An Unusual Presentation of Pulmonary Edema During an Ice Dive at Altitude
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

MILITARY MEDICINE, 188, 1/2:392, 2023
An Unusual Presentation of Pulmonary Edema During an Ice Dive
at Altitude
LCDR Aliye Z. Sanou, DO, MPH, MC, USN*; LCDR Robert L. Murray, MSC, USN*,†;
HMC Eli Hernandez, DWS/EXW/FMF/SW/AW, USN‡; LT David Sherrier, MD, MC, USN§
ABSTRACT Military diving operations occur in a wide range of austere environments, including high-altitude envi-
ronments and cold weather environments; however, rarely do both conditions combine. Ice diving at altitude combines
the physiologic risks of diving, a hypothermic environment, and a high-altitude environment all in one. Careful planning
and consideration of the potential injuries and disease processes affiliated with the aforementioned physiologic risks must
Downloaded from https://academic.oup.com/milmed/article/188/1-2/392/6564824 by guest on 15 March 2024
be considered. In this case report, we describe a Navy diver who became obtunded secondary to hypoxia during an ice
dive at 2,987 m (9,800 ft) elevation and was subsequently diagnosed with high-altitude pulmonary edema. Further con-
sideration of the environment, activities, and history does not make this a clear case, and swimming-induced pulmonary
edema which physiologically possesses many overlaps with high-altitude pulmonary edema may have contributed or
been the ultimate causal factor for the diver’s acute response.
BACKGROUND of HAPE are reported as decreased exercise capacity, dry
A rapid ascent or travel to elevations of 2,500 m (8,000 ft) cough that progresses to tachypnea, tachycardia, productive
or more from the sea level presents humans with the chal- cough with pink frothy sputum, orthopnea, dyspnea at rest,
lenge of decreased ambient partial pressures of oxygen (PO2 ) and hypoxia.7,9
and is associated with the risk of developing different forms High-altitude pulmonary edema (HAPE) is a form of non-
of high-altitude illnesses. Decreased PO2 ultimately affects cardiogenic pulmonary edema due to a failure in the pul-
all aspects of the oxygen transport system to the tissues and monary blood–gas barrier in the setting of hypobaric hypoxia.
as a result complications arise, most commonly acute moun- This failure is the result of many maladaptive physiologic
tain sickness (AMS), high-altitude cerebral edema (HACE), responses; a few of which are exaggerated and nonuni-
and high-altitude pulmonary edema (HAPE).1 While the eti- form pulmonary vasoconstriction, poor hypoxic ventilatory
ology of HAPE is fairly well understood, the pathophysiology response, and inadequate endothelial nitric oxide synthesis.
of pulmonary edema resulting from diving or swimming- At altitude, most persons who are susceptible to HAPE have
induced pulmonary edema (SIPE) has been ambiguous.2,3 a poor hypoxic ventilatory response, leading to a low alveolar
Diving at altitude can confound the symptoms presented for PO2 and therefore a greater stimulus for hypoxic pulmonary
both HAPE and SIPE. vasoconstriction.10 However, hypoxic pulmonary vasocon-
High-altitude illness typically occurs in individuals who striction is nonuniform. This leads to a patchy distribution of
ascend over 2500 m in 24 hours and progresses with symp- the pulmonary edema.1,9 Heavy exercise or exertion itself can
toms of headache; insomnia; gastrointestinal symptoms such contribute to and further increase the risk of pulmonary edema
as anorexia, nausea, vomiting, and diarrhea; and fatigue.4,5 by increasing pulmonary blood flow and exacerbating over
These symptoms attributed most commonly to AMS generally perfusion to sections of the lung, leading to further capillary
resolve with acclimation or decent, but as affected individ- stress and vascular leaking into the lung parenchyma.1,10
uals remain at or ascend in altitude AMS may advance to The treatment for HAPE focuses primarily on descent and
HACE and HAPE.6,7 High-altitude cerebral edema (HACE) supplemental oxygen. When descent is not practical, admin-
is conceptualized as an extreme form and progression of AMS istering supplemental oxygen via nasal cannula or facemask
