Antiemetics in Children With Acute Gastroenteritis: A Meta-analysis - American ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Antiemetics in Children With Acute
Gastroenteritis: A Meta-analysis
Laura F. Niño-Serna, MD, MSc,a,b Jorge Acosta-Reyes, MD, MSc,c Areti-Angeliki Veroniki, PhD,d,e,f Ivan D. Florez, MD, MSca,g
CONTEXT: Several antiemetics have been used in children with acute gastroenteritis. However, abstract
there is still controversy over their use.
To determine the effectiveness and safety of antiemetics for controlling vomiting in
OBJECTIVE:
children with acute gastroenteritis.
DATA SOURCES: Medline,
Embase, Cochrane Central Register of Controlled Trials, Cumulative Index
to Nursing and Allied Health Literature, Latin America and the Caribbean Literature on Health
Sciences, and gray literature, until December 2018.
STUDY SELECTION: We
selected randomized clinical trials comparing metoclopramide, ondansetron,
domperidone, dexamethasone, dimenhydrinate, and granisetron.
DATA EXTRACTION: Two reviewers independently screened abstracts and full texts, extracted the
data, and assessed the risk of bias. We performed pairwise and network meta-analysis using
the random-effects model.
RESULTS: Twenty-four studies were included (3482 children). Ondansetron revealed the largest
effect in comparison to placebo for cessation of vomiting (odds ratio = 0.28 [95% credible
interval = 0.16 to 0.46]; quality of evidence: high) and for hospitalization (odds ratio = 2.93
[95% credible interval = 1.69 to 6.18]; quality of evidence: moderate). Ondansetron was the
only intervention that reduced the need for intravenous rehydration and the number of vomiting
episodes. When considering side effects, dimenhydrinate was the only intervention that
was worse than placebo.
LIMITATIONS: Most
treatment comparisons had low- or very low–quality evidence, because of risk
of biases and imprecise estimates.
Ondansetron is the only intervention that revealed an effect on the cessation of
CONCLUSIONS:
vomiting, on preventing hospitalizations, and in reducing the need for intravenous
rehydration. Ondansetron was also considered a safe intervention.
a
Department of Pediatrics, University of Antioquia, Medellín, Colombia; bHospital Pablo Tobón Uribe, Medellín, Colombia; cDepartment of Public Health, Universidad del Norte, Barranquilla,
Colombia; dDepartment of Primary Education, School of Education, University of Ioannina, Ioannina, Greece; eLi Ka Shing Knowledge Institute, St Michael’s Hospital, Toronto, Ontario, Canada;
f
Department of Surgery and Cancer, Institute of Reproductive and Developmental Biology, Faculty of Medicine, Imperial College, London, United Kingdom; and gDepartment of Health Research
Methods, Evidence, and Impact, McMaster University, Hamilton, Ontario, Canada
Dr Niño-Serna conceptualized and designed the study, performed the data collection, evidence synthesis, and quality-of-evidence assessment, drafted the initial
manuscript, and reviewed and revised the manuscript; Dr Acosta-Reyes performed the data collection, evidence synthesis, and quality-of-evidence assessment and
critically reviewed the manuscript as submitted; Dr Veroniki performed the statistical analyses, drafted the initial manuscript, and critically reviewed the manuscript
as submitted; Dr Florez conceptualized and designed the study, performed the evidence synthesis and quality-of-evidence assessment, drafted the initial manuscript,
and reviewed and revised the manuscript; and all authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
To cite: Niño-Serna LF, Acosta-Reyes J, Veroniki A, et al. Antiemetics in Children With Acute Gastroenteritis: A Meta-analysis. Pediatrics. 2020;145(4):e20193260
Downloaded from www.aappublications.org/news by guest on July 13, 2021
PEDIATRICS Volume 145, number 4, April 2020:e20193260 REVIEW ARTICLE
Diarrheal diseases remain the third whereas dimenhydrinate revealed Search strategies were developed in
cause of death among children a positive effect on vomiting duration. liaison with an experienced librarian
,5 years old, mostly in low- and Nevertheless, the authors did not (Supplemental Information). We used
middle-income countries.1,2 Although compare antiemetics among them validated filters for identifying
in high-income countries the disease and included only 7 studies. Later, pediatric articles and RCTs.7,12 No
is rarely fatal, it is a leading cause of Carter et al10 performed a network language or publication status limits
emergency department (ED) visits meta-analysis (NMA) including all the were used. We performed gray
and hospitalizations.3 The American antiemetics for which there was literature searches through trial
Academy of Pediatrics defines acute evidence at that time. The authors registries (www.clinicaltrials.gov and
gastroenteritis as a diarrheal disease found that ondansetron was the best World Health Organization Clinical
of rapid onset, with or without intervention to reduce vomiting, the Trials Registry Platform).
additional symptoms and signs, such need for intravenous rehydration, and
as nausea, vomiting, fever, or hospitalizations. However, some Eligibility Criteria
abdominal pain.4 Furthermore, acute concerns were raised because We included RCTs and quasi RCTs in
diarrhea is defined by the World ondansetron was associated with an which authors evaluated antiemetics
Health Organization as the passage of increase of diarrhea. used for controlling vomiting in
3 or more loose or liquid stools per In the last decade, many randomized children with ADG. Our interventions
day for 3 or more days but ,14 clinical trials (RCTs) comparing of interest were metoclopramide,
days.5 Both definitions refer to the different antiemetics to placebo or ondansetron, domperidone,
same disease: acute diarrhea and against each other have been dexamethasone, dimenhydrinate,
gastroenteritis (ADG), that is, an published and have not been yet alizapride, and granisetron at any
infectious episode of the synthesized. Specifically, new dose and presentation in children
gastrointestinal tract. evidence from trials studying with ADG and vomiting. Researchers
In addition to diarrhea, ADG dexamethasone, metoclopramide, had to compare any of the
commonly presents with vomiting.5 domperidone, and ondansetron have interventions against them, a placebo,
Vomiting is particularly challenging been available. To date, there is no conventional treatment with ORT, or
for parents and health care systematic review or NMA comparing different doses or administration
professionals because it can hinder all the currently available antiemetics routes of the same intervention and
oral rehydration therapy (ORT), in children with ADG. Therefore, we had to report at least 1 of the
worsen dehydration, and cause aimed to assess the relative outcomes of interest.
