic malnutrition and growth in a rural area of
syndrome similarly in men and women. western Kenya. Am J Phys Anthropol
Eur J Clin Invest,2018 ; 48(7). 2007; 132 : 463 - 469.
24. Maynard LM, Wisemandle W, Roche 29. Buhendwa RA, Roelants M, Thomis M,
AF, Chumlea WC, Guo SS, Siervogel Nkiama CE: Nutritional status and height,
RM: Childhood body composition in weight and BMI centiles of school-aged
relation to body mass index. Pediatrics children and adolescents of 6-18-years
2001, 107:344–330. from Kinshasa (DRC). Ann Hum Biol 2017
44 (6):554-561.
African Journal of Health Sciences Volume 34, Issue No. 1, January - February, 2021 11You can also read