Automation in Krypton Loser Photocoogulation
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Automation in Krypton Loser Photocoogulation
Oleg Pomeranfzeff, George Timberlake, Guong-Ji Wang, Michoil M. Pankrarov,
ond Julianne Schneider-Goren
Histologic study of lesions produced by krypton red (647.1 nm) and krypton yellow (568.2 nm) laser
lights reported here suggests advantages in alternating these two wavelengths in photocoagulation.
Selection of the best wavelength to be used in a given location on the retina should result from pre-
determined absorbance conditions in that location. The feasibility of the relative measurement of ab-
sorbance in different fundus locations by measurement of the relative reflectance is discussed. Instru-
mentation for these measurements and for switching from one wavelength to the other is described.
Instrumentation for the possible expansion of krypton laser applications to clinical problems in the
anterior segment also is suggested. Invest Ophthalmol Vis Sci 25:711-719, 1984
The use of krypton red (647.1 nm) laser light for ferred to the tissue were determined before the irra-
photocoagulation is currently receiving a good deal of diation, and if the beam used for this measurement
clinical attention,1"8 whereas the use of krypton yellow were the actually used coagulating beam.
(568.2 nm) appears to be receiving less.9 This is un- We also think that the variety of laser wavelengths
fortunate because the red and yellow krypton lights available for photocoagulation makes the identification
each have their own advantages for photocoagulation, of those most suitable for photocoagulation essential.
and it seems unlikely that exclusive use of either light Some of the wavelengths, such as the blue ones, are
will be satisfactory in all clinical situations. We believe absorbed in xanthophyll. Their use, at least in older
that the most effective clinical use of the krypton laser patients and in the macular area, should be avoided.
can be obtained by combining the advantageous aspects The blue wavelengths also have a pronounced, objec-
of both of these laser lights and will demonstrate here tionable photochemical action on ocular tissues.
the relative merits of red and yellow laser lights in This work is based on our histologic study of the
photocoagulation by histologic studies of lesions. We effect of red and yellow wavelengths on the ocular
also believe that to increase the safety and efficiency tissues in different fundus locations of the owl monkey.
of photocoagulation in ophthalmology some changes, The results of these studies were used to demonstrate
which are described here, must be made in currently the specific differences of each of the two wavelengths.
used instrumentation.
Little has been done to introduce automatic features,
Materials and Methods
available even in inexpensive photographic cameras,
into photocoagulators.10 To our knowledge, only Birn- The wavelengths with the most specific effect on
gruber and his colleagues in West Germany have ap- ocular tissues are those in the red and green-yellow
proached this problem. They have been interested, range. We selected krypton yellow (568.2 nm), an
however, in automatically terminating the photoco- isobestic wavelength (equally well absorbed in oxy-
agulation when the ophthalmoscopic appearance of genated and reduced blood), because its absorption in
the lesion shows the goal has been attained." We think blood is much higher than the commonly used argon
that the method of stopping the coagulation by mea- green (514.5 nm). (The absorption coefficient of kryp-
suring the amount of energy absorbed in the tissue ton yellow in blood is more than twice as high as that
during the photocoagulation is a step toward increasing of the presently used argon green.) The red, little of
the efficiency and safety of photocoagulation treatment. which is absorbed in blood, is the other specifically
We believe, however, that this technique would be absorbed wavelength. We used the red wavelength of
more efficient if the right amount of energy to be trans- 647.1 nm since it and the yellow (568.2) are both
available in our krypton laser. These wavelengths also
From the Eye Research Institute of Retina Foundation, Boston, can be produced by dye lasers.
Massachusetts. A problem that arises with the clinical use of krypton
Supported in part by National Institutes of Health grant EY-
yellow is its instability below 50 mW (especially for
02725 and by a grant from Allergan Pharmaceuticals, Inc.
Submitted for publication: August 1, 1983. the aiming beam). We have solved this problem by
Reprint requests: Oleg Pomerantzeff, Eye Research Institute, 20 incorporating an Acousto-Optic Deflector Modulator
Staniford Street, Boston, MA 02114. (ADM)12 into the system. The laser is operated con-
711712 INVESTIGATIVE OPHTHALMOLOGY & VISUAL SCIENCE / June 1984 Vol. 25
a preset amount (from almost zero to 90%) of the
power from zero order into the first-order beam, as
commanded by the electronic driver. The delivery sys-
tem is made coaxial with the first-order beam, which
100 mW crosses the mirror through an aperture provided ad
200 ms hoc. The electronic driver can be operated either man-
ually from the switchboard or automatically by signals
from the reflectometer.