hospitalizations.6 In most cases, ORT effectiveness and safety of
can help to control vomiting. antiemetics in children with ADG Outcomes
However, in some cases, vomiting is through direct and indirect Our primary outcomes were cessation
severe and may affect the ORT comparisons using an NMA. of vomiting and hospitalization. The
success. Therefore, some antiemetics secondary outcomes included the
have been used to control vomiting in METHODS need for intravenous rehydration
children with ADG. Nevertheless, (measured as the number of
This systematic review was
some clinical practice guidelines participants who required
registered in the PROSPERO
(CPGs) do not recommend intravenous rehydration during the
International Prospective Register of
antiemetics because some of them ED stay and up to 3 days after
Systematic Reviews
have shown significant side effects.4,7 discharge); revisit to the ED
(CRD42016035236). This article
In contrast, other CPGs8 recommend (measured as the number of
complies with the recommendations
ondansetron and have discouraged participants that revisited the ED up
of the PRISMA (Preferred Reporting
the use of other antiemetics because to 72 hours after discharge); number
Items for Systematic Reviews and
of lack of evidence. of vomiting (measured as the mean
Meta-Analyses) extension for NMA.11
number of vomiting episodes during
The evidence of antiemetics for ADG
Search Process the observation period); and side
was first synthesized by Fedorowicz
effects.
et al.9 In this review, ondansetron We searched Medline (Ovid), Embase
revealed a significant effect on (Ovid), Cochrane Central Register of Regarding side effects, as a post hoc
cessation of vomiting and the need Controlled Trials, Cumulative Index to analysis, we analyzed side effects
for intravenous rehydration. Also, Nursing and Allied Health Literature, (any side effect reported by the
metoclopramide was found to be and Latin America and the Caribbean authors) and diarrhea separately. We
effective in reducing vomiting Literature on Health Sciences from separated the outcomes because
episodes and hospital admissions, the inception to December 31, 2018. diarrhea was reported as
Downloaded from www.aappublications.org/news by guest on July 13, 2021
2 NIÑO-SERNA et al
a dichotomous (presence or absence Assessment of Risk of Bias in NMA
of diarrhea in the observation) and Included Studies
We performed an NMA to analyze
continuous variable (mean number of We assessed, independently and in all the potential comparisons among
diarrheal stools), with the latter being duplicate, all included studies for interventions for each outcome. An
the most commonly reported. The their risk of bias (RoB) using NMA, also known as multiple-
presence of diarrhea (dichotomous) a modified version of the Cochrane treatment comparisons or multiple-
was analyzed along with the rest of RoB tool13 on the basis of the treatment meta-analysis, is a special
the side effects, but it was not following criteria: sequence statistical technique that provides
possible to combine with the generation, allocation concealment, a methodology to address the issue
continuous data. Lastly, the blinding of participants, personal of having available many
worsening of diarrhea has been and outcome assessors, completeness interventions for the same condition
described as a major concern for of follow-up, selective outcome under study, mostly compared against
the use of ondansetron in previous reporting, and other biases. For a placebo but less or not compared
systematic reviews9,10 and CPGs.4,7 each criterion, an RoB score was against each other.16 NMA takes
Thus, we wanted to determine the assigned as “definitely low,” advantage of 2 statistical approaches.
specific effect on the number of stools “probably low,” “probably high,” or First, it takes advantage of the use
beside the incidence of side effects to “definitely high” risk.14 of indirect comparisons: we can
better inform further clinical Disagreements were resolved by estimate the effect of intervention
decision-making. consensus, and a third reviewer A versus intervention B, indirectly
Study Selection was involved (I.D.F) when consensus if both A and B have been compared
was not reached. against an intervention C (usually
Two reviewers (L.F.N.-S. and J.A.-R.) a placebo). Second, the combination
performed independently and in of direct and indirect comparisons
duplicate the screening of available Pairwise Meta-analysis
allows researchers to obtain more
titles and abstracts to assess their We performed a pairwise random- precise estimates (ie, narrower
eligibility. Studies were retrieved in effects meta-analysis of each confidence intervals or credible
full text if either one of the reviewers available direct comparison. intervals in the results).16 With
considered them eligible. Potentially Treatment effects were estimated an NMA, we can obtain an effect
eligible studies were reviewed, and using odds ratios (ORs) for estimate to determine the differences
studies were included if both dichotomous outcomes and mean between any pair of interventions,
reviewers agreed on their eligibility. differences (MDs) for continuous even if they have not been directly
In case of disagreement, a third outcomes, along with their 95% compared, and summarize all
reviewer (I.D.F.) resolved it. We tried credible intervals (CIs). We used the available evidence in one
to contact authors of primary studies vague priors for all model parameters single study.
during data extraction for missing and a common half-normal prior
information. distribution for the between-study For each outcome and a connected
SD (t∼N [0,1], t . 0) across all network of studies, we performed
Data Extraction treatment comparisons per outcome, a Bayesian random-effects NMA if the
We used a prespecified and piloted given that many treatment assumptions of between-study
form to extract the data. Among the comparisons were informed by homogeneity, transitivity, and
extracted data were study single studies (20). Heterogeneity incoherence across treatment
characteristics (design, year, duration in pairwise meta-analysis for all the comparisons were judged to be
of follow-up, sample size, setting); direct comparisons was quantified justifiable. Transitivity17 is the
patient characteristics (age, impatient with the statistic for heterogeneity assumption that an indirect
or outpatient, days of disease, in direct comparisons (I2) expressed comparison is a valid method to
hydration status); intervention details as a percentage of variability that is compare 2 treatments because the
(doses, administration forms); and due to true differences between studies are sufficiently similar in
outcome results (number of events, studies rather than sampling error.15 important clinical and methodological
mean and SD or SEs, per arm) at the All analyses were performed by using characteristics, or in other words,
longest duration of follow-up. Two the Markov chain Monte Carlo they are similar in their distributions
reviewers (L.F.N.-S. and J.A.-R.) method. A geometry plot was used to of effect modifiers.18 Incoherence
independently and in duplicate present all the available direct (also called inconsistency) is defined
conducted data extraction. When comparisons per outcome, in which as the statistical difference between
consensus was not reached, a third each node represents one direct and indirect treatment
reviewer was involved (I.D.F). intervention. effects.19
Downloaded from www.aappublications.org/news by guest on July 13, 2021
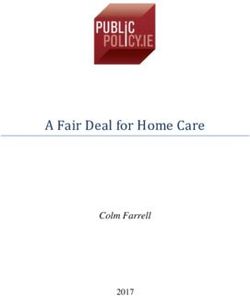
PEDIATRICS Volume 145, number 4, April 2020 3In the absence of direct evidence for Our hypotheses were as follows: Summary and Certainty of the
a given comparison, we indirectly the effect of the interventions Results
estimated treatment effectiveness might be inferior with oral With the aim of optimizing results
and safety. In the presence of both medication (versus intravenous) in interpretation and clinical
direct and indirect evidence, the NMA children with .4 episodes of applicability, we present a summary
provided a combined effect vomiting per hour (versus ,4 using a novel approach that has been
estimate.20 A Bayesian hierarchical episodes) or when outcomes are previously described to summarize
model with vague priors adjusting for measured .12 hours after the results from NMA.35 We grouped the
correlation of multiarm trials was recruitment (versus ,12 hours). interventions according to the
fitted. After discarding the first magnitude of the effect in comparison
10 000 iterations, series of When 10 or more studies were to a placebo and the quality of
100 000 burn-in simulations with available for an outcome, we evidence (according to the GRADE
thinning of 10 values were used to assessed small-study effects and approach). The different categories
allow convergence. The model publication bias using the (marked by different colors) are
convergence was checked by visual comparison-adjusted funnel plot,24 displayed in Fig 1. Dark colors
inspection of the evaluation of the which was used to inform the represent interventions with
mixing of 2 chains. The analysis was Grading of Recommendations, moderate- to high-quality evidence
performed in OpenBUGs (version Assessment, Development, and (high certainty on the results). Light
3.2.3).21 Evaluation (GRADE) assessment colors represent interventions with
(see Rating the Confidence in the very low– to low-quality evidence
Variables used for the assessment of
Effect Estimates section below). We (low certainty on the results).
