Analysis of the Effect of Desvenlafaxine on Anxiety Symptoms Associated vs ith Major Depressive Disorder: Pooled Data from 9 Short-Term, Double-blind
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Original Research
Analysis of the Effect of Desvenlafaxine
on Anxiety Symptoms Associated vs^ith
Major Depressive Disorder: Pooled
Data from 9 Short-Term, Double-blind,
Placebo-Controlled Trials
Karen A. Tourian, MD, Qin Jiang, MS, and Philip T. Ninan, MD
ABSTRACT
FOCUS POINTS
Background: This analysis evaluated the
Symptoms of anxiety are commonly associ-
effects of the serotonin-norepinephrine reup- ated with major depressive disorder (MDD).
take inhibitor, desvenlafaxine (administered as Desvenlafaxine is a serotonin-norepineph-
rine reuptake inhibitor approved for the
desvenlafaxine succinate), on anxiety symptoms treatment of MDD.
associated with depression. This post-hoc analysis evaluated the efficacy of
Methods: Data were pooled from 9 random- desvenlafaxine (50-400 mg/day) compared
with placebo in the treatment of anxiety symp-
ized, placebo-controlled, double-blind, 8 week toms associated with MDD, using pooled individ-
studies of desvenlafaxine (50-400 mg/day, fixed ual patient data from 9 short-term, randomized,
or flexible dose) in patients with major depres- double-blind, placebo-controlled clinical trials.
Desvenlafaxine treatment was associated with
sive disorder (MDD), without a primary anxiety significantly greater improvement on measures
diagnosis. Changes from baseline in scores on of anxiety compared with placebo in outpatients
with a primory diognosis of MDD.
the anxiety/somatization factor of the 17-item
Hamilton Rating Scale for Depression (HAM-D17)
and on the Covi Anxiety Scale at the final eval- cebo, n=1,108]), desvenlafaxine was associated
uation (last observation carried forward) were with significantly greater reductions compared
compared between desvenlafaxine and placebo with placebo in scores on the HAM-Diy anxi-
groups using analysis of covariance. ety/somatization factor (-3.41 vs -2.92, P
Original Research
differences were observed for all dose groups it is expected that treatment with des-
on the HAM-D17 anxiety/somatization factor venlafaxine will result in significant improvement
of anxiety symptoms associated with MDD. The
(Ps.OII), and for the 50, 100, and 200 mg/day
objective of this post hoc analysis of pooled short-
dose groups on the Covi Anxiety Scale {all term studies was to compare the efficacy of des-
Ps.O15 vs placebo). venlafaxine and placebo in reducing symptoms
of anxiety in outpatients with a primary diagnosis
Conclusions: Desvenlafaxine was associ-
of MDD. The effects of baseline anxiety on overall
ated with significantly greater improvement in treatment outcomes and the relationship between
anxiety symptoms connpared with placebo in improvement in anxiety symptoms and remission
were not evaluated in this analysis.
patients with MDD.
CNS Spectr. 2010;15(3):187-193
METHODS
INTRODUCTION Study Design
Although major depressive disorder (MDD) This secondary analysis evaluated the effect
is characterized primarily by depressed mood of desvenlafaxine on anxiety symptoms in adult
and a loss of interest or pleasure in daily activi- outpatients with MDD using pooled data from 9
ties, many cases also are accompanied by some short-term, randomized, double-blind, placebo-
symptoms of anxiety\- -50% of cases in the controlled, multicenter studies of desvenlafaxine.
Sequenced Treatment Alternatives to Relieve These phase II and III clinical trials comprise the
Depression (STAR*D) study met criteria for anx- portfolio of the US Food and Drug Administration
ious depression (defined as a score of >7 on registration studies for the treatment of MDD (Table
the anxiety/somatization factor of the Hamilton 12125,29) ^11 studies were approved by an inde-
Rating Scale for Depression [HAM-D]).^^ The pendent ethics committee or institutional review
coexistence of anxiety symptoms, especially board, were conducted in accordance with the eth-
severe anxiety, increases the severity of depres- ical principles in the Declaration of Helsinki, and
sive illness and worsens functional impairment.
were consistent with Principles of Good Clinical
In some reports,^^ but not all,^' anxious depres-
Practice and applicable regulatory requirements.
sion decreased the likelihood of response or
All studies included in this pooled analysis had
remission, and/or increased the time to achieve
similar study designs and patient samples.