The ADM, in addition to deflecting into the delivery
system a preset percent of the energy contained in the
100 ms total beam, also can deflect each wavelength from the
total (polychromatic) beam separately, at the operator's
choice. The intracavity wavelength selector is replaced
by a broad-band mirror, 100% reflective for red and
yellow. This makes the krypton laser emit both red
and yellow wavelengths together. The ADM electronic
2^ 100 mW
driver commands both features, the deflection of the
100ms i
selected wavelength into the delivery system and the
Fig. 1. Monochromatic (570 nm) photograph of the owl monkey's fixation of its power.
fundus photocoagulated with krypton red (647.1 nm) light. Spot size
diameter was 100 ^m in all applications, but power and exposure Results
time varied among pairs of lesions.
Figure 1 shows the typical ophthalmoscopic ap-
pearance of three pairs of lesions produced with kryp-
tinuously at its maximum power, where it is stable ton red light with spot size of 100 fim. We selected
within ±1%. The laser beam crosses the ADM in its this spot size because it is proportional to the small
zero order with a transmission of 95%. This beam is size of the ocular structure in the owl monkey. (Ob-
deflected to a light trap by a mirror. The ADM diffracts viously, different spot sizes are appropriate for different
r
Fig. 2. Histology section through the center of lesion 3 in Figure 1. A good therapeutic lesion was produced with krypton red light using
spot size 100 fim, power 125 mW, and exposure time 100 msec.No. 6 AUTOMATION IN KRYPTON LASER PHOTOCOAGULATION / Pomeronrzeff er ol. 713
clinical goals. However, for our purpose of comparing
colors, any spot size could be used. Small spot sizes,
as well as lower laser beam power, give more char-
acteristic information on the behavior of a given laser
beam.) The energy was the same for each pair but ;*.*•'
varied among pairs. The ophthalmoscopic appearance
of lesions among pairs is not the same, nor is it the
same within each pair.
Figure 2 shows the histology of lesion 3 from Figure
1, which is a good therapeutic lesion. We consider a
good therapeutic lesion to be one that is confined to
the pigment epithelium and receptor layer and that
leaves the nerve fiber layer and Bruch's membrane
intact. Damage to the nerve fiber layer may create an
unwanted scotoma and breaks in Bruch's membrane
create an entrance to new vascularization. The same
kind of lesion is demonstrated in Figure 3, which shows
the histologic section of a lesion in a macaque fovea
containing xanthophyll. It is this type of lesion that
generates enthusiasm about the clinical value of kryp-
ton red, especially for panretinal photocoagulation
(PRP). In addition, there seem to be fewer postoperative Fig. 3. Histology section through the center of a lesion in a macaque
monkey's fovea produced with krypton red light using 50 fim spot
complications when red light is used.1'268 size, 40 mW power and 50 msec exposure time.
In Figure 4 the histologic section of lesion 4 from
Figure 1 shows deeply penetrating damage into the
choroid with a choroidal hemorrhage. Lesions 3 and tween the two lesions is shown in Figure 5, which
4 were produced with the same dosage of krypton red presents the ophthalmoscopic appearance of the same
laser light. The reason for this dramatic difference be- fundus in red light. In areas where the inner choroidal
Fig. 4. Histology section through the center of lesion 4 in Figure 1. Bruch's membrane is broken, and there is deep penetration into the
choroid with choroidal hemorrhage. Spot size, power, and exposure time are the same as in lesion 3 (Fig. 2).714 INVESTIGATIVE OPHTHALMOLOGY 6 VISUAL 5CIENCE/ June 1984 Vol. 25
produced choroidal hemorrhage was on a heavily pig-
mented inner choroid above another large choroidal
vessel. This variability of lesions produced with the
same dosage of krypton red laser light is the cause of
the dissatisfaction noted by some clinicians. 1 ' 613
In summary, the same dosage of krypton red irra-
diation can produce either excellent therapeutic lesions
or undesirable damage, depending on its location in
the fundus. Clinical use would be much safer if the
laser power could be adjusted to the local absorbance
conditions.
Figure 6 shows a typical ophthalmoscopic appear-
ance of the three pairs of lesions by krypton yellow.
With the exception of lesion 1, they are all very much
alike. Small differences in lesion size are due to dif-
ferences in irradiation dosage between different pairs.