where additional neurological findings of lethargy, ataxia, or with a goal SpO2 greater than 90% may be a suitable alter-
altered mental status affect the individual.7,8 Early symptoms native to descent.11 Further elaboration of the mechanisms
behind HAPE or its presentation and treatment is beyond the
* Force scope of this report but can be reviewed elsewhere.1,5,7,10,11
Surgeon’s Office, Unit 35605, III Marine Expeditionary Force,
FPO, AP 96382-5605, USA Swimming-induced pulmonary edema (SIPE), also some-
† Uniformed Services University, Bethesda, MD 20814, USA times called scuba dive pulmonary edema, occurs in swim-
‡ Surface Warfare Medical Institute, San Diego, CA 92134, USA mers and divers in cold water, with symptoms similar to
§ Navy Experimental Dive Unit, Panama City Beach, FL 32407, USA
HAPE: dyspnea, chest tightness, cough, hemoptysis, and
The opinions and assertions expressed herein are those of the authors and hypoxia occurring during water submersion with exercise.12
do not reflect the official policy or position of the associations with which The SIPE symptoms last up to 48 hours and typically resolve
they are affiliated, including the Department of Defense.
doi:https://doi.org/10.1093/milmed/usac081 spontaneously. Care is supportive and includes removing
Published by Oxford University Press on behalf of the Association of the stricken patient from water and placing them in a warm
Military Surgeons of the United States 2022. This work is written by (a) US environment. More aggressive therapy includes supplemental
Government employee(s) and is in the public domain in the US. oxygen and inhaled beta-2 agonists. Additionally, continuous
392 MILITARY MEDICINE, Vol. 188, January/February 2023
Pulmonary Edema During an Ice Dive at Altitude
positive airway pressure, nitroglycerine, antibiotics, and pred- snow, setting up heavy equipment, and acclimatizing to the
nisolone have also been used as adjunct therapies.12 area without dives. During the first 3 days at the camp, the
In this case, the first of its kind in published literature, diver noted that he felt more winded than usual with exercise
we report on the difficulties in differentiating the diagnoses and snow shoveling. He was able to engage in these activi-
of HAPE and SIPE in a diver at altitude and propose that ties despite this, and his discomfort was not apparent to his
the pathophysiologic pathways that lead to HAPE and SIPE teammates. He reported a stabbing headache to his medical
may work synergistically, rendering ice divers at altitude provider—an independent duty corpsman (IDC)—the fourth
at an increased risk of either or both types of pulmonary night at camp. His headache was partially relieved by 800 mg
edema. Motrin and completely relieved by the addition of caffeine.
Retrospectively, the diver noted that his headache would
CASE PRESENTATION return throughout his time at the camp and was minimal in
A 27-year-old male active duty Navy diver traveled with daytime and worse at night, causing him periods of insomnia.
Downloaded from https://academic.oup.com/milmed/article/188/1-2/392/6564824 by guest on 15 March 2024
a detachment team from his unit on the Atlantic seaboard He did not endorse mental fog, gastrointestinal symptoms, or
(sea level) to a reservoir in Utah (elevation 2,987 m or dyspnea at rest at any time. Vital signs were taken by the IDC
9,800 ft) for the purpose of training for ice dives (Fig. 1). The on all members of the team at the onset of the camp stay,
team flew in to Las Vegas, NV, altitude 610 m (2,001 ft) and and it was noted that pulse oxygen levels of members were
drove to the reservoir diving site within 24 hours in order to anywhere from 89% to 96% on ambient air.
set up camp. The initial plan to acclimatize and ascend more On the morning of the fifth day at camp, the diver and
slowly over a 5- to 6-day period was altered after snowstorms his dive partner completed an ice dive (Fig. 2). Diving at
on the Atlantic seaboard delayed their westward flight. For the altitude requires using a separate set of calculations for dive
first 3 days at the camp, primary activities included shoveling table decompression due to the reduced atmospheric pressure.