the transitivity assumption included
calculated the surface under the
the mean number of vomiting before
cumulative ranking (SUCRA) curve
recruitment (fewer or .4 episodes
values to rank the available RESULTS
per hour), the follow-up time of
treatments according to their efficacy,
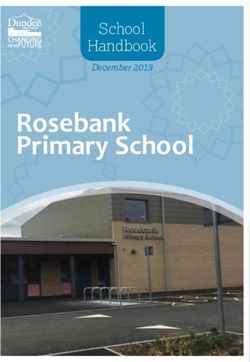
outcome measurement (less than and Selection, Characteristics, and RoB
and we captured the uncertainty
.12 hours), and the route of of Studies
in the parameter values that
administration (intravenous or oral).
informed treatment rankings We identified 3196 titles from
The statistical incoherence between
calculating their corresponding 95% databases and 4 additional records
the direct and indirect estimates was
CI.25-27 We graphically depicted the through other sources. After
assessed with both a global x2 test by
SUCRA curve values for all outcomes removing duplicates, 1840 titles and
using the random-effects design-by-
in a rank-heat plot.28 abstracts were screened. Sixty-six
treatment interaction model22 and
studies were identified for full-text
a local z test by using the loop-
screening. We excluded 42 studies
specific approach calculating the ratio Rating the Confidence in the Effect because of reasons presented in
of OR.23 Estimates Supplemental Table 4 and included
We conducted meta-regression, Reviewers (L.F.N.-S. and J.A.-R.), in 24 RCTs36–59 enrolling 3482 children.
sensitivity, and subgroup analyses pairs and independently, assessed In Supplemental Table 5, we describe
to explore the potential sources of the quality of evidence for each the characteristics of included
heterogeneity and incoherence. reported outcome according to studies. The flow diagram of the
Meta-regression was performed by the GRADE approach.19 Any study selection is shown in Fig 2. The
using the number of vomiting disagreement was resolved by eligible studies were conducted in 16
episodes before the recruitment a third reviewer (I.D.F.). We rated countries from 5 continents. The
as the independent variable. Three confidence as high, moderate, low, or mean number of vomiting episodes
sensitivity analyses were conducted very low. The direct comparisons before recruiting was 7.09 (SD =
on the basis of the RoB, excluding assessment was based in 5 4.28) and the age of children across
studies with (1) overall high RoB, categories: study limitations (RoB),29 the studies was 35.1 months (SD =
(2) high RoB because of allocation imprecision,30 inconsistency,31 24.3; range: 5.2–120.6). The
concealment, and (3) high RoB indirectness,32 and publication bias.33 interventions studied were
because of incomplete outcome. For NMA, the approaches by Puhan metoclopramide, ondansetron,
Lastly, we performed three et al19 and Brignardello-Petersen domperidone, dexamethasone,
subgroup analyses for route et al34 were applied. These consider, dimenhydrinate, and granisetron,
of administration, vomiting number in addition, the assessment of mostly compared against a placebo.
before recruitment, and time of intransitivity and incoherence The search did not retrieve studies on
follow-up for outcome measurement. criteria. alizapride. The network geometry
Downloaded from www.aappublications.org/news by guest on July 13, 2021
4 NIÑO-SERNA et alincoherence was found with the
global assessment (P = .95). The loop-
specific approach also revealed no
statistically significant incoherence,
but the high ratio of OR may suggest
that some degree of incoherence
exists (Supplemental Fig 6).
Ondansetron was the best
intervention measured with the
SUCRA values (SUCRA = 1.0)
(Supplemental Table 8). Forest plots
and funnel plots are displayed in
Supplemental Figs 7 and 8,
respectively.
In the meta-regression analysis
using the number of vomiting
before recruitment as a covariate,
a marginally significant coefficient
was obtained (b = 0.24; CI = 0.01
to 0.48; on log OR scale)
(Supplemental Table 9). In the
subgroup analysis by route of
administration, in comparison to
the placebo, both oral (placebo
versus ondansetron; OR = 0.34
[CI = 0.17 to 0.67]) and intravenous
ondansetron (placebo versus
ondansetron; OR = 0.21 [CI = 0.07
FIGURE 1 to 0.53]) were found to be effective
Categories for summarizing results based on quality of the evidence and effect estimates. Inter- (Supplemental Table 10). In the
ventions are categorized from the most effective to the least effective on the basis of the NMA effect
estimates and the quality of the evidence for the comparison of the intervention versus placebo.
subgroup analyses by severity of
the episodes, only ondansetron was
better than the placebo (placebo
plots with the available direct all comparisons except for the versus ondansetron; OR = 0.32
comparisons for the 6 outcomes are placebo-dimenhydrinate comparison [CI = 0.18 to 0.56]), than
shown in Fig 3. (I2 = 53.5%). Ondansetron was found domperidone (domperidone versus
to be better than metoclopramide, ondansetron; OR = 0.34 [CI = 0.14
Among the included studies, 6 (25%) to 0.90]), and better than
dexamethasone, and placebo in direct
revealed concerns for high RoB due to metoclopramide (metoclopramide
meta-analyses. The remaining
allocation concealment and blinding versus ondansetron: OR = 0.31 [CI =
treatment comparisons revealed no
of participants and/or outcome 0.1 to 0.83]) in the subgroup of ,4
statistical differences (Supplemental
assessors. Five studies had high RoB episodes per hour. We found no
Table 7).