Figure 7 shows the histology of lesion 1 in Figure 6.
Fig. 5. Monochromatic (640 nm) photograph of the same fundus The choroid is entirely destroyed, and an extensive
as in Figure 1 photocoagulated with krypton red light. Large choroidal choroidal hemorrhage resulted from the explosion of
vessels are visible in negative contrast through the lightly pigmented
the large choroidal vessel. The histology of lesion 2
inner choroid.
from Figure 6 is shown in Figure 8. Lesion 2 is a good
therapeutic lesion. The difference in effect produced
layers are not heavily pigmented, illumination with by these applications of equal irradiation dosage is
red light shows the large choroidal vessels in sharp explained in Figure 9, which shows the ophthalmo-
negative contrast. Figure 5 shows that the good ther- scopic appearance of these lesions in red light. Lesion
apeutic lesion was produced on a large choroidal vessel 1, which produced hemorrhage, was placed on a large
with little melanin above it, whereas the lesion that choroidal vessel with a lightly pigmented inner choroid.
Lesion 2, which was therapeutic, was placed on a
heavily pigmented inner choroid. Thus, the unwanted
heavy damage produced by krypton yellow and by
krypton red light seems to occur in opposite absorbance
conditions.
Figure 10 summarizes the damage produced by red
and yellow light for both the lightly and heavily pig-
mented inner choroid. Histologic sections A and C
show lesions produced with red and yellow light on
lightly pigmented inner choroid. Red light (A) produces
a mild, therapeutically useful lesion, whereas yellow
light (C), incident almost directly on a large choroidal
vessel, produces choroidal hemorrhage. Sections B and
D show lesions produced with the same colors and
same dosage on a heavily pigmented inner choroid
with underlying large choroidal vessel. In this case, red
light (B) produces hemorrhage, and yellow light (D)
produces good therapeutic lesions. This figure clearly
shows that a large choroidal vessel under a lightly pig-
mented inner choroid is a condition of high risk for
yellow light, and a heavily pigmented inner choroid
over a large choroidal vessel is a condition where the
use of red light could be dangerous.
Fig. 6. Monochromatic (570 nm) photograph of owl monkey's
fundus photocoagulated with krypton yellow (568.2 nm) light. All Discussion
lesions except lesion 1 have a similar ophthalmoscopic appearance.
Spot size used was 100 Mm m ^1 applications, but power and exposure From these results it follows that: (1) The prede-
time varied among pairs of lesions. termination of absorbance conditions in every targetNo. 6 AUTOMATION IN KRYPTON LASER PHOTOCOAGULATION / Pomeronrzeff er ol. 715
Fig. 7. Histology section through the center of lesion 1 in Figure 6. Bruch's membrane is broken, and there is a choroidal hemorrhage.
Fig, 8, Histology section through the center of lesion 2 in Figure 6. This is a good therapeutic lesion.716 INVESTIGATIVE OPHTHALMOLOGY & VISUAL SCIENCE / June 1984 Vol. 25
often found in older patients, makes absolute mea-
surements difficult. By matching the entrance pupil of
the reflectometer with the patient's dilated pupil, we
make the measurements at the cornea of the light scat-
tered back from retina and choroid, independent of
retinal location, at least in the posterior hemisphere.
This enables us to obtain a quantitative comparison
of the absorbance conditions in any location of the
fundus with those measured in a test location, which
is sufficient for our purpose. The measurement in the
test location is stored in memory, the measurement
in any new location is compared automatically with
the stored value, and the dosage is preset accordingly.
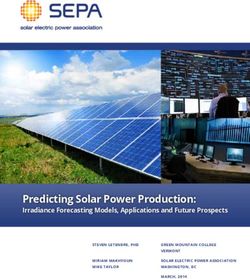
An example of the measurement of the relative ab-
sorbance of the red and yellow light is shown in Figure
12. The upper trace shows the absorbance (obtained
by measuring the reflectance) along a line traced on
the fundus by the krypton red aiming beam. The bot-
tom trace shows the absorbance along approximately
the same line traced by the krypton yellow aiming
beam. The curve for the yellow light is almost flat,
Fig. 9. Monochromatic (640 nm) photograph of the same fundus
showing even absorbance, except for two vessels rep-
as in Figure 6. Large choroidal vessels are visible in negative contrast
through the lightly pigmented inner choroid. resented by two peaks, whereas the curve for red light
shows irregular absorbance.