FIGURE 1. Ice dive—overhead view of camp. The tent, at the center of the circle, is the primary entry and exit point for divers.
MILITARY MEDICINE, Vol. 188, January/February 2023 393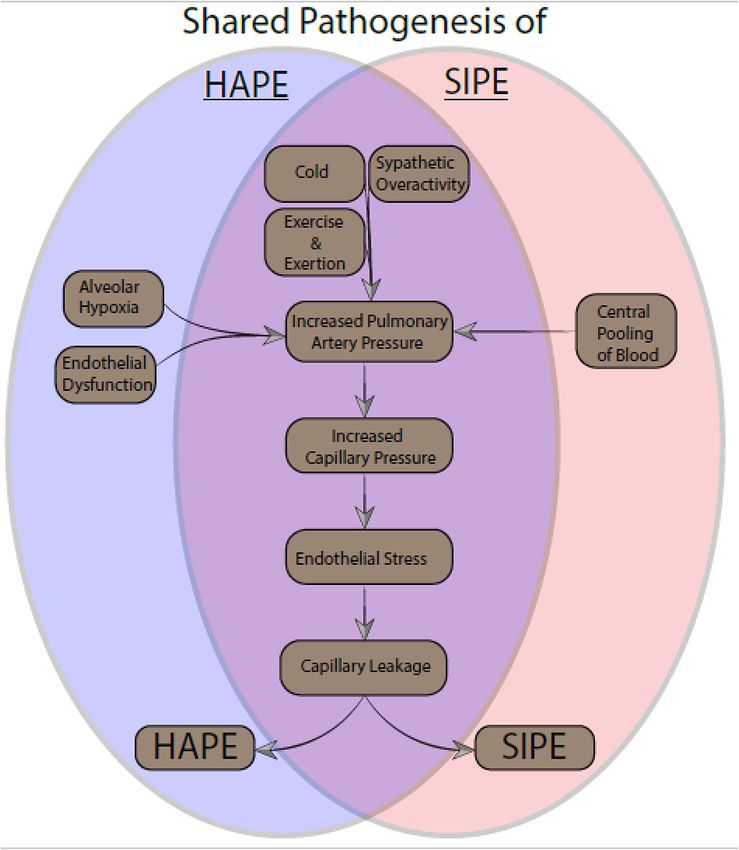
Pulmonary Edema During an Ice Dive at Altitude
To calculate decompression requirements, sea level equivalent water within a minute. His total time underwater for the dive
depth (SLED), also known as the “cross correction” tech- evolution was 20 minutes. At this point the diver experienced
nique, is applied as follows: amnesia. His team noted that he was speaking nonsensically
to his dive partner over the communication system as he was
Equivalent depth (ft seawater) being extracted from the water. At the surface, his facemask
was removed, revealing a cyanotic facial complexion. He was
= Altitude depth (ft seawater)
immediately started on O2 . After less than a minute on a 10-L
Pressure at sea level (1.00 atmosphere) non-rebreather facemask of O2 , the member reported that he
×
Pressure at altitude (atmosphere) could think clearly again. His pulse oxygen (OX) saturation
was noted to be 100% while on non-rebreather after extrac-
tion and resuscitation. His dive unit members remarked that
The altitude environment necessitates divers to have added
he had been breathing heavily during the dive as could be
Downloaded from https://academic.oup.com/milmed/article/188/1-2/392/6564824 by guest on 15 March 2024
decompression to their dives.13 The diver and his partner
heard over the communication system and suspected that his
undertook their first dive to a maximum depth of 15 ft
symptoms were all consistent with a hypoxic event. As per the
(physiologic SLED equivalent 25 ft) without any incident. On
protocol, dive injury was suspected and immediate full neuro-
the morning of the sixth day at camp, the diver and his part-
logic, cardiac, and pulmonary exams were performed, which
ner completed a more strenuous ice dive to a maximum depth
revealed no neurologic or cardiac findings. The pulmonary
of 30 ft (SLED equivalent 45 ft), with finning underwater for
exam was significant for tachypnea, with his respiratory rate
approximately 15 minutes. During this dive, the diver and his
at 20 and pulse ox reading 85% on ambient air after the oxygen
partner returned to the surface to receive equipment and then
mask was removed, but otherwise benign with good inspira-
submerged again and moved approximately 15 ft away from
tory effort and all lung fields clear to auscultation bilaterally.