because of incomplete outcome differences in the subgroup of .4
reporting and 5 studies because of episodes per hour. In the subgroup
In the NMA, we obtained 21 paired
inadequate sequence generation. The analysis by time of follow-up,
effect estimates. Ondansetron
RoB assessment is described in ondansetron was similarly effective,
revealed the largest effect in
Supplemental Table 6. although the effect was larger when
comparison to the placebo (placebo
versus ondansetron; OR = 0.28 [CI = follow-up was ,12 hours than when
Cessation of Vomiting 0.16 to 0.46]) with a high quality of follow-up was .12 hours
We conducted pairwise meta- evidence. Ondansetron was also (Supplemental Table 10). Three
analyses in 10 direct comparisons better than metoclopramide sensitivity analyses based on the RoB
(2627 patients) for cessation of (ondansetron versus were performed; ondansetron
vomiting. According to the I2 result, metoclopramide; OR = 3.27 [CI = 1.20 maintained its effect across all the
heterogeneity was low to medium in to 9.19]) (Supplemental Table 7). No analyses (Supplemental Table 11).
Downloaded from www.aappublications.org/news by guest on July 13, 2021
PEDIATRICS Volume 145, number 4, April 2020 514.5]) (Supplemental Table 15). In
the subgroup of ,4 episodes of
vomiting per hour, only ondansetron
was more effective than the placebo
(placebo versus ondansetron; OR =
2.06 [CI = 1.18 to 3.8]). We found no
differences when vomiting frequency
was .4 episodes per hour. Lastly,
ondansetron revealed to be effective
when follow-up was .12 hours after
the intervention (placebo versus
ondansetron; OR = 2.27 [CI = 1.08 to
5.55]) (Supplemental Table 15).
Ondansetron maintained its effect
across all the sensitivity analyses on
the basis of different RoB criteria
(Supplemental Table 16). In Fig 4, we
display the league table with all the
NMA effect estimates for both
primary outcomes.
Secondary Outcomes
We analyzed 10 comparisons (1544
patients) that measured the need for
intravenous rehydration. In the
pairwise meta-analysis, ondansetron
FIGURE 2 was better than metoclopramide
PRISMA flow diagram of study selection. For more information, visit www.prisma-statement.org. (ondansetron versus
Adapted from Moher D, Liberati A, Tetzlaff J, Altman DG; The PRISMA Group. Preferred Reporting metoclopramide; OR = 0.03 [CI = 0.00
Items for Systematic Reviews and Meta-Analyses: the PRISMA statement. PLoS Med. 2009;6(7):
to 0.46]) and better than the placebo
e1000097.
(placebo versus ondansetron; OR =
3.22 [CI = 2.02 to 5.43])
Hospitalization We found no incoherence with the
(Supplemental Fig 12). In the NMA,
Thirteen studies provided global test (P = .21) or the loop-
ondansetron revealed the greatest
information on hospitalization rates specific approaches (Supplemental effect in comparison to the placebo
(2008 patients). In the pairwise meta- Fig 9). The SUCRA values, forest plots, (placebo versus ondansetron; OR =
analyses, ondansetron was better and funnel plot are displayed in 3.0 [CI = 1.9 to 5.1]; moderate
than domperidone (domperidone Supplemental Table 13 and quality) (Supplemental Fig 13).
versus ondansetron; OR = 2.72 [CI = Supplemental Figs 10 and 11, Ondansetron was also more effective
respectively. than metoclopramide (ondansetron
1.56 to 5.89]) and better than the
placebo (placebo versus ondansetron; versus metoclopramide; OR 0.02 [CI =
In the meta-regression analysis using
OR = 3.63 [CI = 1.16 to 21.3]). 0.00 to 0.48]; moderate quality)
the number of vomiting episodes
Heterogeneity was low in all the (Supplemental Table 17). The
before recruitment as a covariate, we
comparisons except for the incoherence, SUCRA values, and
found no association (b = 20.04 [CI =
domperidone-ondansetron funnel plot for the outcome need for
20.24 to 0.15]; on log OR scale)
comparison (I2 = 65.9%). In the NMA, intravenous rehydration are
(Supplemental Table 14). In the
ondansetron was better than the displayed in Supplemental Fig 14,
subgroup analysis by route of
placebo (placebo versus ondansetron; Supplemental Table 18, and,
administration, the placebo compared
Supplemental Fig 15, respectively.
OR = 2.93 [CI = 1.69 to 6.18]) and to oral ondansetron was found
also better than domperidone effective (placebo versus Seventeen studies reported the
(domperidone versus ondansetron; ondansetron; OR = 3.29 [CI = 1.65 to number of vomiting episodes (2504
OR = 3.31 [CI = 1.21 to 15.8]). The 8.56]) in contrast to intravenous patients). In the direct meta-analysis,
remaining comparisons revealed no ondansetron (placebo versus ondansetron was better than the
differences (Supplemental Table 12). ondansetron; OR = 2.19 [CI = 0.44 to placebo (placebo versus ondansetron;
Downloaded from www.aappublications.org/news by guest on July 13, 2021
6 NIÑO-SERNA et alFIGURE 3
NMA plots. A, Vomit cessation. B, Hospitalization. C, Revisit to the ED. D, Intravenous rehydration. E, Number of vomits. F, Side effects. The nodes are
proportional to the number of patients included in the corresponding treatments, and the edges are weighted according to the number of studies in the
comparisons.
MD = 1.46 [CI = 0.74 to 2.63]) and ondansetron (I2 = 89.1%), placebo ondansetron; MD = 1.48 [CI = 0.81 to
granisetron was more effective than versus domperidone (I2 = 80.6%), 2.62]; very low quality). No
the placebo (placebo versus and placebo versus dimenhydrinate incoherence was found with the
granisetron; MD = 0.60 [CI = 0.11 to (I2 = 43.4%) (Supplemental global or the local assessment (P =
1.09]) (Supplemental Fig 16). Table 19). In the NMA, only .99) (Supplemental Fig 17). The
Heterogeneity was low except for the ondansetron was more effective than SUCRA values, forest plots of NMA,
comparisons of the placebo versus the placebo (placebo versus and funnel plot for number of
FIGURE 4
League table. Results are presented as OR and their corresponding 95% CI. The table should be read from left to right. For vomiting cessation, an OR .1
favors cessation of vomiting. For hospitalization, an OR ,1 favors fewer hospitalizations. Significant results are marked with an asterisk. The colors
represent the certainty of evidence: dark green: high; light green: moderate; light yellow: low; and light red: very low.