response or remission with treatment for MDD,
which underscores the importance of treating
both depression and MDD-associated anxiety. Study Patients
To be eligible for inclusion in any of the 9 tri-
A significant overlap exists in pathophysiologic als, outpatients (218 years of age) were required
components of depression and anxiety, and treat- to have a primary diagnosis of nonpsychotic
ment of both.^ Antidepressants from a variety of MDD based on the Diagnostic and Statistical
classes, particularly selective serotonin reuptake Manual of Mental Disorders, Fourth Edition^°
inhibitors and serotonin-norepinephrine reuptake criteria, with depressive symptoms that had
inhibitors (SNRIs), are effective in treating anxiety been present for at least 1 month. Patients had
disorders^ '^ in addition to treating symptoms of to have a current, moderate to severe depressive
anxiety associated with MDD.* '^'^ episode at both screening and baseline. Criteria
Desvenlafaxine (administered as desvenla- for severity of depression included a 17-item
faxine succinate), the active metabolite of venla- HAM-D^^ total score 220 (4 studies) or a22 {2
faxine, is an SNRI approved in the United States studies) or a Montgomery Asberg Depression
for the treatment of MDD.'^'^° Several phase III, Rating Scale^^ score 2r24 {1 study); HAM-Di7 item
randomized, placebo-controlled, double-blind 1 (depressed mood) score z2; and Clinical Global
studies have established the efficacy, safety, and Impressions-Severity scale^^ total score &4; in 8
tolerability of desvenlafaxine in treating MDD in of the 9 studies, patients were required to have a
adult outpatients.^^ ^^ Covi Anxiety Scaie^"* score ^3 on any single item,
Based on the established efficacy of other and a Covi Anxiety Scale total score ^9 and less
SNRIs in the treatment of anxiety symptoms than the Raskin Depression Scate^^ total score.
associated with MDD or primary anxiety disor- Patients were excluded from eligibility for any
CNS Spectr 15:3 188 March 2 0 1 0
Original Research
of the 9 trials if they had a current W\2 months items 10 [anxiety/psychic], 11 [anxiety/somaticl,
before baseline) primary diagnosis of an anxiety 12 [somatic/gastrointestinal], 13 [somatic/gen-
disorder (eg, generalized anxiety disorder, social eral], 15 [hypochondriasis], and 17 [insight]) score,
anxiety disorder, or panic disorder). All patients the HAM-D17 anxiety-psychic item score, and
provided written, informed consent. the Covi Anxiety Scale total score. The HAMD-ij
was administered in all 9 studies at baseline and
Treatments weeks 1, 2, 3, 4, 6, and 8. The Covi Anxiety Scale
Eligible patients were randomly assigned to was administered in 8 of 9 studies at baseline and
receive desvenlafaxine at doses ranging from weeks 2, 4, and 8; this scale was not administered
50-400 mg/day {n=1,805) or placebo (n=1,108). in the phase 2 study {Table 1).
Four studies used a flexible-dose regimen of des-
venlafaxine 100-400 mg/day (100-200 mg/day Statistical Analysis
[1 study]; 200-400 mg/day [3 studies]}; 5 studies Data from the intent to treat {ITT) population
used a fixed dose desvenlafaxine regimen (50 were analyzed. The ITT population included
mg/day, 2 studies; 100 mg/day, 3 studies; 200 mg/ patients who had a baseline evaluation, al dose
day, 3 studies; and 400 mg/day, 3 studies) {Table of study medication, and &1 HAM-D17 evalua-
1). Data from patients assigned to receive venla- tion after receiving dose 1 of study medication.
faxine extended release 75-226 mg/day {in 2 of Changes from baseline in HAM-D^y anxiety/
the studies) are not described in this report. The somatization factor, HAM-D17 anxiety-psychic
duration of treatment in each study was 8 weeks. item, and Covi Anxiety Scale scores were ana-
lyzed using an analysis of covariance (ANCOVA)
Outcomes model using baseline scores as the covariate,
The efficacy measures for this analysis were adjusted by protocol to test the treatment effect.
the HAM-Di7 anxiety/somatizationfactor^^ (sum of The primary time point was the final evaluation.
TABLE 1 .
