Approach to Urinary Retention in the Emergency Department - Andrew Lohoar SJRH Emergency Department Rounds
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Approach to Urinary Retention in
the Emergency Department
Andrew Lohoar
SJRH Emergency Department Rounds
June 2021
Objectives • Introduction • Physiology • Etiology • Treatment • Discussion/Conclusions
Case 1 • 72 y.o. with history of DM, HTN presents to peripheral hospital (CCH) with inability to urinate x 8 hours
Acute Urinary Retention • Definition: Painful, palpable or percussable bladder when patient is unable to pass any urine* (* Not always perceived by certain patients – i.e. delerium, neurologic conditions, decreased LOC etc.)

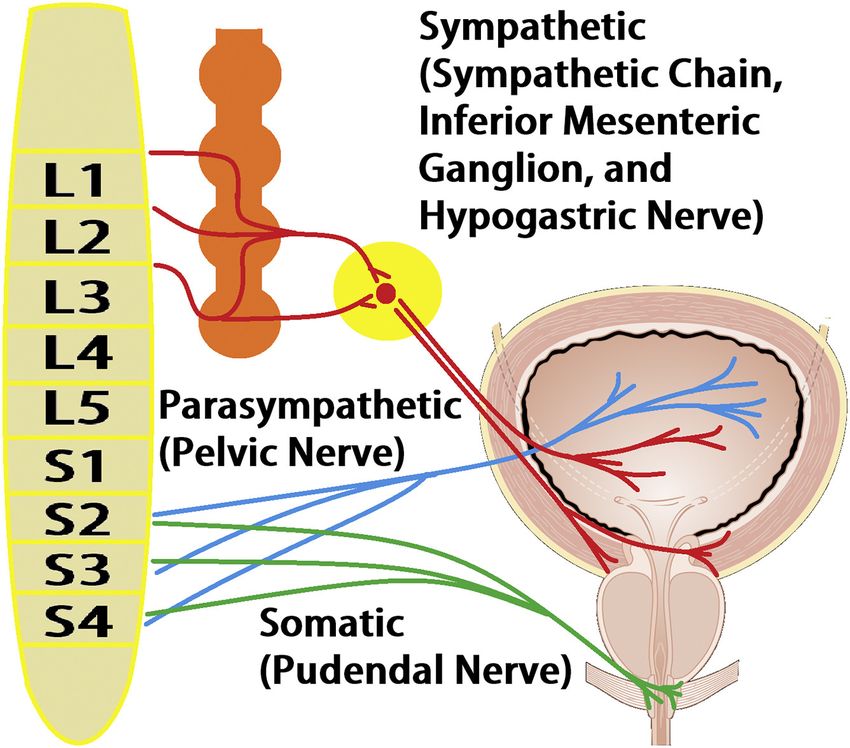
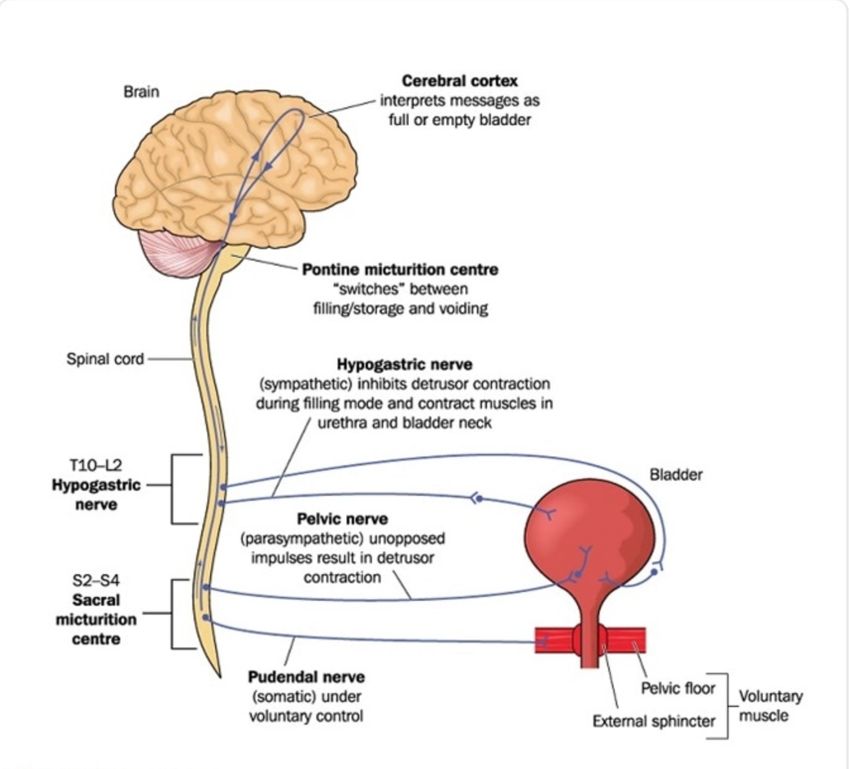
Physiology of Micturition
Physiology of Micturition
Etiology
• Structural – Intrinsic, extrinsic
• Iatrogenic – Pharmacological and
non-pharmacological
• Infectious – Inflammatory narrowing
• Neurologic – CES, stroke, Parkinson’s, DMInvestigations • Physical exam • POCUS, bladder scan • Labs – to identify renal failure, UTI
Calculating bladder volume with
POCUSTreatment • Goal of therapy: 1) Decompress bladder 2) Mitigate cause of retention if possible
Case 1 • 72 y.o. with history of DM, HTN presents to peripheral hospital (CCH) with inability to urinate x 8 hours • Attempt at catheterization with standard Foley catheter fails
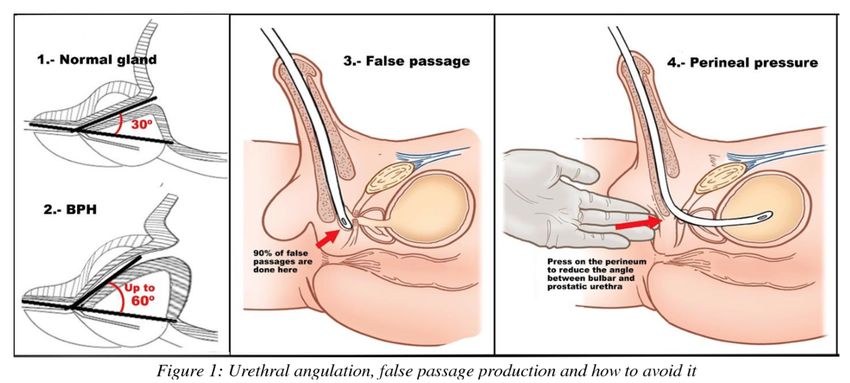
Challenging urethral catheter
placement
• Stepwise approach:
1) Consider contraindications – recent surgery, trauma
2) Anesthesia/lubricant
3) Standard tip Foley catheter (or 3-way catheter in patient with
gross hematuria)
4) Coudé tip
5) Silastic catheterChallenging urethral catheter
placementCase 1 • 72 y.o. with history of DM, HTN presents to peripheral hospital (CCH) with inability to urinate x 8 hours • Attempt at catheterization with standard Foley, Coudé and Silastic all fail • And there is a blizzard outside..
SPC Kit with Trocar
Challenging urethral catheter
placement
• Suprapubic cystostomySPC – Seldinger Kit
SPC as first line for AUR? • 86 consecutive patients to ED in Ireland needing catheterization with AUR from BPH • “In conclusion, this study has shown that the use of suprapubic catheters in acute urinary retention significantly reduces the risk of urinary tract infection and urethral stricture formation. It also allows for a trial of micturition without the discomfort, the urethral trauma and the risk of infection associated with the re- insertion of a urethral catheter.”