Downloaded from www.aappublications.org/news by guest on July 13, 2021
PEDIATRICS Volume 145, number 4, April 2020 7vomiting episodes are displayed in
Supplemental Table 20 and
Supplemental Figs 18 and 19,
respectively.
Twelve studies had information about
the revisiting (1763 patients). In the
pairwise meta-analysis, the placebo
was better than granisetron (placebo
versus granisetron; OR = 0.31 [CI =
0.09 to 0.87]) (Supplemental Fig 20).
In the NMA, none of the interventions
revealed differences to the placebo
(Supplemental Table 21;
Supplemental Fig 21). The
incoherence, SUCRA values, and
funnel plot for revisiting are
displayed in Supplemental Fig 22,
Supplemental Table 22, and
Supplemental Fig 23, respectively.
In 12 studies, the authors reported
side effects (1816 children, 5
treatments). In 4 studies, the authors
reported that no side effects were
found. In the NMA, dimenhydrinate
was the only intervention that
revealed significantly more side
effects than the placebo, including
somnolence, sleepiness, sedation, and
drowsiness (placebo versus
dimenhydrinate; OR = 0.14 [CI = 0.01
to 0.7]; very low quality)
(Supplemental Table 23;
Supplemental Figs 24 and 25). The FIGURE 5
incoherence analyses, SUCRA values, Summary of results for all outcomes. NMA results are sorted on the basis of GRADE certainty of
evidence for the comparisons of active treatments versus placebo for all outcomes (see the
and funnel plot for side effects are Methods section and Fig 1 for more details about the categories). Effect estimates are presented in
displayed in Supplemental Fig 26, the last column as OR (for dichotomous outcomes, such as cessation of vomiting, hospitalization,
Supplemental Table 24, and intravenous rehydration, revisit to the ED, and side effects) or MD (for continuous outcomes such as
vomiting number and diarrheal episodes) and their corresponding 95% CI. a NMA estimates: OR (95%
Supplemental Fig 27, respectively.
CI). b NMA estimates: MD (95% CI).
Regarding diarrhea, domperidone
revealed a reduction of the number of Supplemental Fig 31, respectively. A as the “best intervention.” The best
stools in comparison to ondansetron rank-heat plot summarizing the intervention category means that,
in the pairwise meta-analysis ranking statistic across all with high certainty, ondansetron was
(domperidone versus ondansetron; interventions and outcomes is better than placebo and also better
MD = 21.25 [CI = 21.34 to 21.15]) displayed in Supplemental Fig 32. than at least one of the other
(Supplemental Fig 28) and in the
interventions. For cessation of
NMA (dimenhydrinate versus In Fig 5, we summarize the results on
vomiting and the need for
ondansetron; MD = 22.04 [CI = 23.9 the basis of the effect estimates and
intravenous rehydration, ondansetron
to 20.05]; very low quality) quality of the evidence. With high
(Supplemental Fig 29; Supplemental certainty, we found that for cessation was also better than metoclopramide
Table 25). The incoherence, SUCRA of vomiting, hospitalization (Fig 4 and Supplemental Table 17,
values, and funnel plot for diarrhea prevention and the need for respectively); for hospitalization, it
are displayed in Supplemental Fig 30, intravenous rehydration, ondansetron was also better than domperidone
Supplemental Table 26, and was the only intervention categorized (Fig 4).
Downloaded from www.aappublications.org/news by guest on July 13, 2021
8 NIÑO-SERNA et alFor the same outcomes, the antiemetics. Although these results but in most of the cases, it will not be
remaining interventions were suggest that ondansetron should be clinically significant.
categorized as “similar to placebo” or administered orally and that its effect
as “may be similar to placebo.” The seems to be lower when vomiting is Antiemetics use in children with ADG
similar to placebo category means severe, these findings should be has been controversial. CPGs from
that, with high certainty, studied further. organizations such as the World
metoclopramide, domperidone, Health Organization,5 the National
dexamethasone, granisetron, and Our study is the first NMA that Institute for Health and Care
dimenhydrinate were no different includes all the currently available Excellence,7 and the American
from the placebo. The category may antiemetics used in children with Academy of Pediatrics4 do not
be similar to placebo means that ADG. A previous NMA included only recommend their use. Conversely, the
these interventions, with low 11 studies and studied only European Society for Pediatric
certainty, seem to be similar to the ondansetron, metoclopramide, Gastroenterology, Hepatology, and
placebo. Lastly, ondansetron was granisetron, and dexamethasone.10 In Nutrition CPGs8 recommend
considered similar to the placebo, contrast, we included 24 studies with ondansetron. This disagreement may
with high certainty, for side effects additional evidence from be due to the lack of updated CPGs in
and as may be similar to placebo, dimenhydrinate and ondansetron. We the former organizations that did not
with low certainty, for causing also applied advanced statistical consider recent evidence. Therefore,
diarrhea (Fig 5) techniques to explore causes of our results may be crucial for future
heterogeneity and incoherence, and CPG updates.
we assessed the quality of the
Our study has several strengths. We
DISCUSSION evidence with GRADE. A previous
conducted a comprehensive
Cochrane review9 also summarized
In this systematic review and NMA, systematic review including all the
all the available evidence but only
we evaluated available antiemetics available evidence regardless of the
performed direct comparisons and
for controlling vomiting in children language and publication status of the
therefore did not study differences
with ADG. Moderate to high quality of studies. Our review is based on
among interventions. Despite the
evidence indicates that ondansetron statistical analyses that considered
differences between our work and
is the best intervention for cessation both NMA effect estimates and
previous reviews, we all concluded
of vomiting, preventing probability rankings, including
that ondansetron is most likely the
hospitalization, and the need for subgroup, sensitivity, and meta-
best intervention. Nevertheless, we
intravenous rehydration. There is no regression analyses. This allowed us
can now be more confident in these
evidence to support the use of to explore possible effect modifiers
results because we provide updated
domperidone, dimenhydrinate, and prove the robustness of our
evidence, include more studies and
metoclopramide, alizapride, or results. We used the GRADE to
interventions, and provide more
granisetron for the cessation of appraise the quality of evidence and
precise effect estimates (narrower
vomiting and preventing provided a straightforward
CIs), all of which reduce uncertainty
hospitalizations because they were presentation of our findings (Fig 5),
around the results.
classified as similar or may be similar which summarizes in a single
to placebo in all the effectiveness resource the relative performance of
We found that dimenhydrinate was
outcomes. each intervention per outcome,
the only intervention inferior to the
categorized by the certainty on the
Interestingly, in our subgroup placebo in terms of safety. Regarding
evidence. Lastly, we followed
analyses, we found that the effect of diarrhea, all the interventions
Cochrane13 and International Society
ondansetron seems to be larger when revealed no statistically significant
for Pharmacoeconomics and
used orally (rather than differences against the placebo.