the ice hole. At that time, the diver reported feeling air hunger
The member endorsed no chest pain, dyspnea, palpitations,
mixed with a feeling of euphoria, anxiety, lightheadedness,
coughing, or air hunger. He endorsed that he felt winded with
headache, and tunnel vision. He immediately signaled his dive
minimal exertion and noted the persistent headache, but other-
partner and his tender that he needed to abort the dive and
wise stated that he was feeling well. His IDC tested the pulse
return to the surface. He was extracted and removed from the
ox machine (only one available) on other team members to see
if it was compromised. Other members had readings between
89% and 94% O2 on ambient air.
The diver was given an albuterol inhaler and Mucinex by
his IDC and continued to be observed closely through the day
and overnight. The next day, he was noted to have a pulse ox
reading that dropped from 85% to 74% on ambient air dur-
ing vigorous walking. An adjunct flight nurse present with
a standby helicopter medevac crew drew an arterial blood
gas, with the notable finding of PO2 of 53 mmHg (refer-
ence range 80-90 mmHg). A repeat cardiopulmonary exam
was conducted by the IDC. Although the member remained
clear to auscultation bilaterally in all lung fields, paradoxi-
cally the IDC reported positive findings for bronchophony,
egophony, tactile fremitus, and whispered pectoriloquy, each
indicating signs of consolidation in the right upper lobe.
FIGURE 2. Ice diver entering the water. One of the two divers entering water, FIGURE 3. (A) and (B) Both lateral and posterior–anterior chest X-rays were
with the umbilical line in the hands of the dive tender. read as unremarkable by radiologist.
394 MILITARY MEDICINE, Vol. 188, January/February 2023Pulmonary Edema During an Ice Dive at Altitude
These paradoxical findings were observed by both the IDC use a commercial flight home in the next 24-48 hours by the
and the flight nurse. At this point, the diver was transported treating physician.
by vehicle to a local emergency room at an altitude of 1,830 m
(6,008 ft) for his persistent hypoxia and findings on physical DISCUSSION
exam. This case focuses on a well-trained and physically conditioned
Upon arrival at the local emergency room after a 30-minute 27-year-old diver who became obtunded during his second
transit by car, the member had a benign physical exam without ice dive at altitude, with relief of symptoms with oxygen and
significant findings. Pulse ox readings were 98% on room air. descent to a lower altitude. Before the patient’s second dive,
Preliminary chest X-ray read by the emergency room physi- he experienced symptoms consistent with AMS: headache
cian and IDC showed mild edema between upper and middle that was worse at night but responsive to caffeine and dyspnea
lobes of the right lung. The emergency room physician inter- with minimal exertion. The acute symptoms experienced by
preted this in the context of the patient’s history as HAPE. the diver during the second dive—euphoria, impaired mem-
Downloaded from https://academic.oup.com/milmed/article/188/1-2/392/6564824 by guest on 15 March 2024
However, the X-ray was read as unremarkable by the radiol- ory, and air hunger are consistent with an acute hypoxic event.
ogist on duty (Fig. 3). The D-Dimer was negative. The diver Ultimately, the diver was diagnosed with HAPE; but given the
was diagnosed with HAPE and started on nifedipine and kept constellation of symptoms and their chronology, the case is
at low altitude for the remainder of the trip. He was cleared to worth revisiting.