Slow versus Rapid Bladder
Decompression
Rapid versus gradual bladder decompression in acute urinary retention
Mohamed H. Etafy, Fatma H. Saleh, Cervando – 2017 Urol Ann
• 62 patients with AUR secondary to BPH
• “We conclude that there is no significant difference between rapid and
gradual decompression of the bladder in patients with AUR. Hematuria
and hypotension may occur after rapid decompression of the obstructed
urinary bladder, but these complications are rarely clinically significant”.Treatment • Medications: Alpha-adrenergic blockers • Follow-up • Admission
Medication • 2014 Cochrane review • 9 RCT comparing alpha blockers to placebo • “There was some evidence to suggest that alpha blockers increase the success rates of trial without catheter, and the incidence of adverse effects was low. There was some evidence of a decreased incidence of acute urinary retention. The need for further surgery, cost effectiveness and recommended duration of alpha blocker treatment after successful trial without catheter remain unknown as these were not reported by any trial”
Disposition
• Urology follow-up
– Timing for trial of voiding: 3-7 days
– Higher rates of complications with catheter in
place longer length of time
• Admission
– Large variation worldwide admission rates
– Consider admission with sepsis, significant acute
kidney injury, concerns re: catheter managementApproach to special populations • Pediatrics • Women - Higher incidence serious diagnoses - Usually require more thorough work-up
Conclusions • Medical history should include inquiry into neurologic, infectious, medication as well as structural etiologies for retention • Consider stepwise approach to difficult urethral catheterization • Consider SPC (using Seldinger approach with U/S guidance) • No routine antibiotics after catheterization (consider one time dose if traumatic or repeated attempts) • Discharge with alpha blocker if BPH • Urology follow-up for trial of urination within 7 days
References • Billet M. Urinary Retention. Emerg Med Clin N Am 37 (2019) 649–660 • Gelber J. Management of acute Urinary Retention in the Emergency Department. Emerg Med Practice 2021 23(3): 1-25 • Mohamed H. Etafy et al. Rapid versus gradual bladder decompression in acute urinary retention. Urol Ann. 20`17; 9():339-342. • A. F. Horgan et al. Acute Urinary Retention. Comparison of Suprapubic and Urethral Catheterisation. Br J Urology (1992). 70, 149-151
You can also read