Outcomes Research
intravenously) in children with a low Ondansetron has been previously
recommendations for developing
number of vomiting episodes (,4 associated with an increase in
a rigorous NMA.60
episodes per hour) and when the diarrheal episodes. In our results, we
hospitalization outcome was found that ondansetron increases However, our study is not free of
measured after 12 hours. Meta- diarrhea in comparison to limitations. The evidence in most
regression revealed a significant dimenhydrinate but not in treatment comparisons is of low or
coefficient in cessation of vomiting, comparison to the placebo. very low quality. This is the result of
meaning that the larger the number Ondansetron may have a slight the presence of a significant RoB and
of vomiting episodes before impact on the number of stools that imprecise estimates. The latter is
recruitment, the lower the effects of require monitoring in some children, explained by the lack of enough
Downloaded from www.aappublications.org/news by guest on July 13, 2021
PEDIATRICS Volume 145, number 4, April 2020 9evidence from direct comparisons makers may consider ondansetron ACKNOWLEDGMENT
among the interventions given that as the standard of therapy and We thank Jesenia Avendaño, a health
most of the evidence comes from facilitate the decision-making sciences librarian, for her assistance
comparisons against placebo. process about what interventions in the design of the search strategy.
Our results may be beneficial for should be funded in health
clinicians, researchers, guideline benefit plans or for reimbursement
developers, and decision-makers. policies. ABBREVIATIONS
Clinicians count with updated ADG: acute diarrhea and
evidence to support the use of gastroenteritis
ondansetron, which is the only CI: credible interval
intervention with moderate- to CONCLUSIONS CPG: clinical practice guideline
high-quality evidence that supports Ondansetron is the only ED: emergency department
its use in children with ADG and intervention that, with moderate to GRADE: Grading of
vomiting. Considering the amount high certainty, showed an effect on Recommendations,
of evidence and its quality, when cessation of vomiting, Assessment, Development,
designing new trials, researchers hospitalization prevention, and the and Evaluation
should consider comparing new need for intravenous rehydration. I2: statistic for heterogeneity in
alternatives against ondansetron There is no evidence to support the direct comparisons
rather than against a placebo. use of metoclopramide, MD: mean difference
Guideline developers may use dimenhydrinate, domperidone, NMA: network meta-analysis
our results for future CPG updates. alizapride, and dexamethasone in OR: odds ratio
CPGs that have not recommended these patients. Ondansetron was ORT: oral rehydration therapy
antiemetics may want to consider found to be a safe intervention, RCT: randomized clinical trial
ondansetron as an alternative in whereas dimenhydrinate was the RoB: risk of bias
children at risk for failure of oral only intervention that produced SUCRA: surface under the
rehydration and to prevent more side effects than the cumulative ranking
hospitalization. Finally, decision- placebo.
This trial has been registered with the PROSPERO International Prospective Register of Systematic Reviews (https://www.crd.york.ac.uk/PROSPERO) (identifier
CRD42016035236).
DOI: https://doi.org/10.1542/peds.2019-3260
Accepted for publication Jan 22, 2020
Address correspondence to Ivan D. Florez, MD, MSc, Department of Pediatrics, Hospital Universitario San Vicente Fundación, Pabellón Infantil, Calle 64 N°51 D - 154;
Medellín, Colombia. E-mail: ivan.florez@udea.edu.co
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2020 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
FUNDING: No external funding.
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
REFERENCES
1. Black RE, Morris SS, Bryce J. Where and Lancet. 2013;381(9867):628]. Lancet. Provisional Committee on Quality
why are 10 million children dying every 2012;380(9859):2095–2128 Improvement. Practice parameter: the
year? Lancet. 2003;361(9376):2226–2234 management of acute gastroenteritis in
3. Schnadower D, Finkelstein Y, Freedman
young children. Pediatrics. 1996;97(3):
2. Lozano R, Naghavi M, Foreman K, et al. SB. Ondansetron and probiotics in the 424–435
Global and regional mortality from 235 management of pediatric acute
causes of death for 20 age groups in gastroenteritis in developed countries.
5. World Health Organization. The
Curr Opin Gastroenterol. 2015;31(1):1–6
1990 and 2010: a systematic analysis Treatment of Diarrhoea: A Manual
for the Global Burden of Disease Study 4. American Academy of Pediatrics; for Physicians and Other Senior
2010 [published correction appears in Subcommittee on Acute Gastroenteritis; Health Workers, 4th ed. Geneva,
Downloaded from www.aappublications.org/news by guest on July 13, 2021
10 NIÑO-SERNA et alSwitzerland: World Health Organization; 14. Akl EA, Sun X, Busse JW, et al. Specific 26. Veroniki AA, Straus SE, Rücker G, Tricco
2005 instructions for estimating unclearly AC. Is providing uncertainty intervals in
reported blinding status in randomized treatment ranking helpful in a network
6. Chow CM, Leung AK, Hon KL. Acute
trials were reliable and valid. J Clin meta-analysis? J Clin Epidemiol. 2018;
gastroenteritis: from guidelines to real
Epidemiol. 2012;65(3):262–267 100:122–129
life. Clin Exp Gastroenterol. 2010;3:
97–112 15. Higgins JPT, Thompson SG. Quantifying 27. Trinquart L, Attiche N, Bafeta A, Porcher
heterogeneity in a meta-analysis. Stat R, Ravaud P. Uncertainty in treatment
7. National Collaborating Centre for rankings: reanalysis of network meta-
Med. 2002;21(11):1539–1558
Women’s and Children’s Health (UK).. analyses of randomized trials. Ann
Diarrhoea and Vomiting Caused by 16. Al Khalifah R, Florez ID, Guyatt G,
Intern Med. 2016;164(10):666–673
Gastroenteritis: Diagnosis, Assessment Thabane L. Network meta-analysis:
and Management in Children Younger users’ guide for pediatricians. BMC 28. Veroniki AA, Straus SE, Fyraridis A,
Than 5 Years. London, United Kingdom: Pediatr. 2018;18(1):180 Tricco AC. The rank-heat plot is a novel
Royal College of Obstetricians and way to present the results from
17. Baker SG, Kramer BS. The transitive
Gynaecologists Press; 2009 a network meta-analysis including
fallacy for randomized trials: if A bests
multiple outcomes. J Clin Epidemiol.
8. Guarino A, Ashkenazi S, Gendrel D, Lo B and B bests C in separate trials, is A
2016;76:193–199
Vecchio AL, Shamir R, Szajewska H; better than C? [published correction
European Society for Pediatric appears in BMC Med Res Methodol. 29. Guyatt GH, Oxman AD, Vist G, et al.