Studies Included in Meta-Analysis of Desvenlafaxine in Treating MDD-Related
Symptoms of Anxiety: ITT Population
Desvenlafaxine
Study Desiqn Dose (ma/day) Desvenlafaxine (n) Placebo (n) Total (NI
223'' Phasen,fixed dose 200 63 78 213
400 72
306" Phase III, fixed-dose 100 114 118 461
200 116
400 113
308^' Phase III, fixed-dose 200 121 124 369
400 ^ ^ H^ 124
332'^ Phase III,fixed-dose 50 150 150 447
100 147
333" Phase 111, fixed-dose 50 164 161 483
100 ^
304" Phase III, flexible-dose 100-200 120 114 234
320* Phase III, flexible-dose 200-400 117 118 235
309^^ Phase III, flexible-dose 200^00 116 120 236
317« Phase III, flexible-dose 200^00 110 125 235
Total 1,805 1.108 2,913
' Data on die, Wyelh Research, Collegeville, PA.
MDO-major depressive disorder; ITT=intent to treat
Toiiriaii KA, Jiang Q, Ninan PT. CNS Spectr. Vo\ 15, No 3. 2010
CNS Spectr 15:3 189 March 2010
Original Research using last observation carried forward (LOCF) Efficacy methods for missing data; data from each visit Among all studies and for individual des- (LOCF) were also analyzed. In addition to the venlafaxine dose groups, there was significant analysis of the overall data set, an analysis of improvement from baseline HAM-Di7 anxiety/ data from the subset of fixed-dose studies was somatization factor score at the final evaluation conducted to evaluate the efficacy of each dose compared with placebo (Ps.011; Figure 1). In of desvenlafaxine. Cohen's d effect sizes were the overall data set, significant improvement calculated based on the mean change from base- was apparent by week 3 (P

Original Research chic item were -0.27 for the overall data set and group (P=.OO9) and by week 8 for the 50 mg/day were -0.29, -0.34, -0.35, and -0.35 for the 50, 100, dose group (P

Original Research
mately -3.0 to -4.0 and the magnitude of the augmenting an ineffective or intolerable treat-
difference between drug and placebo (approxi- ment.^ This finding demonstrates that It is critical
mately -0.5) on the HAM-Di7 anxiety/somatiza- to recognize anxious depression and to choose
tion factor reported here, are similar to or greater treatment options accordingly. An analysis of
than those observed after 6-8 weeks of treat- pooled data from clinical trials of venlafaxine in
ment with other SNRIs, such as venlafaxine.^^ MDD suggests that significant improvement in
Although this analysis demonstrated statistically anxiety symptoms may be achieved as early as
significant differences between desvenlafaxine the first week of treatment and early resolution of
and placebo, the results should be considered anxiety symptoms may be a predictor of remis-
in light of the large sample size used here, and sion of MDD.'' In this analysis, some dose groups
as such, the clinical significance of these differ- showed a reduction of anxiety symptoms by
ences may be limited. The effect sizes across all week 2 after initiation of treatment with desven-
measures and all desvenlafaxine dose groups of lafaxine (Figures 2 and 5); however, the relation-
-0.14 to -0.35 are in the range generally consid- ship between improvement in anxiety symptoms
ered small to moderate. The recommended 50 and remission was not evaluated.
mg/day dose of desvenlafaxine was associated There are limitations to pooled analyses, one
with an effect size of -0.29 on each measure; this of which is related to study selection.^^ Often
effect size is similar in magnitude to the effect only positive trial results are published^'; the
size of -0.31 for the 50 mg/day dose group deter- exclusion of unpublished data generally results
mined in a previous analysis of overall efficacy in the exclusion of data from negative trials,
based on the primary outcome measure (change thereby skewing the results of the analysis.
in HAM'Di7 total score).^^ However, this analysis included published and
The utility of desvenlafaxine in treating anxiety unpublished data from all 9 short-term, pla-
symptoms that accompany MDD is a particularly cebo-controiled, registration studies of desven-
pertinent measure in light of recent data from iafaxine in patients with MDD; both positive and
the STAR*D study showing that patients with
anxious depression do not achieve remission as
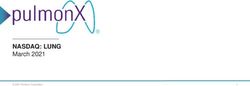
quickly or as frequently compared with patients FIGURE 5.
with non-anxious depression and are likely to Adjusted mean Covi Anxiety Scale
have poorer outcomes after switching from or scores, adjusted means by visit
(LOCF)
^ P l a c e b o (n=1,026l - Oesvenlafaxme 50 mg (n=3I2|
FIGURE 4 . •-Desvenlafaxine 100m9(n=4n) - Desvenlafaxine 200 mg in:232)
Adjusted mean (SE) change fram •— Desvenlataxme 400 mg |n=234) - Dflsvenlafaxme Pooled in-1,6471
baseline in the Covi Anxiety Scale
scores at the final evaluation (LOCF)
P values reflect individual desvenlafaxine dose comparisons with Iheir
respective placebo groups, n=number o) patients in each treatment group
affinal evaluation.