Other important information needed in photoco-
location and the automatic presetting of the irradiation agulation is the melanin concentration in the inner
dosage should permit a safer clinical use of both wave- choroidal layer and in the retinal pigment epithelium.
lengths. (2) Even better results can be obtained by This information can be obtained by measuring the
changing rapidly and automatically from one wave- reflectance with yellow and red, consecutively, in the
length to the other, according to the pigmentation of same location. A large difference between the two
the inner choroid. (3) Automation requires continuous measurements indicates a lightly pigmented inner
processing of an analog signal from a measuring device choroid and a choroidal vessel crossed by the laser
into a digital signal to the device that adjusts the dosage. beam because the red is absorbed only in melanin and
A microprocessor has been built into the system for the yellow in melanin and also in the choriocapillaris
this purpose. and the large choroidal vessel. This describes the con-
To estimate the absorbance conditions in every target ditions of high risk for yellow light. A very small dif-
area and to monitor the formation of the lesion during ference between the two measurements indicates a
photocoagulation, we designed the ophthalmoscopic heavily pigmented choroid and no large choroidal ves-
attachment shown in Figure 11. 1 0 1 4 1 5 The absorbance sels in the laser beam's pathway, or, at least, that the
obviously is not measurable in vivo. One could, how- pigmentation in the inner choroid is sufficient to absorb
ever, obtain a good approximation of absorbance by either wavelength almost entirely before it reaches the
measuring the power of the coagulating beam at the blood vessel. This indicates that either color could be
target location in the retina and the total flux scattered used with a dosage of irradiation sufficiently reduced
back from the retina and choroid in the same location to prevent a penetration of lesions deep into the choroid
at the retinal surface. We assume that the small amount with damage to Bruch's membrane. A sizable difference
of light transmitted through all layers in the fundus, between measurements would indicate more or less
including the sclera, is negligible, and varies little pigmented inner choroid with the large choroidal vessel
throughout the fundus of the same eye. Physically the in the pathway of the laser beam. This difference is
measurement can be done only at the cornea. The due to the absorption of yellow in choriocapillaris and
calculation of the corresponding values at the retina in the large choroidal vessel. This describes a condition
requires the knowledge of the unknown transmission of high risk for red light.
losses of the laser beam on its way in, toward the Introduction of ADM into the photocoagulator per-
retina, and for the flux scattered back from the retina. mits rapid switching from one wavelength to the other,
The difficulty in determining these losses, especially and at the same time it solves another important prob-
in the nonuniformly absorbing and scattering media lem. In case of accidental hemorrhage during treatmentINNER CHOROIDAL PIGMENTATION
LIGHT HEAVY
PTON
ED
THERAPEUTIC LESION HEMORRHAGE
PTON
LOW
HEMORRHAGE THERAPEUTIC LESION
Fig. 10. A histologic analysis of the damage produced byredand yellow light in lightly and heavily pigmented inner choroid.718 INVESTIGATIVE OPHTHALMOLOGY & VISUAL SCIENCE / June 1984 Vol. 25
it permits us to treat with red light all locations with
low absorbance in the inner choroid and switch to
yellow in locations where the inner choroid is heavily
pigmented, thus avoiding the risk of hemorrhage while
at the same time taking full advantage of the red light.
The ADM also permits the conversion of the krypton
laser from continuous to pulsating mode with selectable
frequency from 0-10 MHz. The therapeutic value of
short pulses for clinical work in the anterior segment
seems to be well established. l6~18 The possibility of
using the krypton laser in either a continuous or a
pulsating mode significantly increases the range of its
clinical applications.
In conclusion, we think that this laser photocoag-
ulator isflexibleenough to be used in almost all clinical
cases. It emits two wavelengths that can be used either
continuously or in very short pulses. The selection of
color depends on absorption in the fundus. The in-
Fig. 11. The noncontact ophthalmoscopic attachment for krypton strumentation permits rapid switching from one wave-
laser photocoagulator with on-the-line reflectometer. length to another. In addition, all krypton wavelengths
can be combined for a burst of 3-4 millijoules in a
with the red light, the clinician can switch rapidly from /isec pulse range.
red to yellow and cauterize the bleeding vessel. The However, only an extensive study of histologic sec-
arrangement also permits us to start the treatment tions and their relation to predetermined color and
with one color and continue it with the other. Finally, irradiation dosage will demonstrate the laser photo-
coagulator's reliability. Our hope is that this attempt
will provoke more research in this field that will lead
to safer and more efficient operation.