Gastroenterology, Hepatology, and 2003;3(1):23]. BMC Med Res Methodol. GRADE guidelines: 4. Rating the quality
Nutrition; European Society for 2002;2:13 of evidence–study limitations (risk of
Pediatric Infectious Diseases. European bias). J Clin Epidemiol. 2011;64(4):
18. Cipriani A, Higgins JPT, Geddes JR, 407–415
Society for Pediatric Gastroenterology, Salanti G. Conceptual and technical
Hepatology, and Nutrition/European challenges in network meta-analysis. 30. Guyatt GH, Oxman AD, Kunz R, et al.
Society for Pediatric Infectious Diseases Ann Intern Med. 2013;159(2):130–137 GRADE guidelines 6. Rating the quality
evidence-based guidelines for the of evidence–imprecision. J Clin
management of acute gastroenteritis in 19. Puhan MA, Schünemann HJ, Murad MH, Epidemiol. 2011;64(12):1283–1293
children in Europe: update 2014. et al; GRADE Working Group. A GRADE
Working Group approach for rating the 31. Guyatt GH, Oxman AD, Kunz R, et al;
J Pediatr Gastroenterol Nutr. 2014;
quality of treatment effect estimates GRADE Working Group. GRADE
59(1):132–152
from network meta-analysis [published guidelines: 7. Rating the quality of
9. Fedorowicz Z, Jagannath VA, Carter B. correction appears in BMJ. 2015;350: evidence–inconsistency. J Clin
Antiemetics for reducing vomiting h3326]. BMJ. 2014;349:g5630 Epidemiol. 2011;64(12):1294–1302
related to acute gastroenteritis in 32. Guyatt GH, Oxman AD, Kunz R, et al;
children and adolescents. Cochrane 20. Mills EJ, Thorlund K, Ioannidis JPA.
Demystifying trial networks and GRADE Working Group. GRADE
Database Syst Rev. 2011;(9):CD005506 guidelines: 8. Rating the quality of
network meta-analysis. BMJ. 2013;346:
10. Carter B, Fedorowicz Z. Antiemetic f2914 evidence—indirectness. J Clin
treatment for acute gastroenteritis in Epidemiol. 2011;64(12):1303–1310
children: an updated Cochrane 21. Thomas A, O’Hara B, Ligges U, Sturtz S.
Making BUGS open. R News. 2006;6(1): 33. Guyatt GH, Oxman AD, Montori V, et al.
systematic review with meta-analysis GRADE guidelines: 5. Rating the quality
and mixed treatment comparison in 12–17
of evidence–publication bias. J Clin
a Bayesian framework. BMJ Open. 2012; 22. Higgins JPT, Thompson SG, Deeks JJ, Epidemiol. 2011;64(12):1277–1282
2(4):e000622 Altman DG. Measuring inconsistency in
34. Brignardello-Petersen R, Bonner A,
11. Hutton B, Salanti G, Caldwell DM, et al. meta-analyses. BMJ. 2003;327(7414):
Alexander PE, et al; GRADE Working
The PRISMA extension statement for 557–560
Group. Advances in the GRADE approach
reporting of systematic reviews 23. Veroniki AA, Vasiliadis HS, Higgins JPT, to rate the certainty in estimates from
incorporating network meta-analyses Salanti G. Evaluation of inconsistency in a network meta-analysis [published
of health care interventions: checklist networks of interventions. Int correction appears in J Clin Epidemiol.
and explanations. Ann Intern Med. 2015; J Epidemiol. 2013;42(1):332–345 2018;98:162]. J Clin Epidemiol. 2018;93:
162(11):777–784 36–44
24. Chaimani A, Higgins JPT, Mavridis D,
12. Leclercq E, Leeflang MMG, van Dalen EC, Spyridonos P, Salanti G. Graphical tools 35. Florez ID, Veroniki A-A, Al Khalifah R,
Kremer LCM. Validation of search filters for network meta-analysis in STATA. et al. Comparative effectiveness and
for identifying pediatric studies in PLoS One. 2013;8(10):e76654 safety of interventions for acute
PubMed. J Pediatr. 2013;162(3): diarrhea and gastroenteritis in
25. Salanti G, Ades AE, Ioannidis JPA.
629–634.e2 children: a systematic review and
Graphical methods and numerical
13. Higgins JPT, Green S, eds. Cochrane summaries for presenting results from network meta-analysis. PLoS One. 2018;
Handbook for Systematic Reviews of multiple-treatment meta-analysis: an 13(12):e0207701
Interventions. London, United Kingdom: overview and tutorial. J Clin Epidemiol. 36. Yousefi P, Firouzifar M, Motaghedi F.
The Cochrane Collaboration; 2011 2011;64(2):163–171 Metoclopramide versus serum therapy
Downloaded from www.aappublications.org/news by guest on July 13, 2021
PEDIATRICS Volume 145, number 4, April 2020 11in the control of vomiting due to acute Pediatrics. 2002;109(4). Available at: a randomized controlled trial.
viral gastroenteritis in children: www.pediatrics.org/cgi/content/full/ Pediatrics. 2012;129(6):1050–1055
a single-blind randomized clinical trial. 109/4/e62
54. Golshekan K, Badeli H, Rezaieian S,
Journal of Isfahan Medical School.
45. Ramsook C, Sahagun-Carreon I, Kozinetz Mohammadpour H, Hassanzadehrad A.
2013;30(212):1829–1838
CA, Moro-Sutherland D. A randomized Effect of oral ondansetron on
37. Yilmaz HL, Yildizdas RD, Sertdemir Y. clinical trial comparing oral decreasing the vomiting associated
Clinical trial: oral ondansetron for ondansetron with placebo in children with acute gastroenteritis in Iranian
reducing vomiting secondary to acute with vomiting from acute children. Iran J Pediatr. 2013;23(5):
gastroenteritis in children—a double- gastroenteritis. Ann Emerg Med. 2002; 557–563
blind randomized study. Aliment 39(4):397–403 55. Gheini S, Ameli S, Hoseini J. Effect of
Pharmacol Ther. 2010;31(1):82–91
46. Qazi K, BinSalleeh HM, Shah UH, et al. oral dimenhydrinate in children
38. Van Eygen M, Dhondt F, Heck E, Effectiveness of granisetron in with acute gastroenteritis: a clinical
Ameryckx L, Van Ravensteyn H. A controlling pediatric gastroenteritis- trial. Oman Med J. 2016;31(1):
double-blind comparison of related vomiting after discharge from 18–21
domperidone and metoclopramide the ED. Am J Emerg Med. 2014;32(9): 56. Epifanio M, Portela JL, Piva JP, Ferreira
suppositories in the treatment of 1046–1050 CHT, Sarria EE, Mattiello R. Bromopride,
nausea and vomiting in children.