Week 2,*P=.O33 for 200 mg/day; Week 4, tPs.D15 for 200 and 100 mg/dav,
Placebo • Desvenlafsxine ÎP
Original Research
negative studies were included. Differences In the 7 Nelson JC. Anxiety does not predict response to duloxetine in ma]or depcession: results
of a pooled analysis of individual patient data from 11 placebo-controlled trials. Depress
design of the individual studies or characteristics ^nx/eiy. 2010,27:12-18.
of patient samples also may confound the results 8 Keller MB, Kr/stal JH, Hen R, Neumeister A, Simon NM. untangling depression and anxi-
of pooled analyses. However, all of the studies ety: clinical challenges JO/n ftK:teiïv 2005:66:1477-1484.
9 Soomro GM, Altman D. Rajagopal S, OaWey-Brawne M. Selective serotonin re-uptake
included here had similar study designs, and the inhibitors ISSRIsI versus placebo for obsessive compulsive disorder (DCD). Cochrane
characteristics of the patient samples were largely Database Syst Rev. 2008:( 1ICDOOI765.
10 DeirOsso 8, Nestadt G. Alien A, Hofländer E. Serotonin-norepinephrine reuptake
consistent between studies. Nonetheless, the inhibitors in the treatment of obsessive-compulsive disorder A criticai review. J Clin
results from this analysis should be interpreted Psychiatry 2006:67:600-610
within the context of the limitations of such analy- 11 Pollack M, Mangano R, Entsuah R. Tzanis E. Simon NM. Zhang Y A randomwed controlled
trial of venlafaxine ER and paroxetine in the treatment of outpatients with panic disorder
ses in general as well as the design of the indi- Ps^/jopiia™aco/offf(Berl). 2007,194:233-242.
vidual studies included. 12 KatcmWJ Clinicalpractice.Panicdisorder./Vf/jff/JMerf.2O06:354:2360-23S7.
13. Davidson JR Pharmacntherapy of sociai anxiety disorder what does the evidence tell us?
This analysis examined efficacy of desvenla-
faxine in treating anxiety symptoms in patients 14 Fricchione G- Clinical practice. Generalized anxiety disorder N Eng! J Med
2004.351.675-682.
with MDD, not anxiety disorders. In addition, the 15. Balienger JC. Overview of different pharmacotlierapies for attaining remission in general-
studies used in this analysis excluded patients ized anxiety disorder JCT/jftyc/i/aiO'. 2001,62|suppn91:l 1-19
with severe anxiety, primary anxiety disorders, 16. Feighner JP. Entsuah AH, McPhefson MK. Efficacy of once-daily venlafaxine extended
release IXR) for symptoms of anxiety in depressed outpatients. J Affect Disord.
or anxiety that was more prominent than depres- 1998:47:55-62.
sion. Although the results show a significantly 17 MuttOJ.Careofdepressedpattentswithanxietysymptons JClin Psychiatry. ^^SB:60^supp\
171:23-27.
greater response to desveniafaxine compared 18. Papakostas Gl, Trivedi MH, Aipert JE, et al. Efficacy of bupropion and the selective
with placebo in relieving anxiety, no conclusions serotonin reuptake inhibitors in the treatment of anxiety symptoms in major depressive
or inferences can be drawn about the efficacy of disorder: a meta-analysis of individual patient data from 10 double-blind, randomized
clinicaltrials.Jftyctelf fies 2008:42:134-140.
desvenlafaxine compared with other antidepres- 19 Deecher DC, Beyer CE, Johnston G et al. Desvenlafaxine succinate: A new serotonin and
sants. As such, conclusions about relieving symp- norepinepbrine reuptake inhibitor J Pharmacol EKp Ther. 2006:318:657-665.
20. Desvenlafaxine Ipackage inseij Collegeviiie. PA: Wyeth Pharmaceuticals: 2008.
toms of anxiety are applicable only to patients 21 Septien-Veiei L, PitrosiCopyright of CNS Spectrums: The International Journal of Neuropsychiatric Medicine is the property of MBL Communications and its content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written permission. However, users may print, download, or email articles for individual use.
You can also read