KRYPTON RED Key words: krypton red laser, krypton yellow laser, photo-
coagulation, instrumentation, histologic study
Acknowledgments
The authors thank Patricia Pearson for the histology and
Drs. Noritsugu Mukai and Ilene Gipson for helping to in-
terpret the results.
References
KRYPTON YELLOW L Marshall J and Bird AC: A comparative histopathological study
of argon and krypton laser irradiations of the human retina. Br
J Ophthalmol 63:657, 1979.
2. Bird AC and Grey RHB: Photocoagulation of disciform macular
lesions with krypton laser. Br J Ophthalmol 63:669, 1979.
3. Talbot JF and Bird AC: Krypton laser in the management of
disciform macular degeneration. Trans Ophthalmol Soc UK
100:423, 1980.
••-X 4. Schulenburg WE, Hamilton AM, and Blach RK: A comparative
study of argon laser and krypton laser in the treatment of diabetic
DISTANCE ON RETINA optic disc neovascularisation. Br J Ophthalmol 63:412, 1979.
Fig. 12. A comparison of the absorbance of krypton red and 5. Peyman GA, Li M, Yoneya S, Goldberg MF, and Raichand M:
yellow lights in the owl monkey's retina when weak (aiming) beam Fundus photocoagulation with the argon and krypton lasers: A
sweeps fundus. The curve for red light shows irregular absorbance comparative study. Ophthalmic Surg 12:481, 1981.
and that for yellow light shows even absorbance except for two 6. Yannuzzi LA and Shakin JL: Krypton red laser photocoagulation
vessels, represented as peaks. of the ocular fundus. Retina 2:1, 1982.No. 6 AUTOMATION IN KRYPTON LASER PHOTOCOAGULATION / Pomeronrzeff er ol. 719
7. Singerman LJ: Red krypton laser therapy of macular and retinal Treatment of neovascular senile maculopathy at the foveal cap-
vascular diseases. Retina 2:15, 1982. illary free zone with red krypton laser. Retina 2:127, 1982.
8. Yannuzzi LA: Krypton red laser photocoagulation for subretinal 14. Pomerantzeff O, Wang G-J, Pankratov M, and Schneider J: A
neovascularization. Retina 2:29, 1982. method to predetermine the correct photocoagulation dosage.
9. Trempe CL, Mainster MA, Pomerantzeff O, Avila MP, Jalkh Arch Ophthalmol 101:949, 1983.
AE, Weiter JJ, McMeel JW, and Schepens CL: Macular pho- 15. Pomerantzeff O, Wang G-J, Pankratov M, and Schneider J:
tocoagulation. Optimal wavelength selection. Ophthalmology Time and location analysis of lesion formation in photocoag-
89:721, 1982. ulation. Arch Ophthalmol 101:954, 1983.
10. Pomerantzeff O and Timberlake G: Toward automation in pho- 16. van der Zypen E, Fankhauser F, Bebie H, and Marshall J: Changes
tocoagulation. In Doc Ophthalmol Proc Series, Vol 33, Birn- in the ultrastructure of the iris after irradiation with intense light.
gruber R, editor. Hague, The Netherlands, Dr W Junk, 1983, A study of long-term effects after irradiation with argon ion,
pp. 313-319. Nd:YAG and Q-switched ruby lasers. Adv Ophthalmol 39:59,
11. Weinberg W, Lorenta B, Birngruber R, and Gabel VP: Con- 1979.
trolling retinal photocoagulation by light reflection. In Doc 17. Aron-Rosa D, Aron JJ, Griesemann M, and Thyzel R: Use of
Ophthalmol Proc Series, Vol 33, Birngruber R, editor. Hague, the neodymium-YAG laser to open the posterior capsule after
The Netherlands, Dr W Junk, 1983, pp. 299-311. lens implant surgery: A preliminary report. Am Intra-ocular
12. Korpel A: Acousto-Optics. In Applied Optics and Optical En- Implant Soc J 6:352, 1980.
gineering, Vol VI, Kingslake R and Thompson BJ, editors. New 18. Peyman GA, Kraff M, Viherkoski E, and Ressler N: Noninvasive
York, Academic Press, 1980, pp. 119-130. capsulectomy using a new pulsed infrared laser. Am Intraocular
13. Yassur Y, Axer-Siegel R, Cohen S, Svetliza E, and Ben-Sira I: Implant Soc J 8:239, 1982.You can also read