47. Marchetti F, Bonati M, Maestro A, et al; metoclopramide, or ondansetron for
Postgrad Med J. 1979;55(suppl 1):36–39
SONDO (Study ONdansetron vs the treatment of vomiting in the
39. Uhlig U, Pfeil N, Gelbrich G, et al. pediatric emergency department:
DOmperidone) Investigators. Oral
Dimenhydrinate in children with a randomized controlled trial.
ondansetron versus domperidone for
infectious gastroenteritis: J Pediatr (Rio J). 2018;94(1):
acute gastroenteritis in pediatric
a prospective, RCT. Pediatrics. 2009; 62–68
emergency departments: multicenter
124(4). Available at: www.pediatrics.
double blind randomized controlled 57. Danewa AS, Shah D, Batra P,
org/cgi/content/full/124/4/e622
trial. PLoS One. 2016;11(11):e0165441 Bhattacharya SK, Gupta P. Oral
40. Stork CM, Brown KM, Reilly TH, Secreti ondansetron in management of
L, Brown LH. Emergency department 48. Kita F, Hinotsu S, Yorifuji T, et al.
dehydrating diarrhea with vomiting in
treatment of viral gastritis using Domperidone with ORT in the treatment
children aged 3 months to 5 years:
intravenous ondansetron or of pediatric acute gastroenteritis in
a randomized controlled trial. J Pediatr.
dexamethasone in children. Acad Japan: a multicenter, randomized
2016;169:105–109.e3
Emerg Med. 2006;13(10):1027–1033 controlled trial. Asia Pac J Public
Health. 2015;27(2):NP174-NP183 58. Al-Ansari K, Alomary S, Abdulateef H,
41. Roslund G, Hepps TS, McQuillen KK. The Alshawagfa M, Kamal K.
role of oral ondansetron in children 49. Freedman SB, Adler M, Seshadri R, Metoclopramide versus ondansetron
with vomiting as a result of acute Powell EC. Oral ondansetron for for the treatment of vomiting in
gastritis/gastroenteritis who have gastroenteritis in a pediatric children with acute gastroenteritis.
failed oral rehydration therapy: emergency department. N Engl J Med. J Pediatr Gastroenterol Nutr. 2011;
a randomized controlled trial 2006;354(16):1698–1705 53(2):156–160
[published correction appears in Ann
50. Cubeddu LX, Trujillo LM, Talmaciu I, 59. Salma-Kamal SK, Kudagi BL, Bathina P,
Emerg Med. 2008;52(4):406]. Ann Emerg
et al. Antiemetic activity of ondansetron et al. Clinical outcome with single
Med. 2008;52(1):22–29.e6
in acute gastroenteritis. Aliment dose ondansetron versus domperidone
42. Rerksuppaphol S, Rerksuppaphol L. Pharmacol Ther. 1997;11(1):185–191 in paediatric gastroenteritis-our
Randomized study of ondansetron experience. Journal of Medical Science
versus domperidone in the treatment 51. Shah AA. Effect of Oral Ondansetron in
Children Presenting with Acute and Clinical Research. 2015;3(6):
of children with acute gastroenteritis. 6273–6277
J Clin Med Res. 2013;5(6):460–466 Diarrhoeal Illness and Vomiting With
Some Dehydration. Nairobi, Kenya: 60. Jansen JP, Trikalinos T, Cappelleri JC,
43. Rerksuppaphol S, Rerksuppaphol L. University of Nairobi; 2015 et al. Indirect treatment comparison/
Efficacy of intravenous ondansetron to network meta-analysis study
prevent vomiting episodes in acute 52. Hagbom M, Novak D, Ekström M, et al.
questionnaire to assess relevance
gastroenteritis: a randomized, double Ondansetron treatment reduces
and credibility to inform health care
blind, and controlled trial. Pediatr Rep. rotavirus symptoms-a randomized
decision making: an ISPOR-AMCP-NPC
2010;2(2):e17 double-blinded placebo-controlled trial.
Good Practice Task Force report
PLoS One. 2017;12(10):e0186824
44. Reeves JJ, Shannon MW, Fleisher GR. [published correction appears in
Ondansetron decreases vomiting 53. Gouin S, Vo T-T, Roy M, Lebel D, Gravel J. Value Health. 2016;19(1):121].
associated with acute gastroenteritis: Oral dimenhydrinate versus placebo in Value Health. 2014;17(2):
a randomized, controlled trial. children with gastroenteritis: 157–173
Downloaded from www.aappublications.org/news by guest on July 13, 2021
12 NIÑO-SERNA et alAntiemetics in Children With Acute Gastroenteritis: A Meta-analysis
Laura F. Niño-Serna, Jorge Acosta-Reyes, Areti-Angeliki Veroniki and Ivan D. Florez
Pediatrics originally published online March 4, 2020;
Updated Information & including high resolution figures, can be found at:
Services http://pediatrics.aappublications.org/content/early/2020/03/02/peds.2
019-3260
References This article cites 53 articles, 7 of which you can access for free at:
http://pediatrics.aappublications.org/content/early/2020/03/02/peds.2
019-3260#BIBL
Subspecialty Collections This article, along with others on similar topics, appears in the
following collection(s):
Emergency Medicine
http://www.aappublications.org/cgi/collection/emergency_medicine_
sub
Evidence-Based Medicine
http://www.aappublications.org/cgi/collection/evidence-based_medic
ine_sub
Permissions & Licensing Information about reproducing this article in parts (figures, tables) or
in its entirety can be found online at:
http://www.aappublications.org/site/misc/Permissions.xhtml
Reprints Information about ordering reprints can be found online:
http://www.aappublications.org/site/misc/reprints.xhtml
Downloaded from www.aappublications.org/news by guest on July 13, 2021Antiemetics in Children With Acute Gastroenteritis: A Meta-analysis
Laura F. Niño-Serna, Jorge Acosta-Reyes, Areti-Angeliki Veroniki and Ivan D. Florez
Pediatrics originally published online March 4, 2020;
The online version of this article, along with updated information and services, is
located on the World Wide Web at:
http://pediatrics.aappublications.org/content/early/2020/03/02/peds.2019-3260
Data Supplement at:
http://pediatrics.aappublications.org/content/suppl/2020/03/02/peds.2019-3260.DCSupplemental
Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
has been published continuously since 1948. Pediatrics is owned, published, and trademarked by
the American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 2020
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.
Downloaded from www.aappublications.org/news by guest on July 13, 2021You can also read