FIGURE 4. Shared pathogenesis of HAPE and SIPE. Figure is derived from text and diagrams in Smith et al.3 and Li et al.9
MILITARY MEDICINE, Vol. 188, January/February 2023 395Pulmonary Edema During an Ice Dive at Altitude
The diver was exposed to multiple potentiating factors individuals who have previously ascended or been at altitude
that are shared by both HAPE and SIPE pathophysiologies; many times, despite no history of previous complication.16
these include cold, vigorous exercise, and sympathetic over- Some literature on SIPE cases suggest that once an individ-
activity induced by decreased PO2 . Similarities exist between ual has had one episode, they are more likely to have repeat
the pathophysiologic mechanisms believed to underlie both episodes with cool water or cool air swimming and dives.12
HAPE and SIPE; water immersion and exertion lead to cen- The military experience with special operations reports the
tralized pooling of blood in the cardiovascular unit, elevating opposite—that one episode of SIPE does not predispose to
pulmonary artery pressure.2,3 Patchy or nonuniform areas of further episodes.14 Based on what is known about the patho-
pulmonary vasoconstriction lead to some capillaries experi- physiology and as demonstrated in the reported case here,
encing higher pressure and subsequent leakage.12 Exertion the same physiologic factors are at work, leading to cases of
exacerbates both the work of breathing and airway pressures, HAPE and SIPE that may potentiate each other (see Fig. 4).
resulting in further capillary permeability14 (Fig. 4). These This case illustrates the importance of having dive and swim-
Downloaded from https://academic.oup.com/milmed/article/188/1-2/392/6564824 by guest on 15 March 2024
contributing factors resulted in a pathology common to both ming personnel and their medical attendants understand that
HAPE and SIPE: increased pulmonary artery pressure leading multiple environments may potentiate common pathophys-
to patchy capillary leakage, tachypnea, and eventual dysp- iologies and complicate differential diagnoses. Mitigation
nea and worsening hypoxia. Other diving-specific injuries, strategies and training need to be tailored for each event to
such as decompression sickness or arterial gas embolism, are best support prevention and in case of occurrence, diagnosis
unlikely in this case, given his dive profile and that the onset of and treatment.
symptoms occurred at depth. The possibility of either hypo-
or hypercapnia combined with hypoxia should be considered. FUNDING
Hypocapnia is more likely, given heavy breathing was heard There was no funding received for this case report.
over the communication system and hyperventilation is com-
mon in cold-water diving. When combined with hypoxia, CONFLICT OF INTEREST STATEMENT
hypo- or hypercapnia potentiates the symptoms of hypoxia.15 None declared.
An altitude diver experiencing AMS that may be progressing
toward HAPE would be potentially more prone to respiratory REFERENCES
injury, leading to worsening hypoxia and disturbance in the
1. Luks AM: Physiology in medicine: a physiologic approach to preven-
management of CO2 . tion and treatment of acute high-altitude illnesses. J Appl Physiol 2015;
The diver in this case minimized his initial symptoms of 118(5): 509–19.
AMS (headache and insomnia) as being expected symptoms 2. Moon RE, Martina SD, Peacher DF, et al: Swimming-induced pul-
at altitude. His high level of physical conditioning and the monary edema: pathophysiology and risk reduction with sildenafil.
Circulation 2016; 133(10): 988–96.
high motivation he had to complete a physically and men-
3. Smith R, Ormerod JOM, Sabharwal N, Kipps C: Swimming-induced
tally demanding training evolution allowed him to persist in pulmonary edema: current perspectives. Open Access J Sports Med
his training to the extent that he did. The only symptom of 2018; 9: 131–7.
HAPE before the dives was his retrospective report that he 4. Roberts MJ: Acute mountain sickness—experience on the roof of
was more winded than usual with exertion or snow shoveling. Africa expedition and military implications. J R Army Med Corps
1994; 140(1): 49–51.
Swimming-induced pulmonary edema (SIPE) is much less
5. Zafren K: Prevention of high altitude illness. Travel Med Infect Dis
commonly reported than HAPE in the literature. Most doc- 2014; 12(1): 29–39.
umented cases occur in triathletes and military personnel 6. Kawashima A, Kubo K, Kobayashi T, Sekiguchi M: Hemodynamic
conducting water (swim/dive) training. Most common symp- responses to acute hypoxia, hypobaria, and exercise in subjects suscep-
toms such as dyspnea, cough, and hemoptysis with hypoxia tible to high-altitude pulmonary edema. J Appl Physiol 1989; 67(5):
1982–9.
are also reported.3,12 A further commonality between HAPE
7. Aksel G, Çorbacıoğlu Ş K, Özen C: High-altitude illness: management
and SIPE is that athletes or service members may retrospec- approach. Turk J Emerg Med 2019; 19(4): 121–6.
tively minimize and attribute symptoms to their conditioning 8. Luks AM, Auerbach PS, Freer L, et al: Wilderness medical society
and environmental factors. Because SIPE resolves rapidly clinical practice guidelines for the prevention and treatment of acute
upon cessation of activity, many cases go unexamined.3 In altitude illness: 2019 update. Wilderness Environ Med 2019; 30(4s):
S3–18.
the reported case, the diver surfaced briefly without acknowl-
9. Li Y, Zhang Y, Zhang Y: Research advances in pathogenesis and pro-
edging any symptoms and then started another descent before phylactic measures of acute high altitude illness. Respir Med 2018;
succumbing to an acute hypoxic event. 145: 145–52.
An understanding of specific risk factors that predispose 10. Bärtsch P, Mairbäurl H, Maggiorini M, Swenson ER: Physiological
individuals to develop HAPE or SIPE remains rudimentary aspects of high-altitude pulmonary edema. J Appl Physiol 2005; 98(3):
1101–10.
at present.2,8,12,14 The goal of early diagnosis in both cases
11. Luks AM, McIntosh SE, Grissom CK, et al: Wilderness medical
is to facilitate rapid supportive care. The supportive care in society practice guidelines for the prevention and treatment of acute
either case consists of removing the individual from the incit- altitude illness: 2014 update. Wilderness Environ Med 2014; 25(4):
ing environment. High-altitude illnesses are known to affect S4–14.
396 MILITARY MEDICINE, Vol. 188, January/February 2023Pulmonary Edema During an Ice Dive at Altitude
12. Grünig H, Nikolaidis PT, Moon RE, Knechtle B: Diagnosis of swim- 14. Shearer D, Mahon R: Brain natriuretic peptide levels in six basic
ming induced pulmonary edema—a review. Front Physiol 2017; 8: underwater demolitions/SEAL recruits presenting with swimming
652. induced pulmonary edema (SIPE). J Spec Oper Med 2009; 9(3):
13. Commander, Naval Sea Systems Command: U.S. Navy diving 44–50.
manual revision 7. Available at http://www.navsea.navy.mil/Portals/ 15. Edmonds C, Lowry C, Pennefather RW: Diving and Subaquatic
103/Documents/SUPSALV/Diving/US%20DIVING%20MANUAL_ Medicine. 4th ed. CRC Press; 2001.
REV7.pdf?ver=2017-01-11-102354-393, December 1, 2016; 16. Bärtsch P: High altitude pulmonary edema. Med Sci Sports Exerc
accessed October 2021. 1999; 31(Suppl 1): S23–7.
Downloaded from https://academic.oup.com/milmed/article/188/1-2/392/6564824 by guest on 15 March 2024
MILITARY MEDICINE, Vol. 188, January/February 2023 397You can also